Vol-7, Special Issue-Number2-April, 2016, pp968-978 http://www.bipublication.com
Case Report
The correlation between depression and osteoporosis in
the elderly of Amirkola
Farzan Kheirkhah1, Touska. Nourmohammadi2, Seyed Reza. Hoseini3 , Angela Hamidia4*Ali. Bijani5, .Haji Qhurban Nourodini6 and Sanaz Azadforouz7
1Assistant Professor of Psychiatry,
Research Center for Social Determinants of University Health, Babol University of Medical Sciences, Babol, Mazandaran.
1Associate Professor, Department of psychiatry ,
Baboluniversity of medical scienses
2Medical student, Baboluniversity of medical sciences
3
Professor, Department of Community Medicine, Social Determinants of Health (SDH) Research Centre,
Babol University of Medical Sciences 4Assistant Professor, Department of psychiatry ,
Baboluniversity of medical sciences 5MD
.Non-Communicable pediatric diseases research center –Babol University of medical sciences
6Radiologis ,Babol university of medical sciences
7
Assistant Professor, Department of psychiatry , Baboluniversity of medical sciences *Corresponding Author: Dr. Angela Hamidia
Assistant Professor of l Medicine sicences ;
Address: Yahyanejad Hospital, Babol University of Medical Sciences, Babol, Mazandaran, Iran; Email: [email protected]
ABSTRACT
Background: Depression is correlated with some changes in hormonal system such as increasing cortisol and decreasing sex hormones which can lead to reduce bone mineral density. This study aimed to evaluate the correlation between depression and osteoporosis in the elderly of Amirkola.
Material and method: This cross sectional study is a part of the cohort study of AHAP included 1087 elderly of Amirkola. Depressive symptoms were assessed by Geriatric Depression Scale (GDS) and bone mineral density was obtained by dual energy x-ray absorptiometry on femur and lumbar vertebrae; then, the result was expressed as T-Score. Data was analyzed by spss18 and statistical analysis. P value <0.05 was considered significant.
Result: A total number of 1087 elderly including 55.6% men and 44.4% women with the mean age of 68.39±6.98 were participated in this study in which 41.1% had depressive symptoms and 58.9% didn’t have depressive symptoms. 20.1 % had normal BMD, 44.9% had osteopenia and 35% suffered from osteoporosis. Mean score of GDS in osteoporotic group was 5.30±3.62, compared to the groups of normal BMD (4.12±3.24) and osteopenia (3.38±2.84) which was significantly higher (p-value=0.00). The number of osteoporotic and osteopenic cases in depressive group were significantly more than non-depressive group (p-value=0.00). After gender adjustment, this difference was significant only in men (p-value=0.02). There was also a poor correlation between depressive symptoms and BMD in femur (r= -0.24, p=0.00) and lumbar vertebrae (r= -0.18, p=0.00).
Conclusion: Depression was significantly associated with osteoporosis in the elderly. After gender adjustment, this association was significantly observed in men, not in women.
INTRODUCTION
Today, the elderly population is increasing globally, so that with increasing life expectancy, the elderly had the fastest growth among the world's population groups and thus aging is considered as an important global phenomenon (1, 2) . According to WHO, the number of the elderly in the South West Asia (including Iran) in 2000 was about 7% of the total population and by 2030 this figure will increase to 15% (3).
Among the various diseases of old age, psychiatric disorders, especially depression, is of particular importance. Depression is the second most common psychological disorder in the elderly. Epidemiological studies showed that the prevalence of depression in hospitals is 10-30% and 30-45% in the nursing homes. Furthermore, the prevalence of depression in women is more than men and in singles, widows, and divorced people are more than married ones (4).
Osteoporosis is the most common metabolic bone disease and it is a very epidemic disease in the elderly population that is characterized by the decreased bone mass anddisassemble bone tissue components. Today, the bone mineral density (BMD) is the basis for diagnosis of osteoporosis (5).
The relationship between depression and physical illness is very complex. In some cases depression acts as a risk factor for developing some events or physical ailments, including decreased BMD and osteoporosis (6). However, the results of various studies on this subject have not been consistent. Some studies reported the link between depression and decreased BMD (7-9) and fractures resulting from osteoporosis (10, 11) and others found no relationship (12, 13). The results of some studies also suggested that this relationship can be dependent on gender and race (14, 15).
Given the importance of the subject and the few studies conducted in Iran on this issue and no related reports in the region, this study aimed to assess the association between osteoporosis and depression in the elderly population of the Amirkola.
METHODOLOGY
This study is part of a comprehensive plan to check the health status of the elderly in Amirkola (AHAP) in a cohort study conducted in 2011 on all people over 60 years and in Amirkola, Mazandaran (16). Amirkola has two health centers, which lists all the elderly and their addresses available. The elderly people were invited to participate in the study through phone calls and or home visits, while providing the necessary information about the plan. This cross-sectional study was performed on the elderly population 60 years and older who referred to Health Research Center of University. The study protocol was approved by the Research Council and the Ethics Committee of Research in the University of Medical Sciences.
based on the scores of the results. The score of 0 to 4 is considered as normal, 5-8 as mild depression, 9-11 as moderate depression, 12-15 as severe depression; with the sensitivity of 92% and specificity of 89% (17-19). This questionnaire has been validated for Iranian community by previous researchers. Cronbach's alpha for this questionnaire was reported 0.81 in the elderly population of Amirkola. Those whose score was 5 or more than 5 were referred topsychiatric
clinic for further investigation.
Measuring Bone Mineral Density (BMD) was performed by a DEXA (Dual Energy X-ray Absorptiometry) on the femur and lumbar spine and the results were expressed on the Score. T-Score≤-2.5 was standard deviation, osteoporosis and -2.5<T-Score≤-1 osteopenia and T-Score> -1 was normal.
Data analysis method
The collected data inserted into SPSS, version 18, and descriptive statistics (mean and standard deviation) and analytical tests (chi-square, t-test, ANOVA) were used to evaluate the relationship between bone mineral mass and symptoms of depression. P value less than or equal to 0.05 was considered as the significant level.
Findings
A total number of 1616 individuals were participated in this study, 1087 patients met the inclusion criteria. The mean age of the study cases was 68.39±6.98 years (range 60-92) included 604 men (55.6%) and 483 women (44.4%). The majority of participants were in the age group of 60-64 years. The frequency distribution of the elderly population of Amirkola is shown based on depression and bone mineral density in Table 1. Among the samples, 640 patients (58.9%) had no symptoms of depression and 447 patients (41.1%) had depressive symptoms.
219 cases also had a normal BMD, and 488 patients with osteopenia and 380 cases with osteoporosis were diagnosed.
Most participants were married (87.2%), illiterate (61.5%) and in terms of job status were
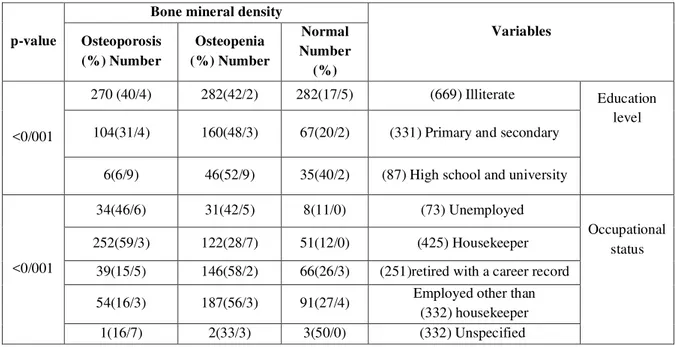
housekeeper (39.1 %). About 18.6% of the participants had a history of smoking and 6.6% reported that they were living alone. The frequency distribution of demographic characteristics based on bone mineral density are shown in Table 2. There was a significant association between age, sex, marital status, BMI, age and living alone with bone mineral density (p<0.001). 72.5% of men vs. 89% of women, 79.1% of married and 93.1% of unmarried, 73.9% of those with a BMI less than 25, 76.9% of individuals with BMI 25-30 and 69.8% of samples with a BMI greater than 30 were diagnosed with osteopenia and osteoporosis. In fact, osteopenia and osteoporosis were significantly higher in women, unmarried individuals and those with BMI less than 25 than men, married individuals, and those with BMI over 25. 82.6% of illiterates, 79.7% of elementary education and 59.8% of high school and university education level were diagnosed with osteopenic and osteoporosis. Results showed that osteoporosis significantly decreased by increasing the education level of individuals. In terms of occupation, 89.1% of unemployed cases, 88% of housewives, 73.7% of employed and retired cases, 72.6% of non-working housewives and 50% of those who had Unknown job had osteopenia and osteoporosis; there was a significant difference between bone mineral density and their job.
by a reduction in bone mineral density at the lumbar spine, but no significant difference
was found (p=0.741, r=-0.015) (Figure 1).
In this study, there was a significant inverse relationship between depression score in men and bone mineral density in the lumbar spine (p=0.018, r =-0.097) and bone mineral density in the femur (p<0.001, r =-0.165). So that, the lower the bone mineral density at the lumbar spine and femur, the higher the depression score; but the correlation was weaker than the general population. In this study, there was a significant inverse relationship between age and bone mineral density in the lumbar spine (p<0.001, r =-0.136) and bone mineral density in the femur (p<0.001, r =-0.322).
In women, a significant inverse relationship was found between these two variables. But the relationship between age and bone mineral density in the lumbar spine was weaker and bone mineral density in the femoral was stronger than the general population. Also in men, an inverse relationship between age and bone mineral density in the lumbar spine was weaker (p<0.001, r =-0.136) and bone mineral density in the femoral was stronger (p<0.001, r =-0.337) (Figure 1). As shown in Table 3, 85.9% of samples with depression and 75.6% of non-depressed samples had osteopenia and osteoporosis; the frequency distribution of BMD status in depressed and non-depressed population showed a significant difference (p<0.001). Also, in terms of depression level, 75.6% of normal depression, 83.4% of mild depression, 89.1% of moderate depression, and 93.1% of severe depression cases were diagnosed with osteopenic and osteoporosis, in which the frequency distribution of BMD status in terms of depression level in the affected population had a significant difference (p<0.001). After gender adjustment, it was revealed that the frequency distribution of occurrence (p=0.02) and depression (p=0.04) in men had significant difference with BMD status, while no significant differences were observed in the female population (Tables 4 and 5).
DISCUSSION
In this study, the association between depression and bone mineral density in elderly men and women were evaluated and the results showed that an average score of GDS in patients with osteoporosis (5.30±3.62) compared to the other two groups of normal BMD (3.38±2.84) and osteoporosis (4.12±3.24) was significantly higher (p<0.001). The number of elderly samples with depressive symptoms was more than those without depressive symptoms which diagnosed with osteoporosis and osteopenia (p<0.001). Although the analysis made on the basis of gender indicated that the difference was significant only in men (p=0.02). Also, an inverse correlation between symptoms of depression and BMD at the femoral (p<0.001, r=-0.24) and spine (p<0.001, r=-0.18) was found. So that, the higher the depression score, the lower the bone mineral density. But by sex, this correlation was significant only in the femoral bone mineral density.
significant relationship between depression and bone density loss (30-32).
Several studies reported a disorder in the hypothalamus-pituitary-adrenal system and the subsequent increase in serum cortisol levels in depressed patients (27). In fact, the increased activity of the hypothalamic-pituitary-adrenal axis is the main endocrine in depression (33). On the other hand, Hypercortisolism is risk factor for low BMD (9, 10, 20, 34). The reduction in bone formation along with an increase in bone desorption can cause increased rate of bone loss in people with depression (35). Leptin Hormone also seems to be effective in the development of osteoporosis in depressed patients. Secretion of this hormone increases in depressed patients at night and inhibits bone formation (36). The increase blood concentrations of inflammatory cytokines such as IL-6 and TNF-alpha plays a role in bone resorption (37, 38) and concentrations of cytokines in depression is high (39-41). Serotonin is another factor that links between the bones and the brain. Although the effect of serotonin on bone varies based on its origin, but the activity of serotonin in the brain can affect the bone mass and prevent the bone formation (34). In our study after the separation of the sexes, a significant difference was observed between depression and bone mineral density in the male population (p=0.02). While such a difference was not seen in women (p=0.81). The results obtained on the basis of gender have been inconsistent in various studies. In a similar study, Oh et al. in 2012 showed that depression in men is associated with decreased bone density, and the risk of having osteoporosis in men with depression was higher compared with men without depression. Unlike men, women's depression was not associated with reduced bone density (42), that this finding was consistent with other studies (43-45). Also previous studies similar to our study showed that there was a significant relationship between depression and BMD in men, but in women, this difference was not significant which was in line with the results of this study (43, 44, 46).
CONCLUSION
According to the findings, the mean score of GDS in patients with osteoporosis was significantly higher than in comparison with the osteopenia and normal groups. Also, the diagnosis of osteoporosis and osteopenia in the elderly population with depression was also significantly more than those without depression symptoms. In this study, similar to other studies, a significant relationship was found between depression and bone mineral density in men, but was not found in women. It seems that there is a need for more comprehensive studies to identify multiple mechanisms of depression on bone density, and to determine depression effects on bone mineral density.
REFERENCES
1. Malakouti SK, Fatollahi P, Mirabzadeh A, Salavati M, Zandi T. Reliability, validity and factor structure of the GDS-15 in Iranian elderly. Int J Geriatr Psychiatry. 2006;21(6):588-93.
2. Ahmadzadeh G. Geriateric depressive disorder (comorbidity of depression with medical conditions in geriatric patients). Behavioural Science Research Journal. 2010;8(2).
3. Sohrabi MB, Zolfaghari, P., Mahdizade, F., Mahdizadeh, F., Aghayan, S.M., Ghasemian-Aghamashhadi, M., et al. Evaluation and Comparison of Cognitive State and Depression in Elderly Admitted in Sanitarium with Elderly Sited in Personal Home. Knowledge & Health. 2008;3(2):27-31.
4. Kashfi SM, Khani-Jeihooni, A., Farhadi, S. . The relationship between social and demographic factors and prevalence of depression among the over 60 years old individuals, Shiraz, Iran. Journal of Hormozgan University of Medical sciences. 2010;14(4):319-25.
5. Wu Q, Magnus JH, Liu J, Bencaz AF, Hentz JG. Depression and low bone mineral density: a meta-analysis of epidemiologic studies. Osteoporos Int. 2009;20(8):1309-20.
6. Schweiger U, Deuschle M, Korner A, Lammers CH, Schmider J, Gotthardt U, et al. Low lumbar bone mineral density in patients with major depression. Am J Psychiatry. 1994;151(11):1691-3.
7. Kahl KG, Greggersen W, Rudolf S, Stoeckelhuber BM, Bergmann-Koester CU, Dibbelt L, et al. Bone mineral density, bone turnover, and osteoprotegerin in depressed women with and without borderline personality disorder. Psychosom Med. 2006;68(5):669-74. 8. Petronijevic M, Petronijevic N, Ivkovic M,
Stefanovic D, Radonjic N, Glisic B, et al. Low bone mineral density and high bone metabolism turnover in premenopausal women with unipolar depression. Bone. 2008;42(3):582-90.
9. Wong SY, Lau EM, Lynn H, Leung PC, Woo J, Cummings SR, et al. Depression and bone mineral density: is there a relationship in elderly Asian men? Results from Mr. Os (Hong Kong). Osteoporos Int. 2005;16(6):610-5.
10. Whooley MA, Kip KE, Cauley JA, Ensrud KE, Nevitt MC, Browner WS. Depression, falls, and risk of fracture in older women. Study of Osteoporotic Fractures Research Group. Arch Intern Med. 1999;159(5):484-90.
11. Mussolino ME. Depression and hip fracture risk: the NHANES I epidemiologic follow-up study. Public health reports. 2005;120(1):71-5. 12. Amsterdam JD, Hooper MB. Bone density
measurement in major depression. Prog Neuropsychopharmacol Biol Psychiatry. 1998;22(2):267-77.
13. Furlan PM, Ten Have T, Cary M, Zemel B, Wehrli F, Katz IR, et al. The role of stress-induced cortisol in the relationship between depression and decreased bone mineral density. Biol Psychiatry. 2005;57(8):911-7.
15. Whooley MA, Cauley JA, Zmuda JM, Haney EM, Glynn NW. Depressive symptoms and bone mineral density in older men. J Geriatr Psychiatry Neurol. 2004;17(2):88-92.
16. Hosseini SR, Cumming RG, Kheirkhah F, Nooreddini H, Baiani M, Mikaniki E, et al. Cohort profile: the Amirkola Health and Ageing Project (AHAP). Int J Epidemiol. 2014;43(5):1393-400.
17. Sheikh JI, Yesavage, J.A. Geriatric Depression Scale (GDS): recent evidence and development of a shorter version. Clin Gerontol. 1986;37(819-20).
18. Gori C, Appollonio, I., Riva, G.P., Spiga, D., Ferrari, A. , Trabucchi, M. Using a single question to screen for depression in the nursing home. Arch Gerontol Geriatr Suppl. 1998;6(235-40).
19. Cheng ST, Chan AC. A brief version of the geriatric depression scale for the chinese. Psychol Assess. 2004;16(2):182-6.
20. Robbins J, Hirsch C, Whitmer R, Cauley J, Harris T. The association of bone mineral density and depression in an older population. J Am Geriatr Soc. 2001;49(6):732-6.
21. Mezuk B, Eaton WW, Golden SH, Wand G, Lee HB. Depression, antidepressants, and bone mineral density in a population-based cohort. J Gerontol A Biol Sci Med Sci. 2008;63(12):1410-5.
22. Zobeihi-Yeganeh M, Jahed, S.A, Rajaee, A., Amini, H. . relationship between bone density and major depression. Pajoohandeh. 2008;32(4):267-70.
23. Cizza G, Mistry S, Nguyen VT, Eskandari F, Martinez P, Torvik S, et al. Do premenopausal women with major depression have low bone mineral density? A 36-month prospective study. PLoS One. 2012;7(7):e40894.
24. Williams LJ, Bjerkeset O, Langhammer A, Berk M, Pasco JA, Henry MJ, et al. The association between depressive and anxiety symptoms and bone mineral density in the general population: the HUNT Study. J Affect Disord. 2011;131(1-3):164-71.
25. Kurmanji JM, Sulaiman SA, Kah LK, Chandrasekaran PK. Depression and low bone mineral density: The correlation among Chinese. Asian J Psychiatr. 2010;3(3):134-7. 26. Konstantynowicz J, Kadziela-Olech H,
Kaczmarski M, Zebaze RM, Iuliano-Burns S, Piotrowska-Jastrzebska J, et al. Depression in anorexia nervosa: a risk factor for osteoporosis. J Clin Endocrinol Metab. 2005;90(9):5382-5. 27. Michelson D, Stratakis C, Hill L, Reynolds J,
Galliven E, Chrousos G, et al. Bone mineral density in women with depression. N Engl J Med. 1996;335(16):1176-81.
28. Whitson HE, Sanders L, Pieper CF, Gold DT, Papaioannou A, Richards JB, et al. Depressive symptomatology and fracture risk in community-dwelling older men and women. Aging Clin Exp Res. 2008;20(6):585-92. 29. Reginster JY, Deroisy R, Paul I, Hansenne M,
Ansseau M. Depressive vulnerability is not an independent risk factor for osteoporosis in postmenopausal women. Maturitas. 1999;33(2):133-7.
30. Bistrovic IL, Roncevic-Grzeta I, Crncevic-Orlic Z, Franciskovic T, Ljubicic R, Crncevic-Orlic A, et al. Connection of depression and bone loss in perimenopausal and postmenopausal women. Coll Antropol. 2012;36(4):1219-23.
31. Ozgoli G, Gharenaz, M.S., Aghadashi, M.A., Salmani, F. assessment of association between depression and osteoporosis in women. urmia medical magazine. 2014;26(1):10-6.
32. Ozsoy S, Esel E, Turan MT, Kula M, Demir H, Kartalci S, et al. [Is there any alteration in bone mineral density in patients with depression?]. Turk Psikiyatri Derg. 2005;16(2):77-82. 33. Altindag O, Altindag A, Asoglu M, Gunes M,
Soran N, Deveci Z. Relation of cortisol levels and bone mineral density among premenopausal women with major depression. Int J Clin Pract. 2007;61(3):416-20.
older women. J Am Geriatr Soc. 2007;55(6):824-31.
35. Freehill AK, Lenke LG. Severe kyphosis secondary to glucocorticoid-induced osteoporosis in a young adult with Cushing's disease. A case report and literature review. Spine (Phila Pa 1976). 1999;24(2):189-93. 36. Coelho R, Silva C, Maia A, Prata J, Barros H.
Bone mineral density and depression: a community study in women. J Psychosom Res. 1999;46(1):29-35.
37. Jilka RL, Hangoc G, Girasole G, Passeri G, Williams DC, Abrams JS, et al. Increased osteoclast development after estrogen loss: mediation by interleukin-6. Science. 1992;257(5066):88-91.
38. Nanes MS. Tumor necrosis factor-alpha: molecular and cellular mechanisms in skeletal pathology. Gene. 2003;321:1-15.
39. Dentino AN, Pieper CF, Rao MK, Currie MS, Harris T, Blazer DG, et al. Association of interleukin-6 and other biologic variables with depression in older people living in the community. J Am Geriatr Soc. 1999;47(1):6-11.
40. Kiecolt-Glaser JK, Glaser R. Depression and immune function: central pathways to morbidity and mortality. J Psychosom Res. 2002;53(4):873-6.
41. Maes M. Major depression and activation of the inflammatory response system. Adv Exp Med Biol. 1999;461:25-46.
42. Oh SM, Kim HC, Ahn SV, Rhee Y, Suh I. Association between depression and bone mineral density in community-dwelling older men and women in Korea. Maturitas. 2012;71(2):142-6.
43. Diem SJ, Harrison SL, Haney E, Cauley JA, Stone KL, Orwoll E, et al. Depressive symptoms and rates of bone loss at the hip in older men. Osteoporos Int. 2013;24(1):111-9. 44. Jacka FN, Pasco JA, Henry MJ, Kotowicz MA,
Dodd S, Nicholson GC, et al. Depression and bone mineral density in a community sample of perimenopausal women: Geelong
Osteoporosis Study. Menopause. 2005;12(1):88-91.
45. Rauma PH, Pasco JA, Berk M, Stuart AL, Koivumaa-Honkanen H, Honkanen RJ, et al. The association between major depressive disorder, use of antidepressants and bone mineral density (BMD) in men. J Musculoskelet Neuronal Interact. 2015;15(2):177-85.
46. Rauma PH, Pasco JA, Berk M, Stuart AL, Koivumaa-Honkanen H, Honkanen RJ, et al. The association between use of antidepressants and bone quality using quantitative heel ultrasound. Aust N Z J Psychiatry. 2015;49(5):437-43.
47. Charles LE, Fekedulegn D, Miller DB, Wactawski-Wende J, Violanti JM, Andrew ME, et al. Depressive symptoms and bone mineral density among police officers in a northeastern US City. Glob J Health Sci. 2012;4(3):39-50.
48. Seeman E. Invited Review: Pathogenesis of osteoporosis. J Appl Physiol (1985). 2003;95(5):2142-51.
49. Greendale GA, Lee NP, Arriola ER. The menopause. Lancet. 1999;353(9152):571-80. 50. Barrett-Connor E, Von Muhlen DG,
Kritz-Silverstein D. Bioavailable testosterone and depressed mood in older men: the Rancho Bernardo Study. J Clin Endocrinol Metab. 1999;84(2):573-7.
51. Amin S, Zhang Y, Felson DT, Sawin CT, Hannan MT, Wilson PW, et al. Estradiol, testosterone, and the risk for hip fractures in elderly men from the Framingham Study. Am J Med. 2006;119(5):426-33.
52. Mussolino ME, Jonas BS, Looker AC. Depression and bone mineral density in young adults: results from NHANES III. Psychosom Med. 2004;66(4):533-7.
54. Heaney RP, Abrams S, Dawson-Hughes B, Looker A, Marcus R, Matkovic V, et al. Peak
bone mass. Osteoporos Int. 2000;11(12):985-1009.
Table 1: Frequency distribution of the elderly based on depression and bone mineral density in Amirkola (91-90).
Variables Number Percentage (%) Depression level Normal 640 9 / 58 Mild 284 1 / 26 Moderate 120 11 Severe 43 4 Depressive symptoms Yes 447 1 / 41 No 640 9 / 58
Total bone mineral density Normal 219 1 / 20 Osteopenia 488 9 / 44 Osteoporosis 380 35
Bone mineral density Lumbar spine Normal 340 3 / 31 Osteopenia 422 8 / 38 Osteoporosis 325 9 / 29 Femur Normal 374 4 / 34 Osteopenia 511 47 Osteoporosis 202 6 / 18
Table 2: Frequency distribution of demographic characteristics based on bone mineral density in the elderly of Amirkola (2011-2012)
Variables Bone mineral density
p-value Normal Number (%) Osteopenia Number (%) Osteoporosis Number (%) Gender Male ) 604 ( ) 5 / 27 ( 166 ) 1 / 56 ( 339 ) 4 / 16 ( 99 001 / 0 < Female ) 483 ( ) 0 / 11 ( 53 ) 8 / 30 ( 149 ) 2 / 58 ( 281 Marital status Married ) 948 ( ) 9 / 21 ( 208 ) 2 / 46 ( 438 ) 9 / 31 ( 302 001 / 0 < Single ) 139 ( ) 9 / 7 ( 11 ) 0 / 36 ( 50 ) 1 / 56 ( 78 Living alone Yes ) 72 ( ) 3 / 8 ( 7 ) 5 / 37 ( 27 ) 2 / 54 ( 39 001 / 0 < No ) 1015 ( ) 0 / 21 ( 213 ) 4 / 45 ( 461 ) 6 / 33 ( 341 BMI Less than 25
) 354 ( ) 1 / 7 ( 25 ) 6 / 46 ( 165 ) 3 / 46 ( 164 001 / 0
Table 3: Frequency distribution of depression and depression level based on bone mineral density in elderly Amirkola (2011-2012)
Table 4: Frequency distribution of depression based on bone mineral density status in the elderly of Amirkola by sex (2011-2012)
Variables bone mineral density
p-value Normal Number (%) Osteopenia Number (%) Osteoporosis Number (%) Male Depression Yes ) 164 ( ) 7 / 20 ( 34 ) 9 / 57 ( 95 ) 3 / 21 ( 35 02 / 0 No ) 440 ( ) 0 / 30 ( 132 ) 5 / 55 ( 244 ) 5 / 14 ( 64 Female Depression Yes ) 283 ( ) 2 / 10 ( 29 ) 4 / 31 ( 89 ) 3 / 58 ( 165 81 / 0 No ) 200 ( ) 0 / 12 ( 24 ) 0 / 30 ( 60 ) 0 / 58 ( 116 Variables Bone mineral density
p-value Normal Number (%) Osteopenia Number (%) Osteoporosis Number (%) Education level Illiterate ) 669 ( ) 5 / 17 ( 282 ) 2 / 42 ( 282 ) 4 / 40 ( 270 001 / 0
< 104(31/4) 160(48/3) 67(20/2) (331)Primary and secondary
High school and university ) 87 ( ) 2 / 40 ( 35 ) 9 / 52 ( 46 ) 9 / 6 ( 6 Occupational status Unemployed ) 73 ( ) 0 / 11 ( 8 ) 5 / 42 ( 31 ) 6 / 46 ( 34 001 / 0 < Housekeeper ) 425 ( ) 0 / 12 ( 51 ) 7 / 28 ( 122 ) 3 / 59 ( 252
retired with a career record ) 251 ( ) 3 / 26 ( 66 ) 2 / 58 ( 146 ) 5 / 15 ( 39
Employed other than housekeeper ) 332 ( ) 4 / 27 ( 91 ) 3 / 56 ( 187 ) 3 / 16 ( 54 Unspecified ) 332 ( ) 0 / 50 ( 3 ) 3 / 33 ( 2 ) 7 / 16 ( 1 Variables bone mineral density
Table 5. Frequency distribution of depression level based on bone mineral density in the elderly of Amirkola by sexes (2011-2012)
Gender Variables
bone mineral density
p-value
Normal
Number (%)
Osteopenia
Number (%)
Osteoporosis
Number (%)
Male Depression
level Normal ) 440 ( ) 30 ( 132 )
5 / 55 ( 244 )
5 / 14 ( 64
04 / 0
Mild ) 118 ( ) 7 / 23 ( 28 )
5 / 58 ( 89 )
8 / 17 ( 21
Moderate ) 38 ( )
8 / 15 ( 6 )
3 / 55 ( 21 )
9 / 28 ( 11
Severe ) 8 ( )
0 ( 0 )
5 / 62 ( 5 )
5 / 37 ( 3
Female Depression
level Normal ) 200 ( ) 0 / 12 ( 24 )
0 / 30 ( 60 )
0 / 58 ( 116
84 / 0
Mild ) 166 ( ) 4 / 11 ( 19 )
5 / 32 ( 54 )
0 / 56 ( 93
Moderate ) 82 ( )
5 / 8 ( 7 )
8 / 26 ( 22 )
6 / 64 ( 53
Severe ) 35 ( ) 6 / 8 ( 3 )
1 / 37 ( 13 )
3 / 54 ( 19