w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Factors
associated
with
osteopenia
and
osteoporosis
in
women
undergoing
bone
mineral
density
test
夽
Ana
Carolina
Veiga
Silva,
Maria
Inês
da
Rosa
∗,
Bruna
Fernandes,
Suéli
Lumertz,
Rafaela
Maria
Diniz,
Maria
Eduarda
Fernandes
dos
Reis
Damiani
UniversidadedoExtremoSulCatarinense,Criciuma,SC,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received10February2014 Accepted17August2014
Availableonline27November2014
Keywords:
Osteoporosis
Dual-energyX-rayabsorptiometry Epidemiology
Metabolicbonediseases
a
b
s
t
r
a
c
t
Theaimofthisstudywastodeterminetheprevalenceofosteopeniaandosteoporosisin a femalepopulation,thathadbonemineraldensity(BMD)measuredbydual-energy X-rayabsorptiometry (DXA)ina specializedclinicinthesouth ofBrazil.We conducteda cross-sectionalstudyincluding1871womenthatperformedscansbetweenJanuaryand December2012. Weconducteda logisticregressionanalysiswithall independent vari-ablesandoutcomes(osteopenia,osteoporosisandfracturerisk).AccordingtoDXAresults, 36.5%ofwomenhadnormalBMD,49.8%werediagnosedwithosteopeniaand13.7%with osteoporosis.Menopauseandageover50yearsoldwereriskfactorsforosteopeniaand osteoporosiswhilepriorhysterectomyandBMIgreaterthan25wereprotectivefactors.For theoutcomeoffractureatanysitetheriskfactorswereageover50yearsold,osteopenia andosteoporosis(OR=2.09,95%CI:1.28–3.40)and(OR=2.49,95%CI:1.65–3.74),respectively. ©2014ElsevierEditoraLtda.Allrightsreserved.
Fatores
associados
à
osteopenia
e
osteoporose
em
mulheres
submetidas
à
densitometria
óssea
Palavras-chave:
Osteoporose Densitometria Epidemiologia
Doenc¸asósseasmetabólicas
r
e
s
u
m
o
Oobjetivodesteestudofoideterminaraprevalênciadeosteopeniaeosteoporoseemuma populac¸ãodemulheresquefizeramexamesdedensitometriaemumaclínicaespecializada nosuldoBrasil.Nósconduzimosumestudotransversal,incluindo1.871mulheresquese submeteramàdensitometriaósseaentrejaneiroedezembrode2012.Foifeitaumaanálise deregressãologísticacomtodasasvariáveisindependenteseosdesfechos(osteopenia, osteoporoseeriscodefraturas).Adensitometriaósseafoidiagnosticadacomonormalem 36,5%dasmulheres,49,8%comosteopeniae13,7%comosteoporose.Estarnamenopausa
夽
Institution:UniversidadedoExtremoSulCatarinense–UNESC,LaboratoryofEpidemiology. ∗ Correspondingauthor.
E-mail:[email protected](M.I.daRosa).
http://dx.doi.org/10.1016/j.rbre.2014.08.011
etermaisde50anosforamfatoresderiscoparaosteopeniaeosteoporose,enquantoter feitohisterectomiaeapresentaríndicedemassacorporal(IMC)maiordoque25foram fatoresdeprotec¸ão.Paraodesfechofraturaemqualquersítio,osfatoresassociadosforam idadeacimade50anoseosteopeniaouosteoporose,(OR=2,09,intervalodeconfianc¸a[IC]: 1,28-3,95%,40)e(OR=2,49,95%CI:1,65-3,74),respectivamente.
©2014ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Osteoporosisisasystemicskeletaldiseasecharacterizedby lowbonemassandmicroarchitecturaldeteriorationofthe bonetissue,resultinginincreasedriskoffractureduetobone fragility.1Itwasrecentlyacknowledgedasoneofthemain publichealthissuesofdevelopedcountries.2
Osteoporosisisdiagnosedbymeasuringthebonemineral density(BMD);abonedensitythatis2.5standarddeviations (SD)ormorebelowtheyoungadultmeanvalue(t-score<−2.5) indicatesosteoporosis.Patientswithbonedensitybetween1 and2.5SDbelowaverage(t-score−1to−2.5)aresaidtohave osteopenia.3
Inwomen,BMDdecreaseswithage,presentingsharpdrop during menopause. It is estimated that one in every two womeninthe UKfromthe ageof50 willsuffersomekind offractureduringtheremainderofherlife.4
Withincreasinglifeexpectancyandanagingpopulation, itisanticipatedthattheimpactofosteoporosisinthe com-ingyearswillhaveasignificantincrease.5Weshouldexpect aneconomicburdenforcurrentandfuturepublichealth sys-temduetothehighprevalenceofosteoporosisandresulting fractures.6
Theaimofthis study was todetermine the prevalence andfactors associatedwithosteopeniaand osteoporosisin womenwhohaveundergonebonemineraldensitytestina specializedservice.
Methods
Across-sectionalstudywasmadewith1871women under-goingbonemineraldensitytestinaspecializedclinicfrom January2012toDecember2012.Theprojectwasapprovedby theResearchEthicsCommitteeofUniversidadeExtremoSul CatarinenseunderProtocolNo.829392012.
Osteopenia and osteoporosis were diagnosed by Dual-energy X-ray absorptiometry (DXA), allowing the BMD to be measuredwiththeGELunarProdigyPrimoequipmentwith software Encore version 13.20. The Lunar Prodigy series showedclinicalaccuracyeven40%highercomparedtoother systems. Astudy suggeststhat BMDmeasurementerror is between5%and8%.7
DXAisconsideredthegoldstandardformeasuringBMD anddiagnosingosteopenia/osteoporosis.DXAresultsare pre-sented by(1)absoluteBMDvalues(g/cm2): absolutevalues areimportantbecausetheyare usedtomonitorchangesin BMDovertime;(2)t-score,calculatedinSD,takingas refer-encethemeanBMDofpeakbonemassinyoungadults.The
diagnosticcriteriaproposedbytheWorldHealthOrganization (WHO)in1994,basedonthe followingdata:up to−1.0SD, normal,from −1.1to−2.49SD,osteopenia,andbelow−2.5 SD,osteoporosis8;(3)Z-score,calculatedonSD,takingas ref-erencethemeanBMDexpectedforindividualsofsameage, ethnicityandgender.
ItisimportanttorecognizethattheDXAresultsdescribed hereareonlyvalidwhenstrictcriteriafortheexam,quality controlandanalysisoftheimagesareobserved.The profes-sionalsresponsiblefortheacquisitionofimages,aswellasfor analyzingandinterpretingthemmustactinaccordancewith recognizedprofessionalqualificationprogramsinthecountry. Theincorrectapplicationofthemethodlimitsitsuse,asinall imagingtests.
General data were taken from the densitometry report and included measurement of weight and height, age, BMI,previousfractures,calciumintake,thyroidmedication, menopause, hormone replacement therapy, symptoms of menopause,hysterectomyandoophorectomy.Agewas cat-egorizedintopercentiles:(1)25thpercentile:aged51yearsor less,(2)between25thand50thpercentile:aged52–57years, (3)between50thand75thpercentile:aged58–65years and (4) abovethe 75thpercentile:aged66 yearsorolder. Other qualitativevariablesweredichotomized.
BMIwascalculatedusingtheformulaweight(kg)/height2 (m).TheDXAdatacollectedincludedBMDvalues(g/cm2)of thefemurneck,preferablytherightone,thetotalfemurand themeanvalueofthelumbarvertebrae(L1-L4).
Descriptive analysis of all variables was performed. A bivariate analysis was performed using the Pearson’s chi-squaretest.
Table1–Characteristicsofthewomenthatperformed DXAscansfromJanuarytoDecember,2012,presented asfrequency(%)oraverage(±SD).
Variable Average± SDorn(%)
Age(yearsold) 59.2 ± 10.5
Weight(kg) 68.7 ± 12.8
Height(m) 1.57 ± 0.06
FemoralneckBMD 0.89 ± 0.27tscore:−1.03 TotalfemoralBMD 0.93 ± 0.15tscore:−0.59 LumbarspineBMD 1.0 ± 0.17tscore:−0.75
BMI(kg/m2) 27.7 ± 5.0
≥24.9kg/m2 592(34.9)
≥25kg/m2 1104(65.1)
Fractures(n=104)
Forearm 45(43.3)
Ribs 24(23.0)
Femur 22(21.2)
Spine 13(12.5)
Calciumintake
Yes 595(31.9)
No 1273(68.1)
DXAdiagnosis
Normal 682(36.5)
Osteopenia 932(49.8)
Osteoporosis 257(13.7)
Useofthyroidmedication
Yes 412(22.1)
No 1455(77.9)
Hysterectomy
Yes 461(24.9)
No 1392(75.1)
Oophorectomy
Yes 332(18.1)
No 1506(81.9)
DXA,dual-energyX-rayabsorptiometry;SD,standarddeviation;n, numberofindividuals;BMD,bonemineraldensity;BMI,bodymass index.
level. Interactionsbetween variables were tested, and they wereallnonsignificantata5%levelofsignificance.
Statistical analysis was performed using the Statistical PackageforSocialSciences(SPSS)version18.0.
Results
Thesampleconsistedof1871womenwho underwentDXA
scaninaspecialized privateclinicinsouth ofSanta
Cata-rina. The average age was 59.2±10.5 years, mean weight
of68.7±12.8 and height of1.57±0.06. Themean BMIwas 27.7±5.0,65.1%had aBMI>25.Theprevalenceoffractures atanysitewasof5.5%;theforearmandribsbeingthemost prevalent(Table1).Itwasfoundthat31.9%ofwomenwere tak-ingcalcium,and22.1%wereonthyroidmedication,24.9%had previouslyhadahysterectomy,and18.1%,anoophorectomy (Table1).
Accordingtothebonemineraldensitytestdiagnosis,36.5% ofwomenwerenormal,49.8%hadosteopeniaand13.7%had osteoporosis(Table1).
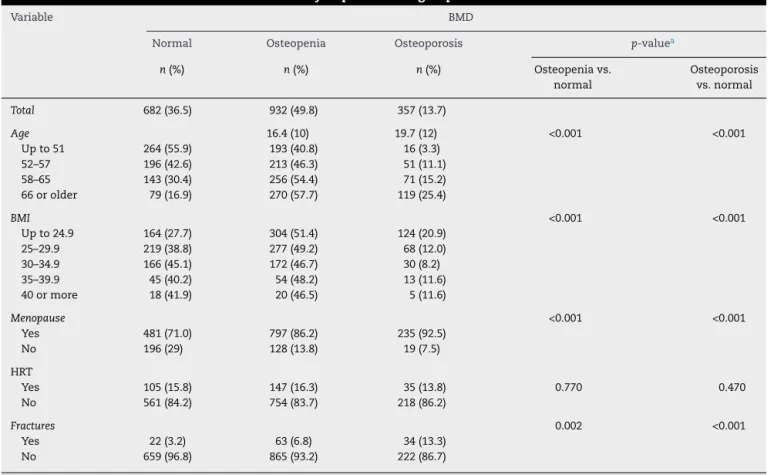
Table2showstheprevalenceofbonemassdensityin differ-entsubgroups,aswellastheanalysisofstatisticalsignificance usingthechi-squaretest.Thelinearincreaseinosteopenia andosteoporosiswasobservedwithadvancingage(p<0.001). TheBMI,however,wasinverselyassociatedwithreducedBMD (p<0.001),i.e.,womenwithhigherBMIhadlessosteopeniaor osteoporosis.
ThecorrelationsbetweentheBMDmeasuredatthespine, femurandfemoralneckandtheBMIwere(r=−0.133,p<0.001,
r=0.590p<0.001andr=0.258,p<0.001),respectively. The BMD atall sites had negative correlation with age (femoral neck r=−0.220, r=−0.337 total femurand lumbar spiner=−0.015,p<0.001).
Themultivariateregressionhadthefollowingoutcomes: osteoporosis,osteopeniaandanyfracture.
Table3showsthefinallogisticregressionmodelforthefirst two outcomes, including the variables mean dichotomized age, menopause, BMI and hysterectomy. One can observe increased risk of osteoporosis for the variables age and menopause.ProtectionwasfoundwithanincreasedBMIand hysterectomy.
Table4showsthefinalfracturemodel,inwhichbeingolder than 50 years old and presenting osteopenia/osteoporosis increasethechancesoffracturesatanysitein2.09and2.49, respectively,whencomparedtowomenaged49yearsorless andwomenwithnormalBMD.
Discussion
Ourstudyuseddatafromaclinicspecializedinthediagnosis ofosteoporosis,sotheprevalenceofosteopeniaand osteo-porosiscannotbeextendedtothegeneralpopulation,being restrictedtoagroupofwomenreferredforaDXAscan.Inthis case,theprevalenceofosteoporosisshould beoverratedin relationtootherpopulationgroups.
AccordingtotheDXAresults,36.5%ofwomenhadnormal BMD,49.8%werediagnosedwithosteopeniaand13.7%with osteoporosis.Theprevalenceofosteopeniaandosteoporosis foundinourstudyshowedalinearincreasewithageinthe fouragepercentilesofthepopulationstudied.
Theprevalencefoundinthis studywas lowerthan that foundinthe literatureon similarstudiesconductedbefore theyear2000.Inastudythatassessedtheprevalenceof osteo-porosisinBrazilianwomen,abovetheageof50,andreferred for bone density test, this prevalence was of40%.9 In the UnitedStates,astudywith600patientsatWayneState Uni-versityinDetroit,foundaprevalenceof52%.10
Table2–Prevalenceofbonemineralmassdensityinpatientssubgroups.
Variable BMD
Normal Osteopenia Osteoporosis p-valuea
n(%) n(%) n(%) Osteopeniavs.
normal
Osteoporosis vs.normal
Total 682(36.5) 932(49.8) 357(13.7)
Age 16.4(10) 19.7(12) <0.001 <0.001
Upto51 264(55.9) 193(40.8) 16(3.3)
52–57 196(42.6) 213(46.3) 51(11.1)
58–65 143(30.4) 256(54.4) 71(15.2)
66orolder 79(16.9) 270(57.7) 119(25.4)
BMI <0.001 <0.001
Upto24.9 164(27.7) 304(51.4) 124(20.9)
25–29.9 219(38.8) 277(49.2) 68(12.0)
30–34.9 166(45.1) 172(46.7) 30(8.2)
35–39.9 45(40.2) 54(48.2) 13(11.6)
40ormore 18(41.9) 20(46.5) 5(11.6)
Menopause <0.001 <0.001
Yes 481(71.0) 797(86.2) 235(92.5)
No 196(29) 128(13.8) 19(7.5)
HRT
Yes 105(15.8) 147(16.3) 35(13.8) 0.770 0.470
No 561(84.2) 754(83.7) 218(86.2)
Fractures 0.002 <0.001
Yes 22(3.2) 63(6.8) 34(13.3)
No 659(96.8) 865(93.2) 222(86.7)
a p-value,chi-squaretest;BMD,bonemineraldensity;BMI,bodymassindex;HRT,hormonereplacementtherapy.
Inbothmale and femaleindividuals,there isabalance betweenboneformationandresorption,butthisbecomes pro-gressivelynegativewithincreasingage.Age-relatedboneloss beginsimmediately afterthepeak bonemass,but mostof thebonelossoccursafterthe ageof65.Men,however,are lesslikelytodeveloposteoporosisthanwomen,fortwo rea-sons: first,theygain morebone massduring pubertyand,
Table3–Logisticregressionmodel,consideringthe outcomevariable–osteopeniavs.normaland osteoporosisvs.normal.
Variable AdjustedOR(CI95%)
Osteopenia Osteoporosis
Age
50yearsorolder 2.80(2.20–3.57) 6.34(4.36–9.23)
Upto49yearsold 1.00 1.00
BMI
25ormore 0.46(0.36–0.59) 0.22(0.15–0.32)
Upto24.9 1.00 1.00
Hysterectomy
Yes 0.67(0.52–0.87) 0.61(0.41–0.92)
No 1.00 1.00
Menopause
Yes 2.17(1.63–2.88) 3.33(1.92–5.77)
No 1.00 1.00
CI,confidenceinterval;BMI,bodymassindex.
second,theyloselessbonemassduringaging,because,unlike
women, mendonotexperienceasudden lossofestrogen.
Elderlylivingatretirementhomesareatgreaterrisk.
Eighty-fivepercentofwomenlivinginnursinghomesover age80
haveosteoporosis.14
Our resultsshowed a linear increaseof osteopenia and osteoporosis withadvancing age.In additiontothe effects onbonemass,theagingalsoincreasestheriskoffractures, regardlessofthebonemass,andanincreaseof20yearsofage meansafourfoldriskoffractures.15
Oxidativestress(OS)isacommonmechanismof pathogen-esisofvariousdegenerativediseasesassociatedwithaging, including osteoporosis.16,17 An increase in reactive oxygen species (ROS) was implicatedin decreased boneformation associatedwithadvancingage,aswellasincreasedresorption
Table4–Finallogisticregressionmodel,consideringthe outcomevariable–anyfracture.
Variable AdjustedOR(CI95%)
Age
50yearsorolder 2.09(1.28–3.40)
Upto49yearsold 1.00
BMD
Osteopenia/osteoporosis 2.49(1.65–3.74)
Normal 1.00
associatedwithestrogendeficiency.16 Inline withthis evi-dence, increased ROSproduction in osteoblasts stimulates apoptosis and decreased bone formation. As ofthe fourth decade,thebone formationislower than the resorption.18 Serumlevelsoftheinsulin-likegrowthhormonethat mod-ulatesthe effectofthe GHinthe bonealso decrease with age.19
Ourstudyshowedahigherprevalenceofforearm,rib,hip andspinefractures,respectively.Accordingtotheliterature, thevertebralfractureisthemostcommonclinical manifes-tation of osteoporosis. Most of these fractures (about two thirds)areasymptomatic,diagnosedasanincidentalfinding on X-ray.20 Hip fractures are relatively common in osteo-porosis and affects 15% ofwomen and 5% of menat the ageof80.Subchondralinsufficiencyfracturesofthefemoral head,resultinginosteopenia,can leadtorapidlossof car-tilage and space-destructiveosteoarthritis.21 In addition to that,fracturesofthedistalradius(Colles’fractures)mayalso occur and are morecommon inwomen after menopause, whilethe risk ofhip fracture increases exponentially with age.
OurresultsshowaninversecorrelationbetweentheBMI andtheriskofosteopeniaandosteoporosis.Publishedstudies showthatlowbodyweight(lessthan58kg)isassociatedwith anincreasedriskofosteoporosisandfractures.Weightlosses aftertheageof50inwomenincreasestheriskofhipfracture, whileweightgainsdecreasesthisrisk.22,23
Menopausewas alsoariskfactor withstatistical signif-icancein ourstudy. Therate ofbone lossin women with postmenopausalhypoestrogenism is probably around 0.5% and1.5%peryear,withasmall percentageofwomenwho are“fastbonelosers”andcanlose3%–5%ofbonemassper year.Therateofbonelossishighlydependentonhormonal factors,environmental and genetic factors.In a longitudi-nalstudywith272healthypre-andperimenopausalwomen, therewas noboneloss inwomenbeyondthe menopause, whileanacceleratedbonelosswasobservedinthe2–3years priortothecessationofmenstruation,withsignificant cor-relation between the rate of bone lost and the elevation offollicle-stimulatinghormone (FSH)and markersof bone metabolism.24–26
Wealsofoundthat hysterectomywould bea protective factor forosteopeniaand could notfind aplausible expla-nationforthisprotection,sinceitgoesagainsttheliterature, whichreportsadecreaseinbonemassafterhysterectomy.27–29 Thisvariableisindependentoftheoophorectomy,whichwas analyzedapartand showednostatistical significance.This analysismaybebiased, sinceconfounding factors,suchas thelifestyleandthereproductivehistoryofthepatients,were notcontrolled.
Conclusion
Ourstudyshowedthattheprevalenceofosteopeniaisgreater thanthat ofosteoporosisand thatoldageand menopause areriskfactorsforbothoutcomes,whileBMIabove25and priorhysterectomywere protectivefactors.For thefracture outcome,thestatisticallysignificantriskswereageabove50 yearsoldandosteopeniaorosteoporosis.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.NIHConsensusDevelopmentPanelonOsteoporosis Prevention,Diagnosis,andTherapy(2001).JAMA. 2001;285:785–95.
2.WorldHealthOrganization.BurdenofdiseaseinDALYsby cause,sex,andmortalitystratuminWHOregions,estimates for2002.TheWorldHealthReportchanginghistory.Geneva: WorldHealthOrganization;2004.p.126–31.
3.WorldHealthOrganization.Assessmentoffractureriskand itsapplicationtoscreeningforpostmenopausalosteoporosis. Geneva:WorldHealthOrganization;1994.p.1–129.Technical ReportSeriesno.843.
4.VanStaaTP,DennisonEM,LeufkensHG,CooperC. EpidemiologyoffracturesinEnglandandWales.Bone. 2001;29:517–22.
5.LaneNE.Epidemiology,etiology,anddiagnosisof osteoporosis.AmJObstetGynecol.2006;194:S3–11.
6.HopkinsRB,TarrideJE,LeslieWD,MetgeC,LixLM,MorinS, etal.Estimatingtheexcesscostsforpatientswithincident fractures,prevalentfractures,andnonfractureosteoporosis. OsteoporosInt.2012[Epubaheadofprint].
7.KuiperJW,VanKuijkC,GrashuisJL,EderveenAG,SchutteHE. AccuracyandtheinfluenceofmarrowfatonquantitativeCT anddual-energyX-rayabsorptiometrymeasurementsofthe femoralneckinvitro.OsteoporosInt.1966;6:25–30.
8.KanisJA,WHOStudyGroup.Assessmentoffractureriskand itsapplicationtoscreeningforpostmenopausalosteoporosis. SynopsisofaWHOReport.OsteoporosInt.1994;4:368–81.
9.TorresR,MarcelinoC,VieiraL,BandeiraF.Prevalênciade osteoporoseem1441mulheresencaminhadaspara determinac¸ãodadensidadeóssea.ArqBrasEndocrinol Metabol.1998;42:S182.
10.NelsonD,MolloyR,KleerekoperM.Prevalenceofosteoporosis inwomenreferredforbonedensitytesting:utilityofmultiple skeletalsites.JClinDensitom.1998;1:5–12.
11.LookerAC,OrwollES,JohnstonCC,LindsayR,WahnerH, DunnW.PrevalenceoflowfemoralboneinolderU.S.adults fromNHANESIII.JBoneMinerRes.1997;12:1761–8.
12.PinheiroMM,dosReisNetoET,MachadoFS,OmuraF,Yang JHK,SzejnfeldJ,etal.Fatoresderiscoparafraturapor osteoporoseebaixadensidadeósseaemmulheresnaprée pós-menopausa.RevSaúdePública.2010;44:479–85.
13.PinheiroMM,ReisN,MachadoET,FelipeFS,YangO,Szejnfeld JH,etal.Riskfactorsforosteoporoticfracturesandlowbone densityinpreandpostmenopausalwomen.RevSaude Publica.2010;44:479–85.
14.BandeiraFC,FreeseE.Prevalênciadeosteoporoseefraturas vertebraisemmulheresnapós-menopausaatendidasem servic¸osdereferência.RevBrasEpidemiol.2007;10:86–98.
15.VuMQ,WeintraubN,RubensteinLZ.Fallsinthenursing home:aretheypreventable?JAmMedDirAssoc.2006;7: S53.
16.HuiSL,SlemendaCW,JohnstonCCJr.Ageandbonemassas predictorsoffractureinaprospectivestudy.JClinInvest. 1988;81:1804.
17.BalabanRS,NemotoS,FinkelT.Mitochondria,oxidants,and aging.Cell.2005;120:483.
18.ManolagasSC.Fromestrogen-centrictoagingandoxidative stress:arevisedperspectiveofthepathogenesisof
19.LipsP,CourpronP,MeunierPJ.Meanwallthicknessof trabecularbonepacketsinhumanliaccrest:changeswith age.CalciformeTissueRes.1978;26:13–7.
20.RudmanD,KutnerMH,RogersCM,LubinMF,FlemingGA, BainRP.Impairedgrowthhormonesecretionintheadult population:relationtoageandadiposity.JClinInvest. 1981;67:1361–9.
21.LindsayR,SilvermanSL,CooperC,HanleyDA,BartonI,Broy SB,etal.Riskofnewvertebralfractureintheyearfollowinga fracture.JAMA.2001;285:320–3.
22.YamamotoT,BulloughPG.Theroleofsubchondral insufficiencyfractureinrapiddestructionofthehipjoint:a preliminaryreport.ArthritisRheum.2000;43:2423.
23.GreenAD,Colón-EmericCS,BastianL,DrakeMT,LylesKW. Doesthiswomanhaveosteoporosis?JAMA.
2004;292:2890–900.
24.VillarealDT,FontanaL,WeissEP,RacetteSB,Steger-MayK, SchechtmanKB,etal.Bonemineraldensityresponseto caloricrestriction-inducedweightlossorexercise-induced
weightloss:arandomizedcontrolledtrial.ArchInternMed. 2006;166:2502–10.
25.ChapurlatRD,GarneroP,Sornay-RenduE,ArlotME,Claustrat B,DelmasPD.Longitudinalstudyofbonelossinpre-and perimenopausalwomen:evidenceforbonelossin perimenopausalwomen.OsteoporosInt.2000;11:493–8.
26.ParkHA,LeeJS,KullerLH,CauleyJA.Effectsofweightcontrol duringthemenopausaltransitiononbonemineraldensity.J ClinEndocrinolMetab.2007;92:3809.
27.WarmingL,HassagerC,ChristiansenC.Changesinbone mineraldensitywithageinmenandwomen:alongitudinal study.OsteoporosInt.2002;13:105–12.
28.HreshchyshynMM,HopkinsA,ZylstraS,AnbarM.Effectsof naturalmenopause,hysterectomyandoophorectomyon lumbarspineandfemoralneckbonedensities.Obstet Gynecol.1988;72:631–8.