Paroxysmal Atrial Fibrillation in Females: Understanding
Gender Differences
Gabriel Odozynski,
1,2Alexander Romeno Janner Dal Forno,
2Andrei Lewandowski,
2Hélcio Garcia Nascimento,
2André d'Avila
2Universidade Federal de Santa Catarina,1 Florianópolis, SC – Brazil
Serviço de Arritmia e Marcapasso - Hospital SOS Cardio,2 Florianópolis, SC – Brazil
Mailing Address: Gabriel Odozynski •
Rodovia SC 401 - Hospital SOS Cardio. Postal Code 88030-000, Itacorubi, Florianópolis, SC – Brazil
E-mail: [email protected]
Manuscript received August 28, 2017, revised manuscript November 09, 2017, accepted November 22, 2017
DOI: 10.5935/abc.20180069
Abstract
Background: The catheter ablation of atrial fibrillation (AF) is performed less frequently in women. In addition, there is divergent information in the literature regarding the effectiveness and safety for the ablative procedure to females.
Objectives: The objective of this study was to compare the clinical characteristics and outcomes in men and women undergoing paroxysmal atrial fibrillation (PAF) ablation.
Methods: Cohort study of patients undergoing first-ever PAF catheter ablation procedure refractory to antiarrhythmic drugs. The information was taken from patients’ records by means of a digital collection instrument and indexed to an online database (Syscardio®). Clinical characteristics and procedures were compared between each gender (M x F), adopting a level of statistical significance of 5%. The primary endpoint associated with efficacy was freedom from atrial arrhythmia over the follow-up time.
Results: 225 patients were included in the study, 64 (29%) women and 161 (71%) men. Women presented more symptoms due to AF according to the CCS-SAF score (1.8 ± 0.8M x 2.3 ± 0.8F p = 0.02) and higher CHADS2 score compared to men (0.9 ± 0.8M x 1.2 ± 1F). Post-ablation recurrence occurred in 20% of the patients, with no difference based on gender (21% M x 20% F p = 0.52). The rate of complications was less than 3% for both groups (p = 0.98).
Conclusion: Women undergoing the first-ever PAF catheter ablation procedure present similar complication rate and clinical outcome compared to men. These findings suggest that the current underutilization of AF catheter ablation in women may represent a discrepancy in care. (Arq Bras Cardiol. 2018; 110(5):449-454)
Keywords:Arrhythmias,Cardiac; Atrial Fibrillation; Catheter Ablation; Cardiac Electrophysiology; Gender.
Introduction
Although age-adjusted prevalence of atrial fibrillation (AF) is relatively higher in men than in women, the absolute number of arrhythmia patients between genders is similar, with most cases occurring in patients between 65 and 85 years of age, a period in which, proportionately, more women are alive.1
Population studies show lower indication and execution rates of ablative treatment for AF in women with atrial fibrillation compared to men.2-5 However, it is not clear
whether this represents a discrepancy in assistance or a real difference. Based on the assumption that higher rates of complications and recurrence occur in women compared to men, the underutilization of AF ablation in women in this case, could be understood as an appropriate difference and not a direct lack of assistance.
Previous studies evaluating differences between genders regarding safety and efficacy AF catheter ablation have conflicting results, and Brazilian literature on the topic is scarce.6-13 In this study, we evaluated clinical characteristics
and outcomes of a current Brazilian women cohort undergoing ablation of AF per catheter compared to results obtained in men.
Methods
Study design and participants
Procedures
All patients underwent circumferential isolation of pulmonary veins (PVs) through irrigated catheter ablation with a 3.5 mm tip without contact force measurement, using radiofrequency energy applications up to 35 Watts and 43°C per 10-45 seconds and demonstration of entrance and exit electrical blockade of PVs in relation to left atrium at the insulation end. All procedures were performed under general anesthesia, orotracheal intubation and invasive blood pressure monitoring by radial or left femoral puncture by the anesthesiologist. Transseptal punctures were performed with the help of intracardiac Eco, which was maintained throughout the procedure. Applications to left atrium posterior wall were monitored by an oesophageal thermometer with multiple covered sensors (Circa) and stopped whenever there was a change in esophageal temperature above 38°C. During all procedures, performed with an electro-anatomical mapping system based on thoracic impedance (EnSite Navx - Abbott), IV heparin bolus of 100mg / kg was performed followed by continuous infusion to maintain coagulation time activated between 350 and 450 sec.
After the procedure, patients remained on antiarrhythmic drugs (propafenone, sotalol or amiodarone depending on preference of attending physician) for 1 month and anticoagulant for a 3 months minimum period regardless CHA2DS2-VASc. It was done clinical follow-up 1, 3, 6 and 12 months after the procedure, performing ECG and at least two Holters throughout all the clinical follow-up. At the 10th week after ablation, patients were encouraged to perform continuous electrocardiographic monitoring (Holter) for 5 days. Any atrial arrhythmia greater than 30 seconds documented duration after 1 month of blanking period indicated arrhythmia recurrence.14 Symptoms severity before
ablation and during eventual recurrences was characterized by the Canadian Cardiovascular Society Severity of Atrial Fibrillation score (CCS-SAF).15
Statistical analysis
Clinical characteristics and procedures were compared between genders (M x W). Recurrence rates after a single procedure, as well as complications were also compared between groups. A convenience sample (non-probabilistic) was adopted during the study time, respecting the inclusion/ exclusion criteria and follow-up time.
Continuous variables were described as mean and standard deviation and compared using unpaired Student's t-test (two-tailed), respecting the criteria of normality by the Shapiro-Wilk test. Categorical variables were described by absolute number and percentages in relation to total sample, and were compared using the χ² test or Fisher's exact test. Level of statistical significance adopted was 5%. Kaplan-Meier curve was used to evidence recurrence rates on the follow-up time and the Log-Rank test to evaluate difference between groups (M x W). Statistical analysis was performed using IBM SPSS Statistics Editor software, version 22.0.
Results
Patients
225 patients undergoing AF ablation were included in the study: 161 (71%) men and 64 (29%) women. Regarding follow-up time, there was no difference between men and women. Table 1 summarizes clinical characteristics
Table 1 – Clinical characteristics of patients undergoing AF ablation, categorization by gender
Variables Men (n = 161) Women (n = 64) p-value
Age (years) 57 ± 11 62 ± 9 0.001*
BMI 27 ± 3.7 27 ± 5 0.64
Ejection Fraction (%) 63 ± 10 66 ± 6 0.02*
LA Diameter (mm) 38 ± 5 38 ± 5 0.93
CHADS2 0.9 ± 0.8 1.2 ± 1 0.04*
CHF 12 (7%) 4 (6%) 0.73
SAH 85 (52%) 43 (67%) 0.06
Diabetes Mellitus 17 (10%) 11 (17%) 0.18
Coronary Artery Disease 25 (15%) 12 (19%) 0.44
Prior Stroke/TIA 6 (4% ) 5 (8%) 0.06
CCS SAF score 1.8 ± 0.8 2.3 ± 0.8 0.02*
Statin Use 44 (27%) 26 (40%) 0.03
ACE/ARA-2 Inhib 66 (41%) 30 (46%) 0.25
Previous / current use of AA 134 (83%) 58 (90%) 0.21
Diagnostic time (months) 11 ± 12 14 ± 10 0.87
Follow-up time (months) 34 ± 17 (12 – 66) 33 ± 14 (13 – 64) 0.87
Table 2 – Results of the procedures: Efficacy and safety
Variables Men (n = 161) Women (n = 64) p-value
N°. of procedures 195 77
-Complications * 5 (3%) 2 (3%) 0.98
Length of stay 2.5 ± 0.7 days 2.1 ± 0.8 days 0.76
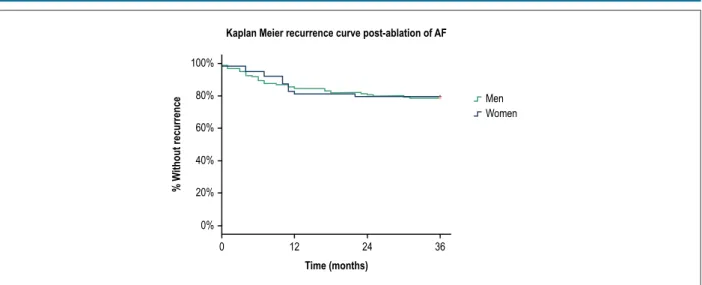
Recurrence 34/161 (21%) 13/64 (20%) 0.89
Values with ± indicate mean and standard deviation; * Men: 3 inguinal pseudo-aneurysms, 1 inguinal hematoma and 1 urethral trauma (bladder catheter). Women: 1 inguinal hematoma and 1 retroperitoneal hematoma; there were no deaths. Student’s t-test and χ2. P-value indicates a statistically significant difference at the level of 5%
of men and women who underwent paroxysmal AF ablation during the study period. Regarding the mean age, women undergoing catheter ablation were older than men (57 ± 11 M x 62 ± 9 W p < 0.01) but there was no difference between groups in relation to body mass index (BMI) and left atrium anteroposterior diameter, although a smaller LV ejection fraction, possibly without clinical relevance, was observed among males (63 ± 10% M x 66 ± 6% W p < 0.05).
There was also no difference between genders regarding comorbidities such as hypertension, diabetes mellitus, heart failure, coronary disease and previous history of stroke/TIA. However, women presented a higher CHADS2 score (0.9 ± 0.8 M x 1.2 ± 1 W, p = 0.04) and were more symptomatic than men according to the CCS-SAF score (1.8 ± 0.8 M x 2.3 ± 0.8 W p = 0.02). Between genders, there was no difference in the proportion of the use of ACE/ARA-2 inhibitors and antiarrhythmic drugs; however, women showed greater use of statins compared to men (27% M x 40% W p = 0.03 - Table 1).
Efficacy and safety of procedures
Recurrence rates after single ablation procedure were similar between groups (21% M x 20% W p = 0.52). Table 2 summarizes procedures results as well as complications by gender. There were 3 inguinal pseudoaneurysms, 1 inguinal hematoma and 1 urethral trauma during bladder catheterization in men; among women, 1 inguinal hematoma and 1 retroperitoneal hematoma (5 (3%) M x 2 (3%) W p = 0.98) were observed. Despite prolonging hospitalization time, none of the complications required surgical intervention to be controlled. Throughout the study, atrium-esophageal fistulas, pericardial effusions, TIA/stroke after ablation or death were not reported.
The Kaplan-Meier curve (Figure 1) shows, throughout the study, gender equity in relation to recurrence rates, which occurred more frequently in first 12 months of follow-up, regardless of patient's gender. There was no difference in patients hospitalization time (days) categorized by gender (2.5 ± 0.7 M x 2.1 ± 0.8 W p = 0.76).
Discussion
Gender-specific differences may influence clinical and therapeutic behaviors in women with AF assistance. In a Canadian study, Singh et al.16 characterized safety and
efficacy equivalence and homogeneity of ablative procedure between men and women with persistent AF (post-hoc MAGIC-AF Trial),16 guaranteeing its safety. In present study,
in a current patients cohort with paroxysmal AF undergoing the first catheter ablation procedure, it is suggested that recurrence rates and complications are independent of patient's gender. These findings indicate that possible clinical considerations about safety and efficacy of ablative procedures in women with AF may be the main cause of ablation underutilization in female patients.
Gender-related differences in cardiac rhythm pharmacological control are well described in literature. Women are more symptomatic by the CCS-SAF score and report a lower improvement in quality of life when submitted to drug treatment, compared to men.17 In addition, female
patients have a higher toxicity and intolerability rate to antiarrhythmic drugs than men, being more prone to Torsade de Pointes and need for pacemaker implants due to drug induced bradycardia.17,18 Therefore, catheter ablation can be
considered as an early alternative for treatment of women with AF; it is a therapeutic method superior to drug therapy in maintenance of sinus rhythm19 with low complications rates
in same proportion than men.
It is speculated that there are biological differences in the mechanism of AF between men and women, that, in theory, could justify different results when they undergo ablation, but such hypothesis seems unlikely. In previous studies, Walters et al.20 demonstrated left atrium and pulmonary veins
electrophysiological characteristics similarity in men and women.20
Similarly; Pfannmuller et al.21 verified that there were no specific
differences between genders due to atrial remodeling in AF through the expression of amyloid, collagen or bound junctions.21
In our study, the hypothesis that women in advanced age with AF present greater atrium electrical and structural remodeling and, consequently, worse post-ablation outcome, was not validated. The group of women was older than men and yet the time of diagnosis of arrhythmia is similar in both genders. In addition, left atrial diameter, a marker for post-ablation clinical recurrence, stroke, and death,22,23 was similar in both
groups. The fact that same clinical outcomes were observed in the long term between the groups also suggests that, in our study, there were no significant biological differences between men and women undergoing AF ablation.24
Limitations
Figure 1 – Kaplan Meier curves for clinical recurrence post ablation by catheter categorized by gender; Log Rank test for trend comparison between groups (MxW) p-value = 0.89
100%
80%
60%
40%
20%
0%
0 12 24 36
Time (months)
% W
ithout recurrence
Kaplan Meier recurrence curve post-ablation of AF
Men Women
submitted to ablation procedure were included in the analysis. Finally, a detailed analysis was not performed in the evaluation of symptoms resulting from AF; instead, the CCS-SAF score was used comprehensively.
Conclusion
In conclusion, in this population, women undergoing first AF catheter ablation procedure present clinical results regarding procedure safety and efficacy similar to men.
Author contributions
Conception and design of the research and Acquisition of data: Odozynski G, Dal Forno ARJ, Lewandowski A, d'Avila A; Analysis and interpretation of the data and Critical revision of the manuscript for intellectual content: Odozynski G, Dal Forno ARJ, Lewandowski A, Nascimento HG, d'Avila A; Statistical analysis and Obtaining financing: Odozynski G, d'Avila A; Writing of the manuscript: Odozynski G, Lewandowski A, Nascimento HG, d'Avila A.
Potential Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Sources of Funding
There were no external funding sources for this study.
Study Association
This study is not associated with any thesis or dissertation work.
Ethics approval and consent to participate
1. Michelena HI, Powell BD, Brady PA, Friedman PA, Ezekowitz MD. Gender in atrial fibrillation: ten years later. Gend Med. 2010;7(3):206-17. doi: 10.1016/j.genm.2010.06.001.
2. Avgil Tsadok M, Gagnon J, Joza J, Behlouli H, Verma A, Essebag V, et al. Temporal trends and sex differences in pulmonary vein isolation for patients with atrial fibrillation. Heart Rhythm. 2015;12(9):1979-86. doi: 10.1016/j. hrthm.2015.06.029.
3. Kummer BR, Bhave PD, Merkler AE, Gialdini G, Okin PM, Kamel H. Demographic difference in catheter ablation after hospital presentation with symptomatic atrial fibrillation. J Am Heart Assoc. 2015;4(9):e002097. doi: 10.1161/JAHA.115.002097.
4. Patel N, Deshmukh A, Takkar B, Coffey JO, Agnihotri K, Patel A, et al. Gender, race, and health insurance status in patients undergoing catheter ablation for atrial fibrillation. Am J Cardiol. 2016;117(7):1117-26. doi: 10.1016/j. amjcard.2016.01.040.
5. Roten L, Rimoldi SF, Schwick N, Sakata T, Hemigartner C, Fuhrer J, et al. Gender differences in patients referred for atrial fibrillation management to am tertiary center. Pacing Clin Electrophysiol. 2009;32(5):622-6. doi: 10.1111/j.1540-8159.2009.02335.x.
6. Bertaglia E, Stabile G, Pappone A, Themistoclakis S, Tondo C, De Sanctis V, et al. Updated national multicenter registry on procedural safety of catheter ablation for atrial fibrillation. J Cardiovasc Electrophysiol. 2013;24(10):1069-74. doi: 10.1111/jce.12194.
7. Zhang XD, Tan HW, Gu J, Jiang WF, Zhao L, Wang YL, et al. Efficacy and safety of catheter ablation for long-standing persistent atrial fibrillation in women. Pacing Clin Electrophysiol. 2013;36(10):1236-44. doi: 10.1111/ pace.12212.
8. Shoemaker MB, Muhammad R, Farrell M, Parvez B, White BW, Streur M, et al. Relation of morbid obesity and female gender to risk of procedural complications in patients undergoing atrial fibrillation ablation. Am J Cardiol. 2013;111(3):368-73. doi: 10.1016/j.amjcard.2012.10.013.
9. Shah RU, Freeman JV, Shilane D, Wang PJ, Go AS, Hlattky MA. Procedural complications, re-hospitalizations, and repeat procedures after catheter ablation for atrial fibrillation. J Am Coll Cardiol. 2012;59(2):143-9. doi: 10.1016/j.jacc.2011.08.068. Erratum in: J Am Coll Cardiol. 2012;59(16):1492.
10. Michowitz Y, Rahkovich M, Oral H, Zado ES, Tilz R, John S, et al. Effects of sex on the incidence of cardiac tamponade after catheter ablation of atrial fibrillation. Circ Arrhythm Electrophysiol. 2014;7(2):274-80. doi: 10.1161/ CIRCEP.113.000760.
11. Forelo GB, Tondo C, De Luca L, Dello Russo A, Casella M, De Sanctis V, et al. Gender-related differences in catheter ablation of atrial fibrillation. Europace. 2007;9(8): 613-20. doi: https://doi.org/10.1093/europace/ eum144
12. Henry L, Hunt S, Holmes SD, Martin LM, Ad N. Are there gender difference in outcomes after the Cox-Maze procedure for atrial fibrillation? Innovations (Phila). 2013;8(3):190-8. doi: 10.1097/IMI.0b013e3182a2306c.
13. Takigawa M, Kuwahara T, Takahashi A, Watari Y, Okubo K, Takahashi Y, et al. Differences in catheter ablation of paroxysmal atrial fibrillation between males and females. Int J Cardiol. 2013;168(3):1984-91. doi: 10.1016/j. ijcard.2012.12.101.
14. Calkins H, Kuck KH, Cappato R, Brugada J, Camm AJ, Chen SA, et al; Heart Rhythm Society Task Force on Catheter and Surgical Ablation of
Atrial Fibrillation. 2012 HRS/EHRA/ECAS expert consensus statement on catheter and surgical ablation of atrial fibrillation: recommendations for patient selection, procedural techniques, patient management and follow-up, definitions, endpoints, and research trial design: a report of the Heart Rhythm Society (HRS) Task Force on Catheter and Surgical Ablation of Atrial Fibrillation. Developed in partnership with the European Heart Rhythm Association (EHRA), a registered branch of the European Society of Cardiology (ESC) and the European Cardiac Arrhythmia Society (ECAS); and in collaboration with the American College of Cardiology (ACC), American Heart Association (AHA), the Asia Pacific Heart Rhythm Society (APHRS), and the Society of Thoracic Surgeons (STS). Endorsed by the governing bodies of the American College of Cardiology Foundation, the American Heart Association, the European Cardiac Arrhythmia Society, the European Heart Rhythm Association, the Society of Thoracic Surgeons, the Asia Pacific Heart Rhythm Society, and the Heart Rhythm Society. Heart Rhythm. 2012;9(4):632-96.e21. doi: 10.1016/j.hrthm.2011.12.016.
15. Dorian P, Guerra PG, Kerr CR, O’Donnell SS, Crystal E, Gillis AM, et al. Validation of a new simple scale to measure symptoms in atrial fibrillation: the Canadian Cardiovascular Society Severity in Atrial Fibrillation scale. Circ Arrhythm Electrophysiol. 2009;2(3):218-24. doi: 10.1161/CIRCEP.108.812347.
16. Singh SM, Avila AD, Aryana A, Kim Y, Mangrum JM, Michaud GF, et al. Persistent atrial fibrillation ablation in females : insight from the MAGIC-AF trial. J Cardiovasc Electrophysiol. 2016 Jul 27. doi: 10.1111/jce.13051. [Epub ahead of print].
17. Rienstra M, Van Veldhuisen DJ, Hagens Vem Ranchor AV, Veeger NJ, Crijns HJ, et al; RACE Investigators. Gender-related differences in rhythm control treatment in persistent atrial fibrillation. J Am Coll Cardiol. 2005;46(7):1298-306. doi: https://doi.org/10.1016/j.jacc.2005.05.078.
18. Torp-Pedersen C, Moller M, Bloch-Thomsen PE, Kober L, Sandoe E, Egstrup K, et al. Dofetilide in patients with congestive heart failure and left ventricular dysfunction. Danish Investigations of Arrhythmia and Mortality on Dofetilide Study Group. N Engl J Med. 1999;341(12):857-65. doi: 10.1056/NEJM199909163411201.
19. Piccini JP, Lopes RD, Kong MH, Hasselblad V, Jackson K, Al-Khatib S. Pulmonary vein isolation for the maintenance of sinus rhythm in patients with atrial fibrillation. Circ Arrhythm Electrophysiol. 2009;2(6):626-33. doi: 10.1161/CIRCEP.109.856633.
20. Walter TE, The AW, Spence S, Morton JB, Kistler PM, Kalman JM. Absence of gender-based differences in the atrial and pulmonary vein substrate: a detailed electroanatomic mapping study. J Cardiovasc Electrophysiol. 2014;25(10):1065-70. doi: 10.1111/jce.12465.
21. Pfannmuller B, Boldt A, Reutermann A, Duerrschmidt N, Krabbes-Graube S, Mohr FW, et al. Gender-specific remodeling in atrial fibrillation? Thorac Cardiovasc Surg. 2013;61(1):66-73. doi: 10.1055/s-0032-1332795.
22. Nedios S, Kosiuk J, Koutalas E, Kornel J, Sommer P, Arya A, et al. Comparison of left atrial dimensions in CT and echocardiography as predictors of long-term success after catheter ablation of atrial fibrillation. J Interv Card Electrophysiol. 2015;43(3):237-44. doi: 10.1007/s10840-015-0010-8.
23. Benjamin EJ, D’Agostino RB, Belanger AJ, Wolf PA, Levy D. Left atrial size and the risk of stroke and death. The Framingham Study. Circulation. 1995;92(4):835-841. doi: https://doi.org/10.1161/01.CIR.92.4.835.
24. Chieffo A, Buchanan GL, Mauri F, Mehilli K, Vaquerizo B, Moynagh A, et al. ACS and STEMI treatment: gender related issues. EuroIntervention. 2012;8 Suppl P:P27-35. doi: 10.4244/EIJV8SPA6.