Acute Primary Actinomycosis Involving the
Hard Palate of a Diabetic Patient
Ana Luiza Dias Leite de Andrade, DDS, MSc,
*
M
arcio Menezes Novaes, DDS,y
Adriano Rocha Germano, DDS, MSc, PhD,z
Kleber Giovanni Luz, MD, MSc, PhD,x
Roseana de Almeida Freitas, DDS, MSc, PhD,k
and
H
ebel Cavalcanti Galv
ao, DDS, MSc, PhD{
~
Actinomycosis is a relatively rare infection caused by saprophytic bacteria of the oral cavity and gastro-intestinal tract that can become pathogenic. The chronic hyperglycemia of diabetes mellitus induces events that promote structural changes in various tissues and are associated with problems in wound healing. This infection remains largely unknown to most clinicians because of its different presentations, and palatal involvement is extremely rare. This report describes the case of a 46-year-old woman who was diagnosed with actinomycosis involving the hard palate. The main clinical, histopathologic, and therapeutic characteristics and differential diagnosis of actinomycosis are reviewed. To date, 3 cases of actinomycosis involving the hard palate have been reported.
Ó2014 American Association of Oral and Maxillofacial Surgeons
J Oral Maxillofac Surg 72:537-541, 2014
Actinomycosis is a slowly progressing infection caused by anaerobic or microaerophilic, gram-positive, non– spore-forming, non–acid-fast bacteria of the genus Ac-tinomyces. The species most frequently isolated is Ac-tinomyces israelii. Three distinct clinical forms of the disease have been described: cervicofacial, abdomino-pelvic, and thoracopulmonary, with the first being the most common.1,2
Oral and cervicofacial diseases are commonly asso-ciated with dental caries and extractions, gingivitis and gingival trauma, infection in erupting secondary teeth, chronic tonsillitis, otitis or mastoiditis, diabetes mellitus, immunosuppression, malnutrition, and local tissue damage caused by surgery, neoplastic disease, or irradiation.3The chronic hyperglycemia of poorly con-trolled diabetes mellitus induces events that promote structural changes in various tissues and are associated
with problems in wound healing and a greater suscep-tibility to infections.4-6
Actinomycosis mimics different diseases and ex-hibits different symptoms, a fact that makes its diagno-sis difficult.3Most commonly, it presents as a slowly progressive, indolent, indurated infiltration with multi-ple abscesses, fistulas, and sinuses. A less common form is acute and rapidly progressive, with fever and a fluctuating swelling that resembles a typical pyo-genic infection.7,8The differential diagnosis includes tuberculosis (scrofula), fungal infections, nocardiosis, suppurative infections by other organisms, and neoplasms.3
Microscopic analysis shows an outer zone of granu-lation tissue consisting of collagen fibers around cen-tral purulent loculations that contain abundant neutrophils that surround multiple ‘‘sulfur granules.’’
Received from the Federal University of Rio Grande do Norte, Natal, RN, Brazil.
*PhD Student, Oral Pathology Postgraduate Program, Department of Dentistry.
yResident, Division of Oral and Maxillofacial Surgery, Department of Dentistry.
zProfessor, Division of Oral and Maxillofacial Surgery, Department of Dentistry.
xProfessor, Division of Infectology, Giselda Trigueiro Hospital.
kProfessor, Oral Pathology Postgraduate Program, Department of Dentistry.
{Professor, Oral Pathology Postgraduate Program, Department of Dentistry.
Address correspondence and reprint requests to Dr de Andrade: Departamento de Odontologia, Universidade Federal do Rio Grande do Norte, Av Senador Salgado Filho, 1787, Lagoa Nova, Natal, RN, Brasil CEP 59056-000; e-mail:ana_luiza_dla@hotmail.com
Received July 8 2013 Accepted August 7 2013
Ó2014 American Association of Oral and Maxillofacial Surgeons 0278-2391/13/01032-X$36.00/0
http://dx.doi.org/10.1016/j.joms.2013.08.006
These granules appear as a basophilic mass with a radi-ating border of eosinophilic clubs after routine staining.3,9
This report describes the fourth case of primary ac-tinomycosis involving the hard palate and discusses the main clinical, histopathologic, and therapeutic characteristics and differential diagnosis of this rare presentation of the disease.
Report of Case
A 46-year-old woman was seen at the Department of Oral and Maxillofacial Surgery, Federal University of Rio Grande do Norte (Natal, Brazil) with a 4-day history of a painful lesion on the hard palate that caused dys-phagia. The patient had a 3-year medical history of poorly controlled type 2 diabetes mellitus and was be-ing treated with metformin, although she reported dis-continuing the treatment 2 months before the appearance of the lesion. The patient had been a smoker for 20 years, consuming 1 pack of cigarettes per day.
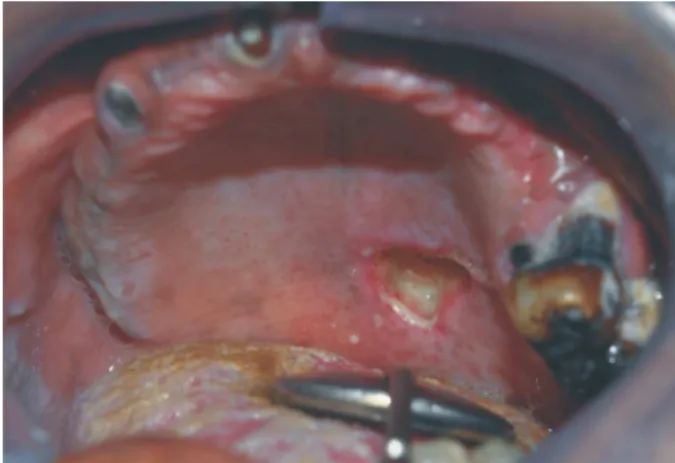
Intraoral examination showed an ulcerative lesion on the left side of the hard palate that measured ap-proximately 1 cm in diameter and exhibited bone destruction and exposure with an overlying yellow-white slough (Fig 1). Several teeth were missing and the patient presented extensive carious lesions, supra-and subgingival dental calculi, extensive root expo-sure caused by gum recession, and a coated tongue. The patient denied episodes of bleeding, purulent dis-charge, headache, heaviness of the cheeks, cough with expectoration, respiratory distress, epistaxis, fatigue, anorexia, weight loss, fever, or more cardinal signs of inflammation. No lesion or symptom was identified in the oropharynx or hypopharynx or in any other re-gion of the body, and there was no evidence of cervical lymphadenopathy.
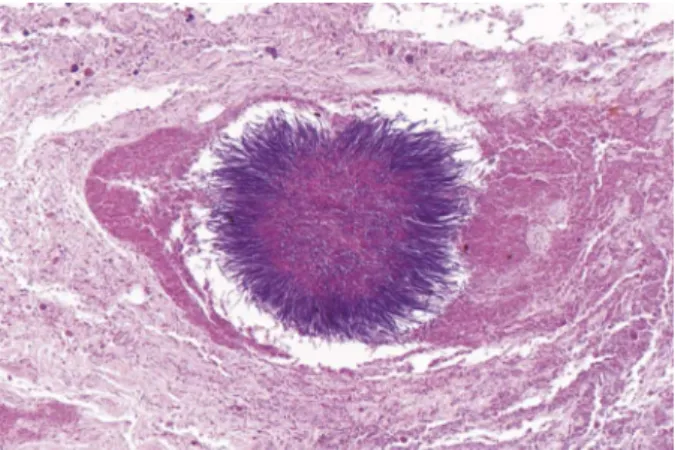
Based on the clinical presentation, the diagnostic hypotheses were necrotizing sialometaplasia, salivary gland neoplasm, and oral squamous cell carcinoma. An incisional biopsy was performed and histopatho-logic analysis showed the presence of microscopic ag-gregates of tangled filaments characterized by a central eosinophilic mass from which numerous peripheral basophilic rays extended (Figs 2 through 4). The surrounding connective tissue was dense and fibrous and contained a discrete inflammatory infiltrate consisting of neutrophils, lymphocytes, and plasma cells. Some foreign body–type multinucleated giant cells and areas of necrosis also were identified.
Based on the microscopic findings, material was col-lected for culture and identification of the microbial agent. However, because the culture result was nega-tive, a new sample was collected, seeded onto sheep blood agar, and incubated under anaerobic conditions.
FIGURE 1. Ulcerative lesion showing bone destruction with an overlying yellow-white slough.
de Andrade et al. Acute Primary Actinomycosis in Diabetes. J Oral Maxillofac Surg 2014.
FIGURE 2. Panoramic view showing colonies of filamentous bacte-ria (hematoxylin and eosin stain; magnification,40).
de Andrade et al. Acute Primary Actinomycosis in Diabetes. J Oral Maxillofac Surg 2014.
FIGURE 3. Numerous microscopic aggregates of tangled bacte-rial filaments in mildly inflamed connective tissue (hematoxylin and eosin stain; magnification,100).
The resulting colonies consisted of gram-positive ba-cilli that were negative by Ziehl-Neelsen staining. No b-hemolysis was observed. Next, the material was ex-amined using the VITEK automated identification system (bioMerieux, Marcy l’Etoile, France), which identified Actinomyces naeslundii with 97% agree-ment. Some laboratory tests were performed (Table 1) to confirm the efficacy of the equipment. The diagnosis of actinomycosis was thus confirmed.
The patient was treated orally with amoxicillin (500 mg) 3 times per day for 4 weeks, which resulted in complete regression of the lesion.
Discussion
Actinomycesspecies are saprophytic bacteria of the oral cavity and gastrointestinal tract. The bacteria ex-hibit a low degree of virulence and are commonly found in the saliva and in dental plaque. However, un-der certain circumstances that compromise anatomic barriers and host susceptibility, their pathogenic form can cause actinomycosis.10,11
In addition to precarious oral hygiene, the present patient had diabetes mellitus. It is believed that the high concentration of glucose in the wound fluid of pa-tients with diabetes is the main reason for the increased
bacterial growth seen in these patients.5,12,13According to Hirsch et al,5nondiabetic patients can resist bacterial invasion much more efficiently, whereas diabetic pa-tients are more likely to succumb to the bacterial chal-lenge. In addition, it is well known, although not completely understood, that diabetes mellitus impairs wound healing.
The typical actinomycosis infection is chronic in na-ture; however, it may be atypical with subacute or acute clinical manifestations.8 Samuels and Martin14 described 3 distinct presentations of the disease: acute painful swellings with duration shorter than 1 month; chronic long-standing infections with duration longer than 3 months; and unsuspected microbiologically proved actinomycotic lesions. Although the present patient did not show all signs and symptoms of acute inflammation, according to the classification of Sam-uels and Martin,14the case can be categorized as the acute type of actinomycosis as a result of the presence of a painful lesion that occurred within a short period. Actinomycosis involving the hard palate is ex-tremely rare, and only 3 cases have been reported in the literature7(Table 2). The first case was a cocaine user who had a circular and necrotic defect in the hard palate without nasal communication on prob-ing.15The second case presented a necrotic ulceration along the hard palate with overhanging yellow-green slough, in addition to perilesional erythema and boggi-ness with reactive swelling of the upper lip.11 The third case was characterized by a firm, infiltrative ul-cerated plaque and significant tissue destruction and deformity, with an overlying yellow-white slough.7
The clinical diagnosis of actinomycosis is difficult because its onset is not specific and the differential di-agnosis covers a wide range of diseases.16Its variable clinical presentations are generally considered repre-sentative of malignancy rather than of an infectious process,3 as seen in the present case. From this per-spective, the diagnosis of actinomycosis on admission is correct in fewer than 10% of cases.15
Different pathologic entities were considered in the differential diagnosis of the present case. Necrotizing sialometaplasia, a benign reactive necrotizing inflam-matory process involving the minor salivary glands of the hard palate,17was one of them. The most com-monly proposed and generally accepted etiology for this condition relates to ischemia and, although not all cases will be correlated with an obvious etiologic event, clinical history is helpful in its diagnosis.18 The present case denied any surgical procedure or other traumatic injuries that could be considered potential predisposing factors. Moreover, the micro-scopic features of necrotizing sialometaplasia (pseu-doepitheliomatous hyperplasia of the overlying epi-thelium, squamous metaplasia of the salivary ducts, and acinar necrosis) were not found.
FIGURE 4. Sulfur granules present a central eosinophilic mass with peripheral basophilic rays (hematoxylin and eosin stain; magnifica-tion,400).
de Andrade et al. Acute Primary Actinomycosis in Diabetes. J Oral Maxillofac Surg 2014.
Table 1. BIOCHEMICAL TESTS PERFORMED TO CONFIRM THE DIAGNOSIS OF ACTINOMYCOSIS
Biochemical Tests Result
Hydrogen sulfide +
Bile esculin +
Urease +
Catalase
Because the palate is one of the most common sites for the development of primary salivary gland neo-plasms, a malignant salivary gland tumor was included in the differential diagnosis of the present case. The most likely candidates based on frequency of occur-rence are mucoepidermoid carcinoma, adenoid cystic carcinoma, and polymorphous low-grade adenocarci-noma.11 However, although more aggressive tumors such as salivary duct carcinoma should be considered, the development of a tumor of the reported extent and bone destruction within such a short period would be highly unlikely.
The propensity of actinomycosis to mimic squa-mous cell carcinoma is well known.16 In agreement with this aspect, the authors also hypothesized that the present lesion was an epithelial malignant tumor based on the rapidly destructive evolution of the dis-ease and the fact that the patient had been a smoker for 20 years. However, carcinomas of the hard palate often present as a papillary or exophytic growth rather than a flat or ulcerated lesion,19 as observed in the present case.
Although not pathognomonic, histologic features of actinomycosis are the presence of sulfur granules whose centers exhibit basophilic staining with eosino-philic rays and that are surrounded by neutrophils.3 The present case differs from previously reported cases by exhibiting microscopic aggregates that did not show the established pattern when stained by rou-tine techniques. In addition, neutrophilic inflamma-tion was scarce. To the authors’ knowledge, this is the first case exhibiting this staining pattern, which
could not be clarified satisfactorily. The mild intensity of the inflammatory infiltrate was probably due to the short duration of the lesion and the systemic condition of the patient. Leukocyte dysfunction is common in patients with diabetes mellitus, and the metabolic anomalies of the disease associated with decreased chemotaxis cause inadequate migration of neutrophils and macrophages to the site of aggression.20,21
Culture results are negative in more than 50% of cases of actinomycosis and an incisional biopsy is fre-quently necessary for diagnosis of the disease.22 In view of the difficulty in identifying the microbial agent, 2 bacterial cultures were necessary in the present case, because the first culture result was negative. The second culture identified A naeslundii as the causative agent of the infection. In the oral cavity, this micro-organism plays an important role in dental biofilm formation and gingival inflammation. It is be-lieved that this bacterium can induce the destruction of soft and hard tissues through root canals and the gin-gival sulcus, playing a key role in the onset of peri-odontal disease or in the transition from gingivitis to periodontitis.23
Treatment of the present case consisted of the oral administration of penicillin as recommended in the lit-erature,7,11,15 and the patient presented complete regression of the lesion.
In conclusion, the diagnosis of infection with Acti-nomycesspecies in oral tissues represents a challenge because of the variable clinical manifestations of the disease. However, health care professionals should be aware of the presence of ulcerative, destructive
Table 2. CASES OF ACTINOMYCOSIS INVOLVING THE HARD PALATE REPORTED IN THE LITERATURE
Reference Year
Age (yr)/
Gender Duration Condition Signs and Symptoms Treatment
Rubin and Krost15 1995 58/M — cocaine snorting nasal congestion,
yellow sputum, and purulence
intravenous aqueous penicillin + oral clindamycin; intravenous penicillin Herman et al11 1998 65/F 2 wk chronic lymphocytic
leukemia
pain, malaise, generalized prostration, difficulty eating and swallowing
intravenous penicillin
De et al7 2011 32/M 2 yr normal — intravenous
crystalline penicillin G Present case 2013 46/F 4 days diabetes mellitus dysphagia and pain penicillin
Abbreviations: F, female; M, male.
oral lesions because they can mimic malignant condi-tions. Among the previously reported cases of actino-mycosis of the hard palate, this is the first report in which A naeslundii was identified as the causa-tive agent.
References
1. Samant S, Sandoe J, High A, et al: Actinomycosis mimicking a ton-sillar neoplasm in an elderly diabetic patient. Br J Oral Maxillofac Surg 47:417, 2009
2. Smego RA Jr, Foglia G: Actinomycosis. Clin Infect Dis 26:1255, 1998
3. Brook I: Actinomycosis: Diagnosis and management. South Med J 101:1019, 2008
4. Bastos AS, Leite AR, Spin-Neto R, et al: Diabetes mellitus and oral mucosa alterations: Prevalence and risk factors. Diabetes Res Clin Pract 92:100, 2011
5. Hirsch T, Spielmann M, Zuhaili B, et al: Enhanced susceptibility to infections in a diabetic wound healing model. BMC Surg 8:5, 2008
6. Iacopino AM: Diabetic periodontitis: Possible lipid-induced de-fect in tissue repair through alteration of macrophage pheno-type and function. Oral Dis 1:214, 1995
7. De D, Dogra S, Kanwar AJ, et al: Actinomycosis presenting as a destructive ulcerated plaque on the palate and gingiva. J Am Acad Dermatol 65:1235, 2011
8. Nielsen PM, Novak A: Acute cervico-facial actinomycosis. Int J Oral Maxillofac Surg 16:440, 1987
9. Lin HC, Yang CH, Friedman M, et al: Atypical presentation of ac-tinomycosis: A giant ulcer of the base of the tongue. Oper Tech Otolaryngol Head Neck Surg 18:329, 2007
10. Ablanedo-Terrazas Y, Ormsby CE, Reyes-Teran G: Palatal actino-mycosis and Kaposi sarcoma in an HIV-infected subject with
disseminated mycobacterium avium-intracellulare infection. Case Rep Med 2012:679728, 2012
11.Herman WW, Whitaker SB, Williams MF, et al: Acute actinomyco-sis presenting as an ulcerated palatal mass. J Oral Maxillofac Surg 56:1098, 1998
12.Blakytny R, Jude E: The molecular biology of chronic wounds and delayed healing in diabetes. Diabet Med 23:594, 2006 13.Schubert S, Heesemann J: Infections in diabetes mellitus. Immun
Infect 23:200, 1995
14.Samuels RH, Martin MV: A clinical and microbiological study of Actinomycetes in oral and cervicofacial lesions. Br J Oral Maxil-lofac Surg 26:458, 1988
15.Rubin MM, Krost BS: Actinomycosis presenting as midline pala-tal defect. J Oral Maxillofac Surg 53:701, 1995
16.Carinci F, Polito J, Pastore A: Pharyngeal actinomycosis: A case report. Gerodontology 24:121, 2007
17.Garcia NG, Oliveira DT, Faustino SE, et al: Necrotizing sialometa-plasia of palate: A case report. Case Rep Pathol 2012:679325, 2012 18.Carlson DL: Necrotizing sialometaplasia: A practical approach to
the diagnosis. Arch Pathol Lab Med 133:692, 2009
19.Johnson N, Franceschi S, Ferlay J, et al: Squamous cell carcinoma
inBarnes L, Eveson JW, Reichart P, et al, (eds). World Health Or-ganization Classification of Tumours. Pathology and Genetics of Head and Neck Tumors. Lyon, France: IARC Press, 2005, p 171
20.Delamaire M, Maugendre D, Moreno M, et al: Impaired leucocyte functions in diabetic patients. Diabet Med 14:29, 1997 21.Wysocki J, Wierusz-Wysocka B, Wykretowicz A, et al: The
influ-ence of thymus extracts on the chemotaxis of polymorphonu-clear neutrophils (PMN) from patients with insulin-dependent diabetes mellitus (IDD). Thymus 20:63, 1992
22.G€oc¸men G, Varol A, G€oker K, et al: Actinomycosis: Report of a case with a persistent extraoral sinus tract. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 112:e121, 2011