Original Article
ANALYZING EFFECT OF CONTOURED FOAM SEAT ON M ULTIDIRECTIONAL
REACHING ABILITY IN ACUTE STROKE SUBJECTS
Teena Padiyar
1, Abhishek Sharma
2, Lipy Bhat
3, Ravinder Narwal
4.
1 Post Graduate, M .P.T (Neurology), 2,3,4 Lect urer,
Depart ment of Physiot herapy, HIHT Universit y, Dehradun U.K, India.
Background & Objective:Cerebrovascular accident is t he m ajor disease t hat leads t o an increase in t he num ber of people w it h m ot or or sensory im pairm ent or loss of f unct ion on one side of t he body (hem ipelgia). Poor sit t ing abilit y is a com m on problem aft er st roke. Sitt ing involves not only t he abi lit y t o m aintain t he seat ed post ure, but also t he abilit y t o reach for a variet y of object s locat ed bot h w it hin and beyond arm ’s lengt h. Cont oured foam seat (CFS) have show n im provem ent in sit t ing post ure, head cont rol and upper ext rem it y funct ion in pediat ric age group suffering from cerebral palsy in previous st udies. So t his st udy w as designed t o evaluat e t he effect iveness of cont oured foam seat on sitt ing post ure and m ult idirect ional reaching abilit y in acut e st roke subject s. M et hodology:The st udy design of t his pilot st udy is having t en Acut e st roke subject s as sam ple. Aft er taking t he inform ed consent , subject s w ere m ade t o sit on a chair and m ult idirect ional reaching abi lit y dist ance w as m easured w it h and w it hout cont oured foam seat . M ult idirect ional reaching dist ance w as assessed w it h CFS and w it hout CFS and obt ained data w as analyzed. Data w as collect ed by m easuring t he m axim um reaching abi lit y dist ance. Result: Reaching abilit y in sit t ing posit ion signif icant ly im proved aft er applicat ion of CFS. Unaffect ed side reaching w as signif icant ly im proved as com pare t o for w ard and affect ed side reach aft er applicat ion of CFS. Discussion & Conclusion: Cont oured foam seat can significant ly im prove pelvic alignm ent and provide a good post ural stabi lit y t hereby im prove sit t ing post ure and funct ional reaching abi lit y in acut e st roke subject s.
KEYW ORDS:Acut e St roke; Reaching Abi lit y; Cont oured foam seat .
Quick Response code
Access this Article online
International Journal of Physiotherapy and Research
ISSN 2321- 1822
w w w.ijmhr.org/ ijpr.html
Received: 09 Sept 2013 Accepted: 05 Oct ober 2013
Published: 11 Oct ober 2013
ABSTRACT
INTRODUCTION
Address for correspondence: Dr.Ravinder Narw al, Lect urer, Depart m ent of Physiot herapy, HIHT Universit y, U.K, India. Email: [email protected]
Stroke is t he leading cause of long term disabilit y among adult s. Longit udinal st udies of recovery after st roke suggest t hat only 50% of patient with significant arm paresis recover useful funct ion. Hemiplegic wit h poor sitt ing abilit y is a common problem after st roke
.
1,2
A prospect ive st udy demonst rated t hat 48% and 27% o f st r o ke p at i ent w er e u n abl e t o si t independent ly at t he onset and t he end of rehabilitat ion respect ively. Funct ional abilit y t o m aint ain norm al sit t ing post ure is based on funct ional act ivit y in a seated post ure. Recovery of sitt ing after st roke is important for individual
because si t t in g i s a ski l l t h at is cr it i cal t o independent living. Sitt ing involves not only t he abilit y t o maintain t he seated post ure, but also the abilit y to reach for a variety of objects located bot h w it hin and beyond arm’s lengt h.3
The disabilit y in reaching tasks arises not only from t he im pairm ent s caused by t he neural lesion, such as weakness and loss of coordinated movement , but also from t he tendency t o adapt behavior t o avoid t he t hreat t o balance. Sitt ing abilit y has been show n t o be a useful prognost ic indicat or of outcome for t his populat ion. 4
M ETHODOLOGY
after st roke are slow er and do not load t heir affected foot or act ivate muscles of t he affected leg sufficient ly w hen reaching beyond arm ’s lengt h in sitt ing (Dean and Shepherd 1997). In previous st udies cont oured foam seat (CFS) have been show n improvem ent in sitt ing post ure, head cont rol and upper ext remit y funct ion in pediat r ic age group suffer ing f rom cerebral palsy.5
Cont oured foam seat is a t ype of adapt ive seat device current ly used by t herapist , w hich is intended t o improve pelvic alignment , increase post ural stabilit y and somat osensory feedback for chi ldren w it h neurom ot or im pair m ent . Benefit s of adapt ive seat ing include improved post ural alignm ent and facilitat ion of upper-ext remit y funct ion.6
It i s i m p er at i ve t h at h eal t h pr o f essio n al s prescribing and engineers designing seat ing equipm ent are w ell infor m ed regarding t he fundamental seat ing principles t hat dictate t he sit t ing post ures of children and young people and t he impact t hey have on long term healt h and funct ion. So t his research w as design t o co nf i n e w h et h er CFS can en h an ce mult idirect ional reaching abilit y in acute st roke subject .
The st udy design of t his pilot st udy is having ten Acute st roke subjects as an sample at Himalayan hospital Dehradun-UK.Inclusion criteria: Bot h m ale and fem ale, GCS should be 15, M M SE-m ore t han 23, Subject s should be SE-m edically cleared by t he physician for physiot herapy and m ob i l izat io n , Age- 40 t o 65, Ab l e t o si t independent ly for 10 second, Sit t ing balance score is 2 according t o M AS ( mot or assessment scale for st roke pat ient s). Exclusion crit eria: V isu al an d hear i n g i m p air m en t s, Sen sor y aphasia, Ort ho-pedic problem s w hich w ould int erfere w it h t he abi lit y t o perform seat ed r each i ng t ask s, p r essu re sor e. Ou t co m e m easure- M axim um reachin g dist ances in forward and sideway direct ion.
Procedure: 10 subject s w ere screened based on t he inclusion and exclusion criteria. Consent was taken and t he purpose and procedure of t he st udy w as explained t o t he pat ient and care takers.
Preparation of the test room: Test room w hich comprise of a chair w it h hand and back support , a vert ical and m ovable m irror, m ovable and vert ical upright pole. A point in t he floor was marked beneat h t he chair by calculat ing t he mid of t he distance bet w een t he front t w o legs of t he chair. From t hat midpoint 1 perpendicular and 2 line at 450 was draw n w it h t he help of
goniom eter and m arker. Then a cello t ape is applied over t he line draw n by t he marker. M irror was placed in front of t he chair.
Pre test reading- pre test reading was taken in the follow ing manner:
Pat ient is shifted t o test ing room and made t o sit on t he chair. Pat ient was asked t o maintain erect sitt ing post ure w it hout using back support distance bet w een acromion process of shoulder and floor was measure wit h measuring tape, t his distance w as m arked in t he pole w it h green ribbon .And t hen ask t o reach forward w it h non affected upper limb and 900 flexion of shoulder
w it hout losing balance. Vert ical pole was made in contact w it h t he middle finger of t he pat ient . 3 t rials w ere given and t he best forward reach distance was measured. Then t he pat ient was ask to reach at 450 side way t oward left and right
in sam e m anner and t he maxim um reaching distance was measured after 3 t rial.7
After collect ion of pretest reading half an hour break was given t o t he pat ient . Then cont oured foam seat was placed on t he chair. Pat ient made t o sit on t he cont oured foam seat and ask t o obtain forward and sideway reach without losing b al an ce. Po st t est m axi m u m r each w as measured again.
RESULTS
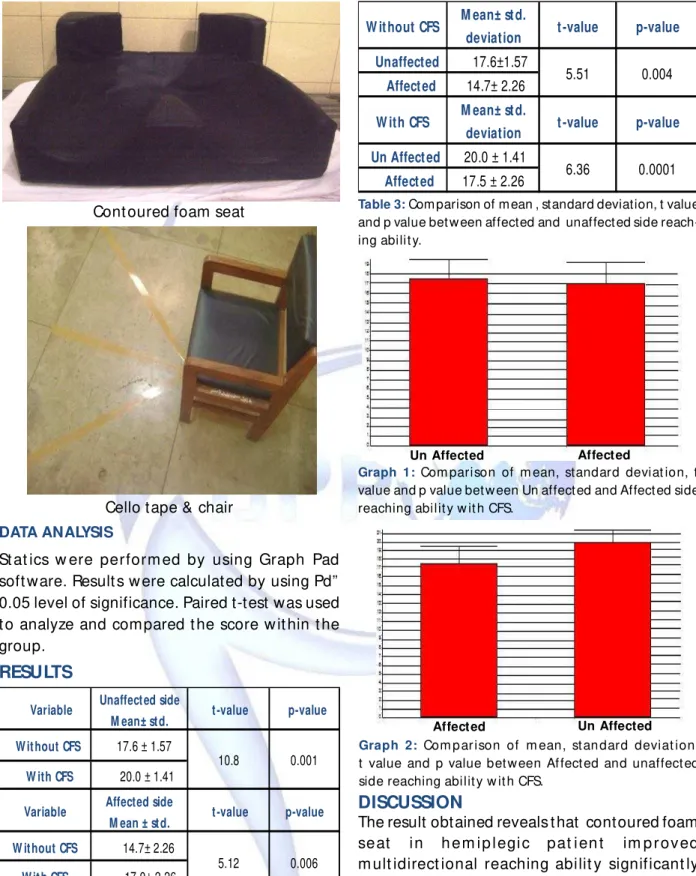
Cont oured foam seat
Cello tape & chair
DATA ANALYSIS
St at ics w ere perform ed by using Graph Pad soft ware. Result s w ere calculated by using Pd” 0.05 level of significance. Paired t-test was used t o analyze and compared t he score w it hin t he group.
W ithout CFS 14.7± 2.26
W ith CFS 17.0± 2.26
10.8 0.001 17.6 ± 1.57
W ithout CFS
W ith CFS 20.0 ± 1.41
Variable Unaffected side
M ean± std. t-value p-value
Variable Affected side
M ean ± std. t-value p-value
0.006 5.12
Table 1: Com parison of m ean, standard deviat ion, t value and p value of reaching abilit y w it h CFS and w it hout CFS.
Table 2: Com parison of m ean, standard deviat ion, t value and p value bet w een for w ard reaching abi lit y w it h and w it hout CFS.
W ith CFS 17.5±2.06
W ithout CFS 15.8± 2.48
5.07
Variable M ean± std.
deviation t-value p-value
0.007
Table 3: Com parison of m ean , standard deviation, t value and p value bet w een affected and unaffect ed side reach-ing abilit y.
Un Affected Affected
Graph 1: Com parison of m ean, standard deviat ion, t value and p value bet w een Un affect ed and Affect ed side reaching abilit y w it h CFS.
Affected Un Affected
Graph 2: Com p ar ison of m ean, st an dard deviat ion, t value and p value bet w een Af fect ed and unaffect ed side reaching abilit y w it h CFS.
DISCUSSION
The result obtained reveals t hat contoured foam seat i n h em i p l egi c pat i en t im p r ov ed m ult idirect ional reaching abilit y significant ly proving t he hypot hesis of t he st udy.
After applicat ion of CFS forward, unaffected and af fect ed sid e r each ing ab i lit y sign if icant ly improve. Seat ing literat ure suggested t hat t he pelvis dictates t he post ure in t he rest of t he body and experimental st udies suggested t hat pelvic posit ion as a determinant of post ural alignment for w it h neuromot or impairment .
CFS im proves post ure alignm ent and of fer biomechanical advantage by keeping t he pelvis
W it hout CFS M ean± st d.
deviation t -value p-value
Unaffected 17.6±1.57
Affect ed 14.7± 2.26
W ith CFS M ean± st d.
deviation t -value p-value
Un Affect ed 20.0 ± 1.41
Affect ed 17.5 ± 2.26
5.51
6.36 0.0001
186 in neut ral posit ion and lim it s t he degree of
freedom. This neut ral posit ion of pelvis increases t he post ural stabilit y t hrough w hich pat ient can cont rol t he ot her segment of body and modify t h eir reachi ng in all dir ect ion .CFS is m o re congr uent as com pare t o norm al seat and provides more body cont act w it h t he seat ing surface t hat facilitates more cont rol and support t o t he subject s.7.8
Post ural cont rol also may have been assisted by nonslip foam surface of CFS The vinyl surface of t he chair allow ed lat eral or for w ard pelvic m ovem ent , leading t o pelvic obliquit y and asymmet rical w eight bearing.
In hem iplegic pat ient t here is a t endency of pelvis t o ret ract and hip goes in external rotation t h ro ugh w h ich f oo t go es i n i nv er si on and supinat ion and at t he end prevent wait bearing on affected foot. CFS t here for prevent ret ract ion and hip external rotat ion by t he lateral support t hat increases wait bearing on affect ed foot . M assion J. et al suggested t hat foot pressure on t he left side w ould be great er t han t he foot pressure on t he right side of t he healt hy subject during t he reaching task because t here w ould be counterbalancing procedure in response t o right reaching arm. 9,10
Unaffected side reaching abilit y is significant ly more t han forward and affected side reach after applicat ion of CFS and W it hout CFS because hemiplegic patient used t heir unaffected foot for most of t he w eight bearing during reaching task an d w h en t her e w as m o v em en t t o w ar d un af f ect ed si de w ait t ransfer in creases in affected foot .11,12
Forward reach is more significant ly improve t han affected side reach w it hout CFS but t here was no significant improvement in forward reach and affected side reach after applicat ion proves t hat affected side reaching is also improve w it h CFS.
CONCLUSION
Cont oured foam seat effect ively cont rol sitt ing post ure and t hereby can significant ly improve mult idirect ional reaching abilit y in acute st roke subject s.
CLINICAL IM PLICATION
After st roke, regaining early sitt ing balance and cont rol is prerequisite for t he t herapy and it is not possible t o perform t herapy for long hours in acute condit ion t herefore CFS can be used t o regain sitt ing balance and im prove funct ional reaching abilit y and for Sit t o stand t hat provides maximum w eight bearing on affected lower limb
LIM ITATION OF THE STUDY
The small sample size was t he major limitat ion of t he st udy. CFS was not tailored as per t he size of each subject . Standard size was taken for t he st udy.
FUTURE RESEARCH
Furt her st udies can be done w it h larger sample size and on long term effect of CFS. CFS can be cust omizing as per t he need of t he pat ient s. Fut ure researches can be done on pusher ’s syn d r om e, cer eb r al p alsy, si t t i n g b al an ce disorder like paraplegia quadriplegia.
Conflict of Interest & ethical approval
There was no conflict of interest was reported am o n g al l au t ho r s. Th is r esearch w o r k i s approved by et hical committee of HIPM S, HIHT Universit y (UK) India.
REFERENCES
1. Leeanne M Careyet .al M ot o r i m pai r m ent and recovery in t he upper lim b aft er st roke 2005; 36: 625-629.
2. Tapas Kum ar Banerjee et .al Epidem iology of st roke in India. Neurology Asia 2006; 11: 1-4.
3. Wade DT, Wood VA. Langt on-Hew er R. Recovery aft- er st roke: t he first 3 mont hs. J Neurol Neurosurg
Psychiatry. 1985;48: 7.
4. M organ P. The relat ionship bet w een sitt ing balance an d m o b i l i t y o u t co m e i n st r o ke . Au st J Physiot herapy.1994;40:91-96.
5. Dean C, and Shepherd, R; Task relat ed t raining im proves per for m ance of seat ed reaching t asks follow ing st roke: A random ized cont rol t rial, 28: 722,1997.
6. Lo ew en SC, And erson BA. Pr edict ors of st roke o u t co m e u si n g o b j e ct i v e m easu r e m en t
scales. Stroke. 1990;21:78-81.
7. Shepherd RB. Adapt ive m ot or behavior in response t o pert urbat ions of balance.Physiot herapy Theory and Pract ice. 1992;8:137-143.
9. M assion J, alexandrov, A,Frolov A: Why and how are post ural sym m et r y in sitt ing in people w it h hem ipelgia ?Brain inj,2003,17:789-797.
10. Snehal Bhupendra Shah, Sm ita Jayavant . St udy of Balance t raining in am bulat ory Hem iplegics. The Indian Journal of Occupat ional Therapy 2006; 38: 1.
11. PM Dalal, M adhum ita Bhattacharjee, Jaee Vairale, Priya Bhat . M um bai St roke Regist ry (20052006) Sur veillance Using WHO St eps St roke Inst rum ent -Challenges and Opport unit ies. JAPI 2008; 56: 675-80.
12. D. Nagaraja, G. Gururaj, N. Girish, Sam hita Panda, A.K. Roy, G.R.K. Sharm a, R. Srinivasa. Feasi bi lit y st udy of st roke surveillance: Data from Bangalore, India. Indian J M ed Res. Oct ober 2009; 130: 396-403.