Vanessa Rahal
ARAÇATUBA-SP
Vanessa Rahal
Teste Sensorial Quantitativo no Estudo da Sensibilidade Dentária
Decorrente de Tratamentos Clareadores
Tese apresentada à Faculdade de Odontologia do Campus de Araçatuba - Unesp, para a obtenção do Grau de ³'RXWRUHP2GRQWRORJLD´- Programa de Pós-Graduação em Odontologia, Área de concentração em Dentística.
Orientador: Prof. Adj. Dr. André Luiz Fraga Briso
ARAÇATUBA-SP
Catalogação na Publicação (CIP)
Serviço Técnico de Biblioteca e Documentação ʹ FOA / UNESP
Rahal, Vanessa.
R147u Teste sensorial quantitativo no estudo da sensibilida-‐
de dentária decorrente de tratamentos clareadores / Vanessa Rahal. -‐
Araçatuba : [s.n.], 2013 96 f. : il. ; tab. + 1 CD-‐ROM
Tese (Doutorado) ʹ Universidade Estadual Paulista,
Faculdade de Odontologia de Araçatuba
Orientador: Prof. Dr. André Luiz Fraga Briso
1. Peróxido de hidrogênio 2. Clareamento dental 3. Sensação 4. Análise quantitativa I. T.
Black D2
CDD 617.6
Dados Curriculares
VANESSA RAHAL
NASCI M ENTO 25/10/1982 - Birigui ± SP
FI LI AÇÃO Ricardo Antonio Rahal
Nilva Garcia Rahal
2001/2004 Graduação
Faculdade de Odontologia de Araçatuba ± UNESP
2007/2009 Curso de Pós-Graduação em Odontologia, área de Dentística, nível de Mestrado
Faculdade de Odontologia de Araçatuba ± UNESP
2010/2012 Obtenção dos créditos referentes ao Curso de Pós-Graduação em Odontologia, área de Dentística, nível de Doutorado
Dedicatória
Dedico esta Tese aos meus pais Ricardo e Nilva, meus maiores amigos e mestres, que me
incentivam a cada passo com muita sabedoria. Grandes guerreiros, meus maiores espelhos,
exemplos de família, honestidade, trabalho, caráter e muito amor. Deixo aqui registrada toda
minha admiração e todo o orgulho que sinto em ser sua filha! Obrigada por tudo... Nem todos
os segundos dessa vida serão tempo suficiente para que eu possa retribuir todo o cuidado e
amor de vocês!
Ao meu noivo Felipe, pelo amor e cumplicidade que me fazem seguir sempre em frente.
Minha maior certeza! Te amo muito, cada dia mais...
À minha irmã Sabrina e meu cunhado Gustavo por todo o amor e carinho e pelas horas de
lazer, conversa e descontração! Seria mais difícil sem poder contar com vocês nos momentos
difíceis!
Ao meu sobrinho João, já muito amado e esperado com muito carinho!
Aos meus avôs e avós, que de algum lugar zelam por nós e nos guiam e iluminam em cada
passo desta jornada... Amor eterno e infinito!
Muito obrigada por me ajudarem a chegar até aqui! Vocês são meus tesouros, minha base,
meu orgulho, meu porto seguro, sem o qual me perderia e minha vida deixaria de ter o sabor
adocicado que ela tem.
Agradecimento Especial
Ao meu orientador, Prof. Adj. Dr. André Luiz Fraga Briso, grande amigo e mestre, que
com sua atenção e carinho me ofereceu todo o seu precioso saber e que, de coração aberto, me
acolheu e se tornou indispensável em meu caminho acadêmico. Serei eternamente grata por
tudo o que fez por mim durante todos esses anos, colaborando com meu crescimento como
pessoa e como profissional. Obrigada por sempre estar ao meu lado e por me ajudar a superar
Agradecimentos
A Deus, que me guia em cada passo de minha vida. A Ele que nas horas difíceis me
acolhe e protege e que me dá forças para alcançar meus objetivos.
À )XQGDFmRGH$PSDURj3HVTXLVDGR(V WDGRGH6DѺR3DXOR - FAPESP, pela
FRQFHVVmRGRDX[tOLRjpesquisa, sem o qual não seria possível a realização destes trabalhos.
À Faculdade de Odontologia do Campus de Araçatuba ± UNESP, na pessoa da Ilma.
Diretora Profa. Adj. Ana M aria Pires Soubhia e Vice-Diretor Prof. Titular Wilson
Roberto Poi, pela oportunidade de realização dos meus estudos.
Ao Programa de Pós-Graduação em Odontologia, na pessoa de sua coordenadora
Profa. Adj. M aria José Hitomi Nagata.
Aos professoresdo Curso de Pós-Graduação Stricto Sensu em Odontologia da
Faculdade de Odontologia de Araçatuba ± UNESP.
Ao meu inesquecível orientador de mestrado, Prof. Adj. Dr. Renato Herman
Sundfeld, que como um verdadeiro pai me ajudou em meus primeiros passos como
pesquisadora. Sou eternamente grata por todo o seu carinho e seus ensinamentos.
Ao querido professor de Pós-Graduação, Prof. Adj. Dr. Paulo Henrique dos Santos,
Ao Prof. Ass. Dr. Luciano Tavares Angelo Cintra pela orientação e paciência
infindável na realização da análise estatística deste estudo.
Ao Prof. Dr. Reynaldo Leite M artins Júnior e à Juliana Stuginski Barbosa por
toda a colaboração durante a idealização e realização deste estudo.
À Profa. Ana Karina Bedran Russo (University of Illinois at Chicago) pela
oportunidade de estudo e aprendizado e pela hospitalidade durante o estágio no exterior.
À Profa. Adj. M aria Lúcia M arçal M azza Sundefeld por toda colaboração durante
todos estes anos.
À Profa. Cléa Adas Saliba Garbin pela sua amizade, compreensão e por todas as
suas palavras de carinho.
Ao Prof. Eloi Dezan Júnior pela grande amizade construída sob os pilares da
confiança e do carinho mútuo. Estarei sempre ao seu lado!
Aos meus professores de Dentística: Laumer Pedro Alcântara Silva e Quintella,
M ara Antônio M onteiro de Castro, Renato Herman Sundfeld, Sandra Rahal M estrener, 6LOYLR-RVHғ0DXUR, Ricardo Coelho Okida e André Luiz Fraga Briso por todo o saber que
A todos os meus queridos professores de graduação, em especial aos professores da
Disciplina deEndodontia do Departamento de Odontologia Restauradora.
A todos os funcionários e ex-funcionários do Departamento de Odontologia
Restauradora da Faculdade de Odontologia de Araçatuba ± UNESP, pelo carinho e momentos
de descontração durante todos esses anos.
Aos queridos amigos de pós-graduação Letícia Cunha Amaral Gonzaga de
Almeida, Ana Paula Albuquerque, Fernanda Garcia de Oliveira e Lucas Silveira
M achado, por todos estes anos de companheirismo e amizade.
Às queridas amigas M arjorie de Oliveira Gallinari e Fernanda Almeida de
Azevedo, por cada dia de ajuda durante a realização deste trabalho e também por todo o
carinho durante esses anos.
Aos estagiários e amigos do Departamento de Odontologia Restauradora Naiara
M ontes, Ana Paula Pereira, Ana Paula Lima, Clícia Ribeiro, Gustavo Arcos, Francine
Benetti, M ariana Campos Hidelbrand, M ariana Fioravante, Fernanda Bernardi e
Laércio Neves M arcon pelos momentos de conversa, risadas e também de estudo.
Aos amigos Rafael Simões Gonçalves, Laura M olinar Franco, André Gustavo de
Lima Godas, Diego Valentim e Aguinaldo Cândido da Silva Facundo pela amizade epor
todos os momentos de estudo e descontraçãodurante a realização deste trabalho e de todos os
Aos meusqueridos pacientes que tornaram possível a realização deste estudo.
A todos osfuncionários da Seção de Pós-Graduação da Faculdade de Odontologia de
Araçatuba ± UNESP, Valéria, Lilian, Diogo, Cristiane e Joilson pela amizade, atenção e
pela paciência.
Aos bibliotecários da Faculdade de Odontologia de Araçatuba ± UNESP, em especial
à Ana Claudia pela colaboração durante todo o período de redação deste trabalho.
Aos meus familiares, em especial à minha tia M aria Eli (Lili), pelo carinho, amor e
cuidados desde o meu nascimento até os dias de hoje.
À minha segunda família, já tão amada: M aria do Carmo, Claudecir, Guilherme,
Tio Tonho, Tia Lu, Leda, Lara, Júnior, Tio Júnior, Tia M ari e Laura.
À minha querida avó que a vida me deu de presente, Dona Cida, por todo o carinho e
amor.
Às minhas amigas de todos os dias, Camila e Dayana, que não mediram esforços para
me ajudar a chegar até aqui.
A todos os meus amigos e àqueles que direta ou indiretamente contribuíram durante
RAHAL V. Teste Sensorial Quantitativo no Estudo da Sensibilidade Dentária Decorrente de
Tratamentos Clareadores [tese]. Araçatuba: Faculdade de Odontologia de Araçatuba da
UniveUVLGDGH(VWDGXDO3DXOLVWD³-~OLRGH0HVTXLWD)LOKR´.
Resumo Geral
Depois de reconhecido como uma terapia esteticamente eficaz, o clareamento dental tem sido
comumente procurado pela maioria dos pacientes na busca por um sorriso mais harmonioso e
agradável. No entanto, o surgimento da sensibilidade dentária em decorrência do uso de
peróxidos faz com que muito pacientes tornem-se insatisfeitos com o tratamento clareador.
Neste contexto, estudos relacionados a essa sintomatologia são frequentes, porém, baseados
em metodologias limitadas e imprecisas. Por isso, torna-se necessário empregar um método
recente no campo odontológico a fim de enriquecer cientificamente as análises de
sensibilidade dentária. Objetivos: Assim, o presente estudo objetivou analisar e quantificar a
ocorrência de sensibilidade dentária por meio do Teste Sensorial Quantitativo (QST) com a
utilização de um equipamento de análise neurosensorial em diferentes momentos do
tratamento clareador e mesmo após o uso de dessensibilizantes. Além disso, relacionar o
limiar de sensação dos pacientes com tal ocorrência para que se estabeleça um protocolo de
indicação individual adequado. Materiais e Métodos: Inicialmente, sessenta voluntários foram
divididos em 4 grupos de acordo com o limiar de sensação da pele (baixo - GI e GIII e alto -
GII e GIV), classificado por meio do QST, e o tratamento clareador (peróxido de hidrogênio -
GI e GII e placebo - GIII e GIV). A sensibilidade dental mensurada por meio do QST, em 10
tempos de estudo. Como estudo complementar, foi realizada a segunda etapa desta pesquisa,
onde os dez pacientes restantes receberam o tratamento clareador com peróxido de hidrogênio
dessensibilizante tópico no hemiarco esquerdo da maxila. No hemiarco direito foi aplicada
uma solução salina a temperatura ambiente (controle). O QST foi realizado antes do
clareamento (AC), imediatamente depois do clareamento (DC) e imediatamente após a
aplicação do dessensibilizante (DD). Resultados: Como resultado da primeira etapa desse
estudo, foram verificadas respostas distintas de sensibilidade nos pacientes de baixo e alto
limiar sensitivo GD SHOHGXUDQWH D SULPHLUD H WHUFHLUD VHVV}HV FODUHDGRUDV SPor sua
vez, no estudo complementar o tratamento clareador promoveu o aumento da sensibilidade
dental, sendo esta ainda presente mesmo após o uso da solução salina. No entanto, com a
aplicação do dessensibilizante, a sensibilidade dental foi reduzida Conclusões: Com base nos
resultados obtidos em nossos estudos, concluímos que o limiar de sensação em pele pode
representar um fator determinante na ocorrência de sensibilidade dental exacerbada pelo
tratamento clareador. Além disso, o uso do dessensibilizante após o clareamento dental
mostrou-se efetivo ao reverter esta condição.
Palavras-chave: Peróxido de Hidrogênio. Clareamento Dental. Sensação. Análise
Quantitativa.
RAHAL V. Dental Sensitivity Assessment During Dental Bleaching Using Quantitative
sensory testing [thesis]. Araçatuba: UNESP ± Univ Estadual Paulista; 2013.
Abstract Geral
After being considered as an esthetically efficient technique, dental bleaching has been
frequently sought by patients that look forward to a harmonious and pleasant smile.
Nevertheless, dental sensitivity due to the use of peroxides makes patients become very
unsatisfied with the bleaching treatment. In this context, studies related to this issue are very
common, but based on limited and inaccurate methodologies. Therefore, we improved a
recent method in dentistry in order to contribute to the enrichment of these scientific analyses.
Objectives: Hence, the present study aimed to perform a Quantitative Sensory Testing (QST),
using a neurosensory analyzer to verify and quantify the occurrence of dental sensitivity, in
different periods of evaluation, during bleaching treatment and after the use of a desensitizer
DJHQW$GGLWLRQDOO\ZHUHODWHGWKHSDWLHQWV¶sensation threshold with this occurrence in order
to establish an appropriate personal protocol statement. Materials and Methods: Seventy
volunteers were criteriously selected and sixty from them were divided into 4 study groups
according to the skin cold sensation threshold (low - GI and GIII and high - GII and GIV),
obtained using QST, and the bleaching treatment (hydrogen peroxide - GI and GII and
placebo - GIII e GIV). After the classification according to the skin cold sensation threshold,
bleaching treatment was performed and dental cold sensation threshold was measured using
QST in 10 different times. As a complementary study, we conducted the second part of this
research. Ten patients underwent bleaching treatment using 35% hydrogen peroxide
(Whiteness HP Maxx). After the bleaching session, a topical desensitizer was applied to the
teeth of the left maxillary hemi-arch. A saline solution at ambient temperature was applied in
immediately after bleaching (AB), and immediately after the desensitizer (AD). Results: In
the first part of the study, distinct responses of dental sensitivity were found in patients with
high and low sensitive thresholds during the first and WKLUGEOHDFKLQJVHVVLRQS. On the
other hand, in the complementary study, bleaching treatment promoted dental sensitivity,
which remain the same even before the saline solution application. However, results revealed
a reduction of dental sensitivity after desensitizing application. Conclusions: Based on these
results, we can conclude that skin cold sensation might represent a determining factor in the
occurrence of dental sensitivity enhanced by the bleaching treatment. Furthermore, the use of
a desensitizing agent after this procedure was effective to revert this condition.
D = nível de significância / significance level
ºC = graus Celsius / degree Celsius
% = porcentagem / percentage
> = maior que / higher than
= menor ou igual a / lower or equal to
= = igual / equal
1st = first
2nd = second
3rd = third
AB = after bleaching
AC = antes do clareamento
AD = after desensitizer
a.m. = ante meridien (antes do meio-dia)
BB = before bleaching
CST = Cold Sensation Threshold
DC = depois do clareamento
DD = depois do dessensibilizante
DP = Desvio Padrão
et al. = e colaboradores
GI = grupo I
GII = grupo II
GIII = grupo III
GIV = grupo IV
HP = Hydrogen Peroxide
Ltd. = Limited
Ltda. = Limitada
ml = mililitro / mililiter (unidade de medida equivalente a 10-3l) mm = milímetro / milimeter (unidade de medida equivalente a 10-3m) n = tamanho da amostra do grupo / group sample size
NaCl = Sodium Chloride
P = evaluation period
pH = Potencial Hidrogeniônico / Hydrogen Potential
QST = Quantitative Sensory Testing
SD = Standard Deviation
SCST = Skin Cold Sensation Threshold
UNESP = Universidade Estadual Paulista ³-~OLRGH0HVTXLWD)LOKR´
CAPÍ TULO 1
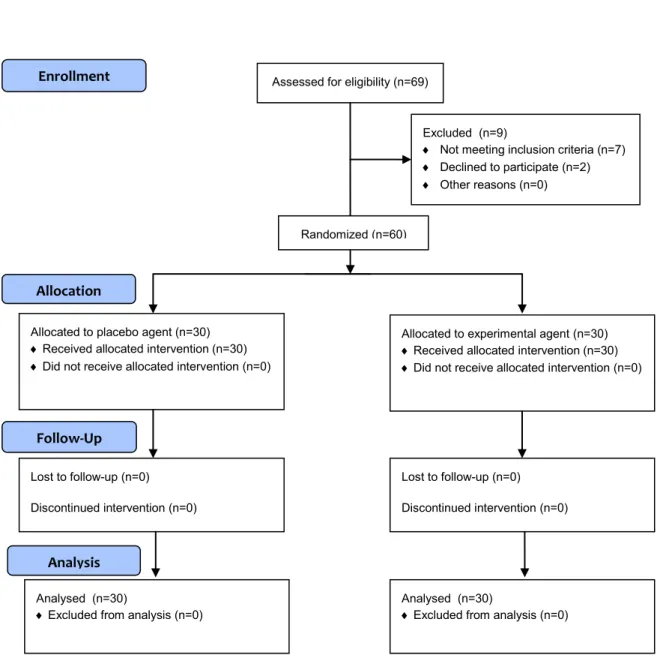
Figure 1: Flow chart diagram detaching the enrollment, allocation, follow-up and analysis during the study (CONSORT Statement).
39
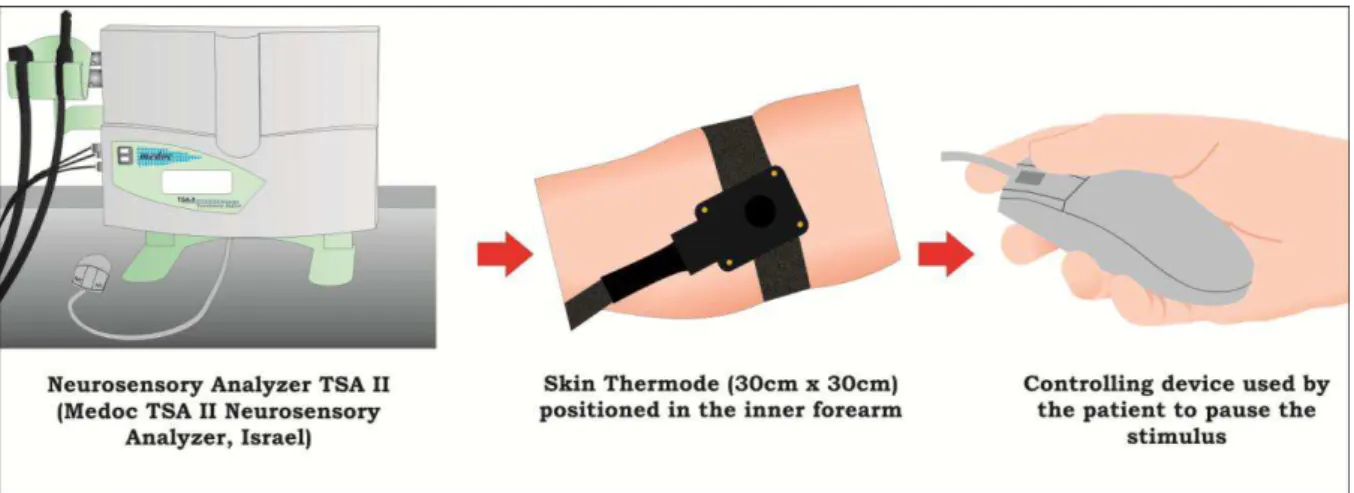
Figure 2: Scheme of the skin neurosensory analysis using the equipment TSA II. 40
Figure 3: Individual perforated tray confectioned to standardize the dental region to be measured.
41
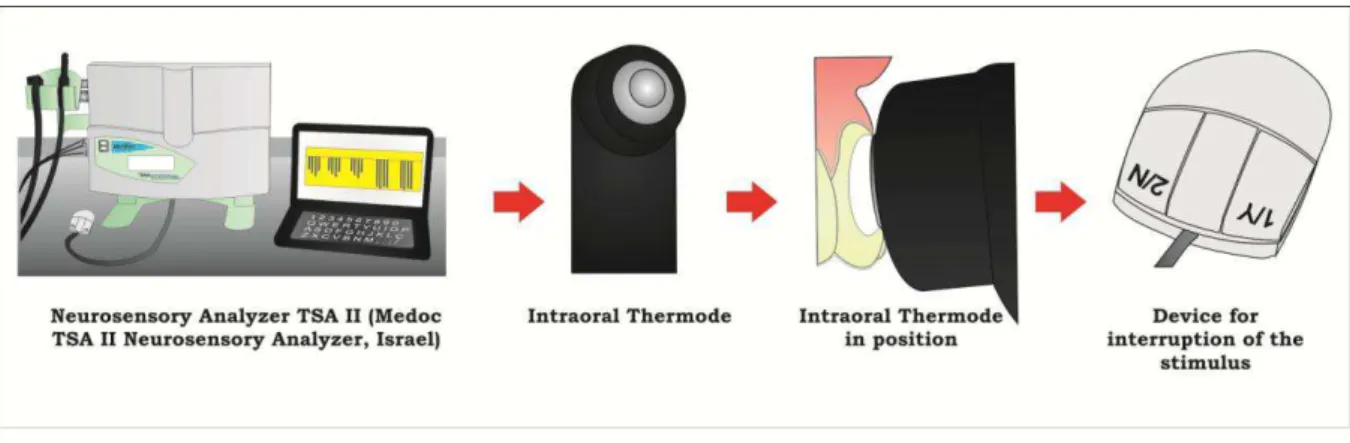
Figure 4: Scheme of the tooth neurosensory analysis using the equipment TSA II. 42
CAPÍ TULO 2
Figure 1: Flow chart diagram detaching the enrollment, allocation, follow-up and analysis during the study (CONSORT Statement).
68
Figure 2: Scheme of the neurosensory analysis using the equipment TSA II. 69
Figure 3: Data of cold sensation threshold in the right and left hemi-arches during the periods of evaluation.
CAPÍ TULO 1
Table 1: Inclusion and exclusion criteria for selection of patients. 43
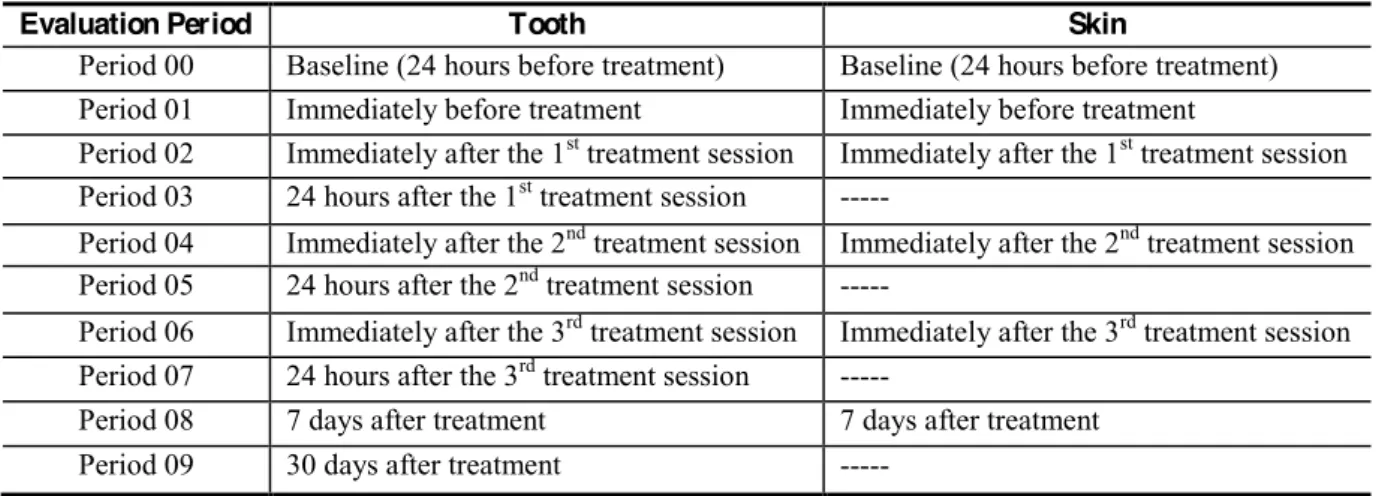
Table 2: Evaluation periods of the skin and dental cold sensation threshold. 44
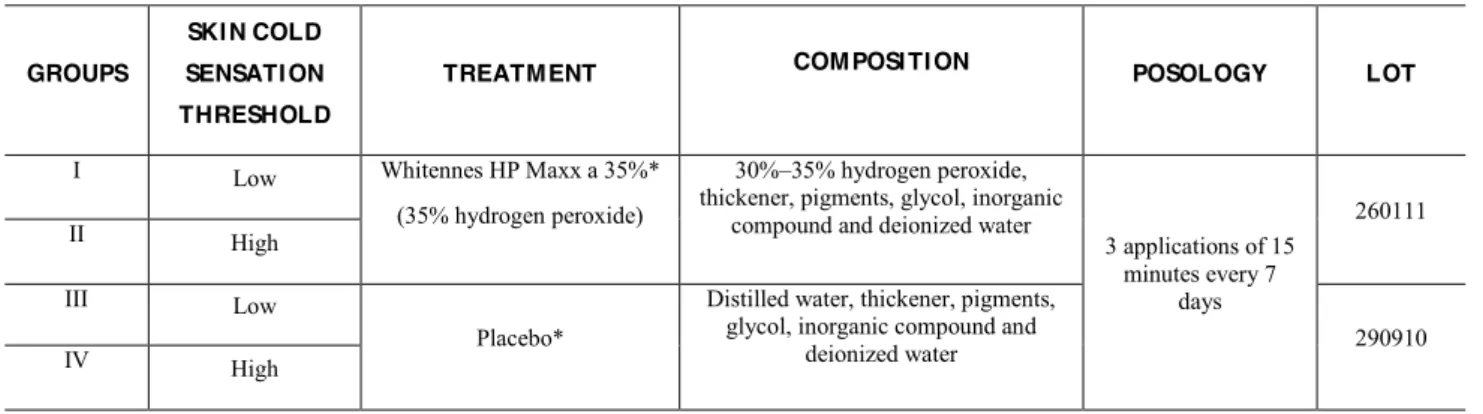
Table 3: Study groups and experimental and placebo products composition. 45
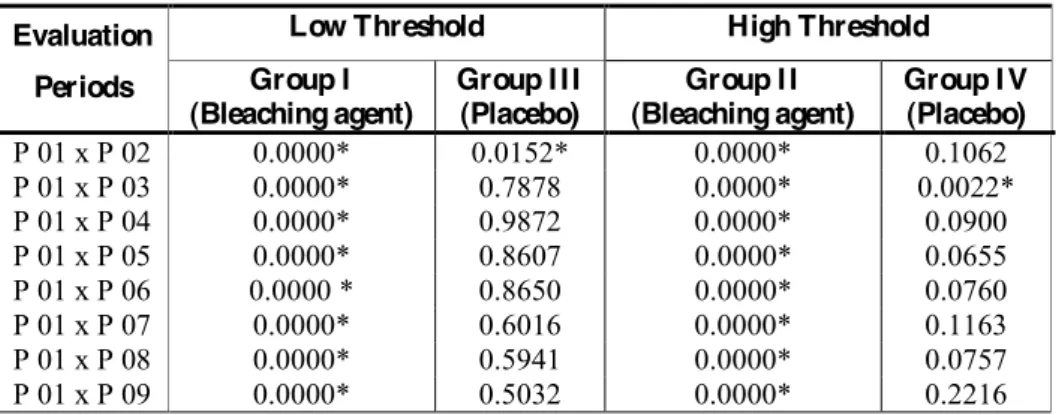
Table 4: P. values obtained after dental cold sensation evaluation in different periods.
46
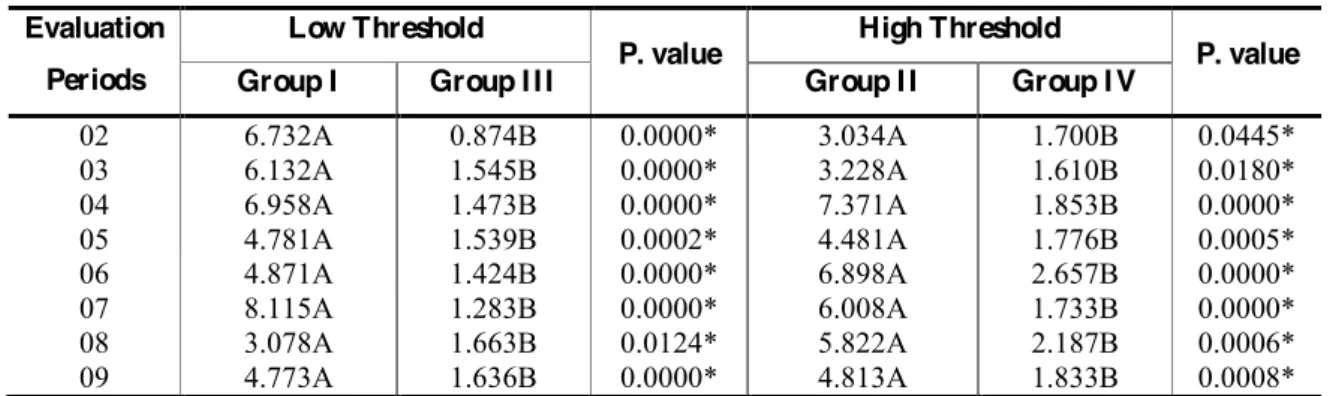
Table 5: Temperature variations for cold sensation (oC) in different evaluation periods, after the beginning of dental bleaching.
47
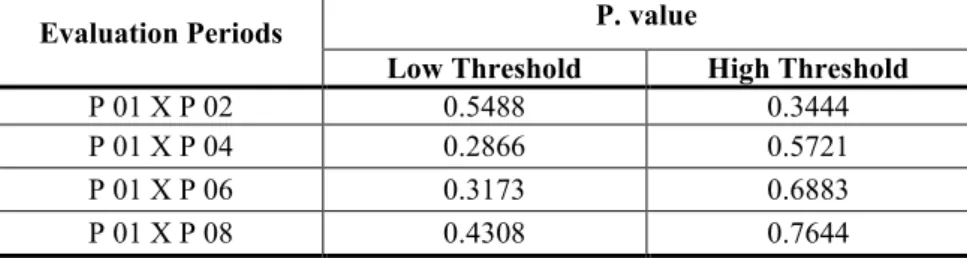
Table 6: P. values obtained after skin cold sensation threshold evaluation in different periods.
48
Table 7: Temperature variations for dental cold sensation (oC) of experimental groups with low and high threshold.
49
CAPÍ TULO 2
Table 1: Inclusion and exclusion criteria for selection of patients. 71
Table 2: Treatment according to the split-mouth design method. 72
Table 3: Composition of the products used in this study. 73
Table 4: Mean temperatures and standard deviation of cold sensation threshold (oC) in right and left hemi-arches.
1 Introdução geral 18
2 Capítulo 1 ± I nfluence of cold sensation threshold in the occurrence of dental sensitivity during dental bleaching: a placebo controlled clinical trial
21
2.1 Resumo 21
2.2 Abstract 22
2.3 Introdution and proposition 23
2.4 Materials and Methods 25
2.5 Results 29
2.6 Discussion 30
2.7 Conclusion 33
2.8 Acknowledgements 34
2.9 References 35
3 Capítulo 2 ± Quantitative Sensory Testing of the effect of desensitizing treatment after dental bleaching
50
3.1 Resumo 50
3.2 Abstract 51
3.3 Introduction and proposition 52
3.4 Materials and Methods 55
3.5 Results 59
3.6 Discussion 60
3.7 Conclusion 62
3.8 Acknowledgements 63
3.9 References 64
1 Introdução Geral
*A busca por tratamentos estéticos nos consultórios odontológicos é cada vez mais
frequente. Dentre os procedimentos que visam melhorar a aparência e a autoestima dos
pacientes (POLYDOROU et al., 2007) destaca-se o clareamento dental, que se caracteriza por
ser uma técnica conservadora capaz de proporcionar resultados impactantes, satisfazendo os
anseios dos pacientes e também de muitos profissionais (DIETSCHI et al., 2006; MATIS et
al., 2007; PARK et al., 2004).
Desde que proposto, o clareamento caseiro foi considerado uma terapia reconhecida
como tecnicamente simples, biologicamente segura e esteticamente eficaz (DIETSCHI, 2005;
DIETSCHI et al., 2006; HAYWOOD & HEYMANN, 1991; LEONARD et al., 1997; PARK
et al., 2004), quando bem indicada e sob adequada supervisão do profissional em
Odontologia.
Recentemente, novas técnicas foram desenvolvidas, como o tratamento de consultório
(in-office), que emprega produtos à base de peróxidos altamente concentrados diretamente
sobre a superfície de esmalte. A possibilidade de obtenção de resultados rápidos e a não
necessidade do incômodo uso das moldeiras são os principais apelos mercadológicos da
técnica, que tem agradado profissionais e pacientes (DOS SANTOS MEDEIROS et al., 2008;
PARK et al., 2004). Seu mecanismo de ação baseia-se na presença de formas reativas de
oxigênio, que, por serem extremamente instáveis, promovem oxidação dos pigmentos
incorporados nos tecidos dentais, tornando-os mais claros (CALLAN et al., 2008; DELFINO
et al., 2009; DIETSCHI et al., 2006; MYERS et al., 2003; USHIGOME et al., 2009).
Apesar da eficácia clareadora, estudos relatam a presença de sensibilidade dentária em
70% dos pacientes tratados, o que pode prejudicar a continuidade do tratamento ou causar
*
uma redução no sentimento de satisfação (BROWNING et al., 2007; KUGEL et al., 2009;
MONCADA et al., 2013).
Neste contexto, a maioria dos estudos clínicos sobre a ocorrência de sensibilidade
durante o clareamento apresenta dados coletados através de relatos de experiência e
questionários de dor, fazendo com que haja o surgimento de um viés de interpretação
referente aos dados coletados, afetando a confiabilidade dos resultados obtidos e
reprodutibilidade do método (BROWNING et al., 2007; CALLAN et al., 2008; KUGEL et
al., 2009).
Alguns estudos que avaliaram clinicamente a intensidade da sensibilidade dental
(BROWNING et al., 2007; LEONARD et al., 1997; MACHADO et al., 2013), mostram que a
ocorrência da sensação dolorosa varia muito de indivíduo para indivíduo e tende a ser mais
intensa no final do tratamento. Esta variação individual pode estar de alguma forma associada
ao limiar de dor ou de sensação de cada pessoa, que podem apresentar respostas distintas
frente a um estímulo de mesma intensidade, independentemente das características clínicas
bucais que cada pessoa apresenta.
Vale destacar que o limiar de dor pode ser definido como o ponto ou momento em que
um dado estímulo é reconhecido como doloroso. Este ponto que provoca a dor, ou mesmo
inicia um processo de desconforto é mais facilmente detectado em alguns pacientes, podendo
ser classificados como indivíduos com limiar de dor baixo. Do contrário, o limiar de dor alto
seria atingido mais dificilmente. Já o limiar de sensação é definido como o momento em que o
estímulo é percebido ou detectado pelo paciente e pode também ser classificado em alto e
baixo (AFFAITATI et al., 2009; GRANGES et al., 1993; STAUD et al., 2011).
O mercado de produtos relacionados à ciência da dor possui hoje equipamentos
modernos e eficientes que permitem quantificar sintomas dolorosos, por meio de análises
PAVLAKOVIC et al., 2008; PIGG et al., 2010). Um desses equipamentos, o TSA-II (Medoc
Advanced Medical Systems Ltd., Ramat Yishai, Israel), fornece dados precisos sobre limiar
de dor e limiar de sensação. O maior diferencial desta tecnologia é a possibilidade de
quantificar a resposta neurosensorial de fibras nervosas maiores e menores (LIST et al., 2009;
PAVLAKOVIC et al., 2008; PIGG et al., 2010), enquanto outros equipamentos permitem
apenas a análise baseada em fibras mais grossas (SIAO et al., 2003). Esta informação é de
grande importância, já que as fibras mielínicas sensitivas mais grossas (AE) perfazem apenas
7% da totalidade das fibras mielínicas pulpares (NAIR et al., 1992). As principais fibras de
condução sensitiva encontradas no tecido pulpar são as fibras mielínicas (A) e amielínicas
(C) que transmitem a sensação térmica ao sistema nervoso central (SACERDOTE et al.,
2012).
Testes de sensibilidade ao frio e ao calor podem ser realizados com o uso do TSA-II,
por meio do termode, que permite aquecimento e resfriamento em diferentes tempos e
temperaturas (GRANOT et al., 2005; KALANTZIS et al., 2007). Por este motivo, almeja-se
que o estudo simultâneo do limiar de sensação e da sensibilidade dentária frequentemente
presente nos tratamentos clareadores, possibilite aos clínicos um novo parâmetro para a
indicação de terapias prévias e de combate à sensibilidade no caso do tratamento de pacientes
predispostos a tal ocorrência. Além disso, esses novos conhecimentos podem auxiliar o
profissional na indicação da terapia clareadora mais adequada a cada indivíduo.
Diante do exposto, nossos estudos clínicos do tipo cego fatorial randomizado
controlado buscam quantificar a ocorrência de sensibilidade dental antes, durante e após o
tratamento clareador levando em consideração o limiar de sensação em pele de cada paciente
e visando, ainda, a prevenção dessa sensibilidade por meio de tratamentos dessensibilizantes
2 Capítulo 1
I nfluência do limiar sensitivo na ocorrência de sensibilidade dentária durante o
clareamento: ensaio clínico controlado
QST: Limiar sensitivo e sensibilidade dentária
2.1 Resumo
O presente estudo verificou a ocorrência de sensibilidade dental em pacientes submetidos ao
procedimento clareador realizado com 3 aplicações de 15 minutos do peróxido de hidrogênio
a 35% (Whiteness HP Maxx 35% - FGM), a ocorrência de variação no limiar sensitivo em
pele de cada um e o papel deste limiar na ocorrência da sensibilidade dentária. Para tanto,
sessenta voluntários foram divididos em 4 grupos de estudo (n=15) de acordo com o limiar de
sensação da pele (baixo ± GI e GIII e alto ± GII e IV) e o tratamento clareador (peróxido de
hidrogênio ± GI e GII e placebo ± GIII e GIV). O limiar de sensação da pele foi determinado
no antebraço dos pacientes em 6 diferentes tempos de estudo, por meio de estímulos térmicos
produzidos pelo equipamento de análise neurosensorial, o TSA II. Após a classificação dos
pacientes de acordo com o limiar sensitivo, o tratamento clareador e placebo foram realizados.
A sensibilidade dental foi então mensurada em 10 tempos de estudo por meio de um
dispositivo intraoral acoplado ao TSA II e posicionado na face vestibular do incisivo superior.
Foram verificadas respostas distintas de sensibilidade nos pacientes de baixo e alto limiar
sensitivo GDSHOHGXUDQWHDSULPHLUDHWHUFHLUDVHVV}HVFODUHDGRUDVSAlém disso, os
dentes submetidos ao clareamento se tornaram mais sensíveis ao frio do que os tratados com o
placebo. O limiar de sensação em pele permaneceu inalterado durante todo o experimento.
Concluiu-se que o limiar de sensação da pele pode representar um fator determinante na
ocorrência de sensibilidade dental, já que os pacientes de limiar sensitivo em pele alto e baixo
responderam de maneiras distintas frente ao estímulo térmico em dente. Significância Clínica:
O estudo da sensibilidade durante o clareamento dental relacionada ao limiar sensitivo em
pele pode auxiliar os profissionais a estabelecer um protocolo adequado de clareamento e de
terapias dessensibilizantes prévias e posteriores ao tratamento, considerando a predisposição à
sensibilidade dentária em pacientes de diferentes limiares sensitivos em pele (alto e baixo).
I nfluence of cold sensation threshold in the occurrence
of dental sensitivity during dental bleaching: a placebo controlled clinical trial
QST: Sensation threshold and dental sensitivity
2.2 Abstract
The present study verified the occurrence of dental sensitivity in patients submitted to 3
15-minute applications of a 35% hydrogen peroxide based product (Whiteness HP Maxx 35% -
FGM), the skin cold sensation threshold (SCST) occurrence and its influence on dental
sensitivity. Sixty volunteers were divided into 4 study groups (n=15), according to the SCST
(low ± GI and GIII and high ± GII and IV) and bleaching treatment (hydrogen peroxide ± GI
and GII and placebo ± GIII and GIV). SCST was determined in the inner forearm in 6
different times using a neurosensory analyzer, the TSA II (Medoc Advanced Medical
Systems, Ramat Yishai, Israel). Dental sensitivity measurements were performed in 10
different times using TSA II attached to an intraoral device, positioned in the buccal surface
of the teeth. Distinct responses of dental sensitivity were found in patients with high and low
SCST GXULQJ WKH ILUVW DQG WKLUG EOHDFKLQJ VHVVLRQ S DQG WKH WHHWK VXEPLWWHG WR WKH
bleaching treatment became more sensitive to cold than those treated with placebo. SCST
remained the same during bleaching treatment. Bleaching agent increased dental sensitivity
and the skin cold sensation threshold might represent a determining factor in this occurrence,
since low and high SCST patients had different responses to the thermal stimulus in tooth.
Clinical Significance: The study of dental sensitivity during dental bleaching considering skin
cold sensation threshold may enable professionals to establish an adequate dental bleaching
protocol and even adequate prior and posterior desensitizing therapies, considering the
predisposition to dental sensitivity in patients of different skin cold sensation threshold (low
and high).
2.3 I ntroduction
Tooth bleaching is one of the most popular esthetic procedures requested by patients
and a conservative approach with efficient results.1-4 The in-office technique using highly
concentrated hydrogen peroxide products has become an excellent alternative for both
professionals and patients.5-7 Its mechanism of action is similar to the at-home technique,
which is based on unstable reactive oxygen species that lighten tooth pigments through
oxidation.1,8
Despite the whitening efficacy, recent studies showed that patients submitted to dental
bleaching reported different intensities of dental sensitivity.9-12 This symptom is a concern for
dentists and patients as a limitation for treatment evolution and satisfaction.
Some clinical trials about dental sensitivity showed that pain is different between
individuals and it is usually stronger at the final phase of treatment.10,13 This variation may be
associated to the sensation threshold of each patient, which is classified as low when cold
sensation is easily detected and high in the opposite situation.
TSA II (Medoc Advanced Medical Systems, Ramat Yishai, Israel) 8,14-17 represents a
modern technology for quantification of neurosensory response related to major and minor
nervous fibers3 through Quantitative Sensory Testing (QST) using thermal, mechanical, or
electrical stimuli.
Thus, test for cold and heat sensation can be conducted using accurate devices that
transfer temperature changes to several body structures under predetermined speed.18,19 In this
sense, a simultaneous study for skin sensation threshold and dental sensitivity experienced
during whitening would provide clinical safety levels to prevent and treat this side effect.
Ώ Normalização segundo a revista Operative Dentistry (Anexo C).
The aim of the present study was to verify the influence of the skin cold sensation
threshold in dental sensitivity using the neurosensory analysis to quantify thermal sensitivity
during dental bleaching.
The null hypothesis assumed that:
- there is no difference in dental sensitivity at different periods during bleaching with 35%
hydrogen peroxide products,
- there is no difference in skin cold sensation threshold during bleaching with 35% hydrogen
peroxide products,
- skin cold sensation threshold of each patient does not influence dental sensitivity during
2.4M aterials and M ethods
Experimental Design
After approval by the Committee of Ethics in Research (00278/2011), 60 male patients
aged from 18 to 25 years were selected according to the criteria shown in Table 1. The
patients were carefully evaluated and submitted to anamnesis and appropriate clinical and
radiographic exams before allocation (Figure1).
This placebo-controlled, blind and factorial clinical trial with equal randomization
included the factors: (1) bleaching treatment in 2 levels (35% hydrogen peroxide and
placebo); (2) skin cold sensation threshold in 2 levels (low and high) and (3) 10 evaluation
periods (Baseline ± 24 hours before treatment; immediately before treatment; immediately
after the 1st treatment session; 24 hours after the 1st treatment session; immediately after the
2nd treatment session; 24 hours after the 2nd treatment session; immediately after the 3rd
treatment session; 24 hours after the 3rd treatment session; 7 and 30 days after the treatment
(Table 2).
It is noteworthy that patients were also instructed no to use analgesic or
anti-inflammatory medications and desensitizing toothpastes during and 30 days after the
bleaching treatment in order to avoid misreading of data.
Quantitative Sensory Testing (QST) ± Skin Cold Sensation Threshold
Skin cold sensation threshold was firstly performed in order to divide the patients
according to experimental or placebo treatment.
The first measurement of skin cold sensation threshold was performed using the
and its skin probe (30 mm x 30 mm), in a silent environment with a constant temperature of
26º C. The sessions were conducted from 8:00 a.m. to 10:00 a.m..
7KH76$,,ZDVFRQILJXUHGXVLQJWKH³/LPLWV´IXQFWLRQDQGWKHWHVWRIFROGVHQVDWLRQ
thresholds (CST) was used for this purpose. Three descending temperature tests were
performed in the inner forearm. The test began at 32 oC (comfort temperature), and the
thermode cooling speed was 1 ºC per second. After patient perception of temperature
alteration, the patient paused the stimulus, and the measurement was repeated for two times,
30 seconds after the previous one (Figure 2).
The values obtained during the first test were discarded, and the mean of the following
tests was used as the temperature for cold sensation threshold testing in skin.
The mean temperature was considered the skin cold sensation threshold and was used
to classify patients in low or high skin cold sensation threshold.
Measurements were performed in different periods according to Table 2.
Quantitative Sensory Testing (QST) ± Dental Cold Sensation Threshold
For standardization of tooth analysis, a 100% ethylene copolymer and vinyl acetate
tray was fabricated for each patient. The tray had a circular perforation with a diameter
similar to the active tip of the intraoral thermode. The perforation was created on the buccal
surface and 2 mm below the cervical, incisal, and proximal margins of the upper right central
incisor (Figure 3).
Quantitative Sensory Testing (QST) for dental cold sensation thresholds was
conducted using an intraoral device of 6 mm diameter connected to TSA II. It was always
positioned in the same area, within the circular perforation of the tray, in the flattest region of
Before measurement, the tooth was covered with thermal paste containing silver oxide
(IPT - Pasta Térmica Implastec, Implastec Eletroquímica Ltd., Votorantim, São Paulo, Brazil)
to optimize thermal conduction. The tests were performed in the same conditions previously
reported.
The patients were able to stop cooling of the intraoral thermode at any time using the
device in their hands. The test began at 36 oC, and the thermode cooling speed was 0.5 ºC per
second, resulting in slow temperature variation that allowed transference of the thermal
stimulus to the dentine-SXOS FRPSOH[ 7KH 76$ ,, ZDV FRQILJXUHG XVLQJ WKH ³/LPLWV´
function, and the test of cold sensation thresholds (CST) was used for this purpose. Three
descending temperature tests were performed. After patient perception of temperature
alteration, the patient paused the stimulus, and the measurement was repeated for two times,
30 seconds after the previous one. The values obtained during the first test were discarded,
and the mean of the following tests was used as the temperature for cold sensation threshold
testing in tooth.
Dental cold sensitivity measurement was performed for both study groups in
predetermined evaluation periods (Table 2).
Treatments performed
Once the patients were classified according to the skin cold sensation threshold (low
cold sensation threshold were the ones who detected thermal sensation up to 30 oC and high
cold sensation threshold, the ones who detected thermal sensation below 30 oC), the in-office
bleaching technique using 35% hydrogen peroxide (Whiteness HP Maxx, FGM Produtos
Odontológicos ± Ltda., Joinville, Santa Catarina, Brazil) was performed in patients in groups
system (one bottle contains the peroxide and the other contains the activator), and the
substances are mixed in a peroxide/activator ratio of 3:1 drops.
After tooth prophylaxis and soft tissue isolation using a light cured resin gingival
barrier (Top Dam ± FGM Produtos Odontológicos Ltda., Joinville, Santa Catarina, Brazil),
the bleaching agent was inserted into a graduated syringe, and 0.06 ml of the bleaching
product was applied on the buccal surface of the teeth for 15 minutes. After the first
application, the teeth were cleaned and dried with gauze, and the procedure was repeated
twice, totalizing 45 minutes of contact between the bleaching product and enamel in each
session. After 7 and 14 days the same procedure was performed.
In groups I I I and I V, a placebo agent, identical to the original bleaching agent
presentation, purchased from the same manufacturer, was applied to the dental surface the
same way as reported for the bleaching agent (Table 3). Patients were not informed of the
group to which they belonged.
Statistical Analysis
Temperature variations (delta) were used to perform the statistical analysis. They were
obtained by subtracting the initial temperatures/baseline from those found in the other periods
of study.
'DWDZDVVXEPLWWHGWR6WXGHQW¶VW-test at a 5% level of significance using Pacotico 5.1
2.5 Results
The values of dental cold sensation in the bleached groups (Groups I and II) were
statistically different from the initial values (SIn groups treated with placebo (Groups
III and IV), cold sensation remained the same during the study (p>0.05), except for P 02 in
JURXS,,,SDQGP 03 in group IV (Table 4).
It was also observed that temperature variations for cold sensation in the bleached
JURXSZHUHVWDWLVWLFDOO\GLIIHUHQWLQFRPSDULVRQWRSODFHERLQDOOSHULRGVSUHJDUGOHVV
the skin cold sensation threshold (Table 5). Data revealed stronger dental sensitivity during
bleaching with 35% hydrogen peroxide compared to placebo.
For the analysis of skin cold sensation threshold during dental bleaching, no statistical
difference was found between the periods (p>0.05) (Table 6).
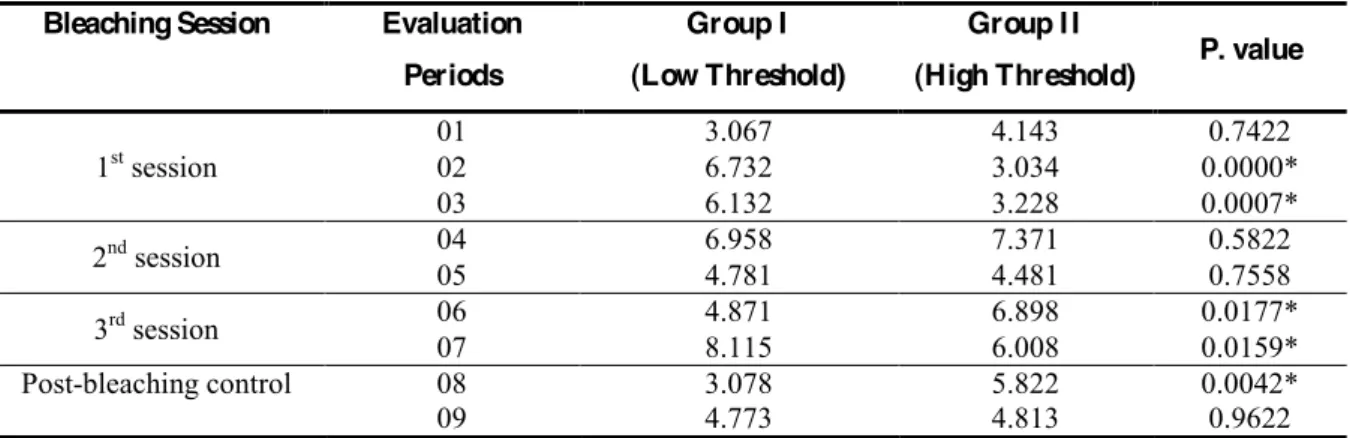
The influence of skin cold sensation threshold on dental cold sensation was evaluated
through comparison of temperature change (delta) for cold sensation in the maxillary central
incisor of experimental groups with low and high threshold. Statistically significant
2.6 Discussion
The Quantitative Sensory Testing (QST) used in this study to measure dental cold
sensation during whitening has been used in several fields for pain evaluation.1,20-22 Among
all devices applied for this technique, the neurosensory analyzer (TSA II) provides
reproducible and reliable tests mainly when conducted by a single operator and associated to
SDWLHQW¶VFROODERUDWLRQ5,9,23,24
This analysis allows evaluation of thick and thin myelinated and unmyelinated
fibers,1,19 which is noteworthy in Dentistry since different types of fiber penetrate into the
apical foramen.15
The test ³Limits´DYDLODEOHLQWKHGHYLFHVRIWZDUHZDVXVHGEHFDXVHLWLVUHSURGXFLEOH
and well tolerated by the patient.25 This characteristic is important since a time-consuming
analysis causes stress and data inaccuracy.
Since the influence of repeated testing in the same tooth should be also considered, an
interval between trials must be established to avoid windup. In the present study, a 30-second
interval was waited between the measurements to reestablish a comfortable temperature. Slow
temperature change was conducted to reach the dentine-pulp complex.
Based on the present results, the first null hypothesis was rejected since the
temperature for dental cold sensation was different during treatment. Previous studies
evaluating dental sensitivity through self-reports and questionnaires with Analogue Visual
Scale are in accordance with the present results.10,13,26 However, the dental cold sensation
threshold remained unaltered in the groups treated with placebo (III and IV), which justifies
its use in the study. The alterations in those groups were observed at P 02 (low threshold) and
P 03 (high threshold) and may be associated to stress and to the placebo response associated
It is noteworthy that its was verified the presence of dental cold sensation even 7 days
after finishing the bleaching treatment. It has been demonstrated that bleaching agents cause
histomorphological alterations in enamel8,28,29 and the present results suggested that some of
those modification persisted over time. The product pH and its action on enamel proteins may
have increased the diffusion channels and tissue permeability, influencing the response to
thermal stimulus.6,12,28,30 In addition, penetration of peroxide into dental pulp may cause
structural damage and inflammation with more inflammatory cells and interruption of
odontoblasts layers as a result of reversible pulpitis.3,12,31,32 On the other hand, 30 days after
finishing the treatment, there was no incidence of dental cold sensation threshold alterations.
The second null hypothesis was accepted since whitening did not change the skin cold
sensation threshold. The skin threshold changes during specific situations, such as systemic
disease and ageing.2 Thus, sample standardization regarding health condition, gender and age
should be established since those factors may influence the results.2,7,33
On the other hand, it plays an essential role in dental sensitivity since those individuals
with high and low skin cold sensation thresholds showed different behavior during the 1st and
3rd sessions of the treatment. In those cases, the skin threshold influenced clinical tooth
response, representing different tolerance levels against thermal stimuli on tooth.2 Thus, the
third null hypothesis was also rejected.
These periods are coincident to the ones in which our patients reported increased
incidence of dental sensitivity and also corroborate with previous studies where, especially at
the beginning and end of the bleaching treatment, cold sensations become exacerbated.13,35
In this context, though the sensitivity has a very negative impact on satisfaction, this
undesirable symptom was not sufficient to cause the discontinuance or interruption of
In general, the neurosensory analysis with TSA II in tooth is beneficial for
Dentistry since knowledge about bleaching side effects30,34,35 is relevant for development of
safe and comfortable protocols. These data also provide practitioners with a better estimate of
what their patients are likely to experience. Otherwise, further investigations are necessary to
improve this method of quantitative analysis of cold sensation in tooth, which is a hard and
2.7 Conclusion
Based on the present results, temperature for dental cold sensation did not remain the
same during bleaching treatment; skin cold sensation threshold did not change during
bleaching treatment using 35% hydrogen peroxide; and skin cold sensation threshold might
2.8 Acknowledgements
This research was supported by Fapesp (10/11627-6). The authors thank FGM
2.9 ReferencesÁ
1. Chong PS & Cros DP (2004) Technology literature review: Quantitative Sensory
Testing Muscle & Nerve29(5):734-747.
2. Lautenbacher S, Kunz M, Strate P, Nielsen J & Arendt-Nielsen L (2005) Age effects
on pain thresholds, temporal summation and spatial summation of heat and pressure
pain The Journal of the International Association for the Study of Pain 115(3) :410-418.
3. Markowitz K (2010) Pretty painful: why does tooth bleaching hurt? Medical
Hipotheses74(5):835-840.
4. Pfab F, Valet M, Sprenger T, Toelle TR, Athanasiadis GI, Behrendt H, Ring J &
Darsow U (2006) Short-Term alternating temperature enhances histamine-induced
itch: a biphasic stimulus model Journal of Investigative Dermatology126(12) :2673-2678.
5. Chaudhry V, Cornblath DR, Mellits ED, Avila O, Freimer ML, Glass JD, Reim J,
Ronnett GV, Quaskey SA & Kuncl RW (1991) Inter- and intra-examiner reliability of
nerve conduction measurements in normal subjects Annals of Neurology 30(6) :841-843.
6. Dezotti MS, SoX]D-XғQLRU0+-U& Nishiyama CK (2002) Evaluation of pH variation
and cervical dentin permeability in teeth submitted to bleaching treatment Pesquisa
Odontológica Brasileira 16(3):263-268.
7. Edwards RR, Fillingim RB & Ness TJ (2003) Age-related differences in endogenous
pain modulation: a comparison of diffuse noxious inhibitory controls in healthy older
and younger adults The Journal of the International Association for the Study of Pain
101(1-2):155±65.
8. Nour El-din AK, Miller BH, Griggs JA & Wakefield C (2006) Immediate bonding to
bleached enamel Operative Dentistry31(1): 106-114.
9. Chaudhry V, Corse AM, Freimer ML, Glass JD, Mellits ED, Kuncl RW, Quaskey SA
& Cornblath DR (1994) Inter- and intra-examiner reliability of nerve conduction
measurements in patients with diabetic neuropathy Neurology Journal 44(8) :1459-1462.
ΐ Referências identificadas no texto em números arábicos sobrescritos e numeradas
10.Kugel G, Ferreira S, Sharma S, Barker ML & Gerlach RW (2009) Clinical Trial
assessing light enhancement of in-office tooth whitening Journal of Esthetic and
Restorative Dentistry21(5):336-347.
11.Pigg M, Baad-Hansen L, Svensson P, Drangsholt M & List T (2010) Reliability of
intraoral quantitative sensory testing (QST) The Journal of the International
Association for the Study of Pain148(2):220-226.
12.Reis A, Tay LY, Herrera DR, Kossatz S & Loguercio AD (2011) Clinical effects of
prolonged application time of an in-office bleaching gel Operative Dentistry
36(6):590-596.
13.Browning WD, Blalock JS, Frazier KB, Downey MC & Myers ML (2007) Duration
and timing of sensitivity related to bleaching Journal of Esthetic and Restorative
Dentistry 19(5):256-264.
14.Lang PM, Stoer J, Schober GM, Audette JF & Irnich D (2010) Bilateral acupuncture
analgesia observed by quantitative sensory testing in healthy volunteers Anesthesia &
Analgesia110(5):1448-1456.
15.Nähri M (1990) The neurophysiology of the teeth Dental Clinics of North America
34(3):439- 448.
16.Olaleye D, Perkins BA & Bril V (2001) Evaluation of three screening tests and a risk
assessment model for diagnosing peripheral neuropathy in the diabetes clinic Diabetes
Research and Clinical Practice 54(2):115-128.
17.Pfau DB, Rolke R, Nickel R, Treede RD & Daublaender M (2009) Somatosensory
profiles in subgroups of patients with myogenic temporomandibular disorders and
Fibromyalgia Syndrome The Journal of the International Association for the Study of
Pain147(1-3):72-83.
18.Fillingim RB, King CD, Ribeiro-Dasilva MC, Rahim-Williams B & Riley JL 3rd (2009) Sex, gender and pain: a review of recent clinical and experimental findings The
Journal of Pain10(5):447-485.
19.Kalantzis A, Robinson PP & Loescher AR (2007) Effects of capsaicin and menthol on
oral thermal sensory thresholds Archives of Oral Biology52(2):149-153.
20.List T, Leijon G & Svensson P (2008) Somatosensory abnormalities in atypical
odontalgia: A case-control study The Journal of the International Association for the
21.Pavlakovic G, Klinke I, Pavlakovic H, Züchner K, Zapf A, Bachmann CG, Graf BM
& Crozier TA (2008) Effect of thermode application pressure on thermal threshold
detection Muscle & Nerve 38:1498-1505.
22.Siao P & Cros DP (2003) Quantitative sensory testing Physical Medicine &
Rehabilitation Clinics of North America 14(2): 261-286.
23.Juhl GI, Jensen TS, Norholt SE & Svensson P (2008) Central sensitization phenomena
after third molar surgery: a quantitative sensory testing study European Journal of
Pain12(1):116-127.
24.Shukla G, Bhatia M & Behari M (2005) Quantitative thermal sensory testing - value of
testing for both cold and warm sensation detection in evaluation of small fiber
neuropathy Clinical Neurology and Neurosurgery107(6):486-490.
25.Yarnitsky D & Sprecher E (1994) Thermal testing: normative data and repeatability
for various test algorithms Journal of the Neurological Sciences125(1):39-45.
26.Charakorn P, Cabanilla LL, Wagner WC, Foong WC, Shaheen J, Pregitzer R &
Schneider D (2009) The effect of preoperative ibuprofen on tooth sensitivity caused
by in-office bleaching Operative Dentistry34(2):131-135.
27.Horin AP, Lee KM & Colloca L (2012) Placebo effects in therapeutic outcomes
Current Clinical Pharmacology³LQSUHVV´
28.Berga Caballero A, Forner Navarro L & Amengual Lorenzo J (2007) In vivo
evaluation of the effects of 10% carbamide peroxide and 3.5% hydrogen peroxide on
the enamel surface Medicina Oral, Patología Oral y Cirurgía Bucal12(5):E404-407. 29.Severcan F, Gokduman K, Dogan A, Bolay S & Gokalp S (2008) Effects of in-office
and at-home bleaching on human enamel and dentin: an in vitro application of fourier
transform infrared study Applied Spectroscopy62(11): 1274-1279.
30.Ushigome T, Takemoto S, Hattori M, Yoshinari M, Kawada E & Oda Y (2009)
Influence of peroxide treatment on bovine enamel surface-cross-sectional analysis
Dental Materials Journal28(3):315-323.
31.Fugaro JO, Nordahl I, Fugaro OJ, Matis BA & Mjör IA (2004) Pulp reaction to vital
bleaching Operative Dentistry29(4):363-368.
32.Kina JF, Huck C, Riehl H, Martinez TC, Sacono NT, Ribeiro APD & Costa CAS
(2010) Response of human pulps after professionally applied vital tooth bleaching
33.Washington LL, Gibson SJ & Helme RD (2000) Age-related differences in the
endogenous analgesic response to repeated cold water immersion in human volunteers
The Journal of the International Association for the Study of Pain89(1):89-96.
34.Delfino CS, Chinelatti MA, Carrasco-Guerisoli LD, Batista AR, Fröner IC &
Palma-Dibb RG (2009) Effectiveness of home bleaching agents in discolored teeth and
influence on enamel microhardness Journal of Applied Oral Science17(4):284-288. 35.Leonard RH, Haywood VB & Philips C (1997) Risk factors for developing tooth
sensitivity and gingival irritation associated with nightguard vital bleaching
Figures
Figure 1 - Flow chart diagram detaching the enrollment, allocation, follow-up and analysis during the study (CONSORT Statement).
Analysed (n=30)
i Excluded from analysis (n=0) Analysed (n=30)
i Excluded from analysis (n=0)
Assessed for eligibility (n=69)
Lost to follow-up (n=0)
Discontinued intervention (n=0)
Allocated to experimental agent (n=30) i Received allocated intervention (n=30) i Did not receive allocated intervention (n=0) Allocated to placebo agent (n=30)
i Received allocated intervention (n=30) i Did not receive allocated intervention (n=0)
Excluded (n=9)
i Not meeting inclusion criteria (n=7) i Declined to participate (n=2) i Other reasons (n=0)
Lost to follow-up (n=0)
Discontinued intervention (n=0) Allocation
Analysis Follow-‐Up Enrollment
Figure 3- Individual perforated tray confectioned to standardize the dental region to
Tables
Table 1 - Inclusion and exclusion criteria for selection of patients.
I nclusion Criteria
Healthy and vital maxillary teeth No decayed teeth
No visible enamel defects No orthodontic brackets Overall good systemic health Healthy oral soft tissue Non-smoking
Pacients who have never undergone bleaching treatment
Exclusion Criteria
Direct and indirect restorations in the maxillary anterior region Adverse reaction to peroxide
Use of opioids or medications influencing neurosensory response Use of pacemaker
Presence of dental staining (tetracycline, trauma, fluorosis, and unknown etiology) Neurological diseases
Table 2 - Evaluation periods of the skin and dental cold sensation threshold.
Evaluation Period Tooth Skin
Period 00 Baseline (24 hours before treatment) Baseline (24 hours before treatment) Period 01 Immediately before treatment Immediately before treatment
Period 02 Immediately after the 1st treatment session Immediately after the 1st treatment session Period 03 24 hours after the 1st treatment session ---
Period 04 Immediately after the 2nd treatment session Immediately after the 2nd treatment session Period 05 24 hours after the 2nd treatment session ---
Period 06 Immediately after the 3rd treatment session Immediately after the 3rd treatment session Period 07 24 hours after the 3rd treatment session ---
Period 08 7 days after treatment 7 days after treatment
Table 3 - Study groups and experimental and placebo products composition.
* FGM ± Dental Products GROUPS
SKI N COLD
SENSATI ON THRESHOLD
TREATMENT COM POSI TI ON POSOLOGY LOT
I Low Whitennes HP Maxx a 35%* (35% hydrogen peroxide)
30%±35% hydrogen peroxide, thickener, pigments, glycol, inorganic
compound and deionized water
3 applications of 15 minutes every 7
days
260111
II High
III Low
Placebo*
Distilled water, thickener, pigments, glycol, inorganic compound and
deionized water 290910
Table 4 - P. values obtained after dental cold sensation evaluation in different periods.
Evaluation Periods
Low Threshold High Threshold
Group I (Bleaching agent)
Group I I I (Placebo)
Group I I (Bleaching agent)
Group I V (Placebo)
P 01 x P 02 0.0000* 0.0152* 0.0000* 0.1062
P 01 x P 03 0.0000* 0.7878 0.0000* 0.0022*
P 01 x P 04 0.0000* 0.9872 0.0000* 0.0900
P 01 x P 05 0.0000* 0.8607 0.0000* 0.0655
P 01 x P 06 0.0000 * 0.8650 0.0000* 0.0760
P 01 x P 07 0.0000* 0.6016 0.0000* 0.1163
P 01 x P 08 0.0000* 0.5941 0.0000* 0.0757
P 01 x P 09 0.0000* 0.5032 0.0000* 0.2216
Table 5 - Temperature variations for cold sensation (oC) in different evaluation periods, after the beginning of dental bleaching.
Evaluation Periods
Low Threshold
P. value High Threshold P. value Group I Group I I I Group I I Group I V
02 6.732A 0.874B 0.0000* 3.034A 1.700B 0.0445*
03 6.132A 1.545B 0.0000* 3.228A 1.610B 0.0180*
04 6.958A 1.473B 0.0000* 7.371A 1.853B 0.0000*
05 4.781A 1.539B 0.0002* 4.481A 1.776B 0.0005*
06 4.871A 1.424B 0.0000* 6.898A 2.657B 0.0000*
07 8.115A 1.283B 0.0000* 6.008A 1.733B 0.0000*
08 3.078A 1.663B 0.0124* 5.822A 2.187B 0.0006*
09 4.773A 1.636B 0.0000* 4.813A 1.833B 0.0008*
Means followed by different letters in lines represent a statistically significant difference according to the
6WXGHQW¶VW-test, p
Table 6 - P. values obtained after skin cold sensation threshold evaluation in different periods.
Evaluation Periods P. value
Low Threshold High Threshold
P 01 X P 02 0.5488 0.3444
P 01 X P 04 0.2866 0.5721
P 01 X P 06 0.3173 0.6883
Table 7 - Temperature variations for dental cold sensation (oC) of experimental groups with low and high threshold.
Bleaching Session Evaluation Periods
Group I (Low Threshold)
Group I I
(High Threshold) P. value
1st session
01 3.067 4.143 0.7422
02 6.732 3.034 0.0000*
03 6.132 3.228 0.0007*
2nd session 04 6.958 7.371 0.5822
05 4.781 4.481 0.7558
3rd session 06 4.871 6.898 0.0177*
07 8.115 6.008 0.0159*
Post-bleaching control 08 3.078 5.822 0.0042*
09 4.773 4.813 0.9622
3 Capítulo 2
Teste Sensorial Quantitativo: efeito de um tratamento dessensibilizante após o
clareamento dental.
QST após tratamento dessensibilizante
3.1 Resumo
O objetivo deste estudo clínico randomizado foi quantificar a sensibilidade dentária durante o
tratamento clareador e após a aplicação de um dessensibilizante. Para tanto, o equipamento de
análise neurosensorial, TSA II, foi utilizado para a realização do Teste Sensorial Quantitativo
(QST) por meio de estímulos térmicos. Dez pacientes (n=10) receberam o tratamento
clareador com peróxido de hidrogênio a 35% (Whiteness HP Maxx) e após a sessão
clareadora foi realizada a aplicação de um dessensibilizante tópico a base de nitrato de
potássio a 5% e fluoreto de sódio a 2% (Desensibilize KF 2%) apenas no hemi-arco esquerdo
da maxila, utilizando o método da boca dividida. No hemi-arco direito foi aplicada uma
solução salina a temperatura ambiente (controle). O QST foi realizado antes do clareamento
(AC), imediatamente depois do clareamento (DC) e imediatamente após a aplicação do
dessensibilizante (DD). Para padronizar o local do estímulo, uma moldeira de acetato com
perfurações circulares foi utilizada durante as mensurações. A análise estatística foi realizada
por meio do WHVWH W GH 6WXGHQW Į $V WHPSHUDWXUDV PpGLDV oC) (DP) do limiar de sensação ao frio para o hemi-arco direito (controle) foram: AC-13,898 (4,81), DC-19,241
(3,68), DD-20,646 (3,72) e para o hemi-arco esquerdo foram: AC-14,102 (3,22), DC-19,646
(4,82), DD-13,835 (3,63). Concluiu-se que clareamento dental com peróxidos de alta
concentração exacerbaram a sensibilidade dental ao estímulo térmico e que o uso do
dessensibilizante foi efetivo para reverter esta situação.
Perspectiva: O novo método utilizado neste estudo pode aumentar a confiabilidade dos estudos clínicos sobre sensibilidade dentária ao analisar quantitativamente a eficácia de
tratamentos dessensibilizantes após o clareamento dental. Esta análise neurosensorial pode
ajudar no desenvolvimento de terapias clareadoras mais seguras e confortáveis.
Quantitative Sensory Testing of the effect of desensitizing treatment after dental
bleaching
QST assessment after desensitizing treatment
3.2 Abstract
The aim of this randomized clinical trial was to quantify dental sensitivity during bleaching
treatment and before a desensitizing treatment using a new device, TSA II, that uses thermal
stimuli to conduct Quantitative Sensory Testing (QST). Ten patients (n=10) underwent
bleaching treatment using 35% hydrogen peroxide (Whiteness HP Maxx). After the bleaching
session, the teeth were cleaned with air/water spray and the split-mouth design was used.
Thus, a topical desensitizer containing 5% potassium nitrate and 2% sodium fluoride
(Desensibilize KF 2%) was applied to the teeth of the left maxillary hemi-arch. A saline
solution at ambient temperature was applied in the right maxillary hemi-arch (control). QST
was performed before bleaching (BB), immediately after bleaching (AB), and immediately
after the desensitizer (AD). For standardization of tooth analysis, an acetate tray, with circular
SHUIRUDWLRQV ZDV XVHG 6WXGHQW¶V W-test was XVHG Į WR DQDO\]H WKH GDWD 0HDQ
temperatures (oC) (SD) of cold sensation threshold for the right hemi-arch (control) were: 13.898 (4.81), AB-19.241 (3.68), AD-20.646 (3.72) and for the left hemi-arch were:
BB-14.102 (3.22), AB-19.646 (4.82), AD-13.835 (3.63). Dental bleaching with highly
concentrated peroxides increased dental cold sensation thresholds, but the topical desensitizer
reversed the immediate cold sensation caused by the cold stimulus.
Perspective: The new method used in this study may increase the reliability of clinical studies regarding dental sensitivity and quantitatively assess the effect of a desensitizing
treatment after dental bleaching. This neurosensory analysis could potentially help to develop
safer and more comfortable bleaching therapies.
3.3 I ntroduction§
Dental professionals often consider dental bleaching to be a conservative technique
that provides low-cost, effective, and fast results. As many patients request dental bleaching,
it has become a primary marketing and a focus of treatment planning for many dental
professionals.1,16,33,38 When supervised by a dentist, home bleaching can be a simple, safe, and
esthetically pleasant approach.15,16,28,38 However, the in-office technique that uses highly
concentrated hydrogen peroxide has been widely used because results are achieved quickly
without the use of trays.6,12,17
Usually, dental professionals apply products containing 30% to 40% hydrogen
peroxide while protecting soft tissues against deleterious effects.14,16 Bleaching occurs using
an unstable type of reactive oxygen that oxidizes tooth pigments, promoting lightening.16,42
Despite the effectiveness of dental bleaching, current studies reveal that patients exposed to
this whitening strategy report different frequency and intensity of dental sensitivity,28,14 a
negative treatment outcome that UHGXFHVSDWLHQW¶VVDWLVIDFWLRQ
The current literature does not clarify the origin of dental sensitivity, which is crucial
in determining an effective bleaching technique that causes minimum patient discomfort. In
the past, desensitizers have been applied to reduce discomfort with no apparent influence on
bleaching efficacy. 20,33,46,48 Among many different options, 5% potassium nitrate, which may
or may not be incorporated with 2% sodium fluoride, has been used as a desensitizing
agent.25,37,46,48
Clinical studies have evaluated the frequency and intensity of dental sensitivity and
have presented subjective data based on personal reports6,5,28,34 and pain questionnaires5
according to the Visual Analogue Scale (VAS). However, misunderstanding of data may have
§