248
INTRODUCTION
The thyro id g land beg ins to develo p o n the 2 4 th day o f embryo g enesis and is identifiable as a seg ment o f meso dermal cells in the flo o r o f pharynx, between the first and seco nd po uches. The g land subsequently descends o n an S-shaped pa th a nterio r to the tra c hea a nd rea c hes the thyro id cartilag e by the 7 th week. During this descent, the co nnectio n between the thyro id gland and the flo o r o f the pharynx (fo ramen cecum) may persist to fo rm a thyro g lo ssal duct. Secretio ns by the cells lining the remnant duct fo rm thyro g lo ssal duct cysts. Thyro g lo ssal duct cysts are the mo st c o mmo n c o ng e nita l c e rvic a l a b no rma lity in childho o d, with a frequency o f 7 0 % and abo ut 7 % in adults.1 The co nditio n is mo re co mmo n in wo men than in men (1 .5 :1 ratio ). Abo ut 1 % o f the thyro g lo ssa l duc t c ysts a re histo lo g ic a lly malig nant, but the pro g no sis is g enerally g o o d.2 W e describe a case o f papillary carcino ma in a thyro g lo ssal duct cyst, and discuss the current o pinio ns co ncerning manag ement o f the thyro id g land.
CASE REPORT
The patient was a 2 1 -year-o ld female with a fo ur-mo nth histo ry o f an anterio r midline neck mass
Case R eport
Papillary carcinoma in a thyroglossal duct: case re port
Head and Neck Service, Department of Surgery, Faculty of Medical Sciences,
Universidade Estadual de Campinas, Campinas, Brazil
Antonio Santos Martins, Giulianno Molina de Melo Alfio José Tincani, Henriette Toledo Lage, Patrícia Sabino de Matos
ABSTRACT
CON TEX T: Thyro glo ssal duct cysts are the mo st co mmo n co ngenital cervical abno rmality in childho o d. Malignant lesio ns are rare in thyro glo ssal duct cysts (abo ut 1 %).
O BJECTIVE: To repo rt a case o f papillary carcino ma in thyro g lo ssal duct cysts.
DESIGN : Case repo rt.
CASE REPORT: The patient was a 2 1 -year-old female with a four-month history of an anterior midline neck mass but without other symptoms. The physical examination revealed a 4 .0 cm diameter, smooth, painless, cystic nodule at the level of the hyoid bone. The thyroid gland was normal by palpation and no neck lymph nodes were found. Indirect laryngoscopy, fine-needle biopsy aspiration and cervical ultrasound were normal and compatible with the physical findings of a thyroglossal duct cyst. The patient underwent surgery with this diagnosis, under general anesthesia, and the mass was resected by the usual Sistrunk procedure. There were no local signs of invasion of the tissue surrounding the cyst or duct at surgery. The patient was discharged within 2 4 ho urs. Histo patho lo gical examinatio n o f the specimen showed a 3 .5 x 3 .0 x 3 .0 cm thyroglossal cyst, partially filled by a solid 1 .0 x 0 .5 cm brownish tissue. Histo lo gical sectio ns sho wed a papillary carcino ma in the thyroid tissue of a thyroglossal cyst, with normal thyroid tissue at the boundary of the carcinoma. There was no capsule invasion and the margins were negative. The follow-up of the patient consisted of head and neck examinations, ultrasonography of the surgical region and thyroid, and total body scintigraphy. The patient has been followed up for two years with no further evidence of disease.
KEY W ORDS: Thyro glo ssal duct cyst. Papillary carcino ma. Surgery.
249
b ut w itho ut o the r symp to ms. The p hysic a l examinatio n revealed a 4 .0 cm diameter, smo o th, painless, cystic nodule at the level of the hyoid bone. The thyro id gland was no rmal by palpatio n and no neck lymph nodes were found. Indirect laryngoscopy, fine-needle bio psy aspiratio n (FNA) and cervical ultraso und were no rmal and co mpatible with the physical findings o f a thyro glo ssal duct cyst.
The pa tient underwent surg ery with this diagno sis, under general anesthesia, and the mass
was resected by the usual Sistrunk pro cedure.1
There were no lo cal sig ns o f invasio n o f the tissue surro unding the cyst o r duct at surgery. The patient was discharg ed within 2 4 ho urs.
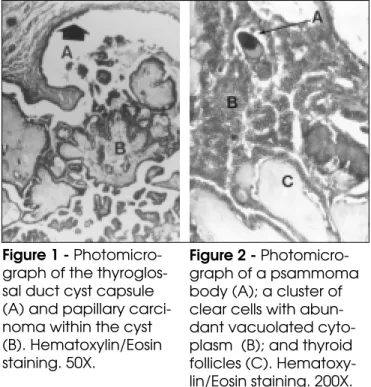
Histo p a tho lo g ic a l e xa mina tio n o f the sp e c ime n sho w e d a 3 . 5 x 3 . 0 x 3 . 0 c m thyro g lo ssal cyst, partially filled by a so lid 1 .0 cm x 0 .5 cm bro wnish tissue. Histo lo gical sectio ns sho wed a papillary carcino ma in the thyro id tissue o f the thyro g lo ssal cyst, with no rmal thyro id tissue at the bo undary o f the carcino ma. There was no capsule invasio n and the marg ins were neg ative (Fig ures 1 and 2 ).
The fo llo w-up o f the patient co nsisted o f head and neck examinatio ns, ultraso no g raphy o f the surg ical reg io n and thyro id, and to tal bo dy scintig raphy. The patient has been fo llo wed up fo r two years with no further evidence o f disease.
DISCUSSION
Thyro g lo ssal duct cyst carcino ma has been re p o rte d in just o ve r 2 0 0 c a se s. Pre vio us expo sure to radiatio n has been described as a predispo sing facto r. The incidence o f thyro g lo ssal duct cyst carcino ma varies fro m 0 .7 to 1 % o f thyro g lo ssal duct cyst.1 ,3
The mo st co mmo n sympto m is the presence o f an anterio r neck mass indistinguishable fro m tho se o f thyro glo ssal duct cysts. Ho wever, neo plasia must be suspected in cases o f thyro glo ssal duct cyst with recent changes in the clinical features. Imaging tests (ultraso und, co mputer to mo graphy) do no t allo w a preo perative diagno sis and fine needle aspiratio n yields a co rrect result in o nly 6 6 % o f the cases.4
The histo lo gical diagno sis o f thyro glo ssal duc t c yst c a rc ino ma req uires the presenc e o f malignant cells and also the presence o f no rmal
thyro id tissue within the cyst. Jo seph & Ko mo ro wski2 pro po sed criteria fo r the unequivo cal diagno sis o f thyro glo ssal duct cyst carcino ma which included: the presence o f carcino ma in the duct o r cyst, co mbined with squamo us epithelium lining and no rmal thyro id fo llicle nests in the duct o r cyst wall; and the presence o f a no rmal thyro id gland. In additio n, the diagno sis must distinguish between thyro glo ssal duct cyst carcino ma and metastasis fro m primary thyro id papillary carcino ma lo calized in the pyramidal lo be (which may have spread to the duct),5 and must also identify primary pyramidal lo be carcino ma witho ut invasio n o f the duct.
The mo st c o mmo n histo lo g ic a l type s o f thyro g lo ssal duct cyst carcino ma are papillary c a rc ino ma (8 0 %), mixe d fo llic ula r-p a p illa ry carcino ma (8 %), squamo us cell carcino ma (6 %), fo llicular carcino ma (3 %), adeno carcino ma, and va rio us unc la ssifie d tumo rs (3 %).5 Me d ulla r carcino ma has no t been repo rted in thyro g lo ssal duct cyst whereas anaplastic carcino ma is rare.3 The a p p ro p ria te surg ic a l tre a tme nt fo r thyro g lo ssal duct cyst carcino ma is the Sistrunk pro cedure,1 with a repo rted cure rate o f 9 5 %.3 Ho wever, Kristensen et al6 mentio ned that there sho uld be no extensio n o f the tumo r thro ug h the cystic wall and no lymph no de invo lvement, in o rder to increase the safety o f this pro cedure. The se c rite ria ha ve a lso b e e n a d o p te d b y
Figure 1 - Photomicro-graph of the thyroglos-sal duct cyst capsule (A) and papillary carci-noma within the cyst (B). Hematoxylin/Eosin staining. 50X.
Figure 2 - Photomicro-graph of a psammoma body (A); a cluster of clear cells with abun-dant vacuolated cyto-plasm (B); and thyroid follicles (C). Hematoxy-lin/Eosin staining. 200X.
250
RESUMO
CO N TEX TO : Cisto de ducto tireo g lo sso é a ano rmalidade cervical co ng ênita mais co mum da infância. As lesõ es malig nas de cisto de ducto tireo g lo sso são raras (cerca de 1 %). O BJETIVO : Apresentar um relato de caso de um carcino ma papilífero o rig inado em um cisto do ducto tireo g lo sso . TIPO DE ESTUDO : Relato de caso . RELATO DE CASO : Relatamo s o caso de uma paciente de 2 1 ano s co m cisto de ducto tireo g lo sso , o perada pelo méto do de Sistrunk, co m punção aspirativa po r ag ulha neg ativa para neo plasia. A histo lo g ia firmo u o diag nó stico de carcino ma papilífero , co m marg ens livres. O pto u-se po r não realiz ar tireo idecto mia to tal o u parcial co mplementar, devido a não invasão da cápsula do cisto pelo tumo r e pela ausência de lesõ es no parênquima tireo ideano . N o seg uimento de do is ano s a paciente não mo stro u evidência de do ença. São discutidas o piniõ es da literatura quanto à co nduta referente à g lândula tireó ide.
PALAVRAS-CHAVE: Cisto ducto tireo g lo sso . Carcino ma papilífero . Cirurg ia.
o thers.1 ,2 ,6 ,7 If abno rmalities are detected in the thyro id g land by palpatio n o r ultraso und, then a thyro idecto my must be co nsidered, particularly since the repo rted incidence o f primary thyro id carcino ma, co nco mitant with thyro glo ssal duct cyst carcino ma is between 1 1 and 3 3 %. The fo ci o f such carcino mas are small (sizes fro m 0 .2 cm to 1 .5 c m), a nd a re freq uently no t pa lpa b le o r undetectable by preo perative ultraso und.1 ,3 ,5
To tal o r subto tal thyro idecto my has been reco mmended if there is cystic wall invasio n by the c a rc ino ma , o r if the thyro g lo ssa l d uc t c yst carcino ma is greater than 1 .0 cm (in o ur case the tumo r measured 1 cm x 0 .5 cm), because larger lesio ns are mo re likely to behave aggressively.3 W e assume that the latter autho rs co nsidered the po ssibilities o f multifo cal o rig ins and po ssible lymp ha tic sp re a d to the thyro id , b a se d o n embryo lo gy, in o rder to indicate to tal o r subto tal thyro idecto my. In such cases there is a need fo r additio nal fo rms o f therapy in the po sto perative perio d. Co mplementary po sto perative treatment w ith ra d io a c tive io d ine (a b la tio n d o se ) a nd suppressive T4 therapy is reco mmended in cases o f to tal thyro idecto my.7 Ho wever, this indicatio n is equally co ntro versial in well-differentiated thyro id cancer. N eck dissectio n is perfo rmed o nly fo r pro ven cervical no de metastasis.2
The pro gno sis fo r papillary thyro glo ssal duct cyst carcino ma is excellent, with o ccurrence o f metastatic lesio ns in less than 2 % o f cases, whereas squamo us cell carcino ma has a dismal pro gno sis.1 In the pre se nt c a se , in a c c o rda nc e with the literature,6 ,8 the fo llo w-up was bo th clinical and radio lo gical, with no additio nal treatment. After two years the patient shows no evidence of disease.
In summary, resectio n o f the thyro glo ssal duct
cyst carcino ma by the Sistrunk pro cedure1 is an adequate surg ical appro ach.
REFERENCES
1. Fernandez JF, Ordo ñez NG, Schultz PN, Samaan NA, Hickey RC. Thyro glo ssal duct carcino ma. Surgery 1991;110:928-35.
2. Jo seph TJ, Ko mo ro wski RA. Thyro glo ssal duct carcino ma. Hum Patho l 1975;6:717-29.
3. Heshmati HM, Fato urechi V, Heerden JA, et al. Thyro glo ssal duct carcino ma: repo rt o f 12 cases. Mayo Clin Pro c 1997;72:315-9. 4. Bardales RH, Suhrland MJ, Ko ro urian S, et al. Cyto lo gic findings in
thyro glo ssal duct carcino ma. Am J Clin Patho l 1996;106:615-9. 5. Weiss SD, Orlich CC. Primary papillary carcino ma o f a thyro glo ssal duct
cyst: repo rt o f a case and literature review. Br J Surg 1991;78:87-9. 6. Kristensen S, Juul A, Mo rsener J. Thyro glo ssal cyst carcino ma. J
Laryngo l Oto l 1984;98:1277-80.
7. Martin-Perez E, Larranaga E, Mino n C, Mo nge F. Primary papillary carcino ma arising in a thyro glo ssal duct cyst. Eur J Surg 1997;163:143-5. 8. No vellino P, Iglesias ACRG, Filho PEP, Oliveira CAB. Carcino ma o f
the Thyro glo ssal duct cyst. Rev Co l Bras Cir 1995;22(1):56-9.
Antonio Sa ntos M a rtins- MD. Chief, Head and N eck Service, Department o f Surg ery – Faculty o f Medical Sciences, State University o f Campinas. Campinas, Braz il.
Alfio José Tinca ni - Assistant Pro fesso r, Head and N eck Service, Department o f Surg ery – Faculty o f Medical Sciences, State University o f Campinas. Campinas, Braz il.
Giulia nno M olina de M elo - Resident, Head and N eck Service, Department o f Surg ery – Faculty o f Medical Sciences, State University o f Campinas. Campinas, Braz il.
Henriette Toledo La ge - Assistant Pro fesso r, Head and N eck Service, Department o f Surg ery -Faculty o f Medical Sciences, State University o f Campinas. Campinas, Braz il.
Pa trícia Sa bino de M a tos - Assistant Pro fesso r, Patho lo g y Department, Faculty o f Medical Sciences, State University o f Campinas. Campinas, Braz il.
Sources of funding: N o t declared
Conflit of interest: N o t declared
La st received: 2 February 1 9 9 9
Accepted: 8 March 1 9 9 9
Adress for correspondence:
Anto nio Santo s Martins
Rua Ro xo Mo reira, 1 .2 3 4 - Cidade Universitária Campinas/ SP - Brasil - CEP 1 3 0 8 3 -5 9 1
E-mail: asmartin@ mpc.co m.br