Copyright © 2007 by Sociedade Brasileira de Pediatria
ORIGINAL
ARTICLE
Procalcitonin in children with sepsis and septic shock
José R. Fioretto,1 Fernanda de C. Borin,2 Rossano C. Bonatto,3
Sandra M. Q. Ricchetti,4 Cilmery S. Kurokawa,5 Marcos A. de Moraes,6
Mário F. Carpi,3 Carlos R. Padovani,7 Joelma G. Martin8
Abstract
Objectives:To study the behavior of procalcitonin and to verify whether it can be used to differentiate children with septic conditions.
Methods:Children were enrolled prospectively from among those aged 28 days to 14 years, admitted between January 2004 and December 2005 to the pediatric intensive care unit at Universidade Estadual Paulista UNESP with sepsis or septic shock. The children were classified as belonging to one of two groups: the sepsis group (SG; n = 47) and the septic shock group (SSG; n = 43). Procalcitonin was measured at admission (T0) and again 12 hours later (T12h), and the results classed as: < 0.5 ng/mL = sepsis unlikely;≥0.5 to < 2 = sepsis possible;≥2 to < 10 = systemic inflammation and≥10 = septic shock.
Results:At T0 there was a greater proportion of SSG patients than SG patients in the highest PCT class [SSG: 30 (69.7%) > SG: 14 (29.8%); p < 0.05]. The proportion of SSG patients in this highest PCT class was greater than in all other classes (≥10 = 69.7%;≥2 to < 10 = 18.6%;≥0.5 to < 2 = 11.6%; < 0.5 = 0.0%; p < 0.05). The behavior of procalcitonin at T12h was similar to at T0. The pediatric risk of mortality (PRISM) scores for the SSG patients in the highest procalcitonin class were more elevated than for children in the SG [SSG: 35.15 (40.5-28.7) vs. SG: 18.6 (21.4-10.2); p < 0.05].
Conclusions:Procalcitonin allows sepsis to be differentiated from septic shock, can be of aid when diagnosing septic conditions in children and may be related to severity.
J Pediatr (Rio J). 2007;83(4):323-328:Procalcitonin, sepsis, septic shock, children, intensive care.
1. Livre-docente, Departamento de Pediatria, Universidade Estadual Paulista (UNESP), Botucatu, SP, Brasil. Chefe, Unidade de Tratamento Intensivo Pediátrica, UNESP, Botucatu, SP, Brasil.
2. Acadêmica de Medicina, UNESP, Botucatu, SP, Brasil.
3. Doutor. Professor assistente, Departamento de Pediatria, UNESP, Botucatu, SP, Brasil. Médico diarista, Unidade de Tratamento Intensivo Pediátrica, UNESP, Botucatu, SP, Brasil.
4. Médica diarista, Unidade de Tratamento Intensivo Pediátrica, UNESP, Botucatu, SP, Brasil.
5. Doutora. Responsável, Centro de Pesquisa Clínica e Experimental, Departamento de Pediatria, UNESP, Botucatu, SP, Brasil. 6. Médico diarista, Unidade de Tratamento Intensivo Pediátrica, UNESP, Botucatu, SP, Brasil.
7. Professor titular, Departamento de Bioestatística, UNESP, Botucatu, SP, Brasil.
8. Mestre, UNESP, Botucatu, SP, Brasil. Médica, Pronto-Socorro de Pediatria, Hospital das Clínicas de Botucatu, Botucatu, SP, Brasil.
Financial support: Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP), grant no. 04/03776-0. Fernanda de C. Borin is the beneficiary of a Scientific Initiative bursary from FAPESP, grant number 2004/09783-9
Suggested citation:Fioretto JR, Borin FC, Bonatto RC, Ricchetti SM, Kurokawa CS, de Moraes MA, et al. Procalcitonin in children with sepsis and septic shock. J Pediatr (Rio J). 2007;83(4):323-328.
Manuscript received Nov 21 2006, accepted for publication Feb 28 2007.
doi 10.2223/JPED.1644
Introduction
Sepsis remains one of the greatest challenges in critical care medicine. Despite improvements in the understanding of its pathophysiology and despite new treatment options, the mortality rate continues to be elevated.1
Several consensus conferences have been held,2,3but the criteria for defining sepsis and related conditions are nevertheless still considered too sensitive and insufficiently specific, which can result in erroneous or delayed diagnoses, particularly among children. Furthermore, the clinical signs or most typical laboratory findings of sepsis occur late on, when multiple organ system failure (MOSF) has already occurred and mortality increased considerably, meaning that the effectiveness of new treatment strategies are directly related to the speed with which diagnosis is established.3,4
these problems with definitions and diagnosis are indications of the need to focus on biochemical mediators capable not only of distinguishing the inflammatory response to infection from other types of inflammation, but also of indicating the severity and prognosis of patients.
Procalcitonin (PCT), is a prohormone of calcitonin, normally produced by thyroid gland C-cells in response to hypercalcemia. Under normal conditions, very low concentrations of PCT in serum (< 0.1 ng/mL) are observed.5 More significantly, inflammatory processes induce extrathy-roid production of PCT, the levels of which increase after 3 to 4 hours, peaking at around 6 hours, with a plateau of up to 24 hours, and can remain elevated for up to 48 hours.6
the part that PCT plays as a mediator of sepsis has not yet been established. Some studies demonstrated that PCT may be useful for early diagnosis and as an indicator of severity in children with sepsis.7,8However, several other studies have reported the opposite results, questioning the value of PCT for diagnosis and prognosis in patients with sepsis and septic shock.9,10Furthermore, there is evidence that serum PCT levels increase in patients with Systemic Inflammatory Response Syndrome (SIRS) of noninfectious etiology.6
the conflicting results about the role of PCT, together with the scarcity of studies of children that have assessed this mediator, indicates that there is a need to better define its utility for the early diagnosis of sepsis in this group. Our hypothesis is that PCT is useful for both diagnosis and for assessing severity of children with septic conditions after the neonatal period.
The study objectives were: 1) to study the behavior of the serum PCT levels of children with clinical diagnoses of sepsis or septic shock and 2) to verify whether PCT was also an indicator of the severity of these patients, and of differentiating the children with diagnoses of sepsis from those with septic shock, after the neonatal period.
Methods
Patients, definitions and monitoring
This was a prospective observational study carried out between January 2004 and December 2005, enrolling children aged 28 days to 14 years, admitted to the pediatric intensive care unit (PICU) at the Hospital das Clínicas, Botucatu Medical Faculty, UNESP and diagnosed with sepsis or septic shock. Children were excluded if they had chronic systemic inflammatory diseases, degenerative neurological diseases, primary or acquired immunodeficiency diseases, were on corticoid therapy, nonsteroidal anti-inflammatories or antibiotics for more than 24 hours, had suffered traumas or burns or were in postoperative care. The study was approved by the Ethics and Research Committee at the Botucatu Medical Faculty, Universidade Estadual Paulista-UNESP. Written consent was obtained from parents or guardians before recruiting their children.
Sepsis and septic shock were defined according the criteria established by the Consensus Conference of 2001.3 Sepsis was defined as the presence of the signs and symptoms of SIRS associated with a documented or suspected infection. Diagnosis of SIRS was made based on the presence of two or more of the following criteria: 1) temperature (rectal, oral or central) > 38.5 ºC or < 35 ºC; 2) tachycardia (may be absent if there is hypothermia); 3) tachypnea; 4) white blood cell count high or low for age (and not secondary to chemotherapy) or immature neutrophils accounting for more than 10% of total count. In addition, at least one of the following had to be present: altered state of consciousness, hypoxemia, increase in serum lactate or wide pulses. Septic shock was defined as the presence of tachycardia (may be absent if there is hypothermia) with signs of reduced perfusion, including weak peripheral pulses compared with central ones, altered state of consciousness or reduced urinary output. Hypotension is a late sign and indicates uncompensated shock.
Patients were assigned to one of two study groups on admission: sepsis group (SG) or the septic shock group (SSG). The diagnoses of sepsis or septic shock was agreed for each patient by a consensus of all researchers at weekly meetings. Since there is a possibility that a patient with sepsis will progress to septic shock, the initial diagnosis was considered the definitive criterion for assigning study group.
pre-established criteria.12Pediatric risk of mortality (PRISM) scores were calculated for all patients at admission.13
Laboratory tests
The first blood sample was taken on admission, and labeled T0. Once 12 hours had passed, another sample was taken and labeled T12h. The results of the biochemical analyses were not made available to the treating doctors. The blood sample taken for PCT assay was 5 mL at T0 and 3 mL on subsequent occasions, from central venous catheter. After collection, the blood was immediately refrigerated and, no more than 8 hours later, the material was centrifuged so that the mediators could be assayed in plasma.
The PCT assay was a semi-quantitative method using immunochromatography (BRAHMS PCT®-Q - Diagnostica GmbH, Hennigsdorf, Germany), the so-called rapid test (30 minutes). The PCT concentration classes and their possible interpretations were as follows:61) < 0.5 ng/mL = sepsis unlikely, there may be a localized infection; 2)≥0.5 ng/mL to < 2 ng/mL = sepsis possible; 3)≥2 ng/mL to < 10 ng/mL = bacterial infection complicated by systemic inflammation; and 4)≥10 ng/mL = septic shock.
Statistical analysis
Analysis of the distribution of sex, foci of infection, PCT classes by time and groups and change in PCT classes by group, was performed using the Goodman test for contrasts between multinomial populations. Evaluation of groups by age and PRISM scores was performed using the Mann-Whitney U test.
All conclusions were drawn based on a 5% significance level.
Results
Inclusion and exclusion of patients
During the period chosen for the study, 689 patients were admitted to the PICU, 59 of whom met the diagnostic criteria for sepsis and 65 of whom had septic shock. Twelve patients were excluded from the SG (six were put on antibiotics for more than 24 hours, four were postoperative patients and two had degenerative neurological diseases), and 22 were excluded from the SSG (12 were given antibiotics for more than 24 hours, three had active chronic inflammatory diseases, two had degenerative neurological diseases, two had been given corticoids and three died before samples could be taken). The final sample, therefore, comprised 90 patients, 47 in the SG and 43 in the SSG.
Comparison of groups: general characteristics
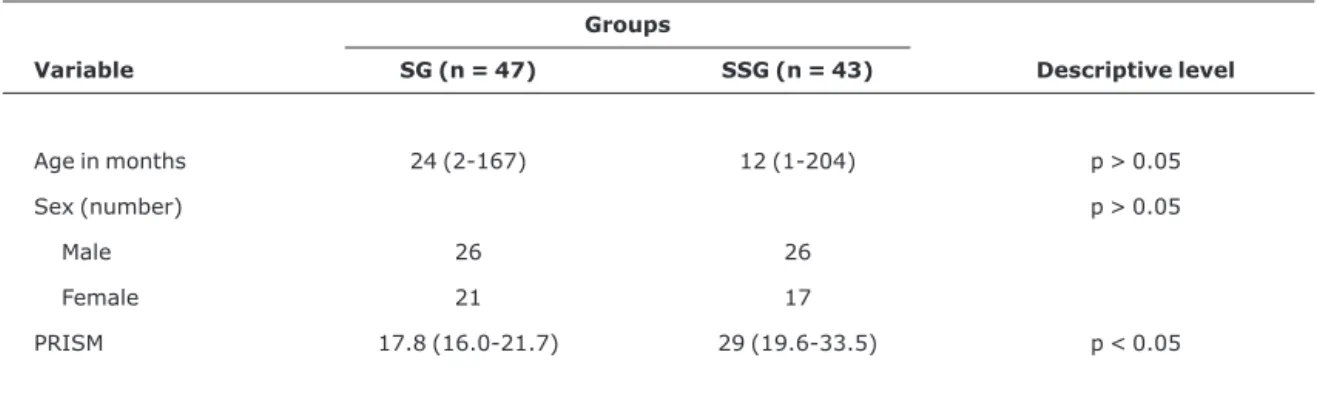
Table 1 is a comparison of the groups by age, sex and PRISM score. The groups did not differ statistically in terms of age or sex. They were, however, statistically difference in terms of severity of disease, assessed by the PRISM score, which was greater in the SSG [SSG: 29 (19.6-33.5) > SG:17.8 (16-21.7); p < 0.05].
The frequency of progression to MOSF was significantly greater in the SSG [SSG: 42/43 (97.7%) vs. SG: 11/47 (23.4%); relative risk = 4.17; p < 0.05]. Three (6.4%) patients in SG and 11 (25.6%) in the SSG died.
It was possible to isolate microorganisms in blood or cerebrospinal fluid cultures in 54 patients. Blood cultures were positive in 40 patients, 29 (72.5%) from the SSG, and cerebrospinal fluid cultures were positive in 14 children, 11 (78.6%) in the SSG. In 38 (70.4%) patients, gram-negative
Table 1- Comparison of SG and SSG in terms of median age (variation), sex and PRISM score
Groups
Variable SG (n = 47) SSG (n = 43) Descriptive level
Age in months 24 (2-167) 12 (1-204) p > 0.05
Sex (number) p > 0.05
Male 26 26
Female 21 17
PRISM 17.8 (16.0-21.7) 29 (19.6-33.5) p < 0.05
germs were identified (P. aeruginosa; H. influenzae; A. baumanii; andKlebsiellaspecies), in 11 (20.4%) cases they
were gram-positive (S. aureus; S. pneumoniae; S. epidermidis) and another four (7.4%) patients the infection was polymicrobial. A fungal infection (C. albicans) was diagnosed in one patient (1.8%).
The primary focus of infection was the lungs in the majority of patients in the SG [lungs: 33 (70.2%) vs. central nervous system: five (10.6%) vs. intestines: four (8.5%) vs. others: five (10.6%); p < 0.05] and in the comparison between the two groups [SG: 33 (70.2%) vs. SSG: 17 (39.5%); p < 0.05]. The distribution of foci was not statistically significant in the SSG, [lungs: 17 (39.5%) vs. central nervous system: 11 (25.6%) vs. intestine: eight (18.6%) vs. others: seven (16.3%); p > 0.05].
PCT at T0 and at T12h
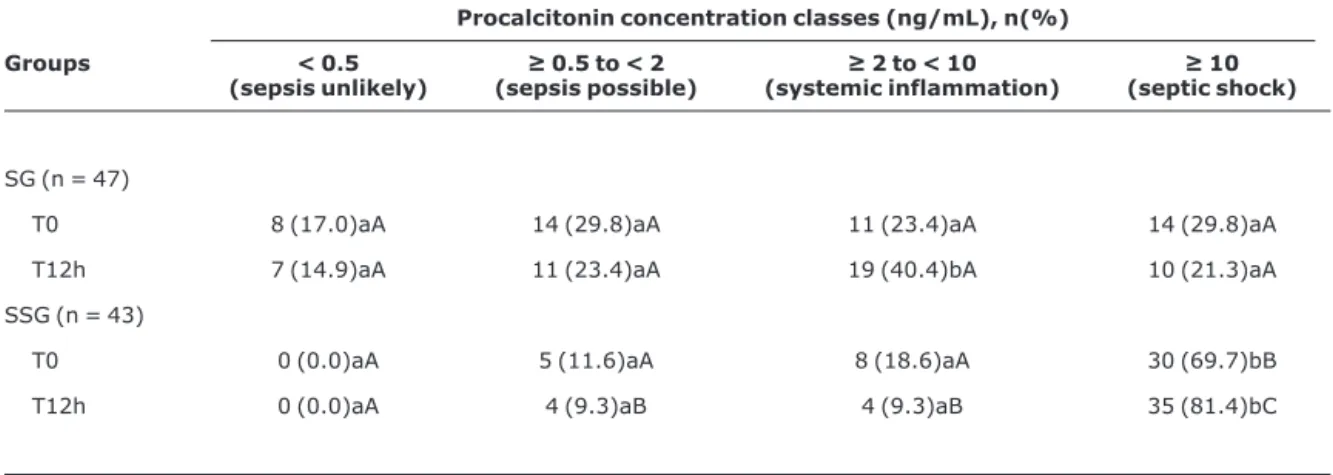
Table 2 shows the distribution of patients across the PCT concentration classes at T0 and T12h for the two groups. At T0, PCT was an indicator of severity, since it discriminated the patients with septic shock from those with sepsis, where the majority of patients in the SSG were in the≥10 ng/mL class, in contrast with what occurred in the SG, with the difference between groups being statistically significant for this class [SSG: 30 (69.7%) > SG: 14 (29.8%); p < 0.05]. The proportion of SSG patients in the highest PCT classes at T0 was significantly greater than that of patients in the other classes [class ≥10: 30 (69.7%) > class≥ 2 to < 10: 8 (18.6%) = class≥0.5 to < 2: 5 (11.6%) = class < 0.5: 0
(0%); p < 0.05]. In contrast, the distribution of SG patients across PCT classes could not be differentiated statistically.
The behavior of PCT at T12h was similar to at T0, i.e. the proportion of patients in the ≥10 class was significantly greater in SSG than in SG [SSG: 35 (81.4%) > SG: 10 (21.3%); p < 0.05]. Furthermore, there was also a statistically significant difference between the groups for≥2 to < 10, in favor of SG and indicating a greater number of patients from that group at lower PCT level classes [SG = 19 (40.4%) > SSG = 4 (9.3%); p < 0.05]. Within the SSG, a statistical difference was observed between the frequency of patients in the highest class, compared with the other classes. In contrast, there were no statistical differences in the distribution of SG patients across PCT classes.
Analysis of the proportion of patients whose PCT class changed between T0 and T12h demonstrated no statistical difference between the groups, with both groups having a predominance of patients who remained in the same class for both samples [SG: maintained same class = 39 (83%) > increased class = five (10.6%) = reduced class = three (6.4%) and SSG: maintained same class = 32 (74.4%) > increase class = nine (20.9%) > reduced class = two (4.7%); p < 0.05]. Nevertheless, in the SSG, despite a predominance of no class change, the number of patients who went from a lower class to a higher class was also significant.
Relationship between PCT and PRISM score
It was observed that the median T0 PRISM score for the 30 patients in the SSG who were in the highest PCT class was
Table 2- Distribution of patients in SG and SSG across procalcitonin concentration classes at T0 and T12h
Procalcitonin concentration classes (ng/mL), n(%)
Groups < 0.5
(sepsis unlikely)
≥0.5 to < 2 (sepsis possible)
≥2 to < 10 (systemic inflammation)
≥10 (septic shock)
SG (n = 47)
T0 8 (17.0)aA 14 (29.8)aA 11 (23.4)aA 14 (29.8)aA
T12h 7 (14.9)aA 11 (23.4)aA 19 (40.4)bA 10 (21.3)aA
SSG (n = 43)
T0 0 (0.0)aA 5 (11.6)aA 8 (18.6)aA 30 (69.7)bB
T12h 0 (0.0)aA 4 (9.3)aB 4 (9.3)aB 35 (81.4)bC
SG = sepsis group; SSG = septic shock group; T0 = admission; T12h = 12 hours later.
significantly greater than the median PRISM score of the 14 SG children in the same PCT class [SSG: 35.15 (40.5-28.7) vs. SG: 18.6 (21.4-10.2); p < 0.05].
Discussion
When managing septic patients, early diagnosis of the infection is the element which has the greatest impact on clinical course, treatment and patient survival.14 In this context, interest in markers of severe infection in children has been growing.
A systematic review followed by a meta-analysis was published in 2004 investigating the value of PCT as a marker of bacterial infection in adults and children.15Just two of the 12 studies analyzed involved children, and one of those enrolled newborn infants.16,17 The conclusions of the meta-analysis were that PCT is a more accurate marker than C-reactive protein for differentiating between viral and bacterial infections, and also for differentiation between bacterial infection and other causes of systemic inflammation. The review left open the question of using PCT for the diagnosis and prognosis of children with sepsis and septic shock.
Our study demonstrated that PCT was already capable of determining the severity of patients at the time of admission, differentiating children with sepsis from those with septic shock. Furthermore, we observed more elevated PRISM scores among patients with septic shock and higher PCT levels. These results are in agreement with findings made by Casado-Flores et al.,8who studied 80 children with suspicion of sepsis and observed that PCT offered better diagnostic and prognostic properties than C-reactive protein, and that levels were significantly more elevated among children with septic shock than among those with sepsis, and that PCT levels were higher among patients with higher PRISM scores. Other studies have reported similar results, identifying PCT as a marker for severity in children with meningococcal sepsis18 and in septic newborn infants,19in common with studies of adults.9,20
Luzzani et al.21studied 70 adults by means of daily PCT assays, demonstrating that this mediator is correlated with progression to MOSF. We were unable to establish a correlation between PCT levels and progression to MOSF. Nevertheless, we did observe that a significantly greater proportion of SSG patients developed MOSF, when compared with the children in the SG, and also that PCT levels were more elevated in the SSG.
In a significant percentage of our septic shock patients PCT levels increased as time passed, which is behavior that may be explained by the kinetics of the mediator itself. As was described earlier, PCT peaks later, between 6 and 24 hours, reducing later, at from 2 to 3 days.4It is also necessary to
consider the influence that antibiotic treatment has on PCT levels. Reductions in plasma concentrations of this marker have been described in response to the administration of antibiotics22and even that PCT might be useful for testing the response to antibiotic treatment.23This being so, our results may have been influenced by the use of antibiotics during the course of the disease, and this influence may have been more accentuated in less severe cases, blocking possible PCT increases in children in the SG.
There have been reports that some patients without clinical symptoms of sepsis present high PCT levels and, in contrast, that some patients who meet the clinical criteria for the disease do not have high levels of the marker. Furthermore, that ≥ 0.5 to 2 ng/mL PCT class (sepsis possible) has been labeled the “grey zone,” because of the difficulties in interpreting the result. We therefore understand that it is possible that in some of our septic patients inflammation was minimal and that others who were initially labeled as having sepsis actually had more severe systemic inflammatory conditions,20explaining the observation that some of the SG patients were in the PCT class that indicates septic shock and some children in the SSG were in the sepsis possible class.
These data support the statement that PCT can be considered an auxiliary method for the diagnosis of sepsis and reflects the severity of infection. However, this diagnostic method must be evaluated in the context of the patient’s clinical status, complementing careful clinical assessment and judgments based on other laboratory parameters, bearing in mind that clinical diagnosis of sepsis/septic shock is very often subjective and, consequently, uncertain. The future lies in demonstrating whether assaying PCT improves the prognosis of patients, by making early diagnosis possible and aiding with monitoring treatment.
Limitations and implications of this study
The reliability of a marker for sepsis/septic shock depends on the precision of clinical diagnosis, which should be sought ceaselessly in order to perfect clinical definitions, especially in children.
Conclusions
Plasma PCT levels on admission allowed sepsis and septic shock to be differentiated, with an even greater level of significance being possible after 12 hours, in the group studied here. The results suggest that PCT is valid for auxiliary diagnosis of septic conditions in children and useful as an indicator of the severity of patients. Double-blind and randomized studies are necessary before these findings can be generalized for the child population.
Acknowledgements
We would like to thank the whole team at the PICU and at the UNESP Pediatrics Department’s Clinical and Experimental Research Center for helping with data collection and laboratory analyses.
References
1. Angus DC, Wax RS. Epidemiology of sepsis: an update. Crit Care Med. 2001;29(7 Suppl):S109-16.
2. American College of Chest Physicians/Society of Critical Care Medicine Consensus Conference: definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Crit Care Med. 1992;20:864-74.
3. Levy MM, Fink MP, Marshall JC, Abraham E, Angus D, Cook D, et al. 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Crit Care Med. 2003;31:1250-6.
4. Meisner M. Biomarkers of sepsis: clinically useful? Curr Opin Crit Care. 2005;11:473-80.
5. Whicher J, Bienvenu J, Monneret G. Procalcitonin as an acute phase marker. Ann Clin Biochem. 2001;38(Pt 5):483-93.
6. Meisner M. Biochemistry. In: Meisner M, ed. Procalcitonin (PCT): a new, innovative infection parameter. Biochemical and clinical aspects. Stuttgard: Georg Thieme Verlag; 2000. p. 15-45.
7. Carrol ED, Thomson APJ, Hart CA. Procalcitonin as a marker of sepsis. Int J Antimicrob Agents. 2002;20:1-9.
8. Casado-Flores J, Blacon-Quirós A, Asensio J, Arranz E, Garrote JA, Nieto M. Serum procalcitonin in children with suspected sepsis: a comparison with C-proteitn and neutrophil count. Pediatr Crit Care Med. 2003;4:190-5.
9. Ugarte H, Silva E, Mercan D, De Mendonca A, Vincent JL. Procalcitonin used as a marker of infection in the intensive care unit. Crit Care Med. 1999;27:498-504.
10. Lapillonne A, Basson E, Monneret G, Bienvenu J, Salle BL. Lack of specificity of procalcitonin for sepsis diagnosis in premature infants. Lancet. 1998;351:1211-2.
11. Carcillo JA, Fields AI; Comitê de Força-Tarefa. Parâmetros de prática clínica para suporte hemodinâmico a pacientes pediátricos e neonatais em choque séptico. J Pediatr (Rio J). 2002;78:449-66.
12. Wilkinson JD, Pollack MM, Glass NL, Kanter RK, Katz RW, Steinhart CM. Mortality associated with multiple organ system failure and sepsis in pediatric intensive care unit. J Pediatr. 1987;111:324-8.
13. Pollack MM, Ruttimann EU, Getson PR. Pediatric risk of mortality (PRISM) score. Crit Care Med. 1988;16:1110-6.
14. Dellinger RP, Carlet JM, Masur H, Gerlach H, Calandra T, Cohen J, et al. Surviving Sepsis Campaign guidelines for management of severe sepsis and septic shock. Crit Care Med. 2004;32:858-73.
15. Simon L, Gauvin F, Amre DK, Saint-Louis P, Lacroix J. Serum procalcitonin and C-reactive protein levels as markers of bacte-rial infection: a systematic review and meta-analysis. Clin Infect Dis. 2004;39:206-17.
16. Hatherill M, Tibby SM, Sykes K, Turner C, Murdoch IA. Diagnostic markers of infection: comparison of procalcitonin with C reactive protein and leukocyte count. Arch Dis Child. 1999;81:417-21.
17. Enguix A, Rey C, Concha A, Medina A, Coto D, Dieguez MA. Comparison of procalcitonin with C-reactive protein and serum amyloid for the early diagnosis of bacterial sepsis in critically ill neonates and children. Intensive Care Med. 2001;27:211-5.
18. Carrol ED, Newland P, Thomson AP, Hart CA. Prognostic value of procalcitonin in children with meningococcal sepsis. Crit Care Med. 2005;33:224-5.
19. Resch B, Gusenleitner W, Muller WD. Procalcitonin and interleukin-6 in the diagnosis of early-onset sepsis of the neonate. Acta Paediatr. 2003;92:243-5.
20. Muller B, Becker KL. Procalcitonin: how a hormone became a marker and mediator of sepsis. Swiss Med Wkly. 2001;131:595-602.
21. Luzzani A, Polati E, Dorizzi R, Rungatscher A, Pavan R, Merlini A. Comparison of procalcitonin and C-reactive protein as markers of sepsis. Crit Care Med. 2003;31:1737-41.
22. Assicot M, Gendrel D, Carsin H, Raymond J, Guilband J, Bohuon C. High serum procalcitonin in patients with sepsis and infection. Lancet. 1993;341:515-8.
23. Brunkhorst FM, Heinz U, Forycki ZF. Kinetics of procalcitonin in iatrogenic sepsis. Intensive Care Med. 1998;24:888-9.
Correspondence: José R. Fioretto
Departamento de Pediatria-UNESP, Distrito de Rubião Júnior CEP 18618-000 – Botucatu, SP – Brazil