Penile Lesion from Gunshot Wound: a 43-Case Experience
Andre G. Cavalcanti, Renato Krambeck, Alexandre Araujo, Carlos H. Manes, Luciano A.
Favorito
Section of Urology, Souza Aguiar Municipal Hospital, Rio de Janeiro, RJ, Brazil
ABSTRACT
Objective: To demonstrate the main aspects of diagnosis, treatment and follow-up of 43 patients with gunshot wounds to the penis.
Materials and Methods: The location of the lesion, the presence of associated lesions, the performance of complementary exams, surgical treatment, postoperative complications and long term follow-up of 43 patients with penile lesions from gunshot wounds were retrospectively analyzed.
Results: Of 43 cases assessed, 41 were submitted to surgical exploration (95.3%) and 2 were submitted to conservative treatment (4.7%). We found penile lesions involving the corpus cavernosum in 37 cases; the remaining 4 patients presented no lesions involving the corpus cavernosum, urethra or testicles but did in the superficial structures. Ten cases presented an association with testicular lesions and 14 cases association with anterior urethral lesions.
Conclusion: Penile lesions from gunshot wounds should be treated with immediate surgical intervention. In exceptional situations featuring superficial lesions only conservative treatment may be applied.
Key words: penis; urethra; wounds, gunshot; surgical procedures, operative Int Braz J Urol. 2006; 32: 56-63
INTRODUCTION
Gunshot wounds to the genitalia are not fre-quent (1), however they need to be immediately in-vestigated to assess the extension of the lesion to re-productive organs and prevent complications, such as bleeding, infection, penile curvature, erectile dys-function and urethral stenosis (2).
The penis can be injured in an isolated way or in association with scrotal traumatism (3). Even though they are not frequent, urethral lesions can oc-cur, making uretrocystography mandatory for some researchers (3.4).
Many studies in the literature analyze diag-noses and conduct in patients who are victims of gun-shot wounds to the genitalia (5.6); however studies with a significant casuistic that solely analyze penile
lesions are rare (7). Studies that analyze conduct in urethral gunshot wounds are also rare (6,7).
The objective of the present study is to dem-onstrate the main aspects in the diagnosis, treatment and follow-up of 43 patients with penile lesions from gunshot wounds.
MATERIALS AND METHODS
as-sociated lesions, the performance of complementary exams, surgical treatment, postoperative complica-tions and patient follow-up were all analyzed.
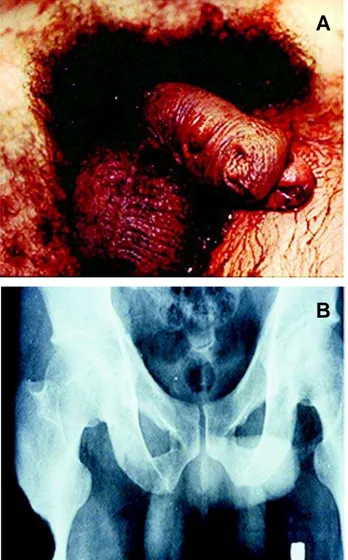
The main form of diagnosis assessment was anamnesis and physical examination (Figure-1). In 5 cases (11.6%), there was a need for complementary exams. Ultrasound was used in 2 cases to exclude corpus cavernosum lesions, and in 3 cases a cystothrogram was performed due to a suspicion of ure-thral lesions.
The surgical technique employed was a subcoronal incision with degloving of the penis and exposure of the corpus cavernosum and urethra.
RESULTS
Of the 43 cases analyzed, 41 were submitted to surgical exploration (95.3%) and only 3 received conservative treatment (4.7%). Table-1 outlines the lesions found during surgical exploration. In 37 cases we found penile lesions involving the corpus cavernosum; the remaining 4 operated patients did not present lesions either in the corpus cavernosum, urethra or testicles, and presented lesions only in su-perficial structures. Associations to testicular lesions occurred in 10 cases while association to anterior ure-thra lesions occurred in 14 cases. Extra-genital le-sions were present in 19 patients (44.2%), with thigh lesions appearing most commonly, as shown in Table-2.
Lesions in the corpus cavernosum were treated with local debridement and primary closure with absorbable sutures. Testicular injuries were treated with orchiectomy in 6 cases (60%) and re-construction in 4 cases (40%).
Of the 14 cases featuring anterior urethra le-sions, 11 (78.5%) had the lesion diagnosed during surgery. Cystostomy and reconstruction of the
ure-Location of the Lesion Cases %
Corpus cavernosum 13 30.2
Testicle + corpus cavernosum 10 23.2 Urethra + corpus cavernosum 14 32.6
Superficial lesion 06 14.0
Table 1 – The table shows the location of the lesions found
in 43 victims of gunshot wounds to the penis.
Table 2 – Location of extragenital lesions found in 43
victims of gunshot wounds to the penis.
Location of the Lesion Cases %
Thigh 15 34.8
Bone lesion 06 13.9
Vascular lesion 03 06.9
Intra-abdominal lesion 10 23.2 Absence of extragenital lesions 24 55.8
Figure 1 – A) Transfixing penile lesion associated to distal
ure-thra and glandar lesion. B) X-ray demonstrates the location of the bullet in the external face of the thigh.
A
thra were performed later in 2 cases and the other 12 cases received immediate treatment of the lesions. In 4 patients with extended partial lesions (> 2 cm) of the pendular urethra, a primary suture over a urethral catheter was performed; 3 of these patients (75%) required a second procedure due to postoperative thral stenosis, while 1 patient (25%) developed ure-thral cutaneous fistula which was treated with pro-longed urethral catheterization.
In 3 patients featuring pendular urethra le-sions (1 with a total lesion and 2 with partial lele-sions), a cutaneous urethrostomy was performed and a later reconstruction was conducted by rotating the cutane-ous flap; there was no postoperative stenosis or fistu-las in any of the 3 cases. In 5 patients, the lesion was to the bulbar urethra (distal portion). In 1 case a pri-mary suture was performed over the catheter and in 4 cases termino-terminal anastomosis was performed, presenting no postoperative complications. In the 2 patients where the cystostomy was performed as a primary treatment, late stenosis occurred, requiring urethral reconstruction.
A greater than 6 month follow-up was pos-sible in 30 patients – 11 with urethral lesions, 10 with lesions only in the corpus cavernosum and 9 with tes-ticle and corpus cavernosum lesions. None of the 30 cases presented penile curvature or erectile dysfunc-tion determining significant impact on the quality of sexual activity.
COMMENTS
Success in the treatment of penile lesions from gunshot wounds depends on early surgical ex-ploration, debridement of the wounded structures and primary lesion repair (8-10). Conservative treatment in these cases is controversial, except when clinical evaluation strongly indicates the presence of only superficial lesions (1). In our study, there was no sur-gical exploration in only 4.8% of the cases and clini-cal indications in those cases were only of superfi-cial lesions. During physical examination, these pa-tients presented presence of a minimum hematoma that allowed an adequate palpation of corpora cavernosa and testicles, with absence of lesions
con-firmed by ultrasound. In the other 4 cases (9.5%), the patients were submitted to surgical exploration based on the findings of physical examination; however, only lesions in superficial structures were found in these cases.
The use of the injury severity score from the American Association for the Surgery of Trauma (AAST) is being utilized to facilitate uniform treat-ment of genitalia lesions (1,11). According to this sification, superficial lesions and contusions are clas-sified as degree I and can be conservatively treated. Lesions classified as degree II (Buck fascia lacera-tions without tissue loss), degree III (cutaneous avul-sion or laceration through glands and meatus, or ure-thral or cavernosum lesions less than 2 cm in area), degree IV (partial penectomy or urethral or cavernosum lesions more than 2 cm in area), and de-gree V (total penectomy) shall be treated with sur-gery (1,11).
The majority of patients with penetrating le-sions in the genitalia should be submitted to immedi-ate surgical intervention; however in doubtful cases of degree I lesions according to AAST, the use of ul-trasound to exclude the lesions of the corpus cavernosum can be useful even though it is an opera-tor-dependent examination (12-15). In our sample, both patients that were not submitted to surgical in-tervention were submitted to ultrasound, which only confirmed the presence of superficial lesions.
3 cases where the exam confirmed the lesion, and in 11 cases the lesion was identified only during surgi-cal intervention.
In cases of suspicion of urethral lesion at ini-tial admission, retrograde cystourethrogram should be performed as the patient’s clinical conditions al-low. Penile degloving for surgical exploration should always be performed after urethral catheterization, as this maneuver will help identify transoperatively the urethral lesions.
In the cases of urethral lesions, primary re-pair is the option of choice (6), except in cases where there is an extended loss of urethral tissue (4), when staged treatment is the best choice. Of the 14 patients with urethral lesions, we performed cystostomy and late urethral reconstruction in only 2 cases (14.2%). Lesions of the pendular urethra (especially in distal and glandar portions) should be treated in a staged form due to the high frequency of complications.
Performing an urethrostomy as an initial pro-cedure seems to be an interesting choice since it will allow reconstruction using tissues where the thermal late lesion of the bullet is already defined. Termino-terminal anastomosis is possible for bulbar urethral lesions limited to the penoscrotal junction when there is an extension less than 1.5 cm. When the urethral lesion is only partial (less than 50% of the urethral circumference with longitudinal extension less than 1 cm), we believe that the primary closure of the le-sion over a catheter can be done; otherwise the op-tion of a termino-terminal anastomosis or staged treat-ment should be done, depending on the location of the lesion.
In the absence of a trained urological medi-cal team to reconstruct the lesion, or when the lesion is extended to the more distal portions of the bulbar urethra or to the posterior urethra, or when the clini-cal conditions do not allow exploration of the lesion, cystostomy shall be performed as a primary treatment.
CONCLUSIONS
Penile lesions from gunshot wounds shall be treated through an immediate surgical intervention, except in cases where there are only superficial
le-sions that should be confirmed by ultrasound. The primary repair of corpus cavernosum lesions seems to prevent the late development of complications. Urethral lesions should be treated, whenever pos-sible, at the moment of surgical intervention, while cases of extended lesions or those localized in dis-tal portions of the urethra should be submitted to 2-step surgery.
CONFLICT OF INTEREST
None declared.
REFERENCES
1. Mohr AM, Pham AM, Lavery RF, Sifri Z, Bargman V, Livingston DH: Management of trauma to the male external genitalia: the usefulness of American asso-ciation for the surgery of trauma organ injury scales. J Urol. 2003; 170: 2311-2315.
2. Morey AF, Metro MJ, Carney KJ, Miller KS, McAninch JW: Consensus on genitourinary Trauma: external genitalia. BJU Int. 2004; 94: 507-15. 3. van der Horst C, Martinez Portillo FJ, Seif C, Groth
W, Junemann KP: Male genital injury: diagnostics and treatment. BJU Int. 2004; 93: 927-30.
4. Tiguert R, Harb JF, Hurley PM, Gomes De Oliveira J, Castillo-Frontera RJ, Triest JA, et al.: Management of shotgun injuries to the pelvis and lower genitourinary system. Urology. 2000; 55: 193-7.
5. Gomez RG, Castanheira AC, McAninch JW: Gunshot wounds to the male external genitalia. J Urol. 1993; 150: 1147-9.
6. Husmann DA, Boone TB, Wilson WT: Management of low velocity gunshot wounds to the anterior ure-thra: the role of primary repair versus urinary diver-sion alone. J Urol. 1993; 150: 70-2.
7. Mydlo JH, Harris CF, Brown JG: Blunt, penetrating and ischemic injuries to the penis. J Urol. 2002; 168: 1433-5.
8. Brandes SB, Buckman RF, Chelsky MJ, Hanno PM: External genitalia gunshot wounds: a ten-year experi-ence with fifty-six cases. J Trauma. 1995; 39: 266-71; discussion 271-2.
10. Cline KJ, Mata JA, Venable DD, Eastham JA: Pen-etrating trauma to the male external genitalia. J Trauma. 1998; 44: 492-4.
11. Moore EE, Malangoni MA, Cogbill TH, Peterson NE, Champion HR, Jurkovich GJ, et al.: Organ injury scal-ing VII: cervical vascular, peripheral vascular, adre-nal, penis, testis, and scrotum. J Trauma. 1996; 41: 523-4.
12. Miller S, McAninch JW: Penile fracture and soft tis-sue injury. In: Traumatic and Reconstructive Urology. Edited by JW. McAninch. Philadelphia, WB. Saunders. 1996; chapt. 59, pp. 693-8.
13. Dierks PR, Hawkins H: Sonography and penile trauma. J Ultrasound Med. 1983; 2: 417-9.
14. Martinez Perez E, Arnaiz Esteban F, Perez Arbej JA, Nogueras Gimeno MA, Crespo Mayor V, Espuela Orgaz R: Fracture of the penis: two new cases. Re-view of the literature. Usefulness of echography. Arch Esp Urol. 1997; 50: 1099-102.
15. Koifman L, Cavalcante AG, Manes CH, Filho DR, Favorito LA: Penile fracture – Experience in 56 cases. Int Braz J Urol. 2002; 29: 35-39.
16. Hall SJ, Wagner JR, Edelstein RA, Carpinito GA: Management of gunshot injuries to the penis and ante-rior urethra. J Trauma, 1995; 38: 439-43.
Accepted after revision: September 30, 2005
Correspondence Address:
Dr. Luciano Alves Favorito Rua Professor Gabizo 104/201 Rio de Janeiro, RJ, 20271-320, Brazil Fax: + 55 21 3872-8802
E-mail: [email protected]
EDITORIAL COMMENT
Gunshot lesions of penis are often mutilat-ing with a high incidence of aesthetic, physical, dys-functional and psychological post-trauma morbidity and urinary and sexual disability. Most of patients develop significant mental disorders after trauma in genitalia area and for this reason, when you deal with this matter, it is mandatory to maintain penis func-tion and cosmesis.
In this issue of the International Braz J Urol, Cavalcanti and colleagues retrospectively reviewed 43 patients with a penile lesion by gunshot. Penile lesions involved the corpus cavernosum in 37 cases and in 14 cases, they found a urethral lesion. Authors stated that the primary repair of corpus cavernosum lesions is the accepted method of treatment in pa-tients who have lesions involving the corpora
cavernosa, but not urethra, and this surgical strategy may prevent the late development of complications, such as penile curvature as well as erectile dysfunc-tion.
Urethral lesion treatment, however, represent the main challenge for urologists, who have to face with acute trauma of penis involving urethra. We do agree with Cavalcanti et al., that urethral lesions should be treated, whenever possible, at the moment of early surgical exploration but cases of extended lesions or those localized in distal portions of the ure-thra with significant loss of tissue should be submit-ted to 2-step surgery.
complications such as hematoma or infection, which in turn can lead to secondary complications such as fistula, cosmetic defects and stenosis. Penile urethral stricture always represents a more difficult challenge in patients with failed primary repair after a trauma. Generally, it is the consequence of the corpus spongiosum damage (lack of it or fibrosis) because it represents the basic tissue to provide the adequate vascular and mechanical support to urethra. Authors did not report exactly what specific technique of ure-throplasty was used in their series or what material they used as transplanted substitute material. In 3 patients with pendular urethra lesions (1 with a total lesion and 2 with partial lesions), a cutaneous ure-throstomy was performed and a later reconstruction was conducted by rotating the cutaneous flap. We would like to advise that after a gunshot lesion of penis you can have a defect of penis and preputial skin and it will become scarred after the first surgical intervention. Therefore, we suggest avoiding the use of skin, and we prefer buccal mucosa graft when one chooses a multistage procedure.
All patients who underwent urethral repair after a gunshot trauma should be fully informed that
any surgical strategy might be complicated by steno-sis and that more than two surgical steps could be necessary to restore both urethral potency and accept-able aesthetic appearance of genitalia. The best strat-egy to repair urethra after the gunshot trauma remains unknown, however, it is probably the one with which the surgeon is most comfortable and it could be ap-propriately tailored on the single patient. No single technique is appropriate for all the complex situations after a penis trauma. It is a useful reminder to readers that this is a challenging surgery and should not there-fore be undertaken by surgeons who only dabble in this field. In the near future, tissue-engineering tech-nology could provide a new urethra with normal spongiosum tissue around the mucosal-urothelium strip, offering urologists a higher quality substitute material with which to work in selected situation.
Finally, I congratulate the authors in present-ing this informative series and a very candid account of their experience with gunshot lesions of penis. I think that the reader would fully concur with my take home message: urethral lesion by a gunshot trauma can be challenging and difficult to correct, even in the hands of experienced urethral surgeons.
Dr. Massimo Lazzeri
Department of Urology Casa di Cura Santa Chiara Firenze, Italy E-mail: [email protected]
EDITORIAL COMMENT
Gunshot wounds of the penis can be devas-tating injuries resulting in soft tissue loss, severe cos-metic deformities, erectile dysfunction and urethral injury. Any one of these results can cause tremen-dous problems for the patient and they involve uro-logical surgery.
Virtually all of these injuries come from hand-guns, which generally are of low velocity, and result
explora-tion should be planned in all patients unless careful examination can demonstrate only superficial skin injury without any large defect.
I believe that all patients with penile gunshot injuries should have preoperative retrograde urethrography. Certainly, most will be detected dur-ing operative exploration, as demonstrated by Cavalcanti and his colleagues. However, retrograde urethrography can accurately diagnose the injury pre-operatively and primary reconstruction can be planned with initial surgical exploration. Without urethrography, a missed urethral injury could result in major complications for the patient. This was not
true in Calvalcanti’s series, which indicate the care-ful evaluation of the urethra during surgical explora-tion. In most situations, the urethra can be repaired at the initial surgery as shown in this series.
Remarkably, these patients usually do ex-tremely well if managed as shown in this paper. Erec-tile function and cosmetic appearance are generally preserved and urethral strictures seldom occur when proper repair has been done.
This large series of penile gunshot wounds provides excellent guidelines for diagnosis and man-agement, and demonstrates the excellent outcomes, which can be achieved.
Dr. Jack W. McAninch
Department of Urology, University of California Chair of Urology, San Francisco General Hospital San Francisco, California, USA E-mail: [email protected]
EDITORIAL COMMENT
Large series describing genital gunshot wounds are rare in the literature. In the past decade, there are fewer than 6 published reports on the subject, describing only about 40 patients. This Brazilian report comes from an area of Rio de Janeiro with a vast and largely untapped experience with the treatment of genitourinary injuries from gunshot.
Need for urethrogram - In this series, urethrography was only rarely (7%) used. Caution must be exercised as 33% of patients ultimately had urethral injury. In the hands of these experienced genitourinary trauma surgeons, the urethral lesions were detected and repaired, but in centers with less experience, it is probably prudent to use preoperative urethrography more liberally than seen in this report. The authors also always placed a urethral catheter before exploration, and you should too.
Ultrasound - Adjuvant studies to determine if penile gunshot wounds injured the corpora cavernosa were used rarely in this report (5%), but this is the first such description of this protocol that I have seen. In general, it is probably a good idea to avoid exploration in those penile gunshot wounds that clearly do not breach the corpora, by either exam or imaging examination. In this series, 10% of patients had negative exploration, but I would suggest that 10% negative explorations is preferable to missing corporal or (especially) urethral injuries.
with pendulous urethral injury, all the 4 primarily repaired patients did poorly (developing fistula or stricture) while 3 were treated in a staged fashion, as in a Johanson urethroplasty. Like the authors, we tend to primarily repair those injuries with limited tissue damage, although in our experience complications were less common, perhaps because of lower caliber gunshot wounds or other patient factors. We also do not hesitate to exteriorize the injured urethral segment and return
for definitive repair at a later date, as the authors did, especially in more severe injuries.
How to repair bulbar urethral injuries? -All of the 5 repaired bulbar urethral injuries did well, and a 4/5 of these required anastomotic repair after excision of the injured segment. This technique is hardly reported in the literature previously, and should be considered by all those faced with this injury.