w w w . r b o . o r g . b r
Original
Article
Association
between
bone
mass
and
functional
capacity
among
elderly
people
aged
80
years
and
over
夽
Vanessa
Ribeiro
dos
Santos
a,
Diego
Giulliano
Destro
Christofaro
b,
Igor
Conterato
Gomes
c,
Jamile
Sanches
Codogno
b,
Lionai
Lima
dos
Santos
b,
Ismael
Forte
Freitas
Júnior
a,b,∗aPostgraduateProgramonMotricitySciences,UniversidadeEstadualPaulista,RioClaro,SP,Brazil bDepartmentofPhysicalEducation,UniversidadeEstadualPaulista,PresidentePrudente,SP,Brazil
cDoctoralProgramonEpidemiologyinPublicHealth,UniversidadedeSãoPaulo,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received17August2012
Accepted28November2012
Keywords:
Aged80andover
Bonedensity
Femur
a
b
s
t
r
a
c
t
Objective:Analyzedtheassociationofbonemasswiththefunctionalcapacityofelderlyaged
80ormore.
Methods:Thesampleconsistedof93elderlyaged80and91years(83.2±2.5years)being61
women(83.3±2.7years)and32men(83.1±2.2years)livinginthecityofPresidentePrudente–
SãoPaulo/Brazil.Theassessmentofbonemasswasrealizedbyabsorptiometrydual-energy
X-ray(DXA),wherehavebeenmeasuredvaluesbonemineralcontent(BMC)andbone
min-eraldensity(BMD)ofthefemurandspine(L1–L4).Thefunctionalcapacitywasevaluatedby
meansofwalkingspeedtests,staticequilibriumandstrengthoflowerlimbscontainedinthe
questionnaireWellnessHealthandAging(SABE).Thevariablesofbonemassandfunctional
capacitywerecategorizedaccordingtothemedianvaluesandscoretests,respectively.For
statisticalanalysiswecarriedoutthechi-squaretest,thesoftwareusedwasSPSS(13.0)and
thesignificancelevelwassetat5%.
Results:Elderlymalewithhigherperformanceinthefunctionaltestsshowedhigherfemur
BMCcomparedtolowerperformance,resultnotfoundwhenevaluatedwomen.
Conclusion:Thus,theboneofthefemurfortheoldestoldmaleisassociatedwithfunctional
capacity.Theconstantassessmentofthebonemineralmassandpractiveofphysicalactivity
throughoutlifewouldbemeasurestopreventfallsintheelderly.
©2013SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora
Ltda.Allrightsreserved.
Associac¸ão
entre
massa
óssea
e
capacidade
funcional
de
idosos
com
80
anos
ou
mais
Palavraschave:
Idosode80anosoumais
r
e
s
u
m
o
Objetivo:Analisaraassociac¸ãoentreamassaósseaecapacidadefuncionaldeidososcom
80anosoumais.
夽
WorkperformedattheSchoolofSciencesandTechnology,UniversidadeEstadualPaulista,PresidentePrudente,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](I.F.FreitasJúnior).
2255-4971/$–seefrontmatter©2013SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditoraLtda.Allrightsreserved.
Conteúdomineralósseo Fêmur
Métodos: Aamostrafoicompostapor93idososentre80e91anos(83,2±2,5anos),61
mul-heres(83,3±2,7anos)e32 homens(83,1±2,2anos)dacidadedePresidentePrudente.A
avaliac¸ãodamassaósseafoifeitapelaabsorptiometriadeduplaenergiaderaiosX(DXA),
naqualforammensuradososvaloresdeconteúdomineralósseo(BMC)edensidade
min-eralóssea(BMD)dofêmuredacoluna(L1–L4).Acapacidadefuncionalfoiavaliadapormeio
dostestesdevelocidadeparacaminhar,equilíbrioestáticoeforc¸ademembrosinferiores
contidosnoquestionárioSaúde,Bem-EstareEnvelhecimento(Sabe).Asvariáveisdamassa
ósseaecapacidadefuncionalforamcategorizadasdeacordocomosvaloresdemedianae
apontuac¸ãoobtidanostestes,respectivamente.Paratratamentoestatísticofez-seoteste
qui-quadrado,osoftwareusadofoiSPSS(13.0)eoníveldesignificânciaestabelecidofoide
5%.
Resultados: Osidososdosexomasculinocommaiordesempenhonostestesfuncionais
apresentarammaioresvaloresdeBMCdefêmurcomparadoscomosdemenordesempenho,
resultadonãoencontradoquandoavaliadasasmulheres.
Conclusão: Dessaforma,amassaósseadofêmurparaidososlongevosdosexomasculino
estáassociadaàcapacidadefuncional.Aavaliac¸ãoconstantedamassamineralósseaea
práticadeatividadefísicaaolongodavidaseriammedidasparaprevenc¸ãodasquedasem
idosos.
©2013SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier
EditoraLtda.Todososdireitosreservados.
Introduction
Withincreasinglifeexpectancyandlongevity,occurrencesof
healthcomplication havealsobeen increasing. These may
includediminishedbonemass,whichisgenerallycausedby
disproportionbetweentheactivitiesofosteoclastsinrelation
toosteoblasts,inwhichthereisgreaterconsumptionand/or
lowerproductionofbone.1Thissituationmayleadto
devel-opmentofosteoporosisinolderindividuals.
Diminished bone mass and advanced age can be
con-sidered to be two of the main risk factors for fractures.2
Bonefracturesareoneofthemaincausesofmorbidity,
mor-talityand hospitalization amongthe elderly and represent
oneofthe biggestpublic healthproblems.3 However,their
developmentandconsequencescanbereducedbyadopting
preventivestrategiessuchasexaminationusingthetechnique
ofdual-energy X-rayabsorptiometry(DXA),whichwas
cre-atedinthe1980s.4Thishasthecapacitytoprovideprecise
bone mineral density (BMD) measurements and thus may
contributetowardsorganizingstrategiesformaintainingBMD
withinappropriatevalues.
Diminishedbonemassalsohasaninfluenceonthe
func-tionalstateofolderindividuals.5Oneoftheoptionsforeasing
thephysiologicalalterationsthatoccurinthe
musculoskele-tal system due to the aging process, and for maintaining
functionalcapacity,istoregularlypracticephysicalexercise
throughoutlife.Exercisecausesweighttobeplacedon
spe-cificboneregions,whichgeneratestensionordeformationas
anexternalstimulusandprovidesanosteogeniceffect.6
For better diagnosis, it is important to choose the best
regionsfordetermining bonemass.The lumbarspineand
thetotalfemurarethemostpreciselocalities.7Italsoneeds
tobeemphasizedthatwithadvancingage,oneofthe
great-estfractureratesamongelderlypeopleisintheregionofthe
femur.7,8However,thereisascarcityofstudiesinthe
litera-tureinvestigatingtherelationshipbetweenbonemassinthe
totalfemurandlumbarspineregionsandfunctionalcapacity
amongelderlypeopleaged80yearsandover.Thus,theaim
ofthepresentstudywastoanalyzetheassociationbetween
bonemassandfunctionalcapacityamongelderlypeopleaged
80yearsandover.
Material
and
Methods
Sampling
Thiswasastudywithacross-sectionaldesignthatwas
con-ducted inthe city ofPresidentePrudente betweenOctober
2009andMay2010.Thiscityhas210,000inhabitants9andis
locatedinthewestofthestateofSãoPaulo,withaHuman
DevelopmentIndex(HDI)of0.846(ranked14thinthestate).10
AccordingtotheBrazilianInstituteforGeographyand
Statis-tics(IBGE),thenumberofBraziliansaged80yearsandover
waspredictedtobe2,653,060in2009,i.e.1.1%ofthecountry’s
population.Fromthisprinciple,thecurrentestimateforthe
numberofelderlypeoplewithinthisagegroupinPresidente
Prudenteis2100inhabitants.TheMunicipalHealth
Depart-mentsuppliednames,addressesandtelephonenumbersof
individualsaged80yearsandover.Fromthisinformation,226
individualswererandomlydrawnandwerecontactedby
tele-phone.Thosewhowereunabletowalk,werebedridden,lived
intheruralzone,wereinstitutionalizedorusedpacemakers,
andthosewhosedatainourdatabasewereincomplete,were
excludedfromthesample.Inthismanner,thesampleforthe
presentstudywascomposedof93individualsofbothsexes.
The individuals who were invited to participate in the
present studyweregivenexplanationsaboutthe objectives
ofthestudyandthemethodologyusedtogatherdata,and
theyweretoldthattheycoulddropoutofthestudyatany
time.Onlythosewhosignedthefreeandinformedconsent
statementformedpartofthesample.Alltheprotocolswere
reviewedandapprovedbytheResearchEthicsCommitteeof
UniversidadeEstadualPaulista(Proceduralnumber26/2009).
participatinginthestudyhadaccesstotheresultsfromthe
teststhattheyunderwent.
BoneMass(FemurandSpine)
Toanalyzethebonemassofthetotalfemurandlumbarspine
(L1–L4),a dual-energyX-rayabsorptiometry(DXA)machine
wasused(Lunar,modelDPX-MD;software4.7).TheDXA
tech-niqueisbasedonmeasuringtheattenuationbythepatient’s
body,ofabeamofradiation generatedby anX-raysource
withtwo energylevels. Theexposureto radiation islower
thanthatofconventionalX-rayexaminations.Thetechnique
makesitpossibletoestimatethe bonemassforthe entire
bodyand perbody segment.Thedurationofthe
examina-tion isapproximately15min.Themeasurementmethod is
simpleanddoesnotrequireanyassistancefromthe
individ-ualunderevaluation,whoshouldremainpositionedindorsal
decubitus,withoutmakingmovements insidethemachine.
Theresultsweretransmittedtoacomputerthatwas
intercon-nectedwiththeapparatus.Thebonemineralcontent(BMC)
andbonemineraldensity(BMD)weresubsequentlyanalyzed
andcategorizedaccordingtomedianvalues.Elderly
individ-ualswhoseBMCandBMDwereabovethemedianvalueswere
consideredtohavehigherBMCandBMD,whilethosebelow
themedianwereconsideredtohavelowerBMCandBMD.
FunctionalCapacity
Functionalcapacitywasanalyzedbymeansofthe testson
staticbalance,walking speed and lower-limbstrength that
appearinsectionLoftheSABEquestionnaire.11Thebalance
testhadthreestages,whichweredoneinsequence(10seach).
Inthefirststage,theelderlyindividualneededtostandup,
withfeettogether;inthesecondstage,standwiththeheelof
onefootnexttothebigtoeoftheotherfoot;andinthethird
stage,standwithonefootinfrontoftheother.Thescores
fromthethreestagesweresummedandthefinalresultwas
obtainedfromthesum.
Inthewalkingtest,theelderlyindividualneededtowalk
forthreemetersatthesamespeedusedtoperformhisdaily
activities.Thetimetakenwasmeasuredandregisteredbythe
evaluators.
Toevaluatelower-limbstrength,the testofstandingup
from andsitting downon achairwasapplied. Inthis,the
elderlyindividualhadtokeephisarmscrossedonhischest
andthen,onasignalfromtheevaluator,hadtostandupfrom
andsitdownonachairasquicklyaspossible,fivetimes
with-outanypause.Individualswhowereunabletodothetestin
lessthan60sweredisqualified.
Thescoresforeachtestrangedfrom0to4points.To
clas-sifytheelderlyindividuals’performance,thesumofthescores
obtainedinthethreetestswasused.Individualswere
consid-eredtopresentlowerfunctionalcapacityiftheirscorewas0–2
points,andhighercapacityiftheirscorewas3–4points.
StatisticalAnalysis
For the numerical variables, the normality of the dataset
was analyzed using the Kolmogorov–Smirnov (K–S) test.
SincethedatafittedintoaGaussiandistributionmodel,the
Table1–Descriptionofthesample,accordingtosex.
Variables Mean± SD P
Male(n=32) Female(n=61)
Age(years) 83.1±2.2 83.3±2.7 0.684
Weight(kg) 71.5±15.6 57.4±11.1 ≤0.001
Height(cm) 164.3±7.1 149.8±6.8 ≤0.001
FemoralBMC(g) 33.1±6 23.0±5.6 ≤0.001
SpinalBMC(g) 73.3±19.3 45.1±12.5 ≤0.001 FemoralBMD(g/cm2) 0.89±0.14 0.74±0.15 ≤0.001 SpinalBMD(g/cm2) 1.16±0.24 0.93±0.17 ≤0.001
BMC:bonemineralcontent;BMD:bonemineraldensity.
descriptive statistical analysiswas composed ofmean val-ues(centraltrend)andstandarddeviations(dispersion).The individualsweredistributedaccordingtosexandthemean values for each variable were compared according to sex, withanalysis bymeansofStudent’st-testforindependent samples.
The chi-square test was used to test the association between performance in the functional capacity tests and bonemass.ThestatisticaltreatmentwasdoneusingtheSPSS software(SPSSInc.,Chicago,IL,USA),version13.0,and the significancelevelwassetat5%.
Results
The values presented in Table 1 are expressed as means
and standard deviationsof the generalcharacteristics and
variables ofthebonemassofthesamplestudied,stratified
accordingtosex.Therewasnodifferenceregardingtheage
oftheelderlypeopleparticipatinginthestudy.Thevariables
of weight, height, femoral BMC, spinal BMC, femoralBMD
and spinalBMD (P≤0.001)presented significant differences
betweenthegroups.
In Table 2, the percentage values of the associations
betweenthevariablesofbonemassandperformanceinthe
threefunctional tests,according tosex,arepresented.The
elderlymenwithbetterperformanceinthefunctionaltests
presented higher femoralBMC valuesthan did those with
worseperformance(P≤0.001),whiletherewerenosignificant
differences relatingtothe variablesofspinalBMC,femoral
BMDorspinalBMD.Inthefemalegroup,therewereno
differ-encesinperformanceinthefunctionaltestsinrelationtothe
bonemassvariables.
In Table 3, the percentage values of the associations
betweenthebonemassvariablesandtheperformanceineach
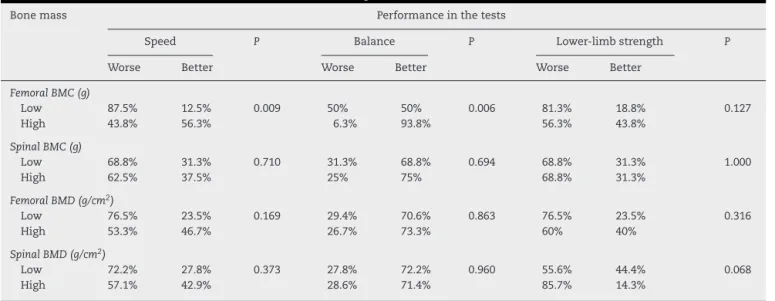
ofthefunctionaltestsinthemalegrouparepresented.The
elderlymenwithbetterperformanceinthespeedandbalance
testspresentedhigherfemoralBMCvaluesthandidthosewith
worseperformance(P=0.009and0.006,respectively).The
vari-ables ofspinalBMC,femoralBMDand spinalBMDdidnot
presentsignificanceinanyofthetests.
In Table 4, the percentage values of the associations
betweenthevariablesofbonemassandtheperformancein
eachofthefunctionaltestsinthefemalegrouparepresented.
Therewerenodifferencesinperformanceinthefunctional
Table2–Associationbetweenbonemassandperformanceinthethreefunctionaltestsonelderlypeopleofbothsexes.
Bonemass Male Female
Performanceinthetests P Performanceinthetests P
Worse Better Worse Better
FemoralBMC(g)
Low 81.3% 18.7% ≤0.001 54.8% 45.2% 0.705
High 18.8% 81.2% 50% 50%
SpinalBMC(g)
Low 56.3% 43.7% 0.480 61.3% 38.7% 0.160
High 43.8% 56.2% 43.3% 56.7%
FemoralBMD(g/cm2)
Low 64.7% 35.3% 0.077 55.3% 44.7% 0.573
High 33.3% 66.7% 47.8% 52.2%
SpinalBMD(g/cm2)
Low 50% 50% 1.000 57.6% 42.4% 0.311
High 50% 50% 44.4% 55.6%
BMC:bonemineralcontent;BMD:bonemineraldensity.
Discussion
Decreasesinbonemassinhumansstarttooccuraroundthe ageof40years.12Ifnopreventiveactionistaken,thisprocess
maycontributetowardsdevelopmentofosteoporosis.13
BMDistheindicatormostusedforanalyzingbonemass
andfordiagnosingosteoporosis.7,14,15However,inadditionto
BMD,BMC isalsoagoodindicator forboneloss.Itsuse is
important,becauseittakesintoconsiderationmorethanjust
themorphologicalbasisofboneloss(diminutionofperiosteal
appositionandendostealboneloss,whichrelatestolossfrom
thetrabecular, endocorticalandintracorticalsurfaces).16 In
thestudybyGuptaet al.12 onpostmenopausalwomen,the
BMCreducedsignificantlywithage.Inourstudy,thefemoral
BMCoftheveryelderly oldmenwas thebonecomponent
thatwasmostassociatedwithfunctionalcapacity.Oneofthe
possiblefactorsisthatthefemuristhebiggestboneofthe
lowerlimbsinhumansandthusaidsinlocomotion,posture
andbalance.Withtheboneinthisimportantregion
compro-mised,performingsomemotoractivitieslikewalkingbecame
moredifficult,therebyincreasingtheriskoffallsandfractures.
Bonemassisoneofthemaindeterminantsoffractures,but
onlyafewstudiessofarhaveanalyzedthisinoldermen.16–18
Thisisanalarmingsituation,giventhattheBrazilian
Osteo-porosisConsensusof2002(PintoNetoetal.19)indicatedthat
advancedageincreasestheriskofosteoporosisandfractures,
independentofsex.Thus,evaluationsonmenofadvanced
agebecomeessential.
Regarding evaluationof functional capacity, Kärkkäinen
et al.20conductedaneight-yearfollow-upstudy andfound
that therewas anassociation between functional
incapac-ity and increased risk offractures amongpostmenopausal
women. Although the incidence of fractures is greater in
Table3–Associationbetweenbonemassandfunctionalperformanceinmen.
Bonemass Performanceinthetests
Speed P Balance P Lower-limbstrength P
Worse Better Worse Better Worse Better
FemoralBMC(g)
Low 87.5% 12.5% 0.009 50% 50% 0.006 81.3% 18.8% 0.127
High 43.8% 56.3% 6.3% 93.8% 56.3% 43.8%
SpinalBMC(g)
Low 68.8% 31.3% 0.710 31.3% 68.8% 0.694 68.8% 31.3% 1.000
High 62.5% 37.5% 25% 75% 68.8% 31.3%
FemoralBMD(g/cm2)
Low 76.5% 23.5% 0.169 29.4% 70.6% 0.863 76.5% 23.5% 0.316
High 53.3% 46.7% 26.7% 73.3% 60% 40%
SpinalBMD(g/cm2)
Low 72.2% 27.8% 0.373 27.8% 72.2% 0.960 55.6% 44.4% 0.068
High 57.1% 42.9% 28.6% 71.4% 85.7% 14.3%
Table4–Associationbetweenbonemassandfunctionalperformanceinwomen.
Bonemass Performanceinthetests
Speed P Balance P Lower-limbstrength P
Worse Better Worse Better Worse Better
FemoralBMC(g)
Low 71% 29% 0.717 41.9% 58.1% 0.332 77.4% 22.6% 0.510
High 66.7% 33.3% 30% 70% 70% 30
SpinalBMC(g)
Low 77.4% 22.6% 0.142 35.5% 64.5% 0.923 74.2% 25.8 0.939
High 60% 40% 36.7% 63.3% 73.3% 26.7
FemoralBMD(g/cm2)
Low 68.4% 31.6% 0.925 39.5% 60.5% 0.476 76.3% 23.7% 0.561
High 69.6% 30.4% 30.4% 69.6% 69.6% 30.4%
SpinalBMD(g/cm2)
Low 66.7% 33.3% 0.759 36.4% 63.6% 0.807 72.7% 27.3% 0.907
High 70.4% 29.6% 33.3% 66.7% 74.1% 25.9%
BMC:bonemineralcontent;BMD:bonemineraldensity.
women,therelativeriskandtheconsequencessubsequent tothefracturearemoresevereinmen.21,22
InthestudyconductedbySakaietal.,23itwasfoundthat
performanceinthebalancetestonasinglefootwasassociated
withBMDamongJapanesewomenaged30–82years.Similar
resultswerealsofoundbyTaaffeetal.,24who,inastudyon
elderlypeopleofbothsexes,observedthattheirperformance
intestsonsittingdownonandgettingupfromchairsandon
balancingononefootwasonlyrelatedtofemoralneckBMD
andtrochantericBMD,respectively.Inourstudy,inthefemale
group,therewasnoassociationbetweenbonemassand
per-formance intestson sitting downon and gettingup from
chairsandonbalance.Thisresultmayindicatethatforelderly
womeninthisagegroup,othercomponentsofbody
composi-tion,suchasfat,aremoreassociatedwithfunctionalcapacity
(Rechetal.25),giventhatwomenpresentgreaterquantitiesof
bodyfat,whichgeneratesamechanicaloverloadonthebones
andmaycontributetowardsmaintainingBMD.26
Theusualwalkingspeedwasassociatedwithfemoralneck
BMDinWhite womenaged57–88, inastudy byBrownbill
etal.,27andwithforearmBMDinpostmenopausalJapanese
womeninalongitudinalstudybyKwonetal.28Lindseyetal.29
foundanassociationbetweenwalkingspeedandhip,spinal,
forearmandtotalBMDinagroupofwomenofmeanage68
years.Inthepresentstudy,noassociationwasfoundbetween
bone mass and performance inthe test on usual walking
speed,amongtheveryelderlyoldwomen.
In studies such as that of Kärkkäinen et al.,30 it was
observedthat women withfemoralneck osteoporosis
pre-sented diminished functional capacity. In our study, no
association was observed between bone mass and
perfor-manceinany ofthe functional tests, inthe femalegroup.
Thisevidencemaysignify thatforelderly womenoverthe
ageof80years,bonemassmayhavelessinfluenceon
func-tionalcapacitythanforwomenoflowermeanage.Thiswas
observedbyMilleretal.31inastudyonmen,andtheresults
revealedthattherelationshipbetweenmusclestrengthand
aerobiccapacitywasstrongeramongmiddle-agedmenthan
amongoldmen.
Inthe presentstudy,thefunctional capacityofthe very
elderly oldmenwas associatedwiththe bonemassofthe
femur,butnotwiththebonemassofthespine.Whenthe
per-formanceofthemalegroupineachofthefunctionaltestswas
analyzed,thebonemassofthefemurwasfoundtobe
asso-ciatedwiththewalkingspeedandbalancetests.Kärkkäinen
etal.30showedthisrelationshipbetweenthebalancetestand
thefemoralandspinalbonemassinpostmenopausalwomen.
InthestudyconductedbyMilleretal.,31theBMCofsomebody
regionssuchasthespine,pelvisandlegswascorrelatedwith
lower-limbstrengthamongmiddle-agedmen,buttherewas
nocorrelationbetweenthesevariablesamongelderlymen.In
ourstudy,therewasnoassociationbetweentotalfemurand
lumbarspinebonemassandperformanceinthelower-limb
strengthtestamongtheveryelderlyoldmen.
AccordingtoCawthonetal.,32thedecreaseinbonemass
among men over the age of 85 years istwice as great as
among 65-year-old men. This finding explains our results,
sincesevere lossofbonemass(BMD andBMC)also
inten-sifies thediminution offunctionalcapacity. Another factor
thatreinforcesourfindingsisthatseverebonelossand
occur-rencesofosteoporosisarerelatedtohormonelevels.Whereas
women’s estrogenlossesbegin aroundthe ageof50years,
men’stestosteronepersistsatfunctionallevelsuntilthe
sev-enthdecadeoflife.33
Theprevalenceofosteoporosisandtheincidenceof
osteo-porotic fractures are less frequentinmenthan inwomen.
Thisis becauseBMDand bonesizeare greater, and
there-forebonesarestrongerinmenthaninwomen,34asobserved
inoursample.However,increasingnumbersofmenare
pre-sentingosteoporosis,alongwiththecomplicationscausedby
thisdisease(falls,fracturesandfunctionalincapacity).
One of the limitations of our study was the absence
of other physical tests, such as tests on manual grip
strength, flexibility and coordination, in order to analyze
functional capacity. However, it is emphasized that there
is still a scarcity of studies aimed towards investigating
thesecharacteristicsamongelderlypeopleovertheageof80
Conclusion
Thus,thefemoralbonemassofveryelderlyoldmenwas
asso-ciatedwithfunctionalcapacity.Preventivemeasures,suchas
physicalactivitypracticethroughoutlifetargetingbonemass
preservation,shouldbeencouraged.Itshouldalsobe
empha-sizedthatassessmentofbonemineralmassamongelderly
peopleneedstobedoneconstantlywithadvancingage,since
thiswouldbeameansofworkingtowardspreventionoffalls,
whichhavehighprevalenceamongtheelderly.Althoughthere
wasnorelationshipamongfemales,limitationssuchasthe
absenceofothertestsandlackofassessmentofdietary
pro-cedures,suchastheuseofcalciumsupplementsamongsome
elderlywomen, may have contributed towardsthe present
findings.
Conflicts
of
Interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
Theauthors thank the National Councilfor Scientific and
TechnologicalDevelopment(CNPq)forfinancialsupportfor
thisstudy.
r
e
f
e
r
e
n
c
e
s
1. PedrinelliA,Garcez-LemeLE,NobreRS.Oefeitodaatividade físicanoaparelholocomotordoidoso.RevBrasOrtop. 2009;44(2):96–101.
2. SouzaMPG.Diagnósticoetratamentodaosteoporose.Rev BrasOrtop.2010;45(3):220–9.
3. MellströmD,JohnellO,LjunggrenO,ErikssonAL,Lorentzon M,MallminH,etal.Freetestosteroneisanindependent predictorofBMDandprevalentfracturesinelderlymen: MrOSSweden.JBoneMinerRes.2006;21(4):529–35.
4. ZhuK,DevineA,LewisJR,DhaliwalSS,PrinceRL.“Timedup andgo”testandbonemineraldensitymeasurementfor fractureprediction.ArchInternMed.2011;171(18):1655–61.
5. BuffaR,FlorisGU,PutzuPF,MariniE.Bodycomposition variationsinageing.CollAntropol.2011;35(1):259–65.
6. Guadalupe-GrauA,FuentesT,GuerraB,CalbetJAL.Exercise andbonemassinadults.SportsMed.2009;39(6):439–68.
7. BandeiraF,CarvalhoEF.Prevalênciadeosteoporoseefraturas vertebraisemmulheresnapós-menopausaatendidasem servic¸osdereferência.RevBrasEpidemiol.2007;10(1):86–98.
8. MacielACC,GuerraRO.Prevalênciaefatoresassociadosao déficitdeequilíbrioemidosos.RBrasCiMov.2005;13(1):37–44.
9. IBGE(InstitutoBrasileirodeGeografiaeEstatística).Censo
DemográficoeContagemdaPopulac¸ão:Populac¸ãoResidente
porSexo,Situac¸ãoeGruposdeIdade;2010.Availableat:
www.sidra.ibge.gov.br
10.IBGE(InstitutoBrasileirodeGeografiaeEstatística).Censo
DemográficoeContagemdaPopulac¸ão:Populac¸ãoResidente
porSexo,Situac¸ãoeGruposdeIdade;2000.Availableat:
www.sidra.ibge.gov.br
11.LebrãoML,LaurentiR.Saúde,bem-estareenvelhecimento:o estudoSabenoMunicípiodeSãoPaulo.RevBrasEpidemiol. 2005;8(2):127–41.
12.GuptaR,Al-SaeedO,AziziehF,AlbusairiA,GuptaP, MohammedA.Evaluationofbonemineraldensityin postmenopausalwomeninKuwait.JClinDensitom. 2011;15(2):211–6.
13.ReginsterJY,BurletN.Osteoporosis:astillincreasing prevalence.Bone.2006;382Suppl1:S4–9.
14.WuXP,HouYL,ZhangH,ShanPF,ZhaoQ,CaoXZ,etal. EstablishmentofBMDreferencedatabasesforthediagnosis andevaluationofosteoporosisincentralsouthernChinese men.JBoneMinerMetab.2008;26(6):586–94.
15.ButtrosDAB,Nahas-NetoJ,NahasEAP,CangussuLM,Barral ABCR,KawakamiMS,etal.Fatoresderiscoparaosteoporose emmulheresnapós-menopausadosudestebrasileiro.Rev BrasGinecolObstet.2011;33(6):295–302.
16.SzulcP,DelmasPD.Bonelossinelderlymen:increased endostealbonelossandstableperiostealapposition.The prospectiveMinosstudy.OsteoporosInt.2007;18(4):303–495.
17.CauleyJA,FullmanRL,StoneKL,ZmudaJM,BauerDC, Barrett-ConnorE.Factorsassociatedwiththelumbarspine andproximalfemurbonemineraldensityinoldermen. OsteoporosInt.2005;16(12):1525–37.
18.FrostM,WraaeK,AbrahamsenB,HøibergM,HagenC, AndersenM,etal.Osteoporosisandvertebralfracturesin menaged60–74years.AgeAgeing.2012;41(2):171–7.
19.PintoNetoAM,SoaresA,UrbanetzAA,SouzaACA,Ferrari AEM,AmaralB.Consensobrasileirodeosteoporose.RevBras Reumatol.2002;42(6),343:54.
20.KärkkäinenM,RikkonenT,KrögerH,SirolaJ,TuppurainenM, SalovaaraK,etal.Associationbetweenfunctionalcapacity testsandfractures:aneight-yearprospective
population-basedcohortstudy.OsteoporosInt. 2008;19(8):1203–10.
21.CenterJR,BliucD,NguyenTV,EismanJA.Riskofsubsequent fractureafterlow-traumafractureinmenandwomen.JAm MedAssoc.2007;297(4):387–94.
22.DiMonacoM,CastiglioniC,ValleroF,DiMonacoR,TapperoR. Menrecoverabilitytofunctionlessthanwomendo:an observationalstudyof1094subjectsafterhipfracture.AmJ PhysMedRehabil.2012;91(4):309–15.
23.SakaiA,TobaN,TakedaM,SuzukiM,AbeY,AoyagiK,etal. Associationofunipedalstandingtimeandbonemineral densityincommunity-dwellingJapanesewomen.Osteoporos Int.2009;20(5):731–6.
24.TaaffeDR,SimonsickEM,VisserM,VolpatoS,NivittMC, CauleyJA,etal.Lowerextremityphysicalperformanceand hipbonemineraldensityinelderlyblackandwhitemenand women:cross-sectionalassociationsintheHealthABCStudy. JGerontolSerA:BiolSciMedSci.2003;58(10):M934–42.
25.RechCR,CruzJL,AraújoED,KalinowskiFG,DellagranaRA. Associac¸ãoentrecapacidadefuncionaleexcessodepesoem mulheresidosas.Motricidade.2010;6(2):47–53.
26.NascimentoTB,GlanerMF,PacciniMK.Influênciada composic¸ãocorporaledaidadesobreadensidadeósseaem relac¸ãoaosníveisdeatividadefísica.ArqBrasEndocrinol Metab.2009;53(4):440–5.
27.BrownbillRA,LindseyC,Crncevic-OrlicZ,IlichJZ.Dualhip bonemineraldensityinpostmenopausalwomen:geometry andeffectofphysicalactivity.CalcifTissueInt.
2003;73(3):217–24.
28.KwonJ,SuzukiT,YoshidaH,KimH,YoshidaY,IwasaH,etal. Associationbetweenchangeinbonemineraldensityand declineinusualwalkingspeedinelderly
community-dwellingJapanesewomenduring2yearsof follow-up.JAmGeriatrSoc.2007;55(2):240–4.
29.LindseyC,BrownbillRA,BohannonRA,llichJZ.Associationof physicalperformancemeasuredwithbonemineraldensityin postmenopausalwomen.ArchPhysMedRehabil.
30.KärkkäinenM,RikkonenT,KrögerH,SirolaJ,TuppurainenM, SalovaaraK,etal.Physicaltestsforpatientselectionforbone mineraldensitymeasurementsinpostmenopausalwomen. Bone.2009;44(4):660–5.
31.MillerLE,PiersonLM,PiersonME,KiebzakGM,RampWK, HerbertWG,etal.Ageinfluencesanthropometricand fitness-relatedpredictorsofbonemineralinmen.Aging Male.2009;12(2/3):47–53.
32.CawthonPM,EwingSK,McCullochCE,EnsrudKE,CauleyJA, CummingsSR,etal.LossofhipBMDinoldermen:the
osteoporoticfracturesinmen(MrOS)study.JBoneMinerRes. 2009;24(10):1728–35.
33.OliveiraLG,GuimarãesMLR.Osteoporosenohomem.Rev BrasOrtop.2010;45(5):392–6.