ISSN: 1557-4989
© 2014 F. Farzianpour et al., This open access article is distributed under a Creative Commons Attribution (CC-BY) 3.0 license
doi:10.3844/ajabssp.2014.147.152 Published Online 9 (2) 2014 (http://www.thescipub.com/ajabs.toc)
Corresponding Author: Fereshteh Farzianpour, Department of Health Management and Economics, School of Public Health, Tehran University of Medical Sciences, Tehran, Iran Tel: +98 21 44648943 Fax: 982188989129
ASSESSMENT OF QUALITY OF
LIFE IN CANCER PATIENTS
1
Fereshteh Farzianpour,
2Jalil Shojaee,
2Ghasem Abedi and
2Farideh Rostami
1
Department of Health Management and Economics, School of Public Health, Tehran University of Medical Sciences, Tehran, Iran
2
Health Sciences Research Center. Mazandaran University of Medical Sciences, Sari, Iran
Received 2014-01-02; Revised 2014-01-04; Accepted 2014-01-09
ABSTRACT
Standards of Joint Commission International (JCI) emphasize on the organizational performance level in basic functional domains including patient right, patient care, medical safety and infection control. These standards are focused on two principles: Expectations of the actual organizational performance and assessment of organizational capabilities to provide high quality and safe Health Care Services (HCS). The aim of this study was to analyze the regression model of the Quality of Life (QOL) in cancer patients from Mazandaran province in 2013. This descriptive cross-sectional study was carried out on 185 cases after a chemotherapy treatment session during in the first three months that was referred to Rajaee Chemotherapy Center in 2013. The method of sampling was Purposive. General quality of life was assessed using WHO questionnaire (WHOQOL-BREF) and particular life quality was assessed using researcher-developed questionnaire. Data analysis was consisted of a multiple regression method and for comparison one-sample test of Kolmogrov-Smirnov was used. Statistical analysis showed that the average of general life quality, particular life quality and total average was evaluated, 1<0.96<5, 1<1.13<5 and 1<1.04<5, respectively. Due to the low quality of general and particular life, fully integration of the care program of patient care in primary health care system, easy access and facilitation in intervention to improve the quality of life is offered.Our motivation behind the research and the implications of the research was improvement of QOL cancer patients.
Keywords: Assessment, Regression, Quality of Life, Patient, Cancer
1. INTRODUCTION
Patient is the core of all the health care providers’ activities and this issue must be clearly considered in all aspects of the activities, since the disease experience as well as the necessity of adherence to the treatment and following the care increases the patients’ vulnerability and their need for comprehensive support. Moreover, changes in the social conditions have raised the patients’ expectations for their rights (Farzianpour et al., 2013). Standards of Joint Commission International (JCI) emphasize on the
organizational performance level in basic functional domains including patient right, patient care, medical safety and infection control. These standards are focused on two principles: Expectations of the actual organizational performance and assessment of organizational capabilities to provide high quality and safe Health Care Services (HCS) (Farzianpour et al., 2011).
disease is diagnosed with the cell abnormal transformation and loss of cell differentiation. Currently, more than 7 million people in the world lose their lives from cancer and it is expected that the number of new cases will receive from 10 million to 15 million per year by 2020 (Azari and Hassanpour, 2006; Abbastabar et al., 2012). In society, cancer is known as incurable disease and after diagnosis; patients suffer from anxiety and depression result from unrealistic fear of death and loss of happiness in society, as the need for frequent hospitalization and continual concern for patients and their families and cause psychological disorders (Bamshad and Safikhani, 2006). Nowadays, people are demanding improved quality of life, so governments are focused on quality of life, around the world and attempt to reduce morbidity and mortality and promote the mental, Social, physical and health and welfare services (Gugqenmous, 1995). Quality of life is a compound variable that is affected by several variables. Changing in living conditions, health, environmental, psychological stress, family happiness, leisure, social relationship and other variables’ determined the quality of life and its changes (Ali et al., 2011; Farzianpour et al., 2013). The World Health Organization (WHO) defines quality of life as; individual perception if their position in life in the context of the culture and value system in which they live and in relation to their goals, expectations, standards and concerns (Awan et al., 2011). Some studies have shown that disease severity and psychological stress affected on quality of life (Caffey et al., 1999; Farzianpour et al., 2012; Iliopoulou et al., 2013; Ovayolu et al., 2013). In other studies, quality of life has been linked to all factors of cancer disease including the type of treatment, type and severity of cancer (Bare and Smeltzer, 2004; Deng et al., 2013; Li et al., 2013; Ding et al., 2012).
Despite the different definitions, there isn’t the definition that involved different aspects of this concept and this provides the ability to evaluate quality of life in cancer patients against other groups (Farzianpour et al., 2012; Rostami et al., 2009). The main goal of care and treatment of chronic diseases is a life satisfaction and being healthy. Researchers found that the most important factor which had affected the quality of life was related to mental health was anxiety in chronic patients with is for 65 years old, but the low education level and unemployment were main
factors in over 50 years of age (Gholamzadeh et al., 2005; Distefano and Riccardi, 2008).
There was association between the high level of mental tension with the disorders in physical, mental and social functions in the study of America Cancer Society’s of Behavioral Research Center Studies on 739 people of the patient’s family (Baker et al., 2008).
In the other hand, these various psychological and social problems cause disorders in the natural process of life quality. In one study on 200 cancer patients 34% of patients didn’t have a good quality of life (Azari and Hassanpour, 2006). According to previous research, all studies are agreed on the decrease of life quality with disease progression. But present study respected to this topic that people have different goals, expectations, standards and priorities according to their position in terms of culture and value system that cannot be viewed by others. So, the present study has assessed the quality of life with a new approach to patient group using two general and particular questionnaires with a method of statistical models. Perhaps assessment the quality of life in a group of people in different situations is considered as a new step for comparison using mathematical techniques to solve problems in medical sciences and other health problems. So the aim of this study was analyzing the quality of the life in cancer patients using a multiple regression model in cancer patients from Mazandaran province in 2013.
2. MATERIALS AND METHODS
weights”) and measuring of the “model fitness” were use for the analysis of quality. In this survey, firstly of all the independent variables were scored and secondly, their proportional share estimated in dependent variables, then the score of each independent variable was done according to its effect on the dependent variable. These numerical values are called “regression weights” or efficiencies. Finally, after standardization of scores or efficiencies, ranking of independent variables were compared with each other (Alavian et al., 2006). The experimental model of the measuring of life quality contains the hierarchical structures: Criteria, sub-criteria and effective criteria in the process of measuring of life quality which make different levels of this model (Bernstein, 2006). This model has been described in four levels (Table 1-4). The first level is the total life quality. The second level consists of 2 criteria including: General and particular quality of life. Third level consist of 4 sub-criteria including: Physical health, mental health, social relations and environment health for general quality of life and sub-criteria like: Physical symptoms, activity, fatigue, emotional and anxious for particular quality of life the forth level of the model is the analyzing to more sub-criteria. For analyzing of data, the multiple
regressions and for comparing results the one-sample test of Kolmogorov-Smirnov have been used.
3. RESULTS
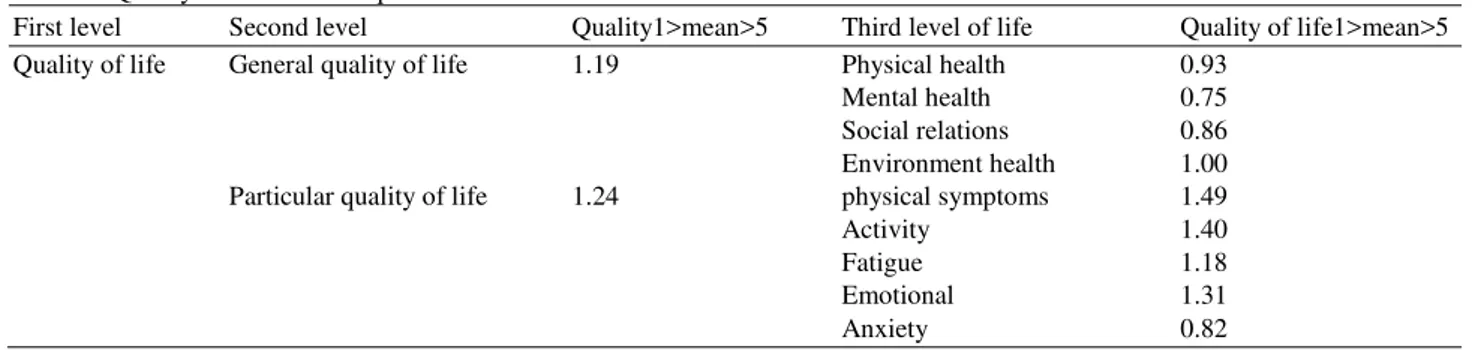
According to finding which were obtained from one-sample t-test and data distribution in two groups of patients (women and men) was normal (p<0.03). So, according to normal distribution, quality of life in woman was lower than men and general and particular quality of life in second level was assessed weak with 1<1.19<5 and 1<1.24<5 score, respectively (Table 1).
To rank the criteria and sub-criteria of life quality, the multiple regression models was used for analysis.
β Coefficient in patients group for General and particular quality of life were 0.226 and 0.319, respectively. Among the all sub-criteria in general quality of life, mental health with β = 0.273 and in the particular quality of life, anxiety with β = 0.483 were contained the higher relative importance (Table 2).
Table 3 and 4 showed that the Situation of
general Quality of Life (QOL) in cancer patients were in third and forth levels (environmental Health = 1) and (physical symptoms = 1.49).
Table 1. Quality of life in cancer patients as the criteria and the sub-criteria
First level Second level Quality1>mean>5 Third level of life Quality of life1>mean>5
Quality of life General quality of life 1.19 Physical health 0.93
Mental health 0.75
Social relations 0.86
Environment health 1.00
Particular quality of life 1.24 physical symptoms 1.49
Activity 1.40
Fatigue 1.18
Emotional 1.31
Anxiety 0.82
Table 2. The importance of the criteria and sub-criteria of life quality according to β Coefficient
First level Second level Β coefficient Third level β coefficient
Quality of life General quality of life 0.226 Physical health 0.234
Mental health 0.184
Social relations 0.227
Environment health 0.259
Particular quality of life 0.319 physical symptoms 0.320
Activity 0.315
Fatigue 0.371
Emotional 0.316
Table 3. Situation of general quality of life in cancer patients as criteria and sub-criteria of third and forth levels
Second Third Quality of Forth Quality of life
level level life1>mean>5 level 1>mean>5
General qualityof life Physical health 0.93 Enoughenergy 0.88
Appearance 0.95
Mobility 0.79
Physicalability 1.10
Mental health 0.75 Life satisfaction 0.68
Significant of life 0.54
Focus 0.86
Self satisfaction 0.88
Work capacity 0.74
Sex relations 1.00
Disappointment 0.60
Stress 0.70
Social relationship 0.86 Relationship with other 1.01
members of family members
Relationship with 0.82
Neighbors
Relationships with colleagues 0.72
Visit others 0.75
Agreement withothers and self 1.00
Security 1.06
Healthy living environment 1.20
Environmental health 1.00 Access toinformation 0.84
Recreationalactivities 0.94
Life location 0.96
Access to healthservices 1.00
Table 4. Situation of general quality of life in cancer patients as criteria and sub-criteria of third and forth levels
Second Third Quality of Forth Quality of
level life level 1<mean<5 level life<mean<5
Particular quality of life Physical symptoms 1.49 Pain feeling 1.10
Disruption in work 1.80
Treatment
Physical ability 1.07
Activity 1.30 Daily activities 1.70
Daily walking 1.20
Exercises 1.03
Fatigue 1.18 Fatigue during daily working 1.18
Daily walking 1.20
Fatigue during exercising 1.36
Fatigue at sometimes 0.98
Emotional 1.31 Loneliness feeling 1.30
Inappropriate compassion
from around 1.02
Nostalgia 1.60
Anxiety 0.82 Stress 0.94
Depression 0.80
Anxious 0.75
Being concerned about
their future 0.67
Concerned about future wife 1.00
4. DISCUSSION
Results showed that the General life quality in cancer patients was weak (1<1.1<5), also, in second level general quality of life was lower (1<1.13<5) than particular quality of life (1<0.96<5). The mean of life quality in women with breast cancer under 50 years old in Sammarco (2001) study has been reported average. Rustoen (1995) study stated that different cancers have different effects on quality of life because they cause specific problems and complications that can be different with other cancers. About sub-criteria of general quality of life, environmental health (1<1<5) was highest and emotional health was lowest (1<0.75<5) and in particular quality of life, physical symptoms was highest (1<1.49<5) and anxious was lowest quality. Bernstin believes that attention to life quality is the main concerns of chronic patients and stated that patents care should propel to maintain life quality such as the ability of maintain job, the ability to maintain relationship with friends, wife and children, the ability of continued happiness and enjoyment of pleasant situation (Bernstein, 2006). As shown in Table 2, general life quality with 0.226 of coefficient (β) had the lowest effect on the total quality of life than particular quality of life with 0.319 of coefficient (β). Sub-criteria of the third level included mental health, social relations and physical and environment health with β coefficient; 0.259, 0.227, 0.184 and 0.234, respectively were effective on general life quality. Also, Sub-criteria of the third level such as Anxious, emotional, fatigue, activity, abdominal symptom with β
coefficient; 0.273, 0.316, 0.371, 0.315 and 0.320, respectively were effective on particular life quality. Based on Ghanbari’s research, in his study stated that age, gender, AST, clinical symptoms, mental and physical health with β coefficient like 0.33, 0.18, 0.19, 0.35, 0.14 and 0.15, respectively are effective on life quality. Physical health as an interface factor change 95% of score of life quality and mental health change it 78%. In total, 58% of changes in life quality fit with this model. The important point is that disease associated with the β coefficient of 0.36 has more effect on mental health in comparison with other independent variables and clinical symptoms with 0.35 of impact coefficient has a direct effect on life quality. Physical health and mental health with 0.15 and 0.14 of β coefficient, respectively affected the life quality (Ghanbari et al., 2010; Annunziata et al., 2013). Study of Abedi et al. (2012) showed that physical
health with 0.224 β coefficients had the highest effective and environmental health with 0.242 β
coefficients the lowest effect on the quality of life.
5. CONCLUSION
The variables of disease in current study were not included due to unclear stages of cancer disease. According to results, it can be suggested that increasing in the number of samples and interfering of structures and other methods of comprehensive and intervention model can help to pay attention to quality of life in these patients from other views. B y integration of cares of cancer patients in Primary Health System (PHC) via more extensive care and comprehensive education can improve the quality of life of these patients.
6. ACKNOWLEDGEMENT
This article has been prepared as a research by full support and sponsorship of the esteemed Head of the Research and Technology Department. The authors would like to thank all the people who helped us in gathering the data especially patients.
7. REFERENCES
Abbastabar, H., H. Fard, P. Soleymani and M. Dodaran, 2012. The relationship between breast cancer and the most common noncontiguous disease risk factors: An ecologic study. Health Syst. Res. J., 8: 11-17.
Abedi, G.H., A. Ahmadi and F. Rostami, 2012. Assessment of quality of life in hepatitis B patients compared with healthy people. Life Sci. J., 9: 5339-5343.
Alavian, S.M., N.A. Asadi, A. Mehran, A. Pourdehkordi and M. Zandi, 2006. Effect of interferon education on the quality of life at chronic hepatitis patients. Ali, M., M.A. Aslam, M.S. Awan and M. Waqas, 2011.
Status of health related quality of life between HBV and HCV patients of Pakistan. Int. J. Bus. Soc. Sci., 2: 213-220.
Annunziata, M.A., E. Bidoli, B. Muzzatti and S. Mella, 2013. Fatigue, quality of life and mood states during chemotherapy in Italian cancer patients. Tumori, 99: 28-33. PMID: 3549018
Azari, E. and A. Hassanpour, 2006. Quality of life and related factors in cancer patients. Ahvaz Univ. Med. Sci., 42-50.
Baker, F., B.A. Matthews, Y. Kim, R.L. Spillers and D.K. Wellisch, 2008. Family caregivers and guilt in the context of cancer care. Psychosomatics, 49: 511-519. DOI: 10.1176/appi.psy.49.6.511
Bamshad, Z. and F. Safikhani, 2006. Assessment of mental health of women with breast cancer. Ahvaz Univ. Med. Sci., 56-70.
Bare, B. and S. Smeltzer, 2004. Textbook of Medical Surgical Nursing. 1st Edn., Lippincott Co., Philadelphia.
Bernstein, D., 2006. Health related quality of life. Herpetology, 26: 1-3.
Caffey, M., L. Deichelbohrer and L.L. Northouse, 1999. The quality of life of African American women with breast cancer. Res. Nurs. Health, 22:
449-460. DOI:
10.1002/1098-240X(199912)22:6<449::AID-NUR3>3.0.CO;2-A Deng, M., Y. Lan and S. Luo, 2013. Quality of
life estimate in stomach, colon and rectal cancer patients in a hospital in China. Tumour Biol. J. Int. Soc., 17: 19-30.
Ding, Y., D. Pang, Q. Lu, L.Q. Sun and P. Yang, 2012. Quality of life in cancer patients with pain in beijing. Chin. J. Cancer Res., 24: 60-66. DOI: 10.1007/s11670-012-0060-8
Distefano, M. and S. Riccardi, 2008. Quality of life and psychological distress in locally advanced cervical cancer patients administered pre-operative chemo radiotherapy. Gynecol. Oncol., 111: 144-150. DOI: 10.1016/j.ygyno.2008.06.034 Farzianpour, F., L. Godarzi, A.T. Hamedani, R. Askari
and S.S.H. Hosseini, 2013. Evaluation of customer relationship management in a teaching hospital. Am. J. Applied Sci., 10: 344-352. DOI: 10.3844/ajassp.2013.344.352
Farzianpour, F., R. Askari, A.T. Hamedani, G. Khorshidi and S. Amirifar et al., 2011. Accreditation of emergency department at a teachinghospital in Tehran. Am. J. Econ. Bus. Admin., 3: 498-505. DOI: 10.3844/ajebasp.2011.498.505
Farzianpour, F., S. Gray, A.R. Foroushan, M. Arab, S. Hosseini, 2013. Evaluating the average access to care and continuity of care patients in Tehran teaching hospitals. Health, 5: 2110-2115. DOI: 10.4236/health.2013.512288
Farzianpour, F., S.H. Hosseini, M. Rostami, S.H. Pordanjani and S.M. Hosseini, 2012. Quality of life of the elderly residents. Am. J. Applied Sci., 9: 71-74. DOI: 10.3844/ajassp.2012.71-74.74
Ghanbari, A., R. Farmanbar and F. Mansourghanaii, 2010. Survey of life quality on patients with hepatitis C and compare it with healthy people and presentation a structure model.
Gholamzadeh, S., S. Mohebbi, M. Saberi-Firoozi, F. Sharif and H.R Tabatabaee, 2005. Effects of psycho educational intervention on health-related Quality of Life (QOL) of patients with chronic liver disease referring to Shiraz University of medical sciences. Health Q. Life Outcomes, 3: 81-85. DOI: 10.1186/1477-7525-3-81
Gugqenmous, H., 1995. Quality of Life and Health. 1st Edn., Blackwell-Wisenchafet, Berlin.
Iliopoulou, M.A., B.E. Kitchell and V. Yuzbasiyan-Gurkan, 2013. Development of a survey instrument to assess health-related quality of life in small animal cancer patients treated with chemotherapy. J. Am. Vet. Med. Assoc., 242: 1679-1687. DOI: 10.2460/javma.242.12.1679
Li, K., J.P. Li, M.J. Huang, R. Zhang and Y.J. Hu, 2013. Quality of life of elderly chinese rectal cancer patients after preventative anal surgery: A cohort study. Hepato-Gastroenterol., 8: 128-135.
Ovayolu, N., O. Ovayolu and S. Serce, 2013. Pain and quality of life in Turkish cancer patients. Nurs. Health Sci., 11: 14-21.
Rostami, M., S.B. Pordanjani, F. Farzianpour and A. Rasekh, 2009. Effect of orem self care model on ederies’ quality of life in health care centers of Masjed Solaiman in 2007-2008. J. Arak Univ. Med. Sci. Original Article, 12: 51-59.
Rustoen, T., 1995. Hope and quality of life, two central issues for cancer patients: A theoretical analysis. Cancer Nurs., 18: 355-361.