Inb o rn e rro rs o f me ta b o lis m: a c linic a l o ve rvie w
Department of Pediatrics, Universidade Federal de São Paulo/
Escola Paulista de Medicina, São Paulo, Brazil
Ana Maria MartinsINTRODUCTION
In 1 9 0 4 the do c to r Arc hib a ld E. G a rro d desc rib ed a lka pto nuria , a disea se he c la ssified a s a life lo ng c o ng e nita l c he mic a l a lte ra tio n. La ter o n, in 1 9 0 9 , he desc rib ed o ther disea ses: a lb inism, c ystinuria , po rphyria a nd pento suria , which he named “ Inbo rn Erro rs o f Metabo lism” . G a rro d’s c o nc lusio ns were c o mpletely c o rrec t in re la tio n to the g e ne tic b a sis o f me ta b o lic diso rders a nd the g ene–enz yme c o nc ept.1
Ac c o rding to Sc river, in the fo rewo rd o f “ Physic ia n’s G uide to the La b o ra to ry Dia g no sis o f Me ta b o lic Dise a se s” ,2 the imp o rta nc e o f G a rro d ’ s o b se rva tio n tha t inb o rn e rro rs o f me ta b o lism (IEM ) a re ma nife sta tio ns o f bio chemical individuality was never reco g niz ed during his lifetime, no r ha s it b een in o ur da ys, b e c a use ma ny d o c to rs still think o f IEM a s situa tio ns o f extreme ra rity tha t will never b e se e n in the typ ic a l me d ic a l p ra c tic e . IEM pro duc es ma nifesta tio ns in every o rg a n, fro m the fe tus to g e ria tric life a nd the y a re o mnipresent in a ppea ra nc e, no t respec ting the d o c to r’ s q ua lific a tio ns a s a g e ne ra list o r spec ia list.
Inb o rn e rro rs o f me ta b o lism c a use he re d ita ry me ta b o lic d ise a se s (HM D) a nd
ABSTRACT
CON TEXT: Inborn errors of metabolism cause hereditary metabolic diseases (HMD) and classically they result from the lack of activity of one or more specific enzymes or defects in the transportation of proteins.
OBJECTIVES: A clinical review o f inbo rn erro rs o f metabo lism (IEM) to g ive a practical appro ach to the physician with fig ures and tables to help in understanding the mo re co mmo n g ro ups o f these diso rders.
DATA SOURCE: A systematic review o f the clinical and bio chemical basis o f IEM in the literature, especially co nsidering the last ten years and a classic textbo o k (Scriver CR et al, 1 9 9 5 ).
SELECTION OF STUDIES: A selectio n o f1 0 8 references abo ut IEM by experts in the subject was made. Clinical cases are presented with the peculiar sympto ms o f vario us diseases.
DATA SYN THESIS: IEM are frequently misdiag no sed because the g eneral practitio ner, o r pediatrician in the neo natal o r intensive care units, do es no t think abo ut this diag no sis until the mo re co mmo n cause have been ruled o ut. This review includes inheritance patterns and clinical and labo rato ry finding s o f the mo re co mmo n IEM diseases within a clinical classificatio n that g ive a g eneral idea abo ut these diso rders. A summary o f treatment types fo r metabo lic inherited diseases is g iven.
CON CLUSION S: IEM are no t rare diseases, unlike previo us thinking abo ut them, and IEM patients fo rm part o f the clientele in emerg ency ro o ms at g eneral ho spitals and in intensive care units. They are also to be fo und in neuro lo g ical, pediatric, o bstetrics, surg ical and psychiatric clinics seeking diag no ses, pro g no ses and therapeutic o r suppo rtive treatment.
KEY W ORDS: Inbo rn erro rs o f metabo lism. Metabo lic inherited disease. Diag no sis.
c la ssic a lly they result fro m the la c k o f a c tivity o f o ne o r mo re spec ific enz ymes o r defec ts in the tra nspo rta tio n o f pro teins. The c o nseq uenc es c a n usua lly b e the a c c umula tio n o f sub sta nc es p re se nt in sma ll a mo unts, the d e fic ie nc y o f c ritic a l intermedia ry pro duc ts, the defic ienc y o f sp e c ific fina l p ro d uc ts o r furthe rmo re the no xio us e xc e ss o f p ro d uc ts o f a lte rna tive meta b o lic pa thwa ys.3
The mo le c ula r b a sis o f b io c he mic a l d iso rd e rs in HMD a re g e ne tic muta tio ns in enz yma tic lo c i tha t a ffec t a c tiva to r pro teins o r c o -fa c to rs fo r enz ymes, pro tein tra nspo rta tio n, c a rrier systems o r rec o g nitio n ma rkers.3 ,4
Incidence
Mo re tha n three hundred huma n disea ses a re kno wn to da y tha t a re c a used b y inb o rn e rro rs o f me ta b o lism a nd this numb e r is c o nsta ntly g ro w ing b e c a use o f ne w id e ntific a tio n te c hniq ue s fo r the va rio us b io c he mic a l p he no ty p e s. Ho w e ve r, the d e te c tio n o f HM D inc id e nc e ha s no t b e e n inc re a sing in pa ra lle l, pro b a b ly b e c a use its d ia g no sis is b e ing und e re stima te d . Fa ulty diag no sis o f IEM is related to a series o f facto rs: (1 ) they a re individua lly c o nsidered ra re a nd therefo re ma ny physic ia ns do no t c o nsider IEM until mo st freq uent c o nditio ns ha ve b een ruled o ut, (2 ) b lo o d a nd urine sa mp le s fo r inve stig a tio n o f me ta b o lic e rro rs ne e d to b e co llected at the rig ht time in relatio n to the co urse o f the disease, and (3 ) many metabo lic diseases o nly pro duc e intermittent a b no rma lities.3 ,5 ,6
IEM are no t rare diseases when we o bserve their cumulative incidence,7 which is abo ut o ne in e ve ry 5 0 0 0 live b irths. N e ve rthe le ss, the prevalence o f each disease has many variables, especially relating to race. Examples o f frequency fo r specific diseases include: 1 in 5 0 0 fo r familial hy p e rc ho le ste ro le mia ;8 1 in 1 2 , 0 0 0 fo r phe nylke to nuria ;4 ,9 1 in 1 5 ,0 0 0 fo r o rg a nic acidurias;1 0 1 in 6 0 ,0 0 0 fo r g lyco g en sto rag e diseases;4 1 in 4 5 ,0 0 0 fo r g alacto semia;8 1 in 1 0 0 ,0 0 0 to ho mo cystinuria8 and 1 in 2 9 0 ,0 0 0 fo r maple syrup urine disease.1 1
In Bra z il the inc idenc e o f so me spec ific
IEM diso rde rs ha ve b e e n fo und to b e : 1 in 1 1 ,8 1 8 to 1 in 1 5 ,0 0 0 fo r phenylketo nuria;1 2 ,1 3 1 in 4 3 ,0 0 0 fo r ma ple syrup urine disea se;1 2 a nd 1 in 1 2 5 ,0 0 0 fo r b io tin defic ienc y.1 4
Inheritance Patterns
The ma jo rity o f HM D a re inhe rite d a uto so ma l re c e ssive tra its, i. e . the y ha ve a rec urrenc e risk o f 2 5 % fo r ea c h g esta tio n o f he te ro z yg o us pa re nts. So me dise a se s a re X-linke d , tha t is, the mo the r is c a rrie r o f the muta tio n, with the risk o f rec urrenc e fo r ea c h g esta tio n in these c a ses b eing 5 0 % fo r ma les a nd 5 0 % fo r fe ma le s to b e c a rrie rs o f the muta tio n who c a n pa ss it o n to their c hildren. There a re in a dditio n mito c ho ndria l disea ses, determined by mutatio ns in mito cho ndrial DN A, in whic h the risk o f rec urrenc e is virtua lly 1 0 0 % o f the c hildren o f b o th sexes.3
CLINICAL CLASSIFICATION OF INBORN
ERRORS OF METABOLISM
O ne o f the mo st educ a tio na l a nd c linic a l c la ssific a tio ns o f IEM is to b e fo und in The Me ta b o lic a nd Mo le c ula r Ba se s o f Inhe rite d Dise a se , 1 9 9 5 e d itio n,1 5 b y Sa ud ub ra y & C ha rp e ntie r,5 w hic h c la ssifie s IEM in a c c o rda nc e with the c linic a l phe no type a nd presents ta b les o f sig ns a nd sympto ms a nd flo w c ha rts tha t a id da ily pra c tic e g rea tly. Ta b le 1 sho ws a summa ry o f the a utho rs’ c la ssific a tio n.
Category 1
Disea ses tha t o nly a ffec t a func tio na l o r a na to mic a l system o r a n o rg a n, suc h a s the endo c rine system, immune system, c o a g ula tio n fa c to rs o r lip o p ro te ins. The symp to ms a re unifo rm a nd the c o rre c t dia g no sis is usua lly e a sy, b e c a use the b a sis o f the b io c he mic a l defec t inc o rpo ra tes the g iven c o nseq uenc e, fo r exa mple, the tendenc y to b leed seen in c a ses o f c o a g ula tio n defec ts.
Category 2
Diseases in which the bio chemical basis affects o ne metabo lic pathway co mmo n to a great
number o f cells o r o rg ans, such as in sto rag e diseases due to lyso so mal diso rders, o r is restricted to o ne o rg a n w ith humo ra l a nd syste mic c o nse q ue nc e s, suc h a s hype ra mmo ne mia in defects o f the urea cycle o r hypo g lycemia in hepatic g lyco g enesis.
Dise a se s in this c a te g o ry ha ve g re a t c linic a l dive rsity. The c e ntra l ne rvo us syste m (CN S) is frequently attacked and in the evo lutio n o f the disea se ma ny sec o nda ry a b no rma lities can appear, making the diag no sis mo re difficult. This c a te g o ry inc lud e s ma ny e rro rs in intermediary metabo lism (carbo hydrate defects; a mino a c id o r o rg a nic a c id meta b o lism with prima ry o r sec o nda ry disturb a nc es o f vita min o r meta l ho meo sta sis; purine a nd pero xiso me diso rde rs), dise a se s o f intra c e llula r tra nspo rt (endo pla smic retic ulum a nd G o lg i a ppa ra tus defec ts) a nd lyso so ma l diso rders.
These disea ses c a n b e divided into three g ro ups fro m a physio pa tho lo g ic a l perspec tive, g rea tly a ssisting in dia g no stic rea so ning .
Group I
Disturbances in the synthesis o r catabo lism o f c o mp le x mo le c ule s. The symp to ms a re p e rma ne nt, p ro g re ssive , ind e p e nd e nt o f inc id e nta l e ve nts a nd a re no t re la te d to a limenta ry ing estio n.
Lyso so ma l Diso rders. Also c a lled sto ra g e d ise a se s. The se le a d to the p ro g re ssive a c c umula tio n o f undig ested sub stra tes, usua lly po lymers, tha t c a nno t usua lly b e hydro lyz ed. The po lymers a c c umula te in lyso so mes, where the y c a n b e se e n using o p tic a l o r e le c tro n mic ro sc o py. The a ffec ted tissues a re tho se in whic h the sub sta nc e is usua lly c a ta b o liz ed in g re a t q ua ntitie s: c irc ula ting lymp ho c yte s, fib ro b la sts, live r, sp le e n, c o njunc tiva , b o ne ma rro w a nd inte stina l muc o sa . The c linic a l ma nife sta tio ns in this g ro up a re g e ne ra lly he p a to me g a ly o r he p a to sp le no me g a ly ; dysmo rphic features (co arse facial features) that a re pre se nt a t b irth (G M1 g a ng lio sido sis) o r
d e ve lo p in the first ye a rs o f life (muc o p o -lysa c c ha rido sis); o phtha lmo lo g ic a l, b o ne, jo int a nd c entra l nervo us system (CN S) invo lvement.
Ta b le 24 lists lyso so ma l diso rders.
Pe ro x iso ma l Bio g e ne sis Diso rd e rs. Invo lving ma ny a na b o lic func tio ns. The se inc lude the b io synthesis o f pla sma lo g en, whic h is a ma jo r myelin c o mpo nent, c ho lestero l a nd bile acids. G eneralized pero xiso mal
β
-o xidatio n defic ienc y results in a va riety o f disturb a nc es that are still no t well understo o d, partly because the re is a n o ve rla p in func tio n b e tw e e n the pero xiso mes a nd o ther o rg a nelles suc h a s the mito c ho ndria a nd the endo pla smic retic ulum. The se multip le a nd c o mp le x b io c he mic a l a b no rma litie s re sult in sp e c ific d e fe c ts o f ne uro na l mig ra tio n w ith ma lfo rma tio ns a nd se ve re ne uro lo g ic d ysfunc tio n, hyp o to nia , me nta l re ta rd a tio n a nd d e ve lo p me nta l reg ressio n. In c o ntra st to lyso so ma l diso rders, the re is no intra c e llula r a c c umula tio n o f undig ested po lymers. A useful ma rker fo r their diag no sis is the accumulatio n o f very lo ng chain fa tty a c id s in p la sma , suc h a s X-linke d adreno leuko dystro phy (“ Lo renz o ’s o il disease” ). Ta b le 24 lists the disea ses in this g ro up.Defects In Intracellular Transpo rt. Invo lving de fe c ts in intra c e llula r tra nspo rt a nd pro te in pro c essing . This g ro up inc ludes
α
1-a ntitrypsind e fic ie nc y a nd c a rb o hy d ra te -d e fic ie nt g lyc o pro tein syndro me.
Group 2
Inbo rn erro rs o f intermediary metabo lism le a d ing to a c ute a nd re c urre nt into xic a tio n (me ta b o lic a c id o sis, vo miting , le tha rg y, dehydratio n, thro mbo embo lic co mplicatio ns) o r
Table 1 - Clinical classification of inborn errors of metabolism5
Categ o ry 1 Invo lving a functio nal system
Categ o ry 2 Affecting metabo lic pathways co mmo n
to a g reat number o f cells o r o rg ans
G ro up 1 Defects in the synthesis o r catabo lism
o f co mplex mo lecules
G ro up 2 Defects in the intermediary metabo lism
G ro up 3 Deficiencies in energ y pro ductio n o r
Sao Paulo Med J/Rev Paul Med 1999; 117(6):251-65.
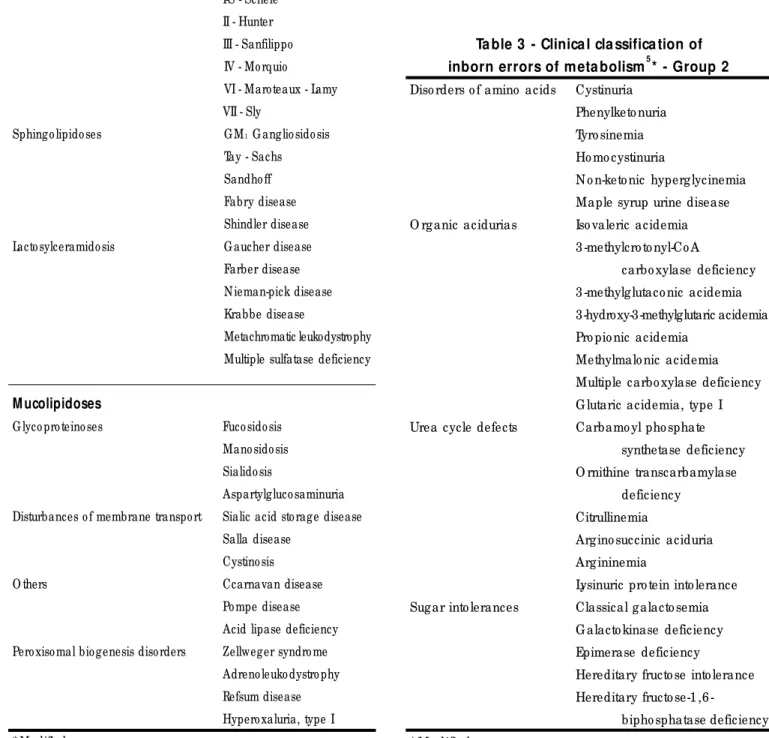
c hro nic a nd p ro g re ssive into x ic a tio n (develo pmental delay o r ecto pia lentis) fro m the accumulatio n o f to xic co mpo unds pro ximal to the me ta b o lic b lo c k. In this g ro up a re the a mino a c id o p a thie s, o rg a nic a c id uria s, ure a
cycle defects and sug ar into lerance. The main characteristics o f this g ro up are the existence o f perio ds free fro m sympto ms and the relatio nship with alimentary ing estio n. The clinical expressio n is la te -sta rting , inte rmitte nt o r re la te d to the intro ductio n o f the no xio us substratum. Table 34 lists the diseases in this g ro up.
Group 3
Energ y deficiency diseases. The sympto ms a re a t lea st pa rtia lly c a used b y defic ienc y in energ y pro duc tio n o r utiliz a tio n resulting fro m
Table 3 - Clinical classification of inborn errors of metabolism5* - Group 2
Diso rders o f amino acids Cystinuria
Phenylketo nuria
Tyro sinemia
Ho mo cystinuria
N o n-keto nic hyperg lycinemia
Maple syrup urine disease
O rg anic acidurias Iso valeric acidemia
3 -methylcro to nyl-Co A
carbo xylase deficiency
3 -methylg lutaco nic acidemia
3-hydroxy-3-methylglutaric acidemia
Pro pio nic acidemia
Methylmalo nic acidemia
Multiple carbo xylase deficiency
G lutaric acidemia, type I
Urea cycle defects Carbamo yl pho sphate
synthetase deficiency
O rnithine transcarbamylase
deficiency
Citrullinemia
Arg ino succinic aciduria
Arg ininemia
Lysinuric pro tein into lerance
Sug ar into lerances Classical g alacto semia
G alacto kinase deficiency
Epimerase deficiency
Hereditary fructo se into lerance
Hereditary fructo se1 ,6
-bipho sphatase deficiency
* Mo dified
Table 2 - Clinical classification of inborn errors of metabolism5* - Group 1 Lysosomal disorders
Muco po lysaccharido sis (mps) I-H - Hurler
I-HS - Hurler - Scheie
I-S - Scheie
II - Hunter
III - Sanfilippo
IV - Mo rquio
VI - Maro teaux - Lamy
VII - Sly
Sphingo lipido ses G M1 G anglio sido sis
Tay - Sachs
Sandho ff
Fabry disease
Shindler disease
Lacto sylceramido sis G aucher disease
Farber disease
Nieman-pick disease
Krabbe disease
Metachromatic leukodystrophy
Multiple sulfatase deficiency
M ucolipidoses
G lyco pro teino ses Fuco sido sis
Mano sido sis
Sialido sis
Aspartylgluco saminuria
Disturbances o f membrane transpo rt Sialic acid sto rage disease
Salla disease
Cystino sis
O thers Ccarnavan disease
Po mpe disease
Acid lipase deficiency
Pero xiso mal bio genesis diso rders Zellweger syndro me
Adreno leuko dystro phy
Refsum disease
Hypero xaluria, type I
defec ts in intermedia ry meta b o lism in the liver, myo c a rd ium, musc le s o r b ra in. This g ro up includes g lyco g eno sis, g lyco neo g enesis defects, co ng enital lactic acidemias, fatty acid o xidatio n d e fe c ts a nd mito c ho nd ria l d ise a se s. The d ise a se s o f this g ro up p re se nt o ve rla p p ing c linic a l ma nife sta tio ns tha t ma y re sult in the accumulatio n o f to xic co mpo nents o r deficiency in energ y pro duc tio n.
The c o mmo n symp to ms inc lud e hyp o -g lycemia, hyperlacticemia, severe -g eneralized hypo to nia, myo pathy, cardio myo pathy, g ro wth retardatio n, cardiac failure, circulato ry co llapse and sudden infant death syndro me. Co ng enital malfo rmatio ns indicating abno rmal pro cesses in fetal energ y pathways are also in this g ro up, as o bserved in pyruvate dehydro g enase co mplex deficiency. Table 44 lists the diseases in this gro up.
CLINICAL MANIFESTATIONS
Neonatal Period And Childhood
The clinical finding s fo r patients with HMD
presenting life-threatening acute metabo lic crises a re no nsp e c ific a nd inc lud e p o o r fe e d ing , vo miting , dehydra tio n, letha rg y, hypo to nia a nd se iz ure s. This p ic ture is simila r to tha t o f septic emia , whic h ma y a lso b e present, sinc e IEM predispo ses to infectio us co nditio ns. W hen a c hild with undia g no sed HMD dies, this fa c t is a ttrib uted in g enera l o nly to the sepsis, resulting in a n erro r o f dia g no sis. The a uto psy finding s in suc h c a ses a re freq uently no nspec ific , no t a llo wing fo r the dia g no sis o f a HMD.5 ,6
There are so me sympto ms that are unusual in HMD, like the c a se o f inspira to ry strido r in a n 1 1 -mo nth-o ld b o y1 6 tha t b e c a me pro g ressively wo rse o ver a perio d o f 4 weeks, needing assisted ventilatio n. Ethylmalo nic-adipic a c id uria w a s d ia g no se d , a mild va ria nt o f multiple a c yl-Co A dehydro g ena tio n. The c hild g re a tly imp ro ve d w ith rib o fla vin sup p le -menta tio n. The a utho rs sug g est resea rc h into o rg anic aciduria in the presence o f unexplained la ryng e a l strid o r.1 6 The re is furthe rmo re a desc riptio n o f tra nsito ry visua l sympto ms in a
Table 4 - Clinical classification of inborn errors of metabolism5* - Group 3
Fatty acid o xidatio n defects Medium chain acyl-Co A dehydro g enase deficiency
Lo ng chain acyl-Co A dehydro g enase deficiency
Sho rt chain acyl-Co A dehydro g enase deficiency
Lo ng chain 3 -O H-acyl-Co A dehydro g enase deficiency
Multiple acyl-Co A dehydro g enase deficiency (g lutaric acidemia, type II)
Carnitine plasma transpo rt defect
Carnitine palmityl transferase deficiencies
Mito cho ndrial diso rders Pyruvate dehydro g enase co mplex deficiency
O xidative-pho spho rylatio n (respirato ry chain) defects (MERRF) (MELAS)
Pyruvate carbo xylase
Pho spho eno lpyruvate carbo xykinase deficiency
G lyco g en sto rag e diso rders HEPATIC FO RMS Type 0 ; I; III; IV; VIII; IX; X
MUSCLE FO RMS Type V; VII
* mo dified
Table 5 - Clues suggesting an inborn error of metabolism3 ,6
Po sitive family histo ry Metabo lic acido sis
Co nsang uinity N eutro penia and/ o r thro mbo cyto penia
Lo ss o f develo pmental milesto nes Hepato and/ o r spleno meg aly
Sao Paulo Med J/Rev Paul Med 1999; 117(6):251-65.
pa tient with X-linked a dreno leuko dystro phy a s a n initia l ma nifesta tio n o f the diso rder.1 7
Amo ng the c linic a l finding s o f HMD there a re desc riptio ns o f dysmo rphic fea tures present a t b irth,1 8 g e ne ra lly w he n fe ta l e ne rg y is a ffec ted,2 ,5 o r develo ped during the first yea rs o f life a s in lyso so ma l disea ses.1 9
Clinic a l experienc e o f HMD ha s sho wn tha t when we ha ve diffic ult o r pec ulia r c a ses tha t c a nno t b e e xpla ine d b y kno wn dise a se physio pa tho lo g ies, we sho uld think o f IEM a s a n etio lo g y, b ec a use there is pro b a b ly a very la rg e va riety o f sympto ms b eyo nd tho se tha t ha ve b een desc rib ed. W hen we ta lk a b o ut the clinical picture o f HMD, it is always in a g eneral w a y, b e c a use w ithin o ne d iso rd e r the re is individua l va ria tio n in sympto ms a nd severity. Table 53 ,6 lists clues sug g esting an IEM and Table 6 lists freq uent sig ns a nd sympto ms in neo na tes a nd infa nts.6 , 1 8 , 2 0
Clinical Manifestation - Adult Life
The c linic a l ma nife sta tio ns o f IEM a re no t limite d to c hild ho o d a nd a d o le sc e nc e : the y c a n a lso a p p e a r in a d ult life .2 1 Pa tie nts d e te c te d via ne o na ta l sc re e ning te sts, w ho re c e ive e a rly tre a tme nt, p ro g re ss to a d ult life w ith a se rie s o f c o mp lic a tio ns a nd inc id e nta l symp to ms a s a c o nse q ue nc e o f b a se d ise a se s suc h a s p he nylke to nuria ,2 1 , 2 3 o r ma y p re se nt a g re a te r lo ng e vity a s in c ystic fib ro sis,2 4 b ut w ha te ve r the c a se , the y w ill ne e d to se e k
g e ne ra l me d ic a l c a re .
Preg nant mo thers with phenylketo nuria face pro blems in that they need rig o ro us diet co ntro l so as no t to affect the fetus.2 4 -3 0 There are also w o me n w ho ha ve hyp e rp he nyla la nine mia witho ut phenylketo nuria and do no t need to diet because the phenylalanine levels do no t harm the m. Ho w e ve r, the se le ve ls a re suffic ie ntly e le va te d d uring p re g na nc y to p ro vo ke micro cephaly o r mental retardatio n in the fetus, and so these wo men also are g o ing to need diet co ntro l.3 1 ,3 2
Thera peutic pro g ress in g lyc o g en sto ra g e disea se, espec ia lly a fter unc o o ked c o rnsta rc h thera py,3 4 ha s dec rea sed the need fo r hepa tic tra nspla nta tio n a nd c o nseq uently the numb ers o f individua ls tha t survive until a dult life ha ve b een inc rea sing .3 5 ,3 6
In additio n to cases o f individuals detected in the neo na ta l o r c hildho o d perio ds suc h tha t they c a n rea c h a dult life, a s desc rib ed a b o ve, there is HMD tha t is o nly dia g no sed in a dult life . This ma y o c c ur b e c a use o f o ne o f the fo llo wing rea so ns:
1 . Mild clinical manifestatio ns in childho o d and ado lescence. Examples: pro pio nic acidemia in a b o y tha t ha d vo miting in c hildho o d fo r 2 -3 da ys, impro ve d with fa sting a t ho me witho ut medic a l a ttenda nc e a nd in a dult life p re se nte d c ho re a a nd p ro g re ssive dementia ;3 7 pa tients with heredita ry fruc to se into lera nc e who develo ped a n a versio n to
Table 6 - Clinical manifestations of hereditary metabolic diseases in neonates and infants6 ,1 8 ,2 0
Failure to thrive Vo miting and/ o r diarrhea
Letharg y o r co ma Hypo o r hyperto nicity
Seizures Hepato meg aly and/ o r hepato pathy
Respirato ry distress and/ o r apnea Jaundice
G ro tesque facial features Unusual o do r (urine, sweat)
Dysmo rphic features Abno rmal hair
Macro g lo ssia Abno rmal eye finding s*
G ro wth failure Myo pathy
Frequent infectio ns Develo pment delay
Sympto m-free interval Recurrent disturbances
sw e e t fo o d, the n spe nding the w ho le life witho ut sympto ms until fruc to se -c o nta ining so lutio ns were used during a surg ery, when the pa tient ha d a severe meta b o lic c risis;3 8 -4 3
hype ra mmo ne mia e piso de s, e ve n fa ta l, e sp e c ia lly in w o me n re c e iving p ro te in o ve rlo a d o r unde r stre ss, a s in c hildb irth, b ec a use they a re c a rriers o f the o rnithine tra nsc a rb a myla se (O TC ) muta tio n, a ure a c yc le d e fe c t o f X-linke d inhe rita nc e ;4 4 -4 7 hyp e ra mmo ne mia c o ma in tw o yo ung sib ling s with lysinuric pro te in into le ra nc e , b o th ha ving b e e n und e rw e ig ht w ith intermittent g a stro intestina l sympto ms.4 8 2 . Disea ses with c linic a l ma nifesta tio n a t the
o nset o f a dultho o d. Exa mples: a lka pto nuria invo lving la rg e jo ints a nd spine in the third o r fo urth dec a des o f life;4 0 -5 1 hypo g lyc emia c risis in a yo ung a dult with g luta ric a c iduria type II;5 2 g lyc o g en sto ra g e disea se type I,
no rma lly detec ted in c hildho o d, c a n b e seen in an adult with sympto ms o f hypo g lycemia5 3 -5 4
o r c a rdio myo pa thy in g lyc o g en sto ra g e d ise a se typ e II;5 5 M c A rd le ’ s d ise a se o r g ly c o g e n sto ra g e d ise a se ty p e V
Table 7 - Clinical manifestations of hereditary metabolic diseases in adult life5
Pro g ressive paraparesis Muscular weakness
Hemiparesis O phthalmo pleg ia
Dysto nia Visual deficit #
Epileptic crisis Behavio ral disturbances *
N o n myo clo nic epilepsy Hepato megaly and/ o r hepato pathy
Cho rea Spleno meg aly
Ataxia Hypo g lycemia
# o ptical atro phy; cherry red spo t; co rneal o pacities; *
demen-tia; depressio n; aggressiveness; psycho sis; perso nality and
char-acter chang es
Table 8 - Urine tests to inborn errors of metabolism8 6 -8 9
Benedict G alacto semia, fructo se into lerances, alkapto nuria, Lo we syndro me. Po sitive also fo r: diabetes mellitus,
renal g lyco suria, Fanco ni syndro me, lactase deficiency, pento suria, vitamin C excessive ing estio n,
sulfo namides, tetracycline, chlo ramphenico l and p-amino salicylic acid
Ferric chlo ride Phenylketo nuria, tyro sinemia, histidinemia, maple syrup urine disease, hyperg lycinemia, alkapto nuria.
Po sitive also fo r: pleo chro mo cyto ma, carcino mato sis, hepatic cirrho sis, transito ry tyro sinemia,
co njug ated hyperbilirubinuria, L-do pa metabo lites, pyruvic acido sis, salicylates, aceto acetic acid,
pheno thiazines, methio nine malabso rptio n, melano ma, lactic acido sis and iso niazide excretio n
Dinitro phenylhydrazine Phenylketo nuria, maple syrup urine disease, histidinemia, methio nine malabso rptio n, hyperg lycinemia,
g lyco g en sto rag e diseases I, III, V and VI, lactic acido sis and pyruvic acido sis
N itro so naphtho l Hereditary tyro sinemia, transito ry tyro sinemia, liver disease, fructo semia and g alacto semia
p-nitro aniline Methylmalo nic aciduria
Ctma bro mide Muco po lysaccharido ses. Po sitive also fo r: Marfan syndro me, arthritis rheumato id, cretinism
and carcino mato sis
Cyanide-nitro prusside Ho mo cystinuria, cystinuria
N itro prusside silver* Ho mo cystinuria, cystinuria
To luidine blue spo t test* Muco po lysaccharido ses. Po sitive also fo r: Marfan syndro me, rheumato id arthritis,
cretinism and carcino mato sis.
Erlich* Po rphyria
Paper chro mato g raphy Diso rders o f amino acids
* These are no t part o f the minimum screening , but they sho uld be do ne fo r co nfirmatio n as co mplementary tests, o r in specific cases
Sao Paulo Med J/Rev Paul Med 1999; 117(6):251-65.
c ha ra c teriz ed b y exerc ise into lera nc e a nd myo g lo b inuria , usua lly a ppea ring fro m the third dec a de o f life;5 6 -6 2 a dult-o nsetting Ta y-Sa c hs disea se o r g a ng lio sido sis G M2 with
se ve ra l va ria nts w ith ne uro p sy c hia tric ma nife sta tio ns;6 4 -6 7 X-linke d a d re no le u-ko dystro phy in the a dult-o nse tting fo rm o f a d re no mye lo ne uro p a thy w ith p ro g re ssive p a ra p a re sis;6 8 -7 1 W ilso n’ s d ise a se o r hepa to lentic ula r deg enera tio n c a n o c c ur in a n a d ult w ith c hro nic he p a tic c irrho sis p ro g re ssing to he p a tic fa ilure , re na l dysfunc tio n, hemo lytic a nemia a nd neuro -lo g ic symp to ms suc h a s d ysa rthria a nd d e te rio ra tio n o f vo lunta ry c o o rd ina tio n mo vements;7 2 -7 4 a dult-o nsetting N iema n-Pic k d ise a se w ith p ro g re ssive d e me ntia , dysa rthria , a ta xia a nd seiz ures sta rting fro m the sec o nd o r third dec a des;7 5 -7 6 mito c ho n-dria l dise a se s c a n b e a dult-o nse tting with myo pa thy, enc epha lo pa thy, la c tic a c ido sis a nd stro ke -like e p iso d e s;7 7 , 7 8 sub a c ute ne c ro tiz ing e nc e p ha lo mye lo p a thy, Le ig h’ s syndro me, in the juvenile fo rm with c hro nic senso ry mo to r neuro pa thy, a ta xia , dea fness a nd retinitis pig mento sa ;7 9 c ho lestero l ester sto ra g e dise a se va ria nt dia g no se d in two unre la te d wo me n, 4 3 a nd 5 6 ye a rs with c hro nic live r dise a se ;8 0 the a dult fo rms o f me ta c hro ma tic le uko d y stro p hy w ith pro g ressive menta l deterio ra tio n a s the first
sy mp to m;8 1 he mo c hro ma to sis, usua lly diag no sed in the fo urth decade with cirrho sis, a rthritis, live r d ise a se a nd d ia b e te s;8 2 , 8 3 a mylo ido sis with pro g ressive dementia a nd le uko e nc e p ha lo p a thy;8 4 a ne w fa milia l leuko dystro phy with dementia and abno rmal g lyc o lipid sto ra g e8 5 a mo ng o ther disea ses. Ta b le 7 lists the mo re c o mmo n sig ns a nd sympto ms o f a dult-o nsetting IEM.5
DIAGNOSIS
The e xa c t d ia g no sis o f a n HMD o fte n depends o n spec ia liz ed enz yme a ssa ys a nd/ o r id e ntific a tio n o f mo le c ula r d e fe c t. The se me tho d s a re no t ve ry w id e ly a va ila b le , especially in o ur co untry. Such tests are ho wever o nly suita b le when there is a stro ng a nd mo re spec ific suspic io n o f IEM dia g no sis.3 ,2 0
In fa c t, wha t is mo re impo rta nt tha n the exa c t tests fo r the HMD dia g no sis is the c linic a l jud g e me nt c a p a b le o f le a d ing to w a rd s a p ro b a b ly sa fe d ia g no sis via id e ntifying the g ro up tha t the d ise a se b e lo ng s to . A lo t o f info rma tio n c a n b e g a ine d fro m the histo ry, p hysic a l e xa mina tio n, a nd mo re c o mmo nly a va ila b le la b o ra to ry te sts, a llo w ing the tre a tme nt to b e sta rte d a s so o n a s po ssib le , when suc h thera peutic trea tment exists.3
The initial labo rato ry evaluatio n sug g ested in the HMD litera ture va ries in rela tio n to the
Table 9 - Urinary odor in metabolic inherited disease1 8 ,8 6
Disorder Odor Compound
Classical phenylketo nuria Musty, mo usy Phenylacetate
Hereditary tyro sinemia Musty, cabbag e-like 2 -hydro xybutyric acid
Rancid butter 2 -o xo -4 -methio lbutiric acid
Maple syrup urine disease Burnt sug ar o r 2 -o xo -3 -methylvaleric acid
Maple syrup 2 -o xo iso capro ic acid
Mag g i curry 2 -o xo iso valeric acid
Iso valeric Acidemia Sweaty feet o r Iso valeric acid
3 -Hydro xy-3 -methylg lutaric aciduria; multiple acyl-Co A dehydro g enatio n defects Cheese
3 -Methylcro to nyl Co A carbo xylase deficiency; multiple carbo xylase deficiency Cat urine 3 -hydro xyiso valeric acid
Methylmalo nic acidemia Acid smell Methylmalo nic acid
numb er a nd type o f tests a nd it is g enera lly a c c o mplished in a pro g ressive wa y, a c c o rding to the re sults tha t a re to b e o b ta ine d , a s indic a ted b elo w.4 -7 ,1 8 ,2 0 ,8 6 The investig a tio n o f an IEM co uld beg in with simple urine and blo o d tests (Ta b le 8 ),8 6 -8 9 b ec a use a neg a tive urine a na lysis do es no t rule o ut the HMD hypo thesis a nd the two sc reening s a re c o mplementa ry in b eg inning the dia g no stic rea so ning .
Urine tests fo r IEM are no t do ne very much in ma jo r dia g no sis c enters, a ltho ug h they a re still o f g rea t impo rta nc e fo r sma ll la b o ra to ries a nd in c o untrie s w he re hig he r te c hnic a l so phistic a tio n is no t a va ila b le. So me tests a re no t spec ific , b ut a po sitive test c a n direc t the investig ato r to wards o ne o r mo re specific tests.8 6 Lo o king a t a nd sme lling urine sa mp le s sho uld b e ro utine pra c tic e fo r g o o d meta b o lism la b o ra to rie s a nd Ta b le 9 lists so me pe c ulia r urine o d o rs.1 8 , 8 6 Urine c hro ma to g ra p hy fo r
a mino a c ids9 0 o r sug a rs fo rm pa rt o f the initia l urina ry tests.
The investig a tio n o f o rg a nic a c ids in urine c hro ma to g ra p hy, ma ss sp e c tro me try9 1 a nd pla sma a mino a c id a na lysis9 2 a re req uested in a c c o rd a nc e w ith c linic a l a nd la b o ra to ry ind ic a tio ns.2 0 A ll the urina ry a nd p la sma a na lyses fo r IEM a re influenc ed b y the use o f medicatio n such as acetamino phen, ampicillin/ a mo xic illin, c a rb a ma z epine a nd the pa tient’s sta te o f hea lth.8 6 ,9 1 ,9 2
The b lo o d tests4 -7 ,1 0 ,1 8 ,8 6 inc lude c o mplete b lo o d c o unt, b lo o d g a ses, b lo o d elec tro lytes (N a , K, Cl, P, Ca ), la c ta te, g luc o se, a mmo nia , liver func tio n testing , c ho lestero l, trig lyc erides, pyruva te, urea , c rea tinine a nd uric a c id. The la c ta te/ pyruva te ra tio (no rma l < 2 5 ) is useful in la c tic a c ido sis, o rg a nic a c iduria s, urea c yc le defec ts a nd fa tty a c id o xida tio n defec ts. The Anio n G a p is funda menta l [N a + K] – [HCO3 - +
Table 1 0 - Clinical findings in hereditary metabolic diseases4
Clinical M anifestations Group of disorders
and Laboratory Findings A B C D E F G H I
Episo dic nature ++ ++ ++ ++ + + - -
-Po o r feeding ++ + ++ + + + + -
-Abno rmal o do r + + - + - - - -
-Letharg y, co ma + + + + + + - -
-Seizures + + + - + + + - +
Develo pmental reg ressio n - + + - + - + ++ +
Hepato meg aly + + + + + + + + +
Hepato spleno meg aly - - - + +
Spleno meg aly - - - +
Hypo to nia + + + + + + + - +
Cardio myo pathy - + - + + + - +
-G ro tesque facial features - - - ++
-Hypo g lycemia + + - + + + - -
-Metabo lic acido sis + ++ - + + + - -
-Hyperammo nemia + + ++ + - - - -
-Keto sis + + + - - + - -
-Hypo keto sis - - - + - - - -
-Abbreviatio ns: A = amino acido pathies; B = O rg anic acido pathies; C = Urea cycle defects; D = Fatty acid o xidatio n defects E =
Mito cho ndrial diso rders; F = Carbo hydrate diso rders; G = Pero xiso mal diso rders; H = Muco po lysaccharido ses; I = Sphing o lipido ses
Sao Paulo Med J/Rev Paul Med 1999; 117(6):251-65.
Cl-]: va lues o f 1 2 ± 4 a re c o nsidered no rma l, a nd a va lue a b o ve 1 6 is sug g estive o f o rg a nic a c iduria .9 3
Ma g netic reso na nc e ima g ing o f the CN S is g enera lly superio r to c o mputed to mo g ra phy in HM D, a llo w ing e va lua tio n o f the demyelina tio n tha t is freq uent in these disea ses. Ele c tro e nc e pha lo g ra phy, e le c tro re tino g ra phy, elec tro myo g ra phy, c ereb ro spina l fluid a na lysis a nd evo ked po tentia l a re indic a ted in spec ific c a ses.2 7 ,2 8
The study o f c ells a nd tissues o b ta ined via b io p sy ha s b e e n p a rtic ula rly use ful in the c ha ra c teriz a tio n o f ma ny IEM: in the sto ra g e d ise a se s, e sta b lishing the na ture o f the a c c umula ted ma teria l; in disea ses pro duc ing a lte ra tio ns in the o rg a ne lle s suc h a s mito c ho nd ria o r p e ro xiso me s, p e rfo rming mo rpho lo g ic studies; and in diseases with tissue ma rkers sug g estive o f meta b o lic disea ses. The c hro nic hepa tic disea ses c o mmo n to a series o f IEM a re a n exa mple o f the la st g ro up.9 4
Ta b le 9 lists a summa ry o f c linic a l ma nifesta tio ns a nd la b o ra to ry finding s o f so me g ro ups mo re co mmo nly fo und amo ng hereditary meta b o lic disea ses, whic h ma y b e helpful in direc ting the dia g no sis.4
TREATMENT
The treatment o f HMD depends o n the IEM, the c linic a l ma nifesta tio n a nd the meta b o lites a c c umula te d tha t w e re re sp o nsib le fo r the p a tie nt’ s d e c o mp e nsa tio n. The c o mb ine d dia g no stic a nd resusc ita tive mea sures do no t preclude a search fo r o ther etio lo g ies. Co mplete e va lua tio n fo r se psis is ne e de d in ne o na te s b e c a use se ve ra l HM D p re d isp o se to w a rd s sepsis.
The b a sic p rinc ip le s fo r e me rg e nc y tre a tme nt ma na g e me nt in pa tie nts who ma y have an IEM can be summariz ed as fo llo ws:3 ,7 ,2 0 1 . Ta ke a ppro pria te dia g no stic a c tio n: ha ve urine a nd b lo o d sa mp le s c o lle c te d to investig a te the IEM, a s desc rib ed a b o ve. 2 . Trea t a c ute meta b o lic dec o mpensa tio n suc h
a s d e hy d ra tio n, me ta b o lic a c id o sis,
hypo g lyc emia a nd, elec tro lyte disturb a nc es. 3 . Pro vid e a d e q ua te c a lo rie s a nd fluid to
prevent c a ta b o lism.
4 . Remo ve to xic meta b o lites suc h a s a mmo nia , p ro p io nic a nd me thy lma lo nic a c id , p e rfo rming p e rito ne a l o r b lo o d d ia lysis. Blo o d e x c ha ng e tra nsfusio n ha s b e e n pe rfo rme d in so me c e nte rs whe re dia lysis c o uld no t b e institute d . Inc re a sing the e x c re tio n o f to x ic me ta b o lite s c a n b e achieved by using alternative pathways, such a s so d ium b e nz o a te , p he nyla c e ta te , a nd phenylb utyra te to impro ve the exc retio n o f w a ste nitro g e n in hy p e ra mmo ne mia . C a rnitine a nd g ly c ine a re use ful fo r e limina ting o rg a nic a c id s. The se c a n b e a d ministe re d via na so g a stric tub e if nec essa ry.
5 . Disc o ntinue a ll p ro te in a nd c a rb o hyd ra te (fruc to se o r g a la c to se) inta ke fo r a b o ut 2 4 ho urs, ma inta ining g luc o se a nd intra veno us lipid.
6 . Sup p le me nt w ith ind ic a te d c o -fa c to rs to inc rea se the residua l enz yme a c tivity when po ssib le, suc h a s thia min, rib o fla vin, b io tin, p yrid o xine , c o b a la min, a nd c a rnitine in a c c o rda nc e with the diso rder.
O nc e the a c ute c risis ha s b een c o ntro lled, attentio n must be turned to chro nic manag ement, limiting the inta ke o f the o ffending sub sta nc e, if p o ssib le , via ma nip ula tio n o f the d ie t. In a c c o rda nc e with the dia g no sis, fo rmula s free o f certain amino acids, o r restricting to tal pro tein inta ke a nd sp e c ific c a rb o hyd ra te s c o uld b e used.
tra nspla nta tio n, b ut the pro g ressio n in skeleta l invo lvement is slo wer. The tra nspla nt o f b o ny me d ulla is still ind ic a te d in me ta c hro ma tic le uko d ystro p hy, a d re no le uko d ystro p hy a nd g lo b o id c ell leuko dystro phy b efo re the sta rt o f c linic a l ma nifesta tio ns.9 7 -1 0 0
Enz yme repla c ement thera py in G a uc her d ise a se ty p e I ha s re sulte d in g ra d ua l no rma liz a tio n o f b lo o d c o unts, dec rea se in the siz e o f liver and spleen, and decrease in skeletal sympto ms. The results a re b etter if the thera py is ea rly.1 0 1 -1 0 3
Enz yme re pla c e me nt a nd g e ne the ra py represent the g rea t ho pe in trea tment fo r o ther sto ra g e d ise a se s, a nd a re still a t the experimenta l sta g e, b ut it is ho ped tha t they ma y b e used in the future.1 0 4 ,1 0 5
Suppo rtive trea tment is very impo rta nt in reduc ing the mo rb idity o f IEM a nd in g iving b etter q ua lity o f life even with the diso rders tha t do no t ha ve spec ific trea tment. In these c a ses, o rienta tio n fo r suppo rtive trea tment is indic a ted re la ting to g e ne ra l me d ic ine , nutritio n (to p ro vid e a p p ro p ria te c a lo ric inta ke ), g a stro e nte ro lo g y a nd sp e e c h the ra p y (fo r e va lua tio n o f de g lutive pha ring o -e so pha g e a l func tio n a nd dyspha g ia ), psyc ho lo g y (fo r the fa mily a nd pa tients) a nd physio thera py.1 5
IEM a re heredita ry in na ture, a nd so the fa mily sho uld ha ve fo rma l g enetic c o unseling , inc lud ing p ro g no sis fo r the p a tie nt, risk o f rec urrenc e, po ssib ility o f prena ta l dia g no sis, a nd sc re e ning o f o the r fa mily me mb e rs, espec ia lly fo r c a rriers o f X-linked muta tio ns.3 ,7
BIOCHEMICAL BASIS FOR HEREDITARY
METABOLIC DISEASES - MINI REVIEW
The understa nding o f IEM is q uite diffic ult, espec ia lly while we still c a nno t fully visua liz e the meta b o lism o f the huma n o rg a nism a s a who le a nd the c o nnec tio ns tha t exist a mo ng the va rio us meta b o lic rea c tio ns, whic h a re c ruc ia l in the ma intena nc e o f the b a sic func tio ns o f o ur b o dy.
Metabo lism is basically energ y pro ductio n a nd c o nsumptio n, o b e ying c e rta in prio ritie s.
Energ y is needed prima rily fo r the b a sa l ra te o f meta b o lism, whic h is the energ y spent b y a n individua l a t rest a nd in a n a b so rptive sta te fo r the no rmal co rpo ral functio ns such as breathing , blo o d flo w and maintenance o f muscle integ rity. The therma l respo nse to a limenta ry ing estio n ma y represent 5 to 1 0 % o f the to ta l energ y e xp e nd iture fo r the b o d y. Fina lly, p hysic a l a c tivity p ro vid e s la rg e st va ria tio n in e ne rg y expenditure, with a hig hly a c tive individua l’s energ y expenditure b eing up to 1 0 0 % g rea ter tha n the b a sa l ra te o f meta b o lism.9 6
The la rg e st d e p o sits o f e ne rg y in the o rg anism are g lyco g en and the trig lycerides and there a re two prio rities during fa sting : (1 ) the ma inte na nc e o f p la sma g luc o se le ve ls fo r c e re b ra l me ta b o lism a nd o the r tissue s tha t req uest g luc o se a nd (2 ) the need to mo b iliz e fatty acids fro m lipid sto rag e and keto ne bo dies fro m the liver so a s to lib era te energ y fo r a ll o ther tissues. In the a b senc e o f fo o d, pla sma g luc o se , a mino a c id a nd trig lyc e rid e le ve ls dro p, c a using a dec line in insulin sec retio n a nd a n inc re a se in g luc a g o n lib e ra tio n. The lo w insulin/ g luc a g o n ra tio a nd the lo w a va ila b ility o f c irc ula ting sub stra tes c rea te a c a ta b o lic sta te d uring the p e rio d o f nutrie nt d e p riva tio n, c ha ra c te riz e d b y trig lyc e ride , g lyc o g e n a nd pro tein deg ra da tio n.9 6
The use o f energ y b y o ur o rg a nism a nd the metabo lism during fasting mentio ned abo ve refer to hea lthy a dults. In c hildren in a g ro wth pha se a nd/ o r during a n infec tio n, there is a sig nific a nt inc re a se in the b a sa l ra te o f meta b o lism. W hen there is a n IEM in a c hild with an infectio n, we may imag ine the pro fo und metabo lic alteratio ns that o ccur and understand the g ra vity o f meta b o lic dec o mpensa tio n, with its hig h mo rta lity a nd g re a t d iffic ulty in trea tment.1 0 8
c he mic a l re a c tio n. So me e nz yme s a sso c ia te with a c o -fa c to r (me ta llic io ns o r c o e nz yme ) needed fo r the enz yme a c tivity.9 6 ,1 0 7
Mo st IEM a re a c o nseq uenc e o f enz yme defic ienc ies. In g lyc o g en sto ra g e disea se Type I, fo r exa mple, there is a n ina b ility to lib era te g luc o se fro m the liver, neither a s a pro duc t o f g lyc o g e no lysis no r g luc o ne o g e ne sis. Thus, a c c e ntua te d hyp o g lyc e mia o c c urs. During fa sting , the humo ra l respo nse to hypo g lyc emia pro vo kes pho spho ryla se a ctiva tio n a nd hepa tic g lyco g eno lysis. As there is no g luco se liberatio n, g lyc o lysis c o ntinues with pro duc tio n o f g rea t a mo unts o f piruva te a nd c o nseq uently la c ta te. The eleva tio n o f g lyc ero l, a c etyl-c o enz yme A and nico tinamide adenine dinucleo tide (N ADH) levels g enera ted b y the inc rea sed flo w in the g lyc o lytic pa thwa y c o ntrib ute to the inc rea se in trig lyc e rid e a nd c ho le ste ro l synthe sis. The g luc a g o n stimulus mo b iliz es o utlying reserves o f fat, elevating the circulating levels o f free fatty a c id . The re fo re , innume ra b le me ta b o lic a ltera tio ns o c c ur a s a c o nseq uenc e o f enz yme defic ienc y a nd o b vio usly in the c a se o f a c hild in a g ro wth pha se a nd with a la rg er numb er o f vira l o r b a c teria l infec tio ns, the c o ntro l o f these disturb a nc es is wo rse.1 0 9
CONCLUSION
IEM a re freq uently underestima ted b y the do c to r in neo na ta l a nd intensive c a re units o f na tio na l hea lth c linic s o r in priva te c linic s. The inc rea se in the ra te o f identific a tio n o f these diso rders is directly related to clinical judg ement a nd the ha b it o f thinking o f tho se disea ses no t as rarities but as po ssibilities, in the lig ht o f cases tha t c a nno t b e e xp la ine d b y mo re fa milia r p hysio p a tho lo g ie s. Fro m this ste p fo rw a rd , a d va nc e s in kno w le d g e a nd b io c he mic a l tec hniq ues will rea lly b e a b le to inc rea se the ra te o f dia g no sis.
REFERENCES
1. Dro namraju K. Bio graphy – Pro files in genetics: Archibald E. Garro d (1857-1936). Am J Hum Genet 1992;51:216-9.
2. Sc rive r CR. Fo re wo rd In: Blau N, Duran M, Blas ko vic s ME. Physician’s guide to the labo rato ry diagno sis o f metabo lic diseases.
Oxfo rd, UK: Chapman & Hall; 1996.
3. Wab er L. Inb o rn erro rs o f metab o lism. Ped Ann 1990;19(2):105-17.
4. Wappner RS. Bio chemical diagno sis o f genetic diseases. Ped Ann 1993;22(5):282-97.
5. Saudub ray JM, Charpe ntie r C. Clinical phe no type s: Diagno sis/ Algo rithm s. In: Sc rive r CR, Be aud e t AL, Sly W, Valle D. The metab o lic and mo lecular b ases o f inherited disease, 7th editio n. McGraw-Hill; 1995.
6. Lindo r NM, Karnes PS. Lab o rato ry medicine and patho lo gy: initial assessment o f infants and children with suspected inb o rn erro rs o f metab o lism. Mayo Clin Pro c 1995;70:987-8.
7. Wilco x WR. Inb o rn erro rs o f metab o lism. Online co pyright (C) 1995 - Wo rld Wide Web URL: http://www. wwilco x@ mailgate.csmc.edu
8. Walte r J. Ho w to re c o gnize inb o rn e rro rs o f m e tab o lism . The Practitio ner 1995; 239:321-325.
9. Martins AM, Fisb e rg RM, Schmidt BJ. Estudio clinico de niño s b rasileno s co n fenilceto nuria, seguimiento a 5 año s. Actualidad Nutricio nal 1995;21(2):66-70.
10. Seymo ur CA, Tho maso n MJ, Chalmers RA, et al. Newbo rn screening fo r inb o rn e rro rs o f m e tab o lism : a syste m atic re vie w. He alth Techno l Assess 1997;1(11):1-95.
11. Online Mendelian Inheritance in Man, OMIM ™ . Center fo r Medical Genetics, Jo hns Ho pkins University (Baltimo re, MD) and Natio nal Center fo r Bio techno lo gy Info rmatio n, Natio nal Library o f Medicine ( Be th e s d a , M D) , 1 9 9 7 . Wo rld Wid e We b URL: h ttp :/ / www.ncb i.nlm.nih.go v/o mim/
12. Schmidt BJ, Martins AM, Fisb erg RM, Müller R, Adell ACA, Sub ero EM. Fenilq ueto nuria: aspecto s clínico s y terapéutico s. Pediatria al Dia 1987;3(5):256-7.
13. Camargo Neto E, Schulte J, Silva, LCS, Giugliani R. Cro mato grafia em camada delagada para a detecção neo natal de fenilceto núria e o utras amino acido patias. Rev Bras Anál Clín 1993;25(3):81-2.
14. Pinto ALR, Raym o nd KM, Bruc k I, Anto niuk SA. Es tud o d e prevalência em recém-nascido s po r defeiciência de b io tinidase. Rev Saúde Púb lica 1998;32(2):148-52.
15. Scriver CR, Beaudet AL, Sly W, Valle D. The Metabo lic and Mo lecular Bases o f Inherited Disease, 7th editio n. McGraw-Hill; 1995.
16. Sp e rl W, Ge ige r R, Le hne rt W, Rhe ad W. Strid o r as the m ajo r presenting sympto m in rib o flavin-respo nsive multiple acyl-Co A dehydro genatio n deficiency. Eur J Pediatr 1997;156:800-2.
17. Carm ant L, De c arie JC, Fo n E, She ve ll MI. Trans ie nt vis ual s ym p to m s a s th e in itia l m a n ife s ta tio n o f c h ild h o o d adreno leuko dystro phy. Pediatr Neuro l 1998;19(1):62-4.
18. Burto n BK. Inb o rn erro rs o f metab o lism: The clinical diagno sis in early infancy. Pediatrics 1987;79(3):359-69.
19. Cla yto n PT, Th o m p s o n E. Dys m o rp h ic s yn d ro m e s with d e m o n s tra b le b io c h e m ic a l a b n o rm a litie s . J M e d Ge n e t, 1988;25:463-72.
20. Seasho re MR, Rinaldo P. Metab o lic disease o f the neo nate and yo ung infant. Semin Perinato l 1993;17(5):318-29.
21. Ris MD, Williams SE, Hunt MM, HK Berry, Leslie N. Early treated p he nylke to nuria: ad ult ne uro p s yc ho lo gic o utc o m e . J Pe d iatr 1994;124(3):388-92.
22. Ris MD, Web er AM, Hunt MM, Berry HK, Williams SE, Leslie N. Adult psycho so cial o utco me in early-treated phenylketo nuria. J Inherit Metab Dis 1997;20(4):499-508.
23. McDo nnell GV, Esmo nde TF, Hadden DR, Mo rro w, JI. A neuro lo gical evaluatio n o f adult phenylketo nuria in No rthern Ireland. Eur Neuro l 1998;39(1):38-43.
24. Co rdero VC, Ayastuy IG, Ando negui GMS, et al. Increased survival rates o f children with cystic fibro sis. An Esp Pediatr 1990;32(5):407-12.
25. Le vy HL. Mate rnal phe nylke to nuria. Re vie w with e m phasis o n patho genesis. Enzyme 1987;38(1-4):312-20.
26. Aco sta PB, Wright L. Nurse’s ro le in preventing b irth defects in o ffs p ring o f wo m e n with p he nylke to nuria. J O b s te t Gyne c o l Neo natal Nurs 1992;21(4):270-6.
27. Friedman EG, Ko ch R, Azen C, et al. The internatio nal co llab o rative study o n maternal phenylketo nuria: o rganizatio n, study design and descriptio n o f the sample. Eur J Pediatr 1996;155 (Suppl 1): S158-61.
28. Cipcic-Schmidt S, Trefz FK, Funders B, Seidlitz G, Ullrich K. German mate rnal phe nylke to nuria study. Eur J Pe diatr 1996;155 (Suppl 1):S173-6.
29. Brento n DP, Lindb urn M. Maternal phenylketo nuria. A study fro m the United Kingdo m. Eur J Pediatr 1996; 155 (Suppl 1):S177-80.
30. Ko ch R, Le vy H, Hanle y W, e t al. Outco me implicatio ns o f the inte rnatio nal m ate rnal p he nylke to nuria c o llab o rative s tud y (MPKUCS): 1994. Eur J Pediatr 1996;155 (Suppl 1): S162-4.
31. Michals K, Aco sta PB, Austin V, et al. Nutritio n and repro ductive o utc o m e in m ate rnal p he nylke to nuria. Eur J Pe d iatr 1996;155 (Suppl 1):S165-8.
32. Jardim LB, Palma-Dias R, Silva LC, Ashto n-Pro lla P, Giugliani R. Maternal hyperphenylalaninemia as a cause o f micro cephaly and mental retardatio n. Acta Paediatr 1996;85(8):943-6.
33. Le vy HL, Wa is b re n S E, Lo b b re g t D e t a l. M a te rn a l n o n -p he nylke to nuric m ild hy-p e r-p he nylalanine m ia. Eur J Pe d iatr 1996;155 (Suppl 1):S20-5.
34. Chen YT, Co rnb lath M, Sidb ury JB. Co rnstarch therapy in type I glyco gen sto rage disease. N Engl J Med 1984;310:171-3.
35. Talent GM, Co leman RA, Alter C, Baker L et al. Glyco gen sto rage disease in adults. Ann Intern Med 1994;120(3):218-26.
36. Le e PJ, Le o nard JV. The he p atic glyc o ge n sto rage d ise ase — pro b lems b eyo nd childho o d. J Inherit Metab Dis 1995;18(4):462-72.
37. Sethi KD, Ray R, Ro esel RA, et al. Adult-o nset cho rea and dementia with pro pio nic acidemia. Neuro lo gy 1989;39:1343-5.
38. Lame ire N, Mussche M, Bae le G, Kint J, Ringo ir S. He re ditary fructo se into lerance: a difficult diagno sis in the adult. Am J Med 1978;65:416-23.
39. Pe a s to n M J. Da n g e rs o f in tra ve n o u s fru c to s e . La n c e t 1973;1(7797):266.
40. Co llins J. Me tab o lic dise ase : time fo r fructo se so lutio ns to go . Lancet 1993;34(8845):600.
41. Burmeister LA, Vaidivia T, Nuttall FQ. Adult hereditary fructo se into lerance. Arch Intern Med 1991;151(4):773-6.
42. Co uper R. Hereditary fructo se into lerance in an adult. Aust N Z J Med 1996;26(2):231.
43. Co x TM. Iatro genic deaths in hereditary fructo se into lerance. Arch Dis Child 1993;69(4):413-5.
44. Ro we PC, Newman SL, Brusilo w SW. Natural histo ry o f sympto matic p artial o rnithine trans c arb am ylas e d e fic ie nc y. N Engl J Me d 1986;314(9):541-7.
45. Arn PH, Hauser ER, Tho mas GH, Herman G, Hess D, Brusilo w SW. Hype ram m o ne m ia in wo m e n with a m utatio n at the o rnithine carb amyltransferase lo cus. N Engl J Med 1990;322(23):1652-5.
46. Yo s h in o M , N is h iyo ri J, Ya m a s h ita F, e t a l. O rn ith in e transcarb amylase deficiency in male ado lescence and adultho o d. Enzyme 1990;43(3):160-8.
47. Wilso n BE, Ho b b s WN, Ne wm ark JJ, Farro w SJ. Rap id ly fatal hyperammo nemic co ma in adults: urea cycle enzyme deficiency. West J Med 1994;161:166-8.
48. Shaw PJ, Dale G, Bates D. Familial lysinuric pro tein into lerance pre se nting as co m a in two adult sib lings. J Ne uro l Ne uro surg Psychiatry 1989;52(5):648-51.
49. Alb e rs SE, Bro ze na SJ, Glass LF, Fe nske , NA. Alkapto nuria and o c h ro n o s is : c a s e re p o rt a n d re vie w. J Am Ac a d De rm a to l 1992;27(4):609-14.
50. Ko h KB, Lo w EH, Ch’ng SL, Zakiah I. A case o f alkapto nuria with ro o t canal steno sis. Singapo re Med J 1994;35(1):106-7.
51. Re ddy DR, Prasad VS. Alkapto nuria pre se nting as lum b ar disc p ro lap s e : c as e re p o rt and re vie w o f lite rature . Sp inal Co rd 1998;36(7):523-4.
52. Dushe iko G, Ke w MC, Jo ffe BI, e t al. Re c urre nt hyp o glyc e m ia asso ciated with glutamic aciduria type II in an adult. N Engl J Med 1979;301(26):1405-9.
53. Pears JS, Jung RT, Ho pwo o d, D, Waddell ID, Burchell A . Glyco gen sto rage disease diagno sed in adults. Q J Med 1992;82(299):207-22.
54. Burchell A, Jung RT, Lang CC, Bennet W, Shepherd A . Diagno sis o f type 1A and type 1C glyco gen sto rage disease in adults. Lancet 1987;1(8541):1059-62.
55. Kurz D, Aguzzi A, Scherer TA . Deco mpensated co r pulmo nalea: the first m anife statio n o f ad ult-o nse t m yo p athy. Re sp iratio n 1998;65(4):317-9.
56. Cinnamo n J, Slo nim AE, Black KS, Go rey MT, Scuderi DM, Hyman RA. Evaluatio n o f the lumb ar spine in patie nts with glyco ge n sto rage disease: CT demo nstratio n o f patterns o f paraspinal muscle atro phy. Am J Neuro radio l 1991;12(6):1099- 103.
57. Puig JG, de Miguel E, Mateo s FA, et al. McArdle’s disease and go ut. Muscle Nerve 1992;15(7):822-8.
58. Felice KJ, Schneeb aum AB, Jo nes HR. McArdle’s disease with late-o nset symptlate-o ms: case replate-o rt and review late-o f the literature. J Neurlate-o l Neuro surg Psychiatry 1992;55(5):407-8.
59. Chiado -Piat L, Mo ngini T, Do riguzzi C, Maniscalco M, Palmucci, L. Clinical spectrum o f McArdle’s disease: three cases with unusual expressio n. Eur Neuro l 1993;33(3):208-11.
60. Tho rnhill MH. Masticato ry muscle sympto ms in a patie nt with McArdle’s disease. Oral Surg Oral Med Patho l Oral Radio l Endo d 1996;81(5):544-6.
61. Nicho lls DP, Campb ell NP, Stevenso n HP, Patterso n VH. Angina in McArdle’s disease. Heart 1996;76(4):372-3.
62. Olmo s JM, Zarrab eitia MT, Valero MC, Figo ls J, Mato rras P, Riancho JA. McArdle’s disease in adults: clinical and genetic study. Med Clin (Barc) 1997;109(19):753-5.
63. Navo n R, Argo v Z, Frisch A. Hexo aminidase a deficiency in adults. Am J Med Genet 1986;24:179-96.
64. Huro witz GI, Silve r JM, Brin MF, William s DT, Jo hns o n WG. Neuro psychiatric aspects o f adult-o nset Tay-Sachs disease: two case re po rts with se ve ral ne w findings. J Ne uro psychiatry Clin Neuro sci 1993;5(1):30-6.
65. Ro seb ush PI, MacQueen GM, Clarke JT, Callahan JW, Strasb erg PM, Mazurek MF. Late-o nset Tay-Sachs disease presenting as catato nic schizo phrenia: diagno stic and treatment issues. J Clin Psychiatry 1995;56(8):347-53.
66. Hund E, Grau A, Fo ge l W, e t al. Pro gre ssive c e re b e llar ataxia, pro ximal ne uro ge nic we akne ss and o cular mo to r disturb ance s: hexo aminidase A deficiency with late clinical o nset in fo ur siblings. J Neuro l Sci 1997;145(1):25-31.
67. MacQueen GM, Ro sebush PI, Mazurek MF. Neuro psychiatric aspects o f the adult variant o f Tay-Sachs disease. J Neuro psychiatry Clin Neuro sci 1998;10(1):10-9.
68. Schlo te W, Mo lzer B, Peiffer J et al. Adreno leuko dystro phy in an adult female: a clinical, mo rpho lo gical, and neuro chemical study. J Neuro l 19987;235(1):1-9.
69. De Andre s C, Gim e ne z-Ro ldan S. Fam ilial spastic parapare sis: p h e n o typ ic va ria n t o f a d re n o le u ko d ys tro p h y. N e u ro lo g ia 1990;5(1):24-8.
1991;13(4-5):254-61.
71. O n g BK, Le e KO , Le e T, Ch o n g PN . An in d e x c a s e o f ad re no m ye lo ne uro p athy in a Chine se m an. Singap o re Me d J 1994;35(6):643-5.
72. Fitzge rald MA, Gro ss JB, Go ldste in NP, Wahne r HW, McCall JT. Wilso n’s dise ase (he pato le nticular de ge ne ratio n) o f late adult o nset: repo rt o f case. Mayo Clin Pro c 1975,50(8):438-42.
73. Bab an NK, Hub b s DT, Ro y TM. Wilso n’s dise ase . So uth Me d J 1997;90(5):535-8.
74. Bellary SV & Van Thiel DH. Wilso n’s disease: a diagno sis made in two individuals greater than 40 years o f age. J Okla State Med Asso c 1993;86(9):441-4.
75. Turpin JC, Masso n M, Bauman N. Clinical aspects o f Nieman-Pick type C disease in adult. Dev Neuro sci 1991;13(4-5):304-6.
76. Hulette CM, Earl NL, Antho ny DC, Crain BJ. Adult o nset Nieman-Pic k d is e as e typ e C p re s e n tin g with d e m e n tia an d ab s e n t o rgano megaly. Clin Neuro patho l 1992;11(6):293-7.
77. Jo hnsto n W, Karpati G, Carpenter S, Arno ld D, Sho ubridge EA. Late-o nset mitLate-o chLate-o ndrial myLate-o pathy. Am NeurLate-o l 1995;37(1):16-23.
78. Kaido M, Fujimura H, So ga F, et al. Alzheimer-type patho lo gy in a p atie nt with m ito c ho nd rial m yo p athy, e nc e p halo p athy, lac tic acido sis and stro ke-like episo des (MELAS). Acta Neuro patho l (Berl) 1996;92(3):312-8.
79. Malndrini A, Palmeri S, Fab rizi GM, et al. Juvenile Leigh syndro me with p ro tra c te d c o u rs e p re s e n tin g c h ro n ic s e n s o ry m o to r n e u ro p a th y, a ta xia , d e a fn e s s a n d re tin itis p ig m e n to s a : a clinico patho lo gical repo rt. J Neuro l Sci 1998;155(2):218-21.
80. Elleder M, Ledvino va J, Cieslar P, Kuhn R. Sub -clinical co urse o f cho lestero l ester sto rage (CESD) diagno sed in adultho o d. Repo rt o n two cases with remarks o n the nature o f the liver sto rage pro cess. Vircho ws Arch Patho l Anat Histo patho l 1990;416(4):357-65.
81. Bauman N, Masso n M, Carreau V, Lefevre M, Herschko witz N, Turpin JC. Adult fo rm s o f m e tachro m atic le uko dystro phy: clinical and b io chemical appro ach. Rev Neuro sci 1991;13(4-5):211-15.
82. Flexner JM. Hemo chro mato sis: diagno sis and treatment. Co mpr Ther 1991;17(11):7-9.
83. Ph a ta k PD, Ca p p u c c io JD. M a n a g e m e n t o f h e re d ita ry hemo chro mato sis. Blo o d Ver 1994;8(4):193-8.
84. Sveinb jo rnsdo ttir S, Blo ndal H, Gudmundsso n G, Kjartansso n O, Jo n s d o ttir S, Gu d m u n d s s o n G. Pro g re s s ive d e m e n tia a n d le uko e nc e p halo p athy as the initial p re se ntatio n o f late o nse t hereditary cystatin-C amylo ido sis. Clinico patho lo gical presentatio n o f two cases. J Neuro l Sci 1996;140(1-2):101-8.
85. Simo n DK, Ro driguez ML, Fro sh MP, Quackenb ush EJ, Feske SK, Nato wicz MR. A uniq ue familial leuko dystro phy with adult o nset d e m e ntia and ab no rm al glyc o lip id sto rage : a ne w lyso so m al disease? J Neuro l Neuro surg Psychiatry 1998;65(2):251-4.
86. Blau N, Blasko vics ME, Duran M. Simple test in urine and b lo o d, pp. 3-11. In: Blau, N, Duran M, Blasko vics ME. Physician’ s guide to the lab o rato ry diagno sis o f m e tab o lic dise ase s, 1st Editio n. Oxfo rd: Chapman & Hall Medical; 1996.
87. Buist N. Set o f simple side-ro o m urine tests o f inb o rn erro rs o f metab o lism. Br Med J 1968;2:745-9.
88. Tho m as GH, Ho we ll RR. Se le c te d sc re e ning te sts fo r ge ne tic metab o lic diseases. Chicago , Year Bo o k Medical Pub lishers; 1973.
89. Gio rgio AJ, Luhb y ALA. A rapid screening test fo r the detectio n o f co ngenital methylmalo nic aciduria in infancy. Am J Clin Patho l 1969;52:374-9.
90. Efro n M L, Yo u n g D, M o s e r HW, M a c Cre a d y RA. A s im p le chro mato graphic screening test fo r the detectio n o f diso rders o f amino acid metab o lism: a techniq ue using who le b lo o d o r urine co llected o n filter paper. N Engl J Med 1964;270:1378-83.
91. Ho ffman GF. Organic acid analysis. Part One C, pp. 31-49. In: Nenad B, Duran M, Blasko vics ME. Physician’s guide to the diagno sis o f
metab o lic diseases. Oxfo rd: Chapman & Hall; 1996.
92. Shih VE. Amino acid analysis. Part 1B, pp. 13-29. In: Nenad B, Duran M, Blasko vics ME. Physician’s guide to the diagno sis o f metab o lic diseases. Oxfo rd: Chapman & Hall; 1996.
93. Ste rn HJ. Lac tic ac id o sis in p e d iatric s: c linic al and lab o rato ry evaluatio n. Ann Clin Bio chem 1994;31:410-9.
94. Ridaura-Sanz C. The patho lo gist’s appro ach to the diagno sis o f metab o lic disease. Path Res Pract 1994;190:1109-22.
95. Dixo n MA, Le o nard JV. Inte rc urre nt illne ss in inb o rn e rro rs o f intermediary metab o lism. Arch Dis Child 1992;67:1387-9.
96. Champe PC, Harvey RA. Bio química Ilustrada. 2nd ed. Artes Médicas; 1996.
97. Harris RE, Leslie N, Krivit W. Lyso so mal and pero xiso mal sto rage disease, Part 6.11, pp. 275-285. In: Burrt RK, Deeg HJ, Lo thian ST, Santo s G. On call in: b o ne marro w transplantatio n. RG Landes Co mpany; 1996.
98. McKinnis EJ, Sulzb acher S, Rutledge JC, Sanders J, Sco tt CR. Bo ne m a rro w tra n s p la n ta tio n in Hu n te r s yn d ro m e . J Pe d ia tr 1996;129(1):145-8.
99. Guffo n N, So uillet G, Maire I, Straczek J, Guib aud P. Fo llo w-up o f n in e p a tie n ts with Hu rle r s yn d ro m e a fte r b o n e m a rro w transplantatio n. J Pediatr 1998;133(1):119-25.
100. Peters C, Shapiro EG, Anderso n J, et al. Hurler syndro me: o utco me o f HLA-ge no typically ide ntical sib ling and HLA-haplo ide ntical related do no r b o ne marro w transplantatio n in fifty-fo ur children. Th e s to ra g e d is e a s e c o lla b o ra tive s tu d y g ro u p . Blo o d 1998;91(7):2601-8.
101. Beutler E, Demina A, Laub scher K , et al. The clinical co urse o f treated and untreated Gaucher disease: a study o f 45 patients. Blo o d Cells Mo l Dis 1995;21(10):86-108.
102. Ch a rro w J, Es p lin JA, Grib le TJ, e t a l. Ga u c h e r d is e a s e : reco mmendatio ns o n diagno sis, evaluatio n, and mo nito ring. Arch Intern Med 1998;158(16):1754-60.
103. Damiano AM, Pasto res GM, Ware JE Jr. The health-related q uality o f life adults with Gaucher’s disease receiving enzyme replacement th e rap y: re s u lts fro m a re tro s p e c tive s tu d y. Q u al Life Re s 1998;7(5):373-86.
104. Bro o ks DA, King BM, Crawley AC, Byers S, Ho pwo o d JJ. Enzyme replacement therapy in muco po lysaccharo do sis VI: Evidence fo r immune re spo nse s and alte re d e fficacy o f tre atme nt in animal mo dels. Bio chim Bio phys Acta 1997;1361(2):203-16.
105. O’Co nno r LH, Lawrence CE, Vo gler CA, et al. Enzyme replacement the rap y fo r m urine m uc o p o lys ac c harid o s is typ e VII le ad s to im pro ve m e nts in b e havio r and audito ry functio n. J Clin Inve st 1998;101(7):1394-400.
Ack now ledgements - To sta ff o f the multidisc iplina ry o utpa tient c linic fo r resea rc h into heredita ry meta b o lic disea ses a nd to the IEM la b o ra to ry o f the Center fo r G enetic Medic ine o f UN IFESP fo r their c o lla b o ra tio n.
Ana M a ria M a rtins – MD. PhD. Depa rtment o f Pedia tric s, Universida de Federa l de Sã o Pa ulo / Esc o la Paulista de Medicina. São Paulo , Braz il.
Sources of funding: FAPESP fo r suppo rting the IEM investig a tio n, g ra nt no . 9 7 / 1 0 8 3 8 -7
Conflict of interest: N o t dec la red
La st received: 5 Ja nua ry 1 9 9 9
Accepted: 2 1 Septemb er 1 9 9 9
Address for correspondence:
Ana Ma ria Ma rtins
Avenida N o ve de Julho , 2 0 2 1 / 1 3 3 Sã o Pa ulo / SP - Bra sil - CEP 0 1 3 1 3 -0 0 1 E-ma il: a na ma rtins.dped@ epm.b r
RESUMO
CON TEX TO: O s erro s inato s do metabo lismo (EIM) causam as do enças metabó licas hereditárias (DMH) e classicamente resultam da falta de atividade de uma o u mais enzimas específicas o u defeito s no transpo rte de pro teínas. OBJETIVOS: Revisão clínica so bre Erro s Inato s do Metabo lismo (EIM) vo ltada para o médico na sua prática diária, co m tabelas e fig uras que
sumariam as diversas do enças que fazem parte deste assunto . Uma pequena revisão das bases bio químicas suficiente para co mpreensão da fisio pato lo g ia do s EIM. FON TES DOS DADOS: Pesquisa biblio g ráfica utilizando livro s de texto s so bre o s EIM e suas bases bio químicas (Scriver, CR et al, 1 9 9 5 ), revisão da literatura que abrang eu o s artig o s clássico s e aqueles publicado s no s último s dez ano s, fo rnecendo assim referências atualizadas so bre as diversas do enças metabó licas hereditárias (DMH). SELEÇÃO DOS ESTUDOS: Fo i realizada seleção de texto s de auto res co nsag rado s pelo co nhecimento e experiência na área do s EIM e descrição de caso s clínico s co m suas manifestaçõ es clínicas mais peculiares e marcantes. SÍN TESE DOS
DADOS: O s EIM são do enças subdiag no sticadas pela falta de hábito do médico g eral, neo nato lo g ista e intensivista em pensar nesta hipó tese. N a revisão são descrito s o s mecanismo s de herança, as principais características clínicas e o s achado s
labo rato riais do s EIM, dentro de uma classificação que fo rnece uma visão g eral so bre o assunto . São abo rdadas sumariamente as fo rmas de tratamento existentes para o s diverso s g rupo s de EIM. CON CLUSÕES: O s EIM não são do enças raras co mo se pensava no passado e pacientes po rtado res de DMH fazem parte do atendimento g eral no s pro nto -atendimento s, nas clínicas cirúrg icas, o bstétricas, pediátricas, neuro ló g icas e psiquiátricas, ag uardando diag nó stico , pro g nó stico e tratamento terapêutic o e/ o u de supo rte.