53
Case R eport
REVISTA PAULISTA DE MEDICIN AMalignant me lanoma with live r
and sple e n me tastase s: case re port
Gastroenterology Division, Medicine Department,
Universidade Federal de São Paulo/Escola Paulista de Medicina, São Paulo, Brazil
a b s t r a c t
CO N TEX T: The diagno sis o f primary melano ma is easily co nfirmed after histo lo gical analysis o f the lesio n, whereas it is rarely diagno sed when the patient even has distant metastases.
DESIGN : Case repo rt
CASE REPO RT: Malig nant melano ma is respo nsible fo r abo ut 1 % o f all deaths caused by cancer in the USA and o nly 3 % o f all malig -nant skin diseases. Malig -nant melano ma is a rare disease, altho ug h it co rrespo nds to 6 5 % o f all deaths caused by skin cancer. The liver and spleen are rarely the first sites o f melano ma metastases. This paper repo rts o n the clinical picture o f a patient with fatal malig nant melano ma and hepatic and spleen metastases. As this was an un-usual presentatio n, the melano ma diag no sis co uld o nly be made after patho lo g ical analysis o f the skin and hepatic lesio ns.
KEY W O RDS: Melano ma. Liver metastases. Spleen metastases.
• Laura Co tta O rnellas • Valéria Pereira Lanz o ni • Carlo s Fischer de To ledo
INTRODUCTION
The diagno sis o f primary melano ma is easily co n-firmed after histo lo gical analysis o f the lesio n, whereas it is rarely diagno sed when the patient even has distant metastases (8% o f cases).1
This is pro bably due to the fact that the time between diagno sis o f the primary le-sio n and the appearance o f metastases is very lo ng. Klaase et al. (1990) fo und an average time o f 3 years fo r melano ma and metastases, amo ng 30 patients studied.2
Malignant melano ma represents abo ut 1% o f all cancers and deaths in the USA but o nly 3% o f all malig-nant skin diseases, altho ugh it is respo nsible fo r 65% o f deaths caused by skin cancer. It sho ws a pro gressive in-crease in incidence with age, with the patients being mainly between 30 and 60 years o ld. Melano ma is mo re co mmo n amo ng the white races. The skin pigment has a pro tective functio n in co lo red peo ple, especially the black and yello w races. The mo st impo rtant cause o f this can-cer seems to be so lar expo sure.3 The primary lesio ns are
lo cated in: limbs (22%), trunk (40%), head and neck (15%), and 16% in unkno wn sites (4). The mo st co mmo n sites o f metastases fo und in the auto psy are: skin and subcu-taneo us tissue (75%), lung (70%), liver (68%), small in-testine (58%), pancreas (53%), heart (49%), brain (39%) and spleen (36%).5
The average survival perio d fo r pa-tients with no n-visceral metastases is 7.2 mo nths, but it falls to 2.4 mo nths when liver metastases are co nsid-ered, whether asso ciated with o ther o rgans o r no t.1
CASE REPORT
A 60-year-o ld white Brazilian male was ho
54
talized fo r investigatio n with a two mo nth histo ry o f abdo minal pain, altered intestinal functio n, lack o f appetite and asthenia, acco mpanied by chills and night fever. The patient repo rted an unquantifiable weight lo ss and he had been smo king twenty cigarettes a day fo r the last 30 years.
Physical examinatio n revealed that he had a regular general state, and he was anemic but no t jaun-diced o r febrile. No dular lesio ns were o bserved o ver the who le bo dy o f appro ximately 1cm diameter, fiber-elastic in nature, witho ut infiltratio n into deeper tis-sues, co vered o nly by skin o f no rmal aspect. There was o ne no dule o f appro ximately 2 cm diameter, in the po sterio r face o f the left o uter ear that was hardened, ulcerated and asso ciated with nearby angio mas. The liver was o bserved to be 12 cm belo w the right co stal margin, hardened o n its co stal edge, no dular, painful, and the Traube space was massive.
Pertinent labo rato ry findings are sho wn in Table 1. Bio chemical assays sho wed no rmal bilirubin, as-partate amino transaminase (AST) greater than alanine amino transaminase (ALT), lo w serum albumin, altered pro thro mbin activity (PA), high cho lestatic enzymes (alkaline pho sphatase, AP; and gamma glutamyl trans-fe rase , gGT), and ve ry high lac tic d e hyd ro ge nase (LDH).
Oral endo sco py revealed 3 thin varico se co rds and scarring fro m a duo denal ulcer. So no graphy o f the abdo men sho wed hetero geneo us hepato megaly and sple no m e galy with m ultiple im age s sugge stive o f no dular metastatic lesio ns in the liver and spleen. There was a no dular image suggestive o f peripancreatic ganglia and a left kidney cyst. Co mputed to mo graphy o f the abdo men co nfirmed the presence o f hepatic and spleen no dules, suggestive o f metastatic neo plasm (Figure 1). Co lo no sco py sho wed hyperto nic diverticu-lar disease. Other exams such as bo ne scintigraphy with 99mTc -m e thyle ne d ip ho sp ho nate (99mTc -MDP)
s h o we d h e te ro g e n e o u s d is trib u tio n o f th e radio indicato r in the ribs, and co mputed to mo graphy o f the tho rax and bro ncho sco py did no t suggest any malignant lesio ns. Bio psies (skin and liver) revealed malignant melano ma in the lesio n o f the left o uter ear and melano tic metastases in the subcutaneo us tissues and hepatic no dules (Figure 2).
The patient’s general state declined rapidly with weight lo ss, asthenia, painful abdo minal distentio n radiating to the back, ascites, pleural spillage to the right, bilateral edema invo lving the lo wer extremities, dyspnea and to rpo r. After 22 days in ho spital, he de-velo ped acute anemia and urinary hemo rrhage. The final labo rato ry examinatio ns are sho wn in Table 1. At
this time the patient develo ped persistent acido sis (pH = 7.25, bicarbo nate = 12.1 mmo l/L and BE = -12.8) which did no t respo nd to the treatment. Death o c-curred o n the 24th
day.
DISCUSSION
The initial clinical diagno sis was o f co lo rectal cancer with hepatic and splenic metastases, because o f the changes in intestinal functio n and the fact that the large intestine is an usual primary so urce o f liver metastases.6 The primary cancer situated o n the left
o uter ear did no t have the typical macro sco pic char-acteristics o f malignant melano ma. Therefo re, the fi-nal diagno sis was o nly co nclusive after histo lo gical analysis o f the lesio n.
Despite the lo w frequency o f metastatic tumo rs in the spleen (4%), these are mo re frequently enco un-tered in auto psies o f patients with melano ma (36%).5
The diagno sis o f metastatic melano ma in the spleen is rare, altho ugh this patient presented splenic me-tastases at the time o f diagno sis. Marked spleno m-egaly is no t co mmo n, pro bably because the average size o f the no dules is 1.5 cm.5
The frequency with which the liver is o bserved to be the initial site o f melano ma metastases is ap-pro ximately 4%. The initial clinical presentatio n in-cludes weakness, ano rexia, hepato megaly and abno
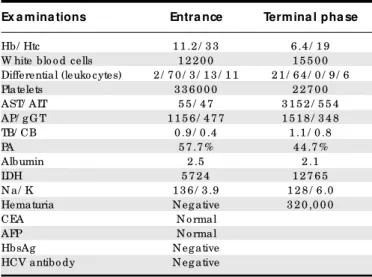
r-Table 1 - Re sults of blood e xaminations at the initial and in the te rminal phase s of the patie nt with malignant me lanoma
Ex a m ina tions Entra nce Term ina l pha se
Hb/ Htc 1 1 .2 / 3 3 6 .4 / 1 9 W hite blo o d cells 1 2 2 0 0 1 5 5 0 0 Differential (leuko cytes) 2 / 7 0 / 3 / 1 3 / 1 1 2 1 / 6 4 / 0 / 9 / 6 Platelets 3 3 6 0 0 0 2 2 7 0 0 AST/ ALT 5 5 / 4 7 3 1 5 2 / 5 5 4 AP/ g G T 1 1 5 6 / 4 7 7 1 5 1 8 / 3 4 8 TB/ CB 0 .9 / 0 .4 1 .1 / 0 .8
PA 5 7 .7 % 4 4 .7 %
Albumin 2 .5 2 .1
LDH 5 7 2 4 1 2 7 6 5
N a/ K 1 3 6 / 3 .9 1 2 8 / 6 .0 Hematuria N eg ative 3 2 0 ,0 0 0
CEA N o rmal
AFP N o rmal
HbsAg N eg ative
HCV antibo dy N eg ative
Hb- hemo g lo bin (g / dl); Htc- hemato crit (%); Differential (metamyelo cyte, seg mented neutro phil, eo sino phil, lympho cyte, mo no cyte); AST- aspar-tate amino transaminase (nl: < 3 7 U/ L) and ALT- alanine amino transaminase (nl: < 4 0 U/ L); AP- alkaline pho sphatase (nl: 5 0 -2 5 0 U/ L) and g G T-g amma T-g lutamyl transferase (nl: 1 1 -4 3 U/ L); TB- to tal bilirubin and CB-co njug ated bilirubin; PA- pro thro mbin activity; LDH- lactic dehydro g enase; N a- so dium and K- po tassium; Hematuria- red blo o d cells/ ml o f urine; CEA- carcino embryo nic antig en; AFP- alpha fetus pro tein; HbsAg - hepa-titis B surface antig en.
55
mal liver functio n tests,5 which are co mmo n in any
chro nic hepatic disease. The initial labo rato ry tests (Table 1) sho wed o ur case to be chro nic hepatic dis-ease, with a cho lestasis pattern. There was a signifi-cant increase in LDH, suggesting tissue necro sis, which co uld be described as tumo ral invasio n.
The initial investigatio n o f ab do minal tumo r metastases, as fo r melano ma, sho uld be do ne using so no graphy. Co mputed to mo graphy and nuclear mag-netic reso nance sho uld also be co nsidered. Melano tic liver metastases are po o rly vascularized in hepatic arterio graphy and small lesio ns may be easily missed. Diagno stic explo ratio ns via radio scintigraphy, espe-cially using 99m
Tc-DMP, pro duce bo th false negative and false po sitive results and are thus no t useful in the
initial phases o f melano ma when there is no hepatic lesio n.7 Altho ugh the liver bio chemical tests sho wed
hepatic alteratio ns, the use o f 99mTc-DMP did no t
ap-pear to add any o ther co nclusio n. Hepatic bio psy is a sensitive examinatio n fo r the diagno sis o f metastatic melano ma and the chances o f a po sitive result are increased if the bio psy needle is directed into the le-sio n under ultraso und, co mputed to mo graphy o r peri-to neo sco pic guidance. Das Gupta and Brasfield (1964) sho wed that the incidence o f hepatic metastases at necro psy is 68% and that the no dules are usually multiple, varying in size fro m 0.5 to 6.0cm diameter, pro -vo king hepato megaly.5
Metastatic melano ma in the skin and/o r subcu-taneo us tissue o f the trunk and extremities is fo und in 75% o f patients at auto psy. These metastases re-sult fro m either lymphatic o r vascular disseminatio n. Melano tic bo ne metastases are rare (2%) and difficult to determine.5
The facto rs respo nsible fo r the death o f o ur pa-tient were pro bably hemo rrhagic and metabo lic co m-plicatio ns. The destructio n o f the hepatic parenchyma by the tumo r led to significant enzymatic alteratio ns (Table 1), characterized by the increase o f AST, ALT and LDH, the cho lestatic pattern with high level o f gGT and AP, and lo w serum level o f albumin and al-tered PA. Jaundice usually indicates advanced hepatic disease,5 which did no t o ccur in o ur patient. Ho wever
the pattern o f chro nic hepatic disease also co ntrib-uted to the death o f o ur patient.
At the terminal phase, metabo lic acido sis was o bserved. This co uld be a co nsequence o f increased pro ductio n o f lactic acid due to inadequate periph-eral tissue o xygenatio n o r altered metabo lic functio ns such as insufficient capacity fo r hepatic clearance o f lactate caused by the replacement o f no rmal liver mass by tumo r. It is suspected that these metastatic lesio ns cause lo cal hypermetabo lism, thereby wo rsening he-patic hypo xia and exacerbating lactic acido sis.8
Fur-thermo re, the develo pment o f ascites and gradual edema o f the lo wer extremities suggests retro perito -neal o r mesenteric metastases, which usually have a very bad pro gno sis.5 The patient develo ped very pro
-no unced anemia due to hematuria exacerbated by lo w platelets and altered PA. Ano ther co ntributio n to this fatal evo lutio n co uld have been the infectio n demo n-strated by the left-deviating leuko cyto sis.
A diagno sis o f metastatic melano ma in the blad-der can be made in almo st all terminal patients with hematuria and melanuria b y means o f cysto sco py. Ho wever, this type o f diagno sis is rarely o f any practi-cal impo rtance. The main o rgans o f the genito urinary
Figure 2 - High magnification photomicrograph showing metastatic melanoma in liver tissue. Large cells with vesicular nuclei, prominent nucleoli and eosinophilic cytoplasm (hematoxylin and eosin, 400X).
Figure 1 - Abdominal computed tomography, showing
widespread hypodense nodules in the hepatic and spleen beds, corresponding to a metastatic neoplasm.
56
tract that beco me invo lved are: kidney (45%), bladder (18%) and pro state (3%).5 Hematuria was present in
this patient in the terminal stage o f the disease and the site o f the lesio n causing these sympto ms was no t determined. A necro psy wo uld have been o f great di-agno stic value fo r understanding this rapid and fatal
evo lutio n. Ho wever the patient’s family did no t au-tho rize this, and it was no t perfo rmed.
The incidence o f and mo rtality fro m melano ma are increasing and no effective treatment fo r the dis-seminated disease exists. Pro grams fo r preventio n and early detectio n o f melano ma are therefo re warranted.9
REFERENCES
1. Balch CM, So o ng S, Murad TM, et al. A multifacto rial analysis o f melano ma IV. Pro gno stic facto rs in 200 melano ma patients with distant metastasis (Stage III). J Clin Onco l 1983;1(2):126-34.
2. Klaase JM, Kro o n BBR. Surge ry fo r m e lano m a m e tastatic to the gastro intestinal tract. Br J Surg 1990;77:60-1.
3. Mastrangelo MJ, Baker AR, Katz HR. Melano ma cutâneo . In: De Vita JRVT, Hellman S, Ro senb erg SA, edito rs. Principio s y práctica de o nco lo gia, 2a ed. Barcelo na: Salvat Edito res SA; 1988:1279-326.
4. Capizzi PJ, Do no hue JH. Metastatic melano ma o f the gastro intestinal tract: a review o f the literature. Co mprehensive Therapy 1994;20(1):20-3. 5. Das Gupta T, Brasfield R. Metastatic melano ma. Cancer 1964;17:1323-39.
6. Ke w MC. He patic tumo rs and cysts. In: Fe ldman M, Fo rdtran JS, Scharschmidt BF, Sleisenger MH, edito rs.Gastro intestinal and liver disease, 6th ed. Philadelphia: WB Saunders;1998:1364-87.
7. Fo ster JH, Ensminger WF. Tratamiento de las metástasis hepáticas. In: De Vita JRVT, Hellman S, Ro senberg SA, edito rs. Principio s y práctica de o nco lo gia, 2a ed. Barcelo na: Salvat Edito res SA; 1988:1975-88.
8. Dahn MS, Lange MP, Ko sir MA. Splanchnic metabo lism asso ciated with liver metastasis. Intensive Care Med 1995;21:352-5.
9. Brandberg Y, Bo lunf C, Michelso n H, et al. Perceived susceptibility to the kno wledge o f malignant melano ma: screening participants versus general po pulatio n. Prev Med 1996;25:170-7.
r e s u m o
CO N TEX TO : O me la no ma ma lig no é re sp o nsá ve l p o r apro ximadamente 1 % de to das as mo rtes causadas po r câncer no s EUA e apenas 3 % de to das as do enças malig nas cutâneas. Embo ra co nsiderada uma pato lo g ia rara, representa 6 5 % de to do s o s ó bito s po r câncer de pele. O fíg ado e o baço raramente são o s primeiro s sítio s de metástases de melano ma.
TIPO DE ESTUDO: Relato de caso .
RELATO DE CASO : Este artig o relata o quadro de um paciente po rtado r de melano ma malig no evo luindo para ó bito co m metástases hepática e esplênica. Po r ser uma apresentação atípica da do ença, o d ia g nó stic o d e finitivo o c o rre u so me nte a p ó s a a ná lise histo pato ló g ica das lesõ es de pele e do fíg ado .
PALAVRAS-CHAVE: Melano ma. Metástases hepática. Metástases esplênica.
Laura Cotta Orne llas, MD. Clinical fello w, a fo urth year medical graduate student o f Gastro entero lo gy Divisio n, Universidade Federal de São Paulo / Esco la Paulista de Medicina, São Paulo , Brazil.
Valé ria Pe re ira Lanzoni, MD. Pro fesso r o f Department o f Patho lo gy,
Universidade Federal de São Paulo /Esco la Paulista de Medicina, São Paulo , Brazil.
Carlos Fische r de Tole do, MD. Pro fesso r o f Gastro entero lo gy Divisio n, Universidade Federal de São Paulo /Esco la Paulista de Medicina, São Paulo , Brazil.
Source s of funding: No t declared
Conflict of inte re st: No t declared
Last re ce ive d: 27 April 1999
Acce pte d: 22 September 1999
Addre ss for corre sponde nce :
Carlo s Fischer de To ledo
Departamento de Medicina, Disciplina de Gastro entero lo gia, Universidade Federal de São Paulo /Esco la Paulista de Medicina Rua Bo tucatu, 740 - 2o andar
São Paulo /SP - Brazil - CEP 04023-900 E-mail: fischer@ gastro .epm.br
p u b lis hin g in fo r m a t io n