This document was prepared under the leadership of Francesco Branca, Director of the Department of Nutrition for Health and Development (NHD), in close collaboration with Gauden Galea and Kwok-Cho Tang from the Health Promotion Unit, Department of Non-Communicable Disease Prevention. This report was developed to inform the discussion at the World Health Assembly on the Comprehensive Plan of Implementation for Maternal, Infant and Young Child Nutrition1 and is a summary of the World Health Organization (WHO) guidelines on effective nutrition programmes.
The causes of malnutrition are directly related to inadequate dietary intake and disease, but indirectly to many factors, including household food security, maternal and child care, health services and the environment. While most nutrition interventions are delivered through the health sector, non-health interventions can also be critical.
In 2011, 6.9 million children under the age of five died, mainly from preventable causes such as pneumonia, diarrhea, malaria and neonatal diseases (3, 4) (Figure 1); approximately 90% of these deaths occurred in 42 countries, while half of the deaths worldwide occurred in just 6 countries (5). Improving exclusive breastfeeding practices, adequate and timely complementary feeding, along with continued breastfeeding for up to 2 years or longer, could save the lives of 1.5 million children under 5 years of age annually (7).

WHO, Global Health Observatory (http://www.who.int/gho/child_health/en/index.html, accessed 17 March 2013). Use of multiple micronutrient powders for home fortification of foods consumed by infants and young children aged 6–23 months.
This section aims to present current WHO recommendations relevant to nutrition of mothers and children through the life-course, as well as their
Interventions targeted at young infants (0–5 months) 1
- Early initiation of breastfeeding WHO RECOMMENDATION
- Exclusive breastfeeding WHO RECOMMENDATION
- Counselling and support for appropriate feeding of low-birth-weight infants
- Infant feeding in the context of human immunodeficiency virus (HIV)
Reduced HIV transmission in the first six months of child life was associated with EBF compared with mixed feeding. Self-modified animal milk is not recommended as a substitute for food in the first six months of life.
Interventions targeted at infants and young children
- Continued breastfeeding WHO RECOMMENDATION
- Complementary feeding WHO RECOMMENDATION
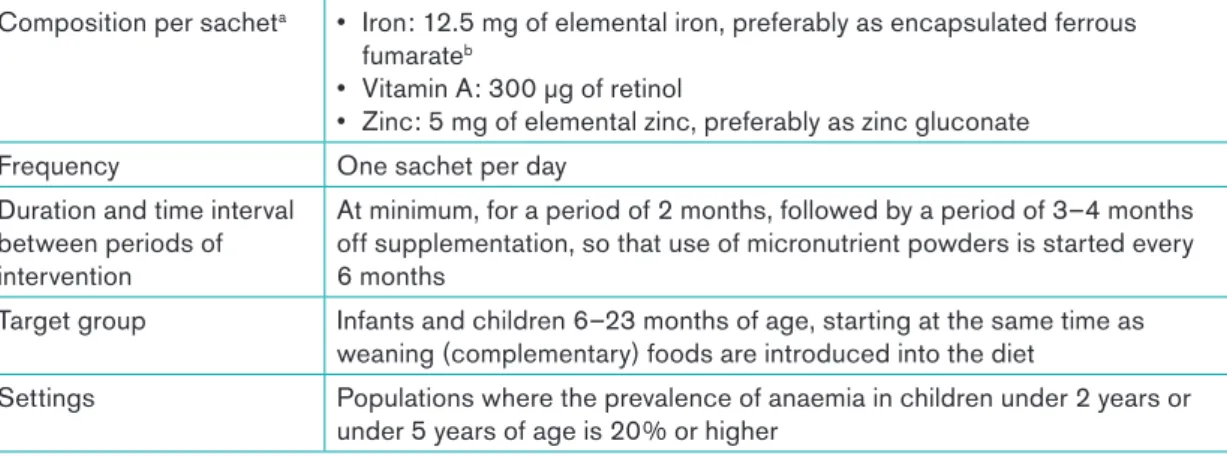
- Use of multiple micronutrient powders (MNPs) for home fortification of foods consumed by infants and young children 6–23 months of age
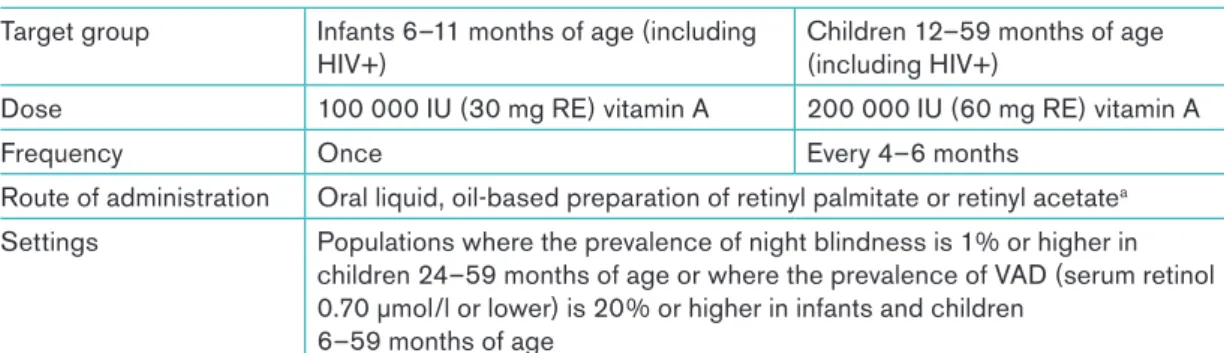
- Vitamin A supplementation for children under five years of age
- Vitamin A supplementation in children with measles WHO RECOMMENDATION
- Daily iron supplementation for children 6 to 23 months old
- Zinc supplementation for diarrhoea management
- Reaching optimal iodine nutrition in young children WHO RECOMMENDATION
- Management of children with severe acute malnutrition (SAM) WHO RECOMMENDATION FOR IDENTIFICATION OF SAM
- Management of children with moderate acute malnutrition WHO RECOMMENDATION
- Nutritional care and support of HIV-infected children 6 months to 14 years old
A suggested schedule of vitamin A supplementation for infants and children 6-59 months of age is shown in Table I-5 (75). Vitamin A supplements should be given to children aged 6-59 months twice a year, during contacts with the health system.

Assess, classify and decide a nutrition care plan
As a result, the development and implementation of guidelines on how to provide the best nutritional care to HIV-infected children has lagged behind. The guidelines for an integrated approach to the nutritional care of HIV-infected children provide guidance on how to integrate nutritional care into the integrated care of the HIV-infected child.
Implement the nutrition care plan
Children with special needs
- Nutritional care and support during emergencies
- Intervention targeted at women of reproductive age
- Intermittent iron and folic acid supplementation in menstruating women WHO RECOMMENDATION
- Interventions targeted at pregnant women
- Daily supplementation with iron and folic acid for women during pregnancy
- Intermittent iron and folic acid supplementation for non-anaemic pregnant women
- Vitamin A supplementation in pregnant women WHO RECOMMENDATION
- Calcium supplements in pregnant women WHO RECOMMENDATION
- Reaching optimal iodine nutrition in pregnant and lactating women WHO RECOMMENDATION
- Nutrition care and support for pregnant women during emergencies 1
- Global intervention
- Wheat and maize flour fortification WHO RECOMMENDATION
This should include nutritional adequacy and appropriateness of the general food ration for older infants and young children; A suggested schedule for daily iron and folic acid supplementation in pregnant women is shown in Table I-9. A suggested schedule for intermittent iron and folic acid supplementation in nonanemic pregnant women is shown in Table I-10.
Recent studies have supported this hypothesis, although there has been some inconsistency in the strength and public health applications of the associations (198, 199). The food should be intended for women in the second and third trimesters of pregnancy and during the first six months of the lactation period (ie for a total period of 12 months). Relative bioavailability of iron and folic acid from a new powder supplement compared with a traditional pill in pregnant women.
A meta-analysis of the effects of oral zinc in the treatment of acute and persistent diarrhea. Effect of therapeutic zinc supplementation in young children with selected infections: a review of the evidence.
The purpose of Part II of this document is to show how some of the essential nutrition actions described in Part I have been implemented
The evolution of evidence for the effects of nutrition interventions,
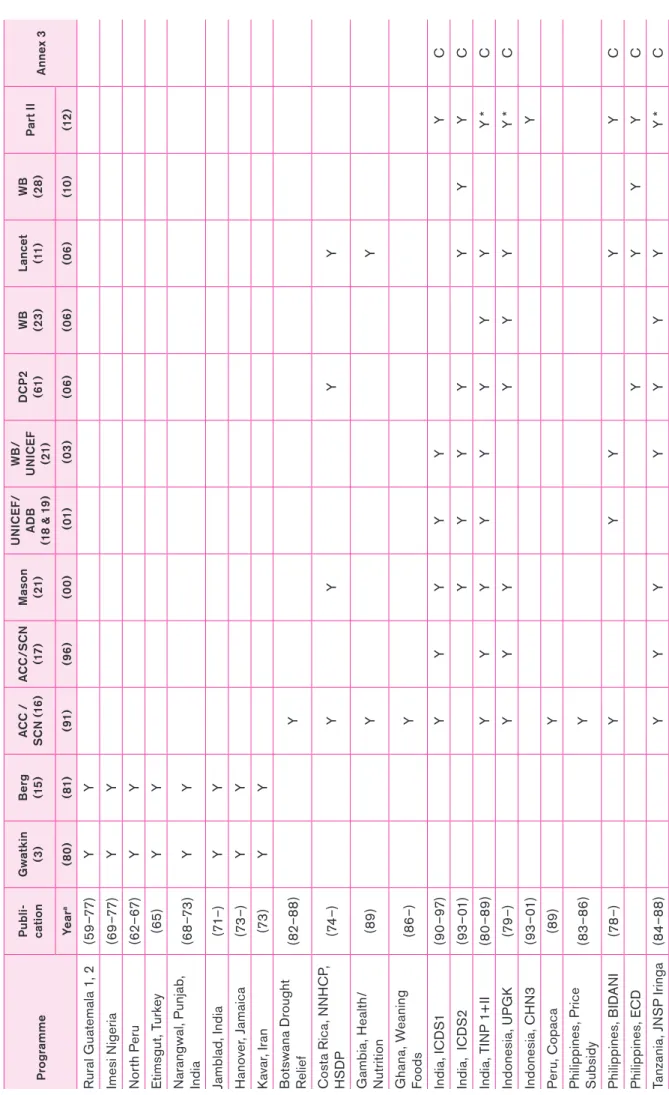
Evidence for the design of effective programs continued to be based primarily on the effectiveness of individual interventions under experimental conditions.1 A few large-scale programs started in the 1980s, such as the Tamil Nadu Integrated Nutrition Program (TINP), supported by the World bank, , and the Iringa Joint Nutrition Support Program (JNSP), supported by UNICEF and WHO, have been closely monitored, and the evidence is still significant. While many large-scale programs began in the 1970s (see Table II-1), few included impact evaluation. Program development continued without a solid evidence base, both as large-scale World Bank investments (eg in Bangladesh, Madagascar and Senegal) and as national program development (eg in Thailand and Vietnam).
1 Effectiveness refers to measured changes in outcome (eg child nutritional status) in large-scale operational programmes; and efficacy against changes in outcome estimated to be attributable to the intervention under controlled conditions. Evaluations and evaluations of operational programs gradually developed from findings from large-scale programs as they expanded from the 1980s onwards. Some of the early projects, such as the Narangwal study, tended towards evidence of efficacy and they provide a basis for later work.
Nevertheless, the lack of rigorous effectiveness evaluations of large programs was highlighted by the extensive Lancet exercise. It acknowledged the likely impact of a number of the programs reviewed and, where possible, estimated effect sizes.
What do we need to know?
The impact on whom is being estimated?
Shape of response curve
Which components via what
Program components in Part II Essential actions of nutrition in Part I of the Lancet Nutrition seriesa General nutritionb. Counseling and promotion of complementary feeding practices, +/- supplementary feeding (children; targeted complementary feeding offered in some projects). Conditional Cash Transfers Not yet covered for effectiveness Conditional Cash Transfers (dietary diversification: no effect).
Iron/Folic Acid Supplements Iron Supplements for Kids Iron Folate and Iron Supplements Iron and Folic Acid Supplements. Immunization and deworming are not included due to lack of program information; usually available in Children's Health Day activities.

Estimating nutrition
- Data sources and calculations
- Do levels of resources relate to rates of improvement?
The initial high rate of improvement among participants (estimated at approximately 8.0 ppt/year) is difficult to distinguish from the sustained rate. However, this latter rate appears to be approximately 5.0 ppt/year; with estimated 40% coverage this gives a sustained population rate of 2.0 ppt/year. The sustained rate of reduction in population underweight attributed to TINP II was 1.1 ppt/year (40).
Although no definitive evaluations exist, most reports on ICDS 1 estimated that the change in underweight attributable to the program was small (41, 42); the rate is plotted as 0.2 ppt/year. The reduction in underweight attributed to UPGK's activities based on previous research was approximately 1.0 ppt/year (22). The rate of reduction in underweight has been reported as 0.86–1.25 ppt/year (47), or approximately 1.1 ppt/year for the sustained rate in the population.
The resource intensity of CNP was approximately USD 40/family per year based on 6 months of participation for children (48).2 The estimated reduction in population underweight was 2.2 ppt/year (48). It has not been possible to derive the base rate (without program) in most cases; however, it would typically be no more than -0.5 ppt/year.
Implications
- Implications for programmes: limitations and caveats
- Specific implications for designing future programmes and sustaining existing ones
Growth monitoring alone would not be expected to improve nutrition, but has been found to be a regular activity in most programs. The reasons for this initial response are unknown and are likely due in part to disease treatment and immunization. The issue of linking with vertical programs – child health days or weeks – was not explicitly examined here.
Experiences in six African countries (58, 59) show that there are opportunity costs associated with child health days/weeks for community-based programs (e.g., while these may be mutually supportive, only some interventions are effective at the six-monthly periodicity typical of days/weeks). weeks in child health care (particularly immunization).In summary, community-based nutrition programs appear to be reasonably effective in significantly reducing child malnutrition.
To do this, they must be sustained and sustained long enough to create lasting change. If they continue long enough to create an intergenerational impact – fewer little girls growing up to be little mothers having little babies – they could in principle help bring about a permanent change in the nutritional status of the population.
Cash Transfer Programmes
- Mechanisms, demand and supply-side
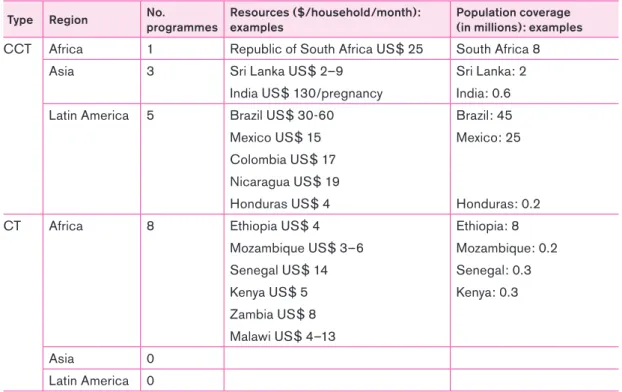
- Coverage and resource intensities
- Effect on nutrition outcomes
- Linkage to direct nutrition programmes
An increase in household purchasing power for food and health services may result from CCT programs (65). The Mexican Oportunidades has several evaluations reporting an increase in height of approximately 1.0 cm in children aged 0–6 months and 12–36 months, all compared to controls (62). An increase in birth weight of 0.13 kg was reported among beneficiaries compared to controls in the Mexican Oportunidades (74).
Nutrition – 0.13 decrease in HAZ scores in children less than 7 years compared to control (1) – no results reported: conditioning not monitored due to lack of available health services (2). Intermediate – 20.2% increase in child health visits (at least 1 in the past month) compared to control – 18.7% increase in women having more than 5 antenatal visits compared to controls (1) Nutritional – No there are changes in health outcomes, including HAZ outcomes; it may be due to lack of program implementation and/or poor evaluation quality.
Intermediate – limited 7% average increase in HH food consumption among the poorest 40% (13) Zambia Kalomo Pilot Social Cash Transfer Scheme 2004–present. A review of the impact of cash transfer programs on children's nutritional status and some implications for Save the Children UK programmes.
Madagascar 11
Pakistan 14
Tanzania 17 Thailand 19
Bibliography 26
The World Bank's implementation report (1) on the National Nutrition Program was critical of the plan and its ineffectiveness. It is estimated that a quarter to a half of the decrease in underweight prevalence can be attributed to the project. A major problem related to the effectiveness of the program is the fact that the coverage is much higher in.
This decrease can be partially attributed to the decline in birth rates in the lowest quintile of the population (28). Galasso and Yau (31) found that "values decrease as time and duration increase, although they do not dissipate to zero." The results also showed higher differential returns in poorer and disease-vulnerable areas. Due to the short duration of the program and the evaluation immediately after its completion, the lack of results is understandable.
The resource intensity of the JNSP ranged from $8 to $17 per child per year (total cost $30 per child per year, which amounts to $6 million). The decline in the first two years of the program was even greater at 8 ppt/year, although the continued decline in underweight in the population was 0.8 ppt/year (for years 2 to 7) . In fact, the figures from 1982 – the first growth monitoring data – and the recent national survey (2005/2006) are somewhat vague, but the overall major improvement is clear.
Evaluating interventions to improve child nutrition: a theory-based impact evaluation of the Bangladesh Integrated Nutrition Project.
EXCLUSIVE BREASTFEEDING - COMPLEMENTA FEEDING - VITAMIN A, IRON, ZINC - BREAST