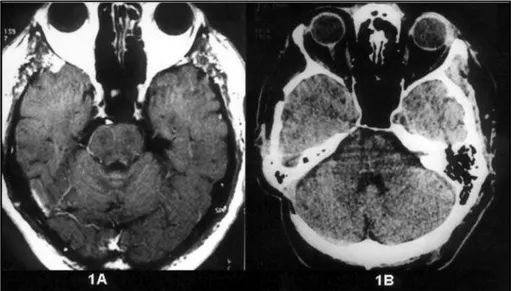
Primary melanoma of Meckel's cave: case report
Texto
Imagem
Documentos relacionados
The probability of attending school four our group of interest in this region increased by 6.5 percentage points after the expansion of the Bolsa Família program in 2007 and
Se a pupila estiver relaxada demais e mostrar um tônus insatisfatório, os músculos da íris (que refletem a musculatura do corpo todo) estarão flácidos. Se a pupila estiver
Cryptococcosis is the most common fungal infection of the central nervous system (CNS) and the second opportunistic disease observed in AIDS pati- ents 5-7,10.. However,
We report a case of primary acquired corneal melanosis without atypia associated with corneal haze in a patient with a history of limbal malignant melanoma and the effect
enquanto Ãquivalenz- como uma constante restrita, especifica para um objetivo e rigorosamente científica - tornou-se estática e unidimensional, equivalence (sem le var em
A promulgação da lei nº 12.527, em 18 de novembro de 2011, a qual ficou conhecida com a Lei de Acesso à Informação Pública (LAI), vem para cumprir esse desiderato, a fim de elevar, na
This report is a review of the most relevant contributions of nonconventional magnetic res- onance techniques to the imaging diagnosis of primary central nervous system lymphoma,
101 meios para obter informações sobre os museus, determinados conteúdos ou eventos, e alguns dos visitantes inquiridos ter referido que a rede social Facebook
