UNIVERSIDADE DE LISBOA
Faculdade de Medicina de Lisboa
Padrões de tratamento e outcomes em doentes com
cancro da mama T1 N0
Time trends of treatment and outcomes in women with
T1 node negative breast cancer
Inês Maria Vaz Duarte Luis
Orientadores: Prof. Doutor Luís António Marques da Costa
Profª.Doutora Nancy
Uan-Tsin
Lin
Tese especialmente elaborada para obtenção do grau de
Doutor em Medicina (Oncologia)
UNIVERSIDADE DE LISBOA
Faculdade de Medicina de Lisboa
Padrões de tratamento e outcomes em doentes com
cancro da mama T1 N0
Time trends of treatment and outcomes in women with
T1 node negative breast cancer
Inês Maria Vaz Duarte Luis
Orientadores: Prof. Doutor Luís António Marques da Costa
Profª.Doutora Nancy
Uan-Tsin
Lin
Tese especialmente elaborada para obtenção do grau de Doutor em
Medicina (Oncologia)
Júri:
Presidente: Doutor José Luis Bliebernicht Ducla Soares, Professor Catedrático e em regime de tenure da Faculdade de Medicina da Universidade de Lisboa.
Vogais: Doutora Nancy Uan-Tsin Lin, Assistant Professor of Medicine da Harvard Medical
School, Estados Unidos da América (co-Orientadora);
Doutor Robert Eduard Coleman, Professor of Medical Oncology da University of Sheffield; Doutor José Luís Passos Coelho, Professor Associado Convidado da Faculdade de Ciências Médicas da Universidade Nova de Lisboa;
Doutor José Manuel Domingos Pereira Miguel, Professor Catedrático Jubilado da Faculdade de Medicina da Universidade de Lisboa;
Doutor Rui Manuel Martins Victorino, Professor Catedrático da Faculdade de Medicina da Universidade de Lisboa;
Doutor José Luis Bliebernicht Ducla Soares, Professor Catedrático da Faculdade de Medicina da Universidade de Lisboa.
Instituições Financiadoras e Âmbito: Fundação para a Ciência e
Tecnologia - HMSP-ICS/0004/2011, Desenvolvimento de Carreira
A impressão desta tese foi aprovada pelo Conselho
Científico da Faculdade de Medicina de Lisboa em
Reunião de 20 de Junho de 2017.
3
ACKNOWLEDGEMENTS
“Eu sou eu e minha circunstância.”
José Ortega y Gasset
This work is the result of an outstanding mentorship and environment. I
would like to acknowledge the support of:
- My outstanding mentors, Luis Costa and Nancy U Lin
- My 'other' mentors, Eric Winer, Ann Partridge, Rachel Freedman,
Harold Burstein, Michael Hassett, Rob Coleman, Rui MM
Victorino, Luis Silva Carvalho, Isabel Rocha, Paulo Cortes
- All my co-investigators and colleagues, particularly, Nancy
Keating, Melissa Hughes, Rebecca Ottensen, Anne O'nneil, Otto
Metzger, Joyce Lii, Arlindo Ferreira, Antonio Di Meglio, Liz Frank
- Breast Oncology Center of the Dana Farber Cancer Institute
- Serviço de Oncologia do Hospital de Santa Maria
- Grupo de estudos de cancro da mama with the support of the
Cancer Registry of Southern Portugal (Registo Oncológico
Regional do Sul, [ROR-Sul])
- My PhD advisor committee
- Harvard Medical School Portugal program
- My friends
- My family, particularly my parents, grandmother, brother and
husband
5 TABLE OF CONTENTS ACKNOWLEDGEMENTS 3 1. SUMMARY 7 1.1 English summary 7 1.2 Portuguese summary 9
1.3 Portuguese extended summary 11
1.4 Publication list 15
1.5 Abbreviation list 17
2. INTRODUCTION 19
3. OBJECTIVES 31
4. MATERIAL AND METHODS 33
5. RESULTS 37
6. LONG-TERM OUTCOMES OF PATIENTS WITH SMALL NODE-NEGATIVE
INVASIVE BREAST CANCER 38
7. THERAPY TRENDS AMONG PATIENTS WITH SMALL NODE-NEGATIVE
INVASIVE BREAST CANCER 62
7.1. Variation in type of adjuvant chemotherapy received among patients with
stage I breast cancer: A multi-institutional study 63
7.2. Variation in type of adjuvant chemotherapy received among patients with stage I breast cancer: a multi-institutional Portuguese cohort study 88 7.3. Trends in the use of mastectomy in women with small node negative
breast cancer treated at US academic centers. 104
8. PATIENTS AND PROVIDERS PREFERENCES REGARDING THERAPY
6
9. DISCUSSION 145
10. FUNDING 151
7 1. SUMMARY
1.1. English Summary
Treatment decisions in Stage I breast cancer patients are challenging. To better inform these decisions, we used quantitative research methods to 1) study survival outcomes among patients with the smallest Stage I breast cancers (tumours with less
than 1 cm [T1a, b N0]), 2) examine treatment time trends among patients with Stage I
breast cancers, and 3) interrogate patients regarding the minimum survival benefit needed in order to accept adjuvant chemotherapy.
Using an US contemporary cohort of ~4.000 patients, we found that, there are women with T1a,b tumors who have an excellent prognosis without chemotherapy, but size and tumor subtype may identify patients in whom the rate of recurrence justifies considering chemotherapy. Expanding the analyses to all stage I breast cancer tumors (~10.000 patients), we also found out that, particularly for subtypes such as human epidermal growth factor 2 (HER2) + and hormone receptor (HR)-HER2- breast cancers, there was an increase of use of chemotherapy over the last decade, and when treated there was an increase in use of intensive chemotherapy with substantial institutional and costs variations. In this same cohort, aggressive surgical strategies were in rise, with an increasing proportion of women with unilateral cancer treated with bilateral mastectomy. In contrast, in a Portuguese cohort of ~500 patients, mostly less-intensive associations of chemotherapy were used, also with substantial institutional variations. Finally, among ~500 patients who received contemporary adjuvant chemotherapy in a randomized controlled trial, we found substantial variation in preferences regarding benefit worth undergoing chemotherapy (57% of patients would
consider 6 months of chemotherapy for 2 months of benefit, whereas there was a small minority [2%] of patients that would say no to 6 months of chemotherapy for 24 months of benefit). Differences between patient and physician choices were also apparent.
This study identifies subgroups of Stage I breast cancer patients to whom we can safely avoid chemotherapy and subgroups of patients to whom chemotherapy can be considered. It also highlights that in an area, which treatments may be questionable, there is substantial institutional and regional variability calling into questioning the challenges around treatment options and highlighting that these patients represent an optimal group to evaluate less toxic adjuvant regimens to maintain efficacy while
8
minimizing short- and long-term risks. Finally, it shows that eliciting preferences regarding risks and benefits of adjuvant chemotherapy is critical.
9 1.2. Portuguese Summary
As decisões de tratamento de doentes com cancro da mama, estádio I, são geralmente complexas.
Neste estudo, foram usados métodos quantitativos para: 1) avaliar a sobrevivência de doentes com tumores estádio I com menos de 1 cm (T1a, b N0); 2) analisar tendências temporais de tratamento destes doentes; 3) inquirir doentes e médicos sobre preferências relativamente ao uso de quimioterapia (qual a vantagem
de sobrevivência necessária para aceitar receber ou prescrever quimioterapia durante 6 meses ?).
Usando uma coorte contemporânea americana de cerca de 4000 doentes, identificamos mulheres com tumores T1a, b, N0 com um excelente prognóstico sem quimioterapia (doentes com tumores com recetores hormonais [RH] +), e, por outro lado, verificamos que tamanho e que subtipo de tumor podem ser usados para seleccionar doentes em que o uso de quimioterapia deve ser considerado (doentes
com tumores >0.5 cm, RH-).Adicionalmente, a análise de cerca de 10.000 doentes
com tumores da mama, estádio I, demonstrou um aumento do uso de quimioterapia, e particularmente do uso de quimioterapia intensiva (em especial para subtipos, como tumores com fator de crescimento epidérmico humano 2 (HER2) + e tumores HR-HER2-) com substanciais variações institucionais e de custos associados. Nesta coorte, uma proporção crescente de doentes optou por cirurgias agressivas, como mastectomia bilateral. Em contraste, numa coorte portuguesa de cerca de 500 doentes, o tipo de quimioterapia utilizada para este grupo de doentes é tipicamente menos intensiva, contudo com variações institucionais substanciais. Finalmente, numa coorte de cerca 500 doentes, que receberam quimioterapia adjuvante intensiva, observou-se uma variação substancial nas preferências em relação ao benefício necessário para se considerar quimioterapia (57% dos doentes consideraria 6 meses
de quimioterapia por 2 meses de benefício, mas existe uma minoria, 2%, que não o faria por um benefício de 24 meses). Paralelamente, foram claras as diferenças entre
as escolhas dos doentes e as dos médicos.
Globalmente, este estudo identificou subgrupos de doentes com cancro da mama, estádio I, para os quais podemos evitar, com segurança, quimioterapia, e subgrupos de doentes em que se poderá considerar quimioterapia. Paralelamente,
10
sublinhou significativa variabilidade de prática institucional e regional, no tratamento de doentes com cancro da mama, estádio I.
Finalmente, este estudo demonstra que a obtenção das preferências dos doentes, relativamente ao uso de quimioterapia adjuvante, tendo em consideração potenciais riscos/benefícios, é crítica, uma vez que existe importante variabilidade associada.
Esta área é, por conseguinte, ideal para realizarmos estudos adjuvantes com regimes menos tóxicos, que permitam manter eficácia de tratamento, minimizando os riscos a curto e a longo prazo.
1.2.1. Palavras-chave: Cancro de mama, estádio I, sobrevivência, tratamento
11 1.3. Portuguese extended summary
Atualmente, nos Estados Unidos da américa (EUA) e na Europa, quase um milhão de doentes/ano são diagnosticados com cancro da mama, estádio I-III. Os paradigmas de tratamento de cancro de mama precoce evoluíram dramaticamente na última década. O uso rotineiro de terapia sistémica adjuvante (quimioterapia e
terapia-alvo, hormonoterapia ou terapêutica anti-HER2) levou a reduções substanciais no
risco de recidiva e morte por cancro de mama. No entanto, essas estratégias podem estar associadas a toxicidade aguda e a longo prazo, o que, em particular, para subgrupos de doentes com bom prognóstico inicial, como doentes de mama em estádio I e sobretudo para doentes com tumores T1abN0, pode tornar as decisões de tratamento complexas.
Neste estudo, foram usados métodos quantitativos para: 1) avaliar a sobrevivência de doentes com tumores estádio I com menos de 1 cm (T1a, b N0)
(subprojeto 1); 2) analisar tendências temporais de tratamento destes doentes com
cancro da mama, estádio I (subprojeto 2); 3) inquirir doentes e médicos sobre preferências relativamente ao uso de quimioterapia (qual a vantagem de
sobrevivência necessária para aceitar receber ou prescrever quimioterapia durante 6 meses?) (subprojeto 3).
Três bases de dados foram utilizadas para este estudo. Duas bases de dados referentes a registos tumorais e uma base de dados de um ensaio clínico: 1) base de dados de cancro da mama do National comphreensive cancer network (NCCN)
(subprojeto 1 e 2); 2) base de dados do registo oncológico regional do sul-Portugal
(ROR-Sul) (subprojeto 2); 3) Base de dados do ensaio do grupo Eastern Cooperative
Oncology Group (ECOG) 5103 focalizada em questões centradas em componentes
de tomada de decisão / qualidade de vida (subprojeto 3).
Para todas as análises, foi utilizada estatística descritiva para caracterizar a população em estudo. Testes de tendência de Cochran-Armitage foram usados para testar tendências de tratamento ao longo do tempo. Estimativas de sobrevivência a 5 anos foram calculadas entre subgrupos, usando estimativas de Kaplan Meier. Quando apropriado, modelos de regressão multivariada foram usados para examinar associações. Todos os p-valores apresentados consideram testes bilaterais de significância estatística de 0,05. As análises estatísticas foram realizadas utilizando ou SAS (SAS Institute Inc) ou Stata (StataCorp LP, College Station, TX).
12
Subprojeto 1. Realizamos um estudo prospectivo de coorte, utilizando a base de dados do NCCN e incluindo 4.113 mulheres com cancros da mama T1a, bN0M0 tratados entre 2000 e 2009. Os tumores foram agrupados por tamanho (T1a, T1b), subtipo biológico (definido pelo status de recetor hormonais [RH] e status do factor de crescimento epidérmico 2 (HER2)] e uso de quimioterapia +/- trastuzumab. O tempo médio de follow up foi de 5,5 anos. 8% dos pacientes com RH+ HER2-tumores foram tratados com quimioterapia. 52% das pessoas com tumores da mama, HER2 + e RH-HER2-, receberam quimioterapia, com um aumento substancial na última década. Globalmente a recidiva a distancia aos cinco anos não excedeu 10% em nenhum subgrupo. A DRFS (sobrevivência livre de recidiva a distancia) aos 5 anos para doentes não tratados com quimioterapia com tumores T1a variou de 93% a 98% (n = 49-972) e para doentes com tumores T1b de 90% a 96% (n = 17-2005); os doentes com doença RH+HER2- apresentaram as melhores estimativas e DRFS, os doentes com RH-HER2-tumores tiveram as mais baixas estimativas de sobrevivência. Neste estudo de coorte observacional não-randomizado, a DRFS de 5 anos para pacientes tratados com tumores T1a foi de 100% para todos os subgrupos (n = 12-33) e com tumores T1b variou de 94% a 96% (n = 88- 241).
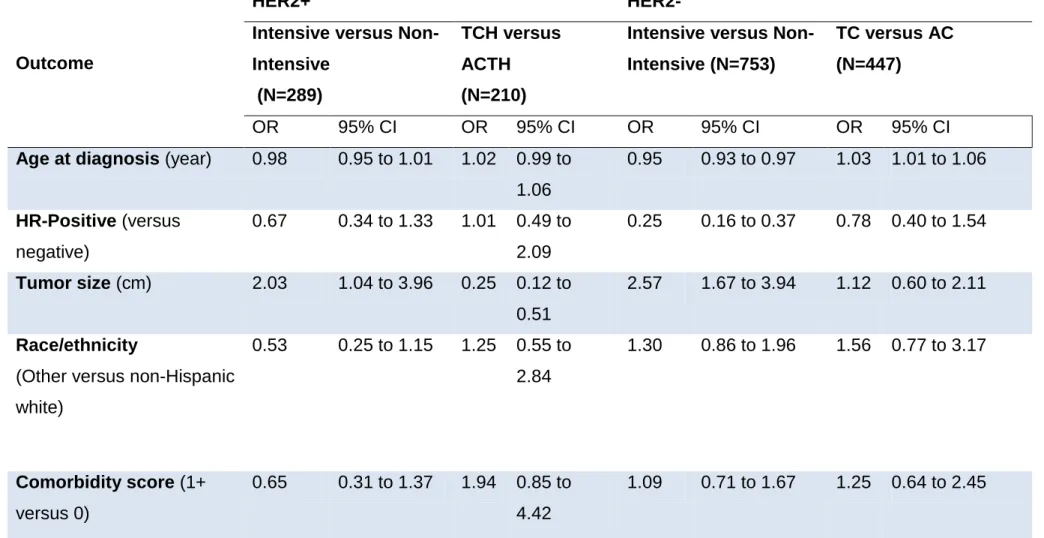
Subprojeto 2. Primeiro, realizamos um estudo prospectivo de coorte utilizando a base de dados do NCCN e incluindo mulheres com cancros da mama, estádio I, tratadas entre 2000 e 2009. Numa coorte de 8907 doentes, 33% receberam quimioterapia adjuvante. Entre doentes com doença HER2+, registou-se um aumento no uso de quimioterapia intensiva na última década, de 31% entre 2000 e 2005 para 63% entre 2008 e 009 (incluindo um aumento no uso da associação de docetaxel, carboplatina e trastuzumab). Entre doentes com doença HER2-, registou-se um aumento de 15% entre 2000 e 2005 para 41% entre 2008 e 2009. Entre os doentes tratados com regimes não intensivos, observou-se um aumento no uso da associação de docetaxel e ciclofosfamida, com uma diminuição no uso da combinação de doxorrubicina e ciclofosfamida. A escolha do regime variou significativamente de acordo com a instituição. Os principais fatores que influenciaram a variação de custos incluíram a incorporação de terapias biológicas (por exemplo, trastuzumab) e fatores de crescimento. Numa coorte semelhante de 10.249 doentes, 23% foram submetidos a mastectomia como cirurgia inicial. Não se registou diminuição no uso da mastectomia como cirurgia inicial, no entanto verificou-se variação institucional
13
significativa, com taxas de mastectomia inicial variando de 14 a 30% (odds ratio ajustado: 0,42-1,38). Dos doentes que receberam mastectomia inicial, 22% fizeram mastectomia bilateral, com aumento ao longo do tempo (2000: 13% vs. 2009: 30%) e substancial variação institucional (11-34%). As mulheres tratadas com mastectomia inicial tiveram tempos medianos mais longos, desde o diagnóstico até a cirurgia definitiva completa (6 vs. 4 semanas) assim como ao início da quimioterapia adjuvante (12 vs. 11 semanas). Para complementar esta análise com dados Portugueses, realizamos um estudo retrospectivo de coorte utilizando a base do ROR-Sul. Dos 595 doentes elegíveis, 22,4% foram tratados com quimioterapia, 33,9% com idade <55 anos versus 12,7% com idades> 65 anos (p <0,001). 13.0% dos doentes com tumores RH+HER2-, 52,7% dos doentes com tumores HER2+ e 66,0% dos pacientes com tumores RH- HER2- receberam quimioterapia (p <0,001). Além disso, encontramos variabilidade interinstitucional com o uso de quimioterapia, variando de 0,0% a 43,4% (p <0,001). 85% dos doentes tratados com quimioterapia receberam regimes menos intensivos baseados em antraciclinas, como a doxorrubicina e a ciclofosfamida, enquanto regimes com docetaxel e ciclofosfamida foram utilizados apenas em 1,5% dos casos.
Subprojeto 3. Realizamos um estudo transversal utilizando a base de dados do ensaio clínico E5103 focalizada em questões centradas em componentes de tomada de decisão/qualidade de vida. Este ensaio é um estudo de fase 3 que randomizou doentes com cancro da mama para receber doxorrubicina, ciclofosfamida e paclitaxel com bevacizumab ou com placebo. Dos 519 doentes elegíveis para esta análise, 87,8% participaram neste estudo. Em paralelo, 175 médicos foram também inquiridos para esta análise. Observou-se uma variação substancial nas preferências em relação ao benefício necessário para se considerar quimioterapia (57% dos doentes consideraria 6 meses de quimioterapia por 2 meses de benefício, mas existe uma minoria 2% que não o faria por um benefício de 24 meses). Paralelamente, foram claras as diferenças entre as escolhas dos doentes e as dos médicos, com a classe médica a ter menor probabilidade de propor quimioterapia para benefícios modestos. Globalmente, este estudo identificou subgrupos de doentes com cancro da mama, estádio I, para os quais podemos evitar, com segurança, quimioterapia e subgrupos de doentes em que se poderá considerar quimioterapia. Paralelamente, sublinhou importante variabilidade de prática institucional e regional no tratamento de
14
doentes com cancro da mama estádio I. Finalmente, este estudo demonstra que a obtenção das preferências dos doentes relativamente ao uso de quimioterapia adjuvante, tendo em consideração potenciais riscos/benefícios, é crítica, uma vez que existe importante variabilidade associada. Esta área é, assim, ideal para realizarmos estudos adjuvantes com regimes menos tóxicos, que permitam manter eficácia de tratamento, minimizando os riscos a curto e a longo prazo.
15 1.4 PUBLICATION LIST GENERATED BY THIS THESIS
1.4.1 Main original publications generated
1. Vaz-Luis I, Ottesen RA, Hughes ME, Mamet R, Burstein HJ, Edge SB,
Gonzalez-Angulo AM, Moy B, Rugo HS, Theriault RL, Weeks JC, Winer EP, Lin NU.Outcomes by tumor subtype and treatment pattern in women with small, node-negative breast cancer: a multi-institutional study. J Clin Oncol. 2014 Jul 10;32(20):2142-50. PMID: 24888816
2. Vaz-Luis I, Hughes ME, Cronin AM, Rugo HS, Edge SB, Moy B, Theriault RL,
Hassett MJ, Winer EP, Lin NU. Variation in type of adjuvant chemotherapy received among patients with stage I breast cancer: A multi-institutional study. Cancer. 2015 Jun 15;121(12):1937-48. doi: 10.1002/cncr.29310. Epub 2015 Mar 10. PMID: 25757412
3. Vaz-Luis I, Hughes ME, Cronin A, Rugo HS, Edge SB, Moy B, Theriault RL,
Hassett MJ, Winer EP, Lin NU.Trends in the use of mastectomy in women with small node-negative breast cancer treated at US academic centers. Breast Cancer Res Treat. 2016 Feb;155(3):569-78. doi: 10.1007/s10549-016-3707-1. Epub 2016 Feb 11. PMID: 26868124
4. R Ferreira A, Palha A, Correia L, Filipe P, Rodrigues V, Costa L, Miranda A,
André R, Fernandes J, Gouveia J, Passos-Coelho JL, Moreira A, Brito M, Ribeiro J, Metzger-Filho O, U Lin N, Vaz-Luís I.Variation in type of adjuvant chemotherapy received among patients with stage I breast cancer: A multi-institutional Portuguese cohort study. Breast. 2016 Oct;29:68-73. PMID: 27468923
5. Vaz-Luis I, O'Neill A, Sepucha K, Miller KD, Baker E, Dang CT, Northfelt DW,
Winer EP, Sledge GW, Schneider B, Partridge AH. Survival benefit needed to undergo chemotherapy: Patient and physician preferences. Cancer. 2017 Mar 21. PMID: 28323331
1.4.2. Associated publications generated:
1. Vaz-Luis I, Burstein HJ.Optimizing Adjuvant Chemotherapy and Surgery for Early- and Late-Stage Breast Cancer. JAMA Oncol. 2016 Nov 1;2(11):1399-1400. doi: 10.1001/jamaoncol.2016.36 PMID: 27631400
16
1;33(1):125. doi: 10.1200/JCO.2014.58.9655. PMID: 2540321418.
3. Barroso-Sousa R, Paes FR, Vaz-Luis I, Batista RB, Costa RB, Losk K, Camuso K, Metzger-Filho O, Hughes ME, Bunnell CA, Golshan M, Winer EP, Lin NU. Variation in the use of granulocyte-colony stimulating factor for dose dense paclitaxel: A single institution retrospective study. Breast. 2016 Dec;30:136-140. PMID: 27721193
4. Luis I, Burstein HJ.With better adjuvant therapy, does breast cancer stage still matter? Vaz- BMJ. 2015 Oct 6;351:h5273. doi: 10.1136/bmj.h5273.PMID: 26443566
17 1.5 ABBREVIATION LIST
1.5.1 Portuguese abbreviation list
EUA: Estados Unidos da América RH: receptores hormonais
ROR-Sul: registo oncológico regional do sul-portugal RH: receptores hormonais
1.5.2. English abbreviation list
A: doxorrubicin
AC: doxorubicin-cyclophosphamide ACTH: AC-paclitaxel-trastuzumab AE: adverse events
AJCC: american joint committee on cancer APT: adjuvant paclitaxel-trastuzumab ASP: average sales price
BCSS: breast cancer specific survival BCS: breast conserving surgery BMI: body mass index
BSA: body surface area C: cyclophosphamide
CAF: cyclophosphamide-doxorubicin-5-fluorouracil CI: confidence interval
CMF:cyclophosphamide, methotrexate and 5-fluorouracil CT: chemotherapy
D:docetaxel
DRFS: distant relapse free survival EC: epirubicin-cyclophosphamide
ECOG: eastern cooperative oncology group EIC: extensive intraductal component, EIO: european institute of oncology ER: estrogen receptor
18
FAC: cyclophosphamide, doxorubicin, 5-fluorouracil FEC: cyclophosphamide, epirubicin, 5-fluorouracil; HER2: human epidermal growth factor 2
HR: hormone receptor
IDFS: invasive disease free survival IRB: institutional review board
KPNC: kaiser permanente northern california LVI: lymphovascular invasion
M:methotrexate MAST: mastectomy
MDACC: MD Anderson cancer center MF: methotrexate-5-fluorouracil; MRI: magnetic resonance imaging NA: not applicable.
NCCN: national comprehensive cancer network No: N
NOS: not otherwise specificied NST: no special type
OR: odds ratio OS: overall survival QOL: quality of life
ROR-Sul: cancer registry of southern Portugal RS: recurrence score
SEER: surveillance, epidemiology, and end results T:docetaxel
TAC: docetaxel-doxorubicin- cyclophosphamide TC: docetaxel-cyclophosphamide
TCH: docetaxel-carboplatin-trastuzumab TNBC: triple negative breast cancer negative Y: yes
19 2. INTRODUCTION
2.1. Breast cancer overview
2.1.1. Overall breast cancer incidence and mortality
Breast cancer is the most common cancer in women worldwide, with the woman´s risk of developing breast cancer during her lifetime being estimated at 12% (~ 1 in 8 women who reach 85).(1) In 2012, the incidence of breast cancer worldwide adjusted to age was reported to be 43.3 per 100,000 women.(1) In the same year, 464,000 new cases were reported in Europe, representing 28.8% of cancer cases among female and 13.5% of all cancer cases of both sexes(2) and in Portugal, around 6.000 new breast cancer cases/year were diagnosed. (2)
In 2012, 522,000 breast cancer deaths worldwide have been reported;(1) in Europe, breast cancer is the principal cause of cancer death among women, with 131,000 deaths registered in 2012 (3) and in Portugal, the breast cancer mortality rate is estimated of 18 per 100,000 individuals. (3)
2.1.2. Breast cancer, a shift towards Stage I breast cancer and treatment advances
Over the past 50 years, substantial reductions in breast cancer mortality were documented throughout the western world.(4-6) Such improvements were not a result of a single scientific breakthrough; rather they were coincidental with advances in early detection and better treatment options, and related to the implementation of better medical care processes, enhancements in medical education and increased population and patient education.(7) In the late 1970’s, guidelines started to emerge recommending the use of screening mammography for women over the age of 40; this was followed by the wide implementation of national and regional screening programs across most developed countries. (8) Soon after, adjuvant therapy, with endocrine and chemotherapy, was found to reduce the risk of recurrence and death due to breast cancer leading to its increased use. (7) More recently, we witnessed the development and adoption of targeted human epidermal growth factor receptor 2 (HER2) therapies.(9, 10) Advances in local management of breast cancer, moving away from mutilating surgeries, such as the radical mastectomy, to breast conserving surgery in
20
combination with radiation therapy, were also implemented. (11) In addition, we all observed establishment of international guidelines, algorithms and consensus conferences, with emphasis on multidisciplinary care and high and better population and patient breast cancer awareness and education, all of each promote better care. Therefore, regarding Stage I breast cancer over the past 50 years we observed: 1) A stage shift due with screening mammography. Currently, almost one million patients/year are diagnosed with Stage I-III breast cancer in the United States (US) and in Europe, (12) and in the past two decades, the incidence of Stage I breast cancers has increased dramatically, and these tumors now comprise nearly half of Stage I-III breast cancer diagnoses.(13) Between 1990 and 1998, there has been almost a 15% increase in the rate of T1 (0-2cm) tumors within the Surveillance, Epidemiology, and End Results (SEER) Program (from 143,500 to 163,500/1000.000). (14)
2) Better treatment that led to breast cancer mortality at 5 years for Stage I breast cancers around 10%.(15-17)
In making adjuvant therapy decisions in breast cancer, the potential absolute benefits of treatment must be weighed against the treatment-related risks. Although the risk of death during breast cancer adjuvant therapy is extremely small, it is not absent.(18, 19) The absolute benefit of treatment is a function of the baseline prognosis and impact of therapy on risk of recurrence.
In a setting where we have a substantial amount of small breast cancers is essentially to understand their heterogeneity, prognosis, treatment patterns
and patients preferences regarding therapy options.
2.1.3. Breast cancer heterogeneity and Stage I disease
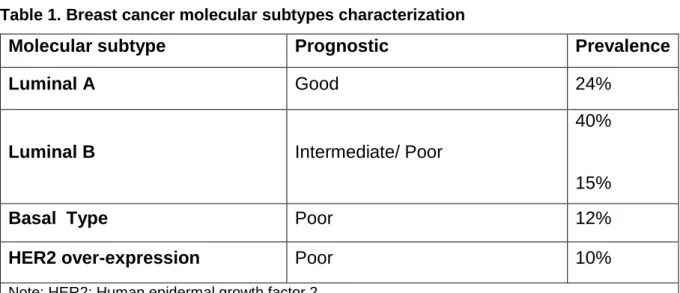
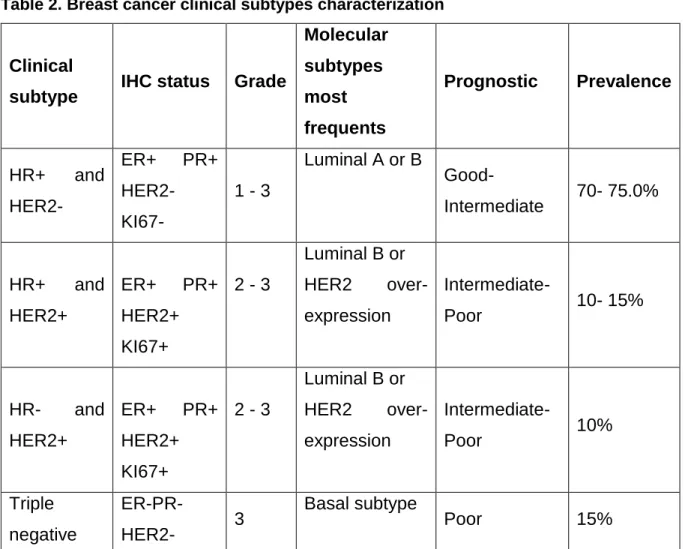
Breast cancer is a heterogeneous disease, with substantial genotypic and phenotypic diversity. Four molecular subtypes, defined by profiling techniques, such as cDNA microarrays, were characterized in breast cancer in the early’s 2000 – Luminal A, Luminal B, HER2 type and Basal type, with specific prognostic factors and different therapeutic targets. Table 1 summarizes the original breast tumour molecular subtypes. (20) In clinical practice, four main breast cancer subtypes associated with these molecular subtypes drive treatment decisions: HR+ and HER2-, HR+ and HER2+, HR- HER2+ and triple-negative breast disease (HR- and HER2-). (Table 2)
21
Therefore, in clinical practice among breast cancer prognosis and treatment strategies are defined by clinical subtypes.
2.1.4. Outcomes of patients with small node-negative invasive breast cancer (Stage 1 disease)
As previously mentioned, unselected for subtype, breast cancer patients with Stage I tumors have an excellent prognosis.(15-17) Nevertheless, these metrics are highly impacted by clinical subtype.
The problem, is that until recently there were no good data regarding outcomes and treatment patterns of Stage 1, particularly of tumors under 1cm (T1a, b node negative tumors). This is partially due to the fact of these breast cancers have been largely excluded from adjuvant therapy trials and the information of subtype in registries was not available until recently. This is a particular problem in the setting of chemotherapy decisions given its toxicity.
Traditionally, there has been a general consensus that it is reasonable to omit chemotherapy in patients with baseline distant recurrence risk less than 10% and particularly for tumors under 1cm it is not clear if this is the case.
There remains persistent uncertainty about the prognosis of some patients with Stage I HR+HER2-, particularly if T1a,bN0 tumours. Both national and international treatment guidelines remain ambiguous about the management of such patients.(21) For example, the 2013 NCCN guidelines indicate that for patients with T1b/c N0 HR+HER2- tumors, a 21-gene recurrence score can be requested, with chemotherapy to be considered in patients with an intermediate or high score. Even in the absence of recurrence score data, the National comprehensive cancer network (NCCN) guidelines recommend consideration of chemotherapy.(21)
The situation is somewhat different in patients who have either HR- or HER2+ tumors (particularly those with HR-HER2- disease).In these settings the risk of recurrence appears higher and the absolute benefit of treatment may be greater. Given the variability in prognostic estimates and the potential benefits for therapy among these subsets, there has been widespread debate on the appropriate threshold for adjuvant chemotherapy+/-trastuzumab recommendations, with a steady evolution of the guidelines: Prior to 2003, NCCN guidelines recommended adjuvant chemotherapy for tumors >1 cm in size, and/or with nodal involvement. In 2003, guidelines
22
recommended adjuvant chemotherapy ”to be considered” for patients with moderate to poorly differentiated T1bN0 breast cancers, regardless of subtype; in 2007 this was adjusted to encompass HER2+ tumors and since 2008 this recommendation also covered HR- cancers. Finally, since 2010 the guidelines have recommended consideration of chemotherapy and trastuzumab for patients with HER2+ T1bN0 tumors.(21)
Few retrospective series analysed the outcomes of T1a, bN0M0 HER2+ disease. One analyzed the risk of recurrence among 98 patients with T1a,b N0M0 HER2+ disease who did not received chemotherapy or trastuzumab, and reported a 5-year recurrence free survival of 77%. (57) In contrast, another series of 150 patients, the 5-year disease free survival was 92%in patients with HR+HER2+ tumors, and 91% in patients with HR-HER2+ tumors.(22) Approximately one-third of patients in this series received adjuvant chemotherapy, most of them with HR- disease.(22) Finally, in another series of 237 patients (116 T1a and 121 T1b), the 5-year recurrence free survival was 96% for patients with T1a tumors and 91% for patients with T1b tumors. 25% of those patients received adjuvant chemotherapy and 9% adjuvant trastuzumab.(23)
Better prognostic estimates are needed for these tumours.
2.1.5. Therapy trends small node-negative invasive breast (Stage 1)
There is few data regarding treatment patterns among these patients.
2.1.5.1. Chemotherapy trends
Among patients with Stage 1 breast cancer it is unclear chemotherapy use and when the chemotherapy decision is taken it is unclear the type of regimens that are used.
The chemotherapy landscape for early breast cancer has changed over the last 20years.(24, 25) In the early 2000’s, several trials showed that multi-agent chemotherapy regimens such as anthracycline-taxane combinations were more effective in the treatment of early breast cancer when compared with anthracycline-based regimens such as doxorubicin- cyclophosphamide (AC), though they lengthened the duration and expense of therapy and were associated with more toxicity .(25, 26) In approximately 2006, taxane-based regimens without anthracyclines also demonstrated efficacy, though also had other potential toxicities, such as febrile
23
neutropenia and neurotoxicity.(25-27) At the same time, multiple phase III trials suggested that adding trastuzumab to chemotherapy was associated with a 40% risk reduction in recurrence when compared to chemotherapy alone.(28) Stage I patients have generally been excluded or underrepresented in such trials and therefore, there is uncertainty regarding the preferred chemotherapy to be used.(25, 29)
2.1.5.1 Surgical trends
More than three decades ago, several randomized controlled clinical trials showed similar survival outcomes for breast conserving surgery (BCS) in association with adjuvant radiotherapy versus mastectomy. This led to the 1990 National Institute of Health recommendation of BCS as the preferable surgical treatment for unilateral breast cancer.(30-35) Recent population-based data suggest there may be better outcomes with BCS and that bilateral mastectomy is unlikely to be associated with any significant survival advantage over BCS with adjuvant radiotherapy for the treatment of unilateral breast cancer.(36) Nevertheless, in the last decade, rates of mastectomy and bilateral mastectomy remained stable and may be rising. (37-49)
Data for initial surgical options focused on women who meet medical criteria BCS are limited. One such group is women with Stage I disease who, by definition, have tumors under 2 cm in size and are most often amenable to BCS. A recent study from the National Cancer Data Base which included over 1,000,000 patients with Stage I-III breast cancer suggested an increase in the rate of mastectomy and particularly of bilateral mastectomy from 2003-2011, with steeper increases in women with node negative disease.(49) In contrast, analyses using the Surveillance, Epidemiology, and End Results Medicare (SEER) dataset looking at definitive surgery trends among breast cancer patients, found declines in mastectomy rates for Stage I disease in recent years.(50, 51)
2.1.6. Treatment preferences
There is an increasing recognition that patients’ preferences should play an important role in medical treatment decisions. This is particularly important, when the benefit of chemotherapy maybe uncertaint.
Very few data exist regarding patients’ preferences for modern adjuvant chemotherapy.(52) Older studies suggested that most patients with early breast cancer were willing to receive 6 months of adjuvant cyclophosphamide, methotrexate and
5-24
fluorouracil (CMF) chemotherapy for modest survival benefits (most women would have accepted 3-6 months extension of life), even when acknowledging potential adverse effects. (53-55) In addition, it has been suggested that physicians frequently do not necessary share patients’ views, sometimes being less likely to recommend chemotherapy for a small chance of benefit.(55, 56)
2.2. Outcomes research overview
In medical oncology, traditionally we relied on clinical trial data to make treatment decisions. Nevertheless, there are populations of patients that are underrepresented on clinical trials and for whom alternative evidence should be used. In recent years, data from observational studies have become an increasingly important source of evidence in these areas, becoming a complementary analytic technique. This was possible due to 1) construction of well-defined datasets 2)
Strategic use of data sources and application of statistical techniques the impact of treatment interventions in non-experimental settings and examine practice patterns.
Rules to build datasets are now defined and can be checked to ensure good quality of data. International consortiums were built to safeguard this process.
The ideal dataset should follow standard methodological quality criteria for observational studies.(57) It should 1) have an independent steering committee involved in the definition of the study methodology, study implementation, and analytic strategy, 2) be registered in public repositories, 3) have implemented data quality procedures, 4) have few missing data for measures of interest; 4) have a well-defined patient population, with well described inclusion and exclusion criteria reflecting the target patient population; 5) the outcomes of interest and variables should be well characterized, 6) the length of observations should have sufficient duration to capture outcomes of interest and 7) the sample size should calculated based on defined hypotheses.(57)
The design and analytic plan of observational studies can prevent, reduce, and assess bias, confounding, and chance, so that a causal unbiased association between exposure and outcome is estimated.
Three main study designs are used in observational studies: cohort (follow up), case–control, and cross sectional designs (Figure 1). Case-control and cohort studies offer specific advantages by measuring disease occurrence and its association with an
25
exposure by offering a temporal dimension (i.e. prospective or retrospective study design). Cross-sectional studies, also known as prevalence studies, examine the data on disease and exposure at one particular time point. Because the temporal relationship between disease occurrence and exposure cannot be established, cross-sectional studies cannot assess the cause and effect relationship.
A variety of analytic techniques can be used. In some cases, especially when data are collected on detailed clinical risk factors, these differences can be controlled using standard statistical methods, including multivariable modelling. In other cases, when unmeasured patients characteristics affect both the decision to treat and the outcome, these differences can be overcome using techniques such as propensity score risk adjustment, and propensity-based matching, which control for overt bias, and instrumental variable analysis. (58, 59)
2.3. Summary
Currently, almost one million patients/year are diagnosed with Stage I-III breast cancer in the United States (US) and in Europe. (12) Treatment paradigms of early breast cancer had dramatically evolved over the last decade. The routine use of adjuvant systemic therapy (chemotherapy and targeted therapy) led to substantial reductions in the risk of breast cancer recurrence and death, nevertheless, these strategies can be associated with substantial acute and long-term toxicity, which, particularly among subgroups of patients with upfront good prognosis, such as patients with Stage I breast cancers, can make treatment decisions challenging.(12)
In the past two decades, the incidence of Stage I breast cancers has increased dramatically, and these tumors now comprise nearly half of Stage I-III breast cancer diagnoses. (13, 14, 60)
Unselected for subtype, breast cancer patients with Stage 1 and T1a and T1b (≤ 1 cm) node negative tumors have an excellent prognosis, with breast cancer specific survival at 10 years exceeding, 90% and 95%.(15-17) However, data on outcomes for these patients are highly variable across different biologic subtypes. For example, the reported recurrence free survival of patients with Human Epidermal Growth Factor Receptor 2 (HER2) positive T1a, b node-negative breast cancer has ranged from 77%- 99%, based on institutional retrospective series with sample sizes ranging from 98 to 237 patients, and with variable treatment. (22, 23, 61)
26
Compounding this problem, patients with T1 node-negative breast cancer have been largely excluded from adjuvant chemotherapy trials, and this has led to widespread variation in the use of chemotherapy without a clear understanding of the true risk-benefit ratio of using chemotherapy and the best regimen to use. There are no studies that had examined comprehensively treatment trends among this population.
Finally, there is no recent data on patients’ preferences regarding treatment choices. The available data dates almost twenty years and focus on old treatment regimens, with some studies suggesting that most patients with early breast cancer were willing to receive 6 months of adjuvant cyclophosphamide, methotrexate and 5-fluorouracil (CMF) for modest survival benefits (most women would have accepted 3-6 months extension of life) even acknowledging potential adverse effects. (53-55, 3-62) In addition, it was also suggested that physicians frequently do not share patient preferences, being less likely to accept chemotherapy for a small chance of benefit. (55, 56)
In this work, we used observational quantitative research methods to inform treatment decisions among patients with small node negative disease,
particularly we examined 1) outcomes, 2) trends in treatment patterns and 3) patients preferences among patients with Stage I breast cancer.
27
2.4. Tables and Figures
Table 1. Breast cancer molecular subtypes characterization
Molecular subtype Prognostic Prevalence
Luminal A Good 24%
Luminal B Intermediate/ Poor
40%
15%
Basal Type Poor 12%
HER2 over-expression Poor 10%
28
Table 2. Breast cancer clinical subtypes characterization
Clinical
subtype IHC status Grade
Molecular subtypes most frequents Prognostic Prevalence HR+ and HER2- ER+ PR+ HER2- KI67- 1 - 3 Luminal A or B Good- Intermediate 70- 75.0% HR+ and HER2+ ER+ PR+ HER2+ KI67+ 2 - 3 Luminal B or HER2 over-expression Intermediate- Poor 10- 15% HR- and HER2+ ER+ PR+ HER2+ KI67+ 2 - 3 Luminal B or HER2 over-expression Intermediate- Poor 10% Triple negative ER-PR- HER2- 3 Basal subtype Poor 15%
Note: Hormone receptor, HER2: Human epidermal growth factor 2, ER: estrogen receptor, PR: progesterone receptor
29
31 3. OBJECTIVES
There is substantial controversy on the prognosis and how to treat small node negative breast cancer. In this work, three work projects were performed using quantitative research methods to:
Aim 1) Determine long-term outcomes of patients with small node negative invasive breast cancer (T1a,bN0M0).
(Work project 1. This work project used the NCCN Breast cancer Outcomes Database and generated Manuscript 1 [Vaz-Luis et al, Journal of Clinical Oncology, 2014])
Aim 2) Evaluate therapy trends small node-negative invasive breast, particularly:
To characterize type chemotherapy (± trastuzumab) receipt over the last decade
To evaluate local therapy tendencies over the last decade
To evaluate predictors of treatment decisions
(Work project 2. This work used the NCCN Breast cancer Outcomes Database and the Cancer Registry of Southern Portugal [Registo Oncológico Regional do Sul, ROR-Sul and generated Manuscripts 2, 3, 4 [Vaz-Luis et al, Cancer, 2015, Vaz-Luis et al, Breast Cancer
Research and Treatment, 2016, Ferreira, Breast, 2016])
Aim 3) Evaluate patients and providers preferences regarding adjuvant therapy choices.
(Work project 3. This work project used Eastern Cooperative Oncology Group Protocol (E5103) Decision-Making/Quality of Life (QOL) component and generated Manuscript 5 [
33 4. MATERIALS AND METHODS
Three datasets were used for this study, two registry-based datasets and one clinical trial dataset, respectively:
NCCN Breast cancer Outcomes Database (Work project 1,2: Manuscript 1, 2,3)
Cancer Registry of Southern Portugal (ROR-Sul) (Work project 2: Manuscript
4)
E5103 Decision-Making/Quality of Life (QOL) component (Work project 3:
Manuscript 5)
In this section a brief description of the methods used in the setting of each dataset are described. Detailed description of the methodology used in each work project is described in the manuscripts presented.
4.1. NCCN Breast cancer Outcomes Database (Work project 1,2: Manuscript 1,2,3) 4.1.1. Study design and Data Source
This was a prospective cohort study using the NCCN Breast Cancer Outcomes Database. Patients were included in the database if they received all or some of their treatment at a reporting center; those with one-time consultations were not included. Eight centers contributed data to this analysis: City of Hope National Medical Center; University of Texas MD Anderson Cancer Center (MDACC); Fox Chase Cancer Center; Dana-Farber Cancer Institute; Roswell Park Cancer Institute; H. Lee Moffitt Cancer Center; University of Michigan Cancer Center; and Ohio State University. All centers adhered to the data collection procedures and definitions developed by the NCCN Breast Cancer Outcomes Database, subjected to rigorous quality assurance.(63)
Institutional review boards (IRBs) from participating centers approved data collection, transmission, and storage protocols. At centers where the IRB required signed informed consent for data collection, only patients who provided consent were included in the database; elsewhere, the IRB granted a waiver of signed informed consent.
34
4.1.2. Key Variables
The database contains tumor information on tumor size, nodal status, grade, lymphovascular invasion (LVI), HR and HER2 status, as abstracted from pathology reports. Data on race/ethnicity and comorbidity score (64, 65) came from patient surveys collected at initial presentation to the NCCN center. The following variables are abstracted by chart review: age at diagnosis, drug treatment, type and date of recurrence, vital status and cause of death. Vital status and cause of death are also confirmed using the Social Security Death Index and the National Death Index, current as of December 31, 2009. Invasive disease free survival (IDFS), distant relapse free survival (DRFS), BCSS and overall survival (OS) were defined as time in years from diagnosis to date of death or last known vital status or recurrence using the STEEP system.(66)
4.1.3. Statistical Analyses
Descriptive statistics were used to characterize the clinicopathological and treatment characteristics. The Cochran-Armitage trend test was used to test trends of receipt of therapy over time Estimates of 5-year survival were calculated among subgroups using Kaplan Meier estimates for OS, BCSS, IDFS, and DRFS. When appropriate, multivariate logistic regression models were used to examine associations. All p-values presented are two-sided tests of statistical significance at 0.05. All statistical analyses were performed using SAS 9.3 (SAS Institute Inc).
4.2. Cancer Registry of Southern Portugal [ROR-Sul]) (Work project 2: Manuscript 4)
As part of this study a Portuguese breast cancer working group was created. This work group recovered clinical and treatment data regarding breast cancer patients treated between 2006-2008 in four Portuguese centers: Instituto Português de Oncologia de Lisboa Francisco Gentil (a public referral cancer center), Centro Hospitalar de Lisboa Norte (a public hospital and an academic center), Hospitais CUF Lisboa (a private hospital) and Hospital da Luz (a private hospital). The Cancer Registry of Southern Portugal (ROR-Sul) platform was used to collect the data.
35 4.2.1. Study design and Data source
This was a retrospective cohort study. Patients were included if they received at least part of their treatment at one of the participating reporting centers. The ROR-Sul platform was used for this study. All centers adhered to the same data collection procedures and to the variables definitions previously developed by ROR-Sul. Data audits were performed to assure data quality. The audits focused on 10% of the cases and all variables had a higher than 95% concordance rate across all variables and all centers. IRBs from participating centers, the ROR-Sul direction and ROR-Sul review board approved the study protocol.
4.2.2. Key Variables
All the variables were abstracted from a combination of chart, pathology and pharmacy reports review. The dataset includes information about age at diagnosis, year of diagnosis tumor size, tumor subtype, histological type, tumor grade, and treatment type.
4.2.3. Statistical Analyses
Descriptive analyses were performed. Due to very small numbers in some subgroups, multivariate comparisons were not performed. In this dataset, statistical analyses were conducted using Stata - version 13.1 (StataCorp LP, College Station, TX).
4.3. E5103 Decision-Making/Quality of Life component (Work project 3: Manuscript 5)
4.3.1. Study design and Data source
Eastern Cooperative Oncology Group Protocol (E5103) was a phase III trial which randomized node positive or high risk node negative breast cancer patients to receive adjuvant chemotherapy (doxorubicin, cyclophosphamide and paclitaxel) with either placebo or bevacizumab. Telephone based surveys were administered to all patients enrolled on E5103 between 01/Jan/10 and 08/Jun/10, as part of a Decision-Making/QOL component of this study. IRBs approval for the clinical trial was received through participating sites for study participation, and written informed consent was obtained from participants prior to study enrolment.
36
At 18 months post enrolment, patients who participated on the Decision-Making/QOL component of E5103 responded to a series of chemotherapy preference questions. In addition, a corresponding physicians’ survey was also sent to doctors who enrolled patients.
4.3.2. Data collection
Patients: Patients’ interviews were completed on the telephone by centralized
staff. Patients were mailed a copy of the survey two weeks prior to the phone interview. Most patients filled it out before the interview and the interview served to collect answers. If not filled out ahead of time, survey questions were read. If patient didn't have a copy, questions were read. Patient could ask questions about survey questions at any point.
Physicians: Physicians were mailed a brief survey of their background and
practice and the preferences surveys. Physicians would mail back the surveys.
4.3.3. Key variables
Patients: The dataset contains information on the proportion of
patients/physicians willing to consider chemotherapy, age, race, marital status, education, HR status, grade, tumor size, node, surgery, toxicity experienced, treatment arm.
Physicians: For the physicians preferences analyses the covariates of interest
included age, gender, race, years in profession, years in current practice, practice size, practice setting, new patients per month, new breast cancer patients per month, patients on clinical trials per month.
4.3.4. Statistical Analyses
Descriptive statistics were used to summarize patients and physicians characteristics and trade-offs of survival benefit to consider 6 months of chemotherapy were examined. Multivariate logistic regression models adjusting for the covariates listed above to examine associations between willingness to consider chemotherapy and the features examined. All statistical analyses were conducted using SAS version 9.4 (SAS Institute, Cary, NC).
37 5. RESULTS
This study generated 5 original manuscripts that will be presented in separate sections.
Long-term outcomes of patients with small node-negative invasive breast cancer (Work project 1) generated manuscript 1:
‘Outcomes by tumor subtype and treatment pattern in women with small, node-negative breast cancer: A multi-institutional study’
Therapy trends among patients with small node-negative invasive breast cancer (Work project 2) generated manuscripts 2,3,4:
‘Variation in type of adjuvant chemotherapy received among patients with Stage I breast cancer: A multi-institutional study’
‘Trends in the use of mastectomy in women with small node negative breast cancer treated at US academic centers’
‘Variation in type of adjuvant chemotherapy received among patients with stage I breast cancer: a multi-institutional Portuguese cohort study’ Patients and providers preferences regarding adjuvant therapy choices cancer
(Work project 3) generated manuscript 5:
‘Survival Benefit Needed to Undergo Chemotherapy: Patient and Physician Preferences’
For all work projects Ines Vaz-Luis, led the design of the study, took on the driving of analyses, interacting with biostatisticians, performing data analysis, interpreting results and writing all the manuscripts that are presented in this study.
The tables and figures are numerated separately for each manuscript. The references for all manuscripts are presented in a separate section.
38
6. LONG-TERM OUTCOMES OF PATIENTS WITH SMALL NODE-NEGATIVE INVASIVE BREAST CANCER
The work project 1 generated Manuscript 1 that was published in the Journal of Clinical Oncology (Appendix 1 with facsimile). This first work provides information regarding the prognosis of patients with small node negative invasive breast cancer with or without adjuvant chemotherapy.
Ines Vaz-Luis, led the design of the study, took on the driving of analyses, interacting with biostatisticians and performing herself some data analysis, interpreting results and writing the manuscript that is presented here.
6.1. Outcomes by tumor subtype and treatment pattern in women with small, node-negative breast cancer: A multi-institutional study
6.1.1 Authors
Ines Vaz-Luis 1, 2, Rebecca A. Ottesen 3, Melissa E. Hughes 1, Rizvan Mamet 3, Harold J. Burstein 1, Stephen B. Edge4,5, Ana M. Gonzalez-Angulo 6, Beverly Moy 7,
Hope S. Rugo 8, Richard L. Theriault 6, Jane C. Weeks 1, Eric P. Winer 1, Nancy U. Lin 1
Author Affiliations: 1Dana-Farber Cancer Institute, Boston, MA; 2Instituto de
Medicina Molecular, Lisbon, Portugal; 3City of Hope, Duarte, CA; 4Roswell Park
Cancer Institute, Buffalo, NY; 5 Baptist Cancer Center, Memphis, TN; 6University of
Texas MD Anderson Cancer Center, Houston, TX; 7Massachusetts General Hospital,
Boston, MA;8University of California, San Francisco Helen Diller Family
Comprehensive Cancer Center, San Francisco, CA
6.1.2 Abstract
Purpose: Treatment decisions in T1a,bN0M0 breast cancer patients are
challenging. We studied the time trends in use of adjuvant chemotherapy and survival outcomes among these patients.
Patients and Methods: This was a prospective cohort study within the National
Comprehensive Cancer Network Database which included 4,113 women with T1a,bN0M0 breast cancer treated between 2000-2009. Tumors were grouped by size
39
(T1a, T1b), biologic subtype [defined by HR, HER2 status], and receipt of chemotherapy+/-trastuzumab.
Results: Median follow-up time was 5.5 years. 8% of patients with HR+HER2-
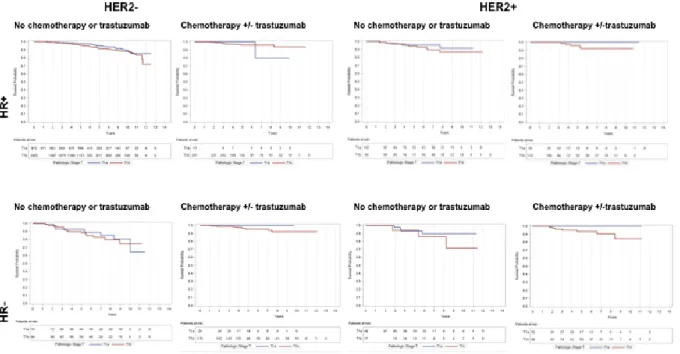
tumors were treated with chemotherapy. 52% of those with HER2+ and HR-HER2- breast cancers received chemotherapy, with an increase over the last decade. Survival outcomes diverged by subtype and size, but the 5-year distant-relapse-free-survival (DRFS) did not exceed 10% in any subgroup. The 5-year DRFS for patients untreated with chemotherapy with T1a tumors ranged from 93%-98% (n=49-972) and for patients with T1b tumors from 90%-96% (n=17-2005); patients with HR+HER2- disease had the best DRFS estimates and patients with HR-HER2- tumors had the lowest. In this observational, non-randomized cohort study, the 5-year DRFS for treated patients with T1a tumors was 100% for all subgroups (n=12-33) and with T1b tumors ranged from 94%-96% (n=88-241).
Conclusions: Women with T1a,b tumors have an excellent prognosis without
chemotherapy. Size and tumor subtype may identify patients in whom the rate of recurrence justifies consideration of chemotherapy. These patients represent an optimal group to evaluate less toxic adjuvant regimens to maintain efficacy while minimizing short- and long-term risks.
6.1.3 Introduction
Over the past two decades, the incidence of Stage I breast cancers has increased dramatically, and these tumors now comprise nearly half of Stage I-III diagnoses.(13) Between 1990 and 1998, there has been almost a 15% increase in the rate of T1 (0-2cm) tumors in the US as assessed by the Surveillance, Epidemiology, and End Results Program (from 143.5 to 163.5/100,000), (14) largely attributed to detection of non-palpable breast cancer associated with screening mammography.(13, 14, 60)
Breast cancer patients with T1a,b (≤1 cm) node-negative tumors generally have an excellent prognosis, with breast cancer specific survival (BCSS) at 10 years exceeding 95%. (15-17) However, outcomes for these patients may vary by biologic subtype.(22, 23, 61, 67-72) Compounding this problem, these patients have been excluded from adjuvant chemotherapy trials, which have resulted in uncertainty regarding the true risks and benefits of chemotherapy.
40
Since 1997, the NCCN Breast Cancer Outcomes Database collected detailed tumor and treatment data on a large cohort of women with newly diagnosed breast cancer presenting to many of its member institutions across the US.(73-75) In this work, we examined time trends of chemotherapy use in the last decade and outcomes of breast cancer patients with T1a,bN0M0 tumors by biologic subtype, size and treatment among women included in the NCCN database.
6.1.4 Methods
6.1.4.1.Study design and Data Source
This was a prospective cohort study performed in the NCCN Breast Cancer Outcomes Database. Patients were included in the database if they received all or some of their treatment at a reporting center; those with one-time consultations were not included. Eight centers contributed data to this analysis: City of Hope National Medical Center; University of Texas MDACC; Fox Chase Cancer Center; Dana-Farber Cancer Institute; Roswell Park Cancer Institute; H. Lee Moffitt Cancer Center; University of Michigan Cancer Center; and Ohio State University. All centers adhered to the data collection procedures and definitions developed by the NCCN Breast Cancer Outcomes Database, subjected to rigorous quality assurance.(63)
IRBs from participating centers approved data collection, transmission, and storage protocols. At centers where the IRB required signed informed consent for data collection, only patients who provided consent were included in the database; elsewhere, the IRB granted a waiver of signed informed consent. An analytic cohort of 4,113 patients with T1a,bN0 breast cancer was identified (Figure 1).
6.1.4.2 Key Variables
The database contains tumor information on tumor size, nodal status, grade, LVI, HR and HER2 status, as abstracted from pathology reports. HR is considered positive if the estrogen receptor (ER) and/or progesterone receptor are positive. For HER2 classification, the fluorescence in situ hybridization result was used, if available. If only immunohistochemistry was available, 3+, “high positive”, or “positive not
otherwise specified
(NOS)” were considered HER2+; while 2+, 1+, 0, or “negative” were considered HER2-negative; 1% (n=32) of the patients were “positive NOS”. Tumors were grouped by
41
biologic subtypes (HR+ HER2-, HR+HER2+, HR-HER2+, or HR-HER2-) and tumor size [T1a (≤ 0.5cm) or T1b (>0.5cm <1cm)]. Patients were classified as having received chemotherapy+/-trastuzumab or not. Six patients received trastuzumab alone. Tumor grade is categorized as high (according to histologic grade, or, if not available, by nuclear grade) or low-intermediate. Data on race/ethnicity and comorbidity score (64, 65) came from patient surveys collected at initial presentation to the NCCN center. The following variables are abstracted by chart review: age at diagnosis, drug treatment, type and date of recurrence, vital status and cause of death. Vital status and cause of death are also confirmed using the Social Security Death Index and the National Death Index, current as of December 31, 2009. IDFS, DRFS, BCSS and OS were defined as time in years from diagnosis to date of death or last known vital status or recurrence using the STEEP system (Table A1).(66)
6.1.4.3 Statistical Analyses
Descriptive statistics were used to characterize the clinicopathological and treatment characteristics. The percentage of patients who received chemotherapy+/-trastuzumab was calculated by subgroups. The Cochran-Armitage trend test was used to test the receipt of chemotherapy+/-trastuzumab over time. Estimates of 5-year survival were calculated among subgroups using Kaplan Meier estimates for OS, BCSS, IDFS, and DRFS. Beside stratification, no further adjustment for other clinicopathological features was performed due to the small sample size of some subgroups.
Sensitivity analyses were performed. First, we included patients who did not have follow-up at the NCCN institution in the first 365 days after diagnosis (n=589) (Table-A2 represents deaths/censuring among these patients). Second, we excluded the patients treated with trastuzumab only (n=6).Finally, for patients with HR+HER2- disease we also examined the impact of grade on outcomes.
All p-values presented are two-sided tests of statistical significance at 0.05. All statistical analyses were performed using SAS 9.3 (SAS Institute Inc).
42
6.5. Results
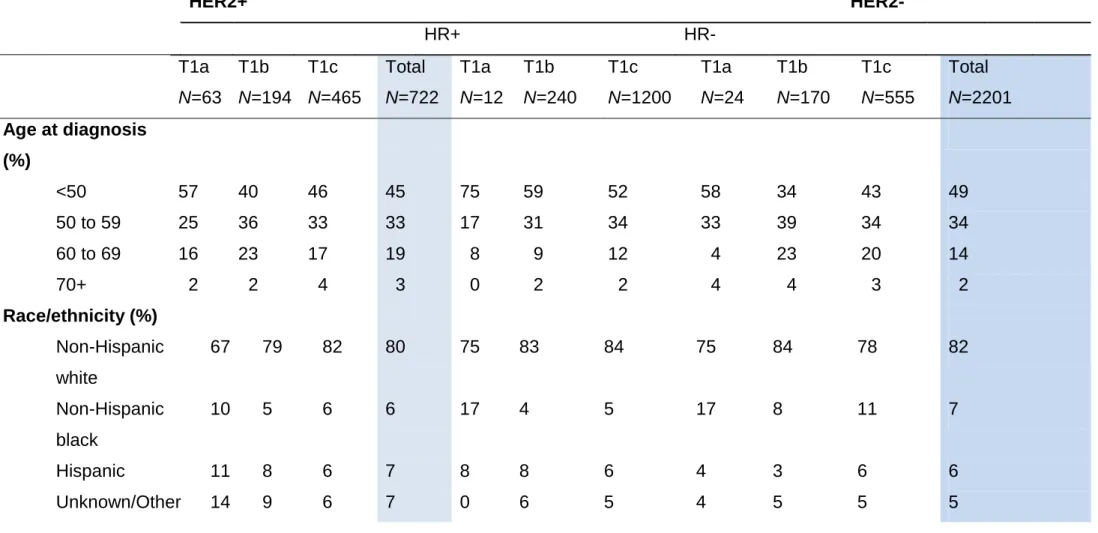
6.5.1. Characteristics of the study population
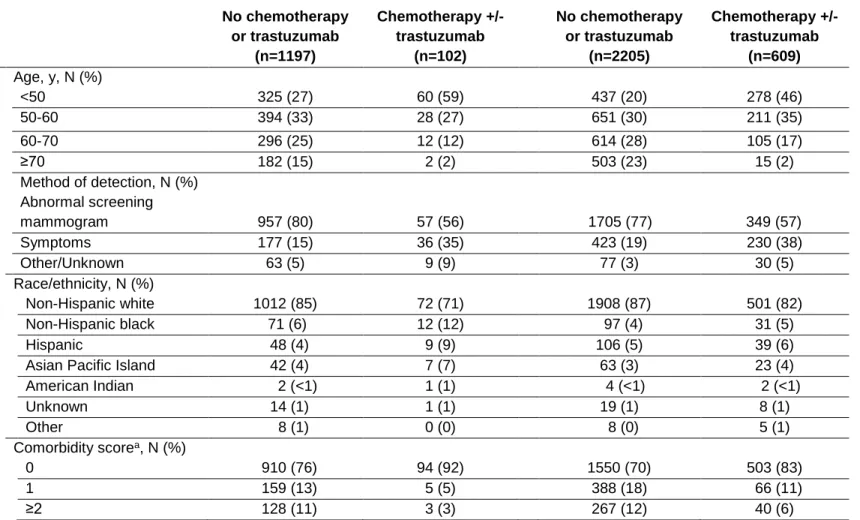
Median follow-up time was 5.5 years (1-13 years). Baseline clinicopathological characteristics differed by subgroups (Table-1). As expected, compared to patients who received chemotherapy+/-trastuzumab, patients untreated with chemotherapy or trastuzumab were older and had more comorbidities. Moreover, fewer patients treated without chemotherapy+/-trastuzumab presented with adverse prognostic features, such as HER2 expression, high grade and LVI.
19% of patients in the analytic cohort were deemed lost to follow-up (defined as >2-years without a contact at a NCCN center). Age and year of diagnosis differed by group (P<0.001).However, no other significant differences in patient or tumor characteristics were found between those lost to follow-up versus the others (data not shown).
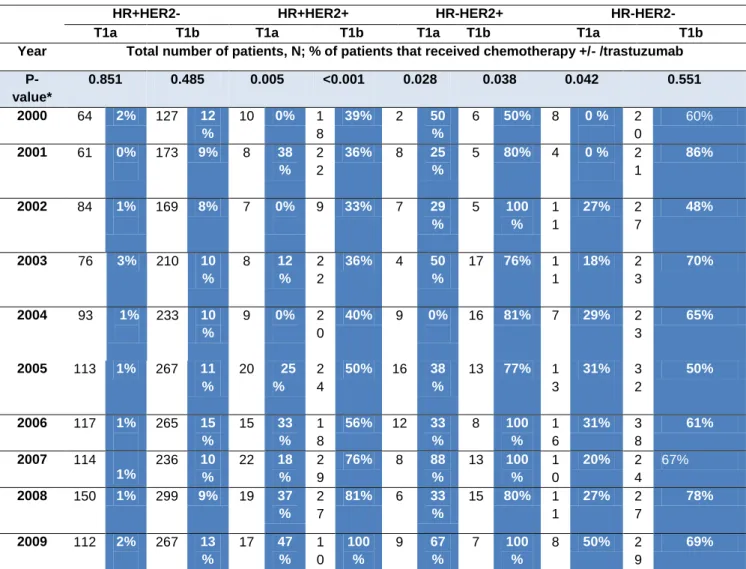
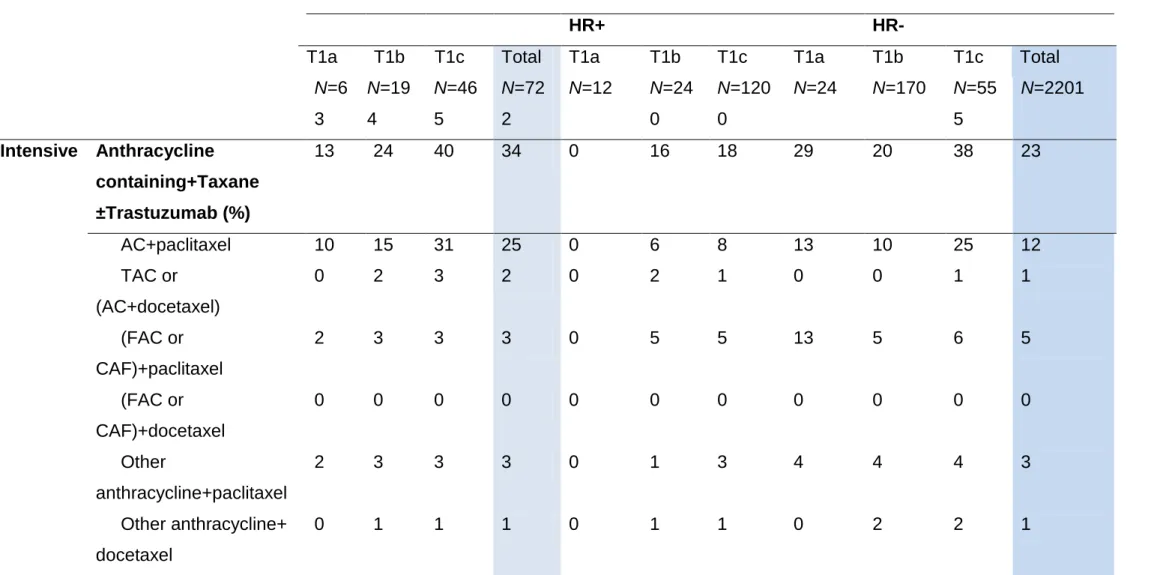
6.5.2. Treatment characteristics and time trend in the use of chemotherapy
There were striking differences in chemotherapy utilization between tumor subtypes (Table A3). Chemotherapy was rarely administered in patients with HR+HER2- tumors and their pattern of care was unchanged over the last decade. In contrast, a high proportion of patients with HER2+ and HR-HER2- tumors received adjuvant trastuzumab and there was an increase in chemotherapy+/-trastuzumab utilization among patients with HER2+ and in patients with T1a HR-HER2- tumors over the past decade (Table 2).
6.5.3. Survival outcomes
Table 3 lists the survival outcomes for patients treated and not treated with chemotherapy+/-trastuzumab by tumor subtype and size. In the overall cohort, the 5-year OS for patients not treated with chemotherapy+/-trastuzumab with T1a or T1b tumors exceeded 95%. The 5-year DRFS estimate was 97% for T1a and 95% for T1b tumors.
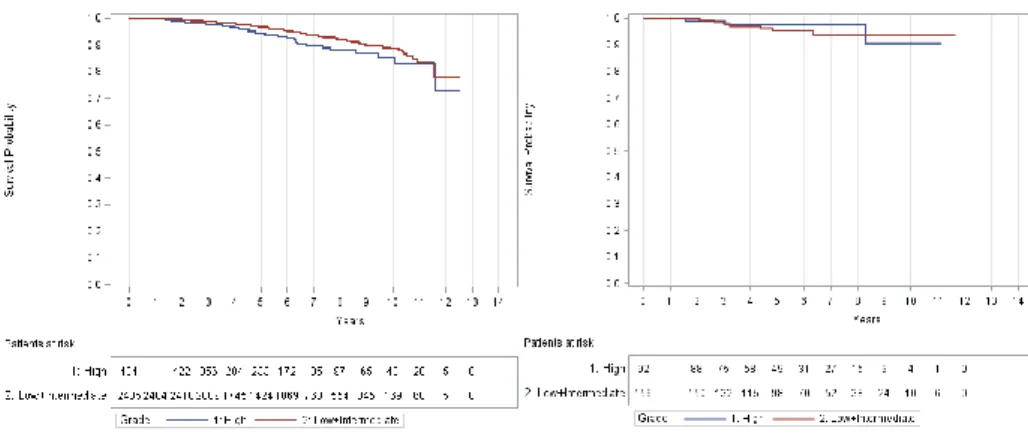
Among patients with HR+HER2- breast cancer, 5-year OS and BCSS exceeded 95% in both T1a and T1b and exceeded 90% for IDFS and DRFS irrespective of the receipt or non-receipt of chemotherapy. Among patients with HR+HER2-tumors those with high grade tumors not treated with chemotherapy experienced numerically lower
43
DRFS estimates (94%) compared to patients treated with chemotherapy (98%), though the absolute difference, even in this high-grade subset, was small (Table-A4, Figure-A1). For patients with HER2+ tumors, the 5-year OS and BCSS were similarly high and the point estimates for 5-year distant recurrence rate did not exceed 7%, albeit with very wide confidence intervals for the HR-HER2+ subset, given the small sample size (n=17). The 5-year DRFS for patients who did not receive chemotherapy or trastuzumab with T1bN0 tumors was 94% for both HR+HER2+ (95% CI=86, 99) and HR-HER2+ (95%CI=63, 99). The 5-year DRFS for patients with T1b tumors who received chemotherapy+/-trastuzumab was 96% (95% CI= 88-99) for HR+HER2+ and 94% (95% CI=85-97) for HR-HER2+. For patients with HR-HER2-tumors untreated with chemotherapy, the point estimate for 5-year DRFS was for T1a tumors 93% (95% CI= 84-97), and for T1b tumors 90% (95% CI= 81-95; however among one of the sensitivity analyses this point estimate for T1b tumors was 86%, Table-A5). The 5-year DRFS for treated HR-HER2- T1a tumors was 100% and for HR-HER2- T1b tumors was 96% (95% CI=90-98) (Figure-2). Additional results of sensitivity analyses were similar (data not shown).
6.1.6. Discussion
Over the last decade among patients with T1a,bN0M0 breast cancer treated at academic centers geographically distributed across the US there was an increase in chemotherapy usage for HER2+ and T1a HR-HER2- breast cancers. Across all subgroups, these patients experienced an excellent prognosis with the 5-year point estimate for distant relapse for patients untreated with chemotherapy with T1a tumors ranging from 2-7% and for patients with T1b tumors from 4-10%; patients with HR+HER2- tumors had the best prognosis and patients with HR-HER2- tumors had the lowest outcomes estimates. For treated patients with T1a tumors there were no distant recurrence events at 5 years and for T1b tumors the 5-year distant recurrence rate was 4% for patients with HR+ and HER2- tumors and 6% for patients with HR-HER2+ tumors. This observational, non-randomized cohort study, calls into question what treatment is justified and appropriate for these patients.
In making adjuvant chemotherapy decisions in breast cancer, the potential absolute benefits of treatment must be weighed against the treatment-related risks. Although the risk of death during breast cancer adjuvant chemotherapy is less than