www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Newborn
physiological
responses
to
noise
in
the
neonatal
unit
夽
,
夽夽
Sandra
Maria
Schefer
Cardoso
a,b,∗,
Lorena
de
Cássia
Kozlowski
c,
Adriana
Bender
Moreira
de
Lacerda
a,
Jair
Mendes
Marques
a,
Angela
Ribas
daCommunicationDisorders,UniversidadeTuiutidoParaná(UTP),Curitiba,PR,Brazil bHospitaldeClínicasdoParaná(UFPR),Curitiba,PR,Brazil
cHearingandLanguageCenter,UniversidadeTuiutidoParaná(UTP),Curitiba,PR,Brazil dDepartmentofPhonoaudiology,UniversidadeTuiutidoParaná(UTP),Curitiba,PR,Brazil
Received5December2013;accepted6November2014 Availableonline7September2015
KEYWORDS
Prematurebirth; Hearing; Neonatology; Noiseeffects; Noise
Abstract
Introduction:The incorporation of technologies in the care of infants has contributed to increasedsurvival;however,thishasturnedneonatalunitintoanoisyenvironment.
Objective: Toevaluatethephysiologicalandfunctionaleffectsresultingfromtheexposureto noiseonlow-weightnewbornsinincubatorsinaneonatalunit.
Methods:Prospective,observational,quantitative,exploratory,descriptivestudy.Theadopted statisticalmethodincludedtablesoffrequency,descriptivestatistics,andStudent’st-test,with a0.05levelofsignificance.Asdata collectiontools, theenvironmental noiseandthenoise insideoftheincubatorwereevaluated,andtheAssessmentofPretermInfantBehaviorscale was usedtoassess prematurenewbornbehaviorandprojectedspecificallytodocumentthe neurobehavioralfunctioningofpreterminfants.ThedatacollectionoccurredfromSeptember of2012toAprilof2013;61low-weightnewbornsadmittedintheneonatalunitandinincubators wereobserved.
Results:Significantdifferencesinthevariablesheartrateandoxygensaturationwerenoted whennewbornswereexposedtonoise.
Conclusion: Low-weightneonatesinincubatorspresentphysiologicalalterationswhenfacing discomfortcausedbyenvironmentalnoiseinneonatalunits.
© 2015Associac¸ãoBrasileira de Otorrinolaringologiae CirurgiaCérvico-Facial. Publishedby ElsevierEditoraLtda.Allrightsreserved.
夽 Pleasecitethisarticleas:CardosoSMS,KozlowskiLC,deLacerdaABM,MarquesJM,RibasA.Newbornphysiologicalresponsestonoise
intheneonatalunit.BrazJOtorhinolaryngol.2015;81:583---8.
夽夽Institution:HearingandLanguageCenter,UniversidadeTuiutidoParaná(UTP),Curitiba,PR,Brazil.
∗Correspondingauthor.
E-mail:[email protected](S.M.S.Cardoso). http://dx.doi.org/10.1016/j.bjorl.2014.11.008
PALAVRAS-CHAVE
Recém-nascidode baixopeso; Audic¸ão; Neonatologia; Efeitosdoruído; Ruído
Respostasfisiológicasdeneonatosfrentearuídosemunidadeneonatal
Resumo
Introduc¸ão:A incorporac¸ãode tecnologias no cuidado dos recém-nascidos contribui para o aumentodasobrevivência,porém,transformouasunidadesneonataisemlocaismuitoruidosos.
Objetivo:Avaliarosefeitosfisiológicosefuncionaisdecorrentesdeexposic¸ãoaruídosemuma unidadeneonatalemrecém-nascidosdebaixopesoemincubadora.
Método: Estudoprospectivo,decaráterobservacional,deabordagemquantitativaenatureza descritivaexploratória.Ométodoestatísticoutilizadofoiodetabelasdefrequência,estatística descritivaeotestetdestudentpareado,aoníveldesignificânciade0,05.Comoinstrumento decoletadosdadosfoiavaliadooruídoambiental enointeriordasincubadoraseutilizada aescalaassessmentofpreterminfantbehaviorparaavaliac¸ãodocomportamentodosbebês prematuroseprojetadaespecificamenteparadocumentarofuncionamento neurocomporta-mentaldosbebêspré-termo.Acoletadosdadosaconteceunoperíododesetembrode2012a abrilde2013eforamobservados61recém-nascidosdebaixopesoemincubadorainternados naunidadeneonatal.
Resultados: Verifica-seaexistênciadediferenc¸assignificativasnavariávelfrequênciacardíaca esaturac¸ãodeoxigêniofrenteàexposic¸ãoaruídos.
Conclusão:Recém-nascidosde baixopeso emincubadora apresentamalterac¸õesfisiológicas quandoseencontramemdesconfortocausadopeloruídoambientedeunidadesneonatais. ©2015Associac¸ãoBrasileira deOtorrinolaringologiaeCirurgiaCérvico-Facial.Publicadopor ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Neonatal intensive care units (NICUs) are important resources for the treatment of severely or potentially severelyillpatientsinneed ofcontinuousandspecialized care as a result of a wide variety of pathophysiological changes.1
The incorporation of technologies for the care of the
newborn(NB)contributestoincreasesurvival;however,this
turnedneonatalunits(NUs)intoverynoisyenvironments.2
IntheNU,theNBusuallyisinanincubator,which
func-tions toreplace the mother’swomb, maintaining a warm
environmentandregulatingtemperature,dependingonthe
NB’s temperature. The incubator provides the necessary
moisturefortheNB’sbalanceandprotectsitfrominfection
andnoise.2,3Allcareandtreatment,includingweighing,are
carriedoutinsidetheincubator.3,4
ExcessivenoisefoundinNUscomesfromvarioussources,
suchaslifesupportequipment,includingmechanical
ven-tilators,radiantwarmers,infusion pumps,andincubators;
voices/talkingandmovementofpeopleintheunit;alarms;
medicalandfamilyvisits;handlingofincubators;circulation
oftestequipment;carelesshandlingwhenlockingcabinets,
drawers,trashlids,anddoors;andairconditioning,among
others.5Thesideeffectsofthetherapeuticprocess,in
addi-tionto the biological fragility and the long stay in those
units,canincreaseriskstohealth,includinghearingcare.5,6
InaNICU,environmentalconditionsaffectthe
physiolog-icalandneurobehavioralstatusoftheNB,thustheneedto
promoteasuitableenvironment,acquaintingtheNBwithit
anddecreasingtheamountandintensityofexcessivenoise
andlightstimuli.7,8
The noise of the equipment can affect NBs, causing
increases in heart rate (HR) and respiratory rate and
decreases in peripheral oxygen saturation, as well as
changes in motor activity. NB placement in a noisy
envi-ronmentfor morethan48his consideredarisk factorfor
hearingloss.9
TheBrazilianregulatorystandard(normabrasileira
regu-lamentadora[NBR])10152/1987oftheBrazilianAssociation
for Technical Standards (Associac¸ão Brasileira de Normas
Técnicas[ABNT])determines35---45dBA(dBA---decibelswith
a frequency Aweightingfilter thatapproximates the
cor-responding auditory sensation to a isophonic curve of 40
phones)asacceptablelevelsfor emptyhospitals;thefirst
value is thedesired level,and thesecond theacceptable
limit.10
AuditoryrestisimportanttoNBsfortheirdevelopment
andgrowth,andtoavoidrespondingtothestresscausedby
thenoise,whichcanresultindelayinweightgainandeven
indelayintheNB’sdischarge.11,12Inadditiontothedamage
alreadymentioned,ifthenoisereachesveryhighlevels,it
cancausehearinglossandhighbloodpressure
(physiologi-caleffects);disturbances(psychologicaleffects),stress,low
performance, interference with oral communication, and
irritability.7,11,12
The aim of this study was to evaluate the effects on
physiologicalandfunctionalresponsesresultingfromnoise
exposureintheenvironmentofaNUwithlow-birthweight
infantsinincubators.
Methods
The study was approved by the Ethics Committee for
Research in Humans, according to the tasks specified in
Resolution CNS 196/96, under opinion No. 105.197 on
Parentsorguardiansofallstudyparticipantsspontaneously
signedtheinformedconsent.
TheNBsampletoparticipateinthestudywasperformed
byasystematicsamplingtechnique(simplifiedformof
ran-domsampling).Arepresentativesample ofthenumberof
NBsattendedtoin thehealth unit (n=61) wasused.
Sta-tistical analysis was performed using descriptive (mean,
minimum,maximum,andstandarddeviation)and
inferen-tial(Student’st-testforpaireddata,atthe0.05significance
level)methods.Theanalyseswereperformedusing
Statis-tica7.0software.
Toparticipateinthestudy,NBswererandomlychosenas
theywerebeingadmittedtotheNICU;theNBswere
evalu-atedaccordingtoinclusionorexclusioncriteriaestablished
forthisstudy.
Theinclusioncriteriawere:Informedconsentsignedby
parents or guardians; weightbetween 1500 and 2500g (a
lowweightbypediatricparameters);duringhospitalization,
continuedplacementintheincubator; andanotoacoustic
emissions test (OAET) with a result of ‘‘approved.’’ The
testisperformedwiththeNBinastateofnaturalsleep,is
painless,hasnocontraindications,andlastsaround10min.
Forthistest,aheadsetconnectedtoacomputerisapplied
totheNB’sear.Thedeviceemitslow-intensitysoundsand
collectstheresultsproducedbytheNB’sear.Forthis
exam-ination,theotoReadversionTE(Interacoustics)equipment
wasused.
The exclusion criteria were: OAET with a result of
‘‘failed’’; refusal of parents or guardians to participate
in the study; refusal to sign informed consent; NB not
within 1500---2500g during the study period; presence of
syndrome(s);anddeathoccurringduringthestudy.
The measurementsof sound pressure levels wereheld
attheNUinNovember2012andMarch2013,accordingto
thelegalcriteriaestablishedbyBrazilianlaw,OrdinanceNo.
3214/78of theMinistryof LaborandEmployment,NR 17,
Ergonomics,andNBR10152/2000.13
Theinstrumentusedtonoiseevaluationwasahandheld
soundmeter,BruelandKjaerIntegratorbrand,type2230,
withmonthlycalibrationandownedbyFUNDACENTRO/PR;
the evaluation was performed by an engineer of the
institution. For evaluation of sound pressure levels, the
operationwasconductedincompensatingcurve‘‘A’’,and
variousmeasurementswereconductedinthemorningand
afternoon,bymeasuringtheminimumandmaximumlevels
and the mean level provided by the Leq measurement
resourceinNUrooms.
Themeasurementofenvironmentalnoiseoccurredintwo
characteristictimes,asfollows:(1)theusualsituationinthe
NICU,thatis,atthetimeofhighestnoiseinthosemoments
ofhigherflowofpeople,useofequipmentforclinical
con-trol,shiftchanges,medicalvisits, performingprocedures;
(2)inquietermoments,thatis,whenthereisless
produc-tionofnoise(naptime).The‘‘naptime’’intheNUisthe
timefor complyingwiththeNB’sneed forrest.There are
three‘‘naptime’’moments:oneinthemorning,anotherin
theafternoon,andthethirdatnight.During‘‘naptime’’,
thecaretakersdecreasetheiractivities,trynottotalk,the
parametersofdeviceswithalarmsaredecreased,andthe
movementofpeopleisalsodiminished.
Concomitanttoeachmeasurement,noisewasmeasured
withinincubators, that is, during the time of more noise
intheNU, thenoisewasmeasuredoutside andinsidethe
incubators, aswell asat the time of least production of
noise.
Datacollectionwasconducteddailyduringabout30min
foreachobservation,andintwoperiods(dutyshifts);thus,
alltimesonthesamedayofobservationwereconsidered.As
adatacollectioninstrument,APIB(AssessmentofPreterm
InfantBehavior)scale validated byAls in1982, wasused.
Thisisawidelyusedtoolfor prematureNBs’performance
evaluation,designedspecificallytodocument
neurobehav-ioralfunctioningofpretermNBs.
Theresultswerecomparedinthetwotimeperiods(the
usualsituationoftheNICUandduringthenaptime).
Asthestatisticalmethod,frequencytablesandthe
Stu-dent’spairedt-testwereusedatthe0.05significancelevel
(5%).ThesoftwareusedwasStatisticaversion7.0.
Sixty-oneunderweightNBswereobserved;theyweighed
between1500and2500gandwereintheincubator.NoNBs
hadanykindofhealthproblemotherthanlowweight.
Results
Table1liststheresultsofthedescriptivestatisticsofthe
variablesunderanalysis:Leqnoise(meanlevel),minimum
noise,maximumnoise,weight,oxygensaturation(O2),HR,
andAPIB (n=61), comparing twopredetermined times of
observationinthestudymethodology:quietnesstime(nap)
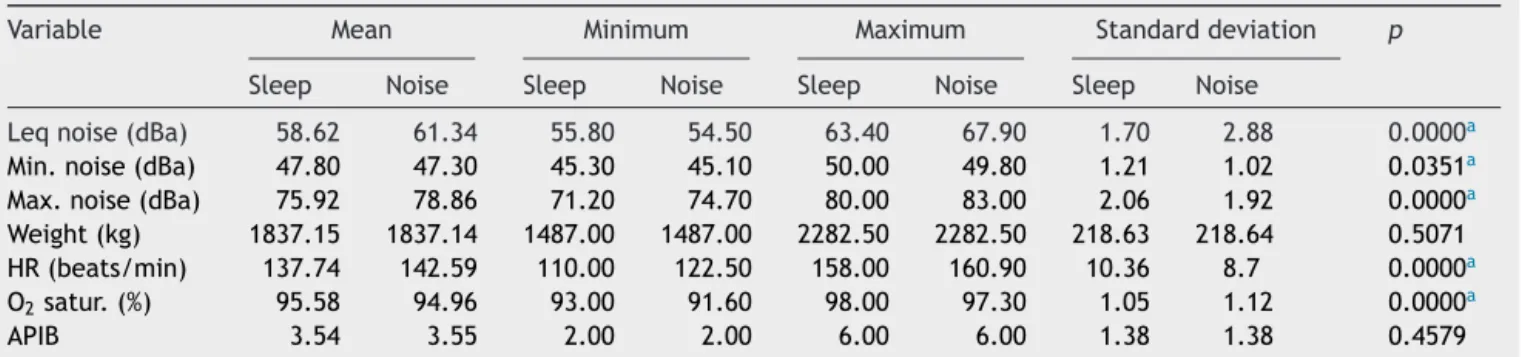
Table1 Descriptivestatisticsofthevariablesanalyzedandcomparisonbetweengroups:SandR(n=61).
Variable Mean Minimum Maximum Standarddeviation p
Sleep Noise Sleep Noise Sleep Noise Sleep Noise
Leqnoise(dBa) 58.62 61.34 55.80 54.50 63.40 67.90 1.70 2.88 0.0000a
Min.noise(dBa) 47.80 47.30 45.30 45.10 50.00 49.80 1.21 1.02 0.0351a
Max.noise(dBa) 75.92 78.86 71.20 74.70 80.00 83.00 2.06 1.92 0.0000a
Weight(kg) 1837.15 1837.14 1487.00 1487.00 2282.50 2282.50 218.63 218.64 0.5071 HR(beats/min) 137.74 142.59 110.00 122.50 158.00 160.90 10.36 8.7 0.0000a
O2satur.(%) 95.58 94.96 93.00 91.60 98.00 97.30 1.05 1.12 0.0000a
APIB 3.54 3.55 2.00 2.00 6.00 6.00 1.38 1.38 0.4579
and usual situation (increased production of noise). This
tableliststhemean,minimum,andmaximumofvariables
andthestandarddeviation.
Withtheuse ofthe pairedStudent’s t-test at the0.05
significancelevel(5%),significantdifferenceswereobserved
amongthemeansforthefollowingvariables:Leqnoise,
min-imumnoise,maximumnoise,HR,andO2saturation,thatis,
infaceofintensenoise,anincreaseinHRandadecreasein
O2saturationwereobserved.
As for the relationship of physiological and functional
variablesbetweenthetwomostdifferenttimesoftheday
(naptimeandthe mostnoisy time),it wasobservedthat
theresultofthisdatacrossinghassignificanceamongnoise
variablesandphysiologicaldata,especiallyHRandoxygen
saturation.ForthevariableHR,avariationbetween110and
160beatsperminutecanbenoted,whichisanimportant
change, considering thereference standard for NBs,even
forunderweightNBs,isameanof120beatsperminute.
Another variable, O2 saturation, which represents the
percentageof inspiredoxygen that reachesthe more
dis-tantcellsinthebody,alsoshowsaverysignificantvariation,
between91%and98%,consideringthatthenormallevelis
100%.
AsfortheregistryofAPIBevaluationindexes,which
mea-sure the behavioral reaction of NBs in times of rest and
untilactivestimulationbytheevaluator,2avariationfrom2
(verygood)to6(moderatetopoor)wascomputed.
There-fore,itcanbeconcludedthatNBsexhibitphysiologicaland
functionalchangeswheninastateofdiscomfortcausedby
environmentalnoise.
Discussion
Akeyaspect inthecareof aprematureNB istomake an
attempttoreproduce,intheNICU,thoseconditions
expe-rienced bythe NB in the intrauterineenvironment, while
producingsufficientappropriateincentivesinorderto
pro-motedevelopment.14
However,inthepresentNU,aswellasinmanyBrazilian
NUs,theintensityofthemeasurednoiseexceedsacceptable
levels.15---18
InastudyperformedinaNUtodecreasethenoiselevel
intheenvironment,itwasfoundthateveninsignificantly
reduced noise levels, the remaining noise was still more
intensethantherecommended.19
Themeasurementatbothtimesstudiedhere(naptime
and time of greatest noise) exceeded 45dBA, and in the
‘‘naptime’’, the resultof the ‘‘minimummeasurement’’
variable is greater than when more noise generators are
functioning.Thisisjustifiedwithnoisesofimpact(alarms,
handlingofincubators,circulationoftestequipment,
care-less handling of cabinet locks,drawers, trash lids, doors,
airconditioning,etc.)producedinmomentsofsilence,but
recordedbythesoundequipment.
In2011,theBrazilianMinistryofHealthstatedthatNICUs
showquitehighnoiselevels,withameanof77.4dB(A)for
background noise, a meanof 85.8dB(A) for noise peaks,
andwithasignificant increase duringcare proceduresfor
theNB.
InaNICUstudyconductedin2011,thenoisemeasured
for48h achievedamean of65---74dB(A).20 InNICUs, the
desiredlevelsshouldnotexceedLeq=50dB(A),Lmin=55dB
(A),andLmax<70dB(A).21,22
Analyzingthedata ofthe authors’research,thesound
pressure levels in the NICU studied were: Lmin. 47.80dB
(A)and47.30dB(A)andLmax.75.92dB(A),and78.86dB
(A);therecordedmeanwas58.62dB(A)and61.34dB(A)
---valuesgreaterthantherecommendedstandard.
In a noisy environment, behavioral and physiological
changes in people exposed to this phenomenon can be
observed.4,6---8,23
Intheliterature,thereisevidenceofdeleteriouseffects
ofhighlevelsofsoundpressureoccurringinNBs,for
exam-ple,higherO2consumptionandincreasedHR,whichresultin
higherenergyconsumptionandinadelayinweightgain.14,24
PhysiologicalandbehavioraleffectsinNBsexposedtonoise,
suchascrying,agitation,andsleepdisorders,amongothers,
arealsoemphasized.25,26
When observing NBs in a NU, the principal observed
changes occur in HR and oximetry; these changes were
described in a study where signs of stress were noted in
noisyenvironments,notablyincreasedHRanddecreasedO2
saturation.14
Another study observed physiological effects of noise
in the NICU including changes in HR, increases in blood
pressure, decreases of O2 saturation, apnea, increased
intracranial pressure, and possible immune and
neuroen-docrine effects, in addition to behavioral and cognitive
changes.21
Thepresentstudyhadthefollowingresults:increasedHR
(p=0.0000andstandard deviationof10.36,whensleeping
and8.7innoise,respectively)anddecreaseofO2saturation
inNBsinincubators,inthepresenceofhigherenvironmental
noiselevels(p=0.0000andastandarddeviationof1.05and
of1.12,whensleepingandinnoise,respectively).
Basedontheabovementionedstudies,itisinferredthat
theNBsobservedinthisstudyrespondedphysiologically,in
linewithliteraturefindings.
AsfortheuseofAPIBforobservingthebehaviorofNBsin
incubatorsintheNICUusedinthisstudy,thistoolenabled
averystraightforwardmethodofscoringtheNB’sbehavior
andtheNB’sabilitytoadapttonewsituations.Asaresult,a
variationinthescoregiventoadaptivebehavioroccurred,
from2(verygood)to6(moderatetopoor).Itwasalsofound
thatNBswithgreaterweightandgestationalagearebetter
abletoadaptbehaviorally.
Searchingtheliteratureforsupportforthisobservation,
it wasfound thatit is essential torespectthe behavioral
state of the NB when in deep sleep; if the NB is
cry-ing,onemust fullycomfortthe NBbeforeperformingthe
manipulation.8Alsointhissense,theliteraturepointsout
that thecaregiver,when watchingthe NB,shouldbe
cog-nizant of signals of poor adaptation to the environment
issued by the NB, for instance, breathing, posture,
mus-cletone,changesinbodymovement,irritability,continuous
crying,diffusesleep,andhyperarousal,amongothers.8
Inthebook‘‘UniversalDeclarationofRightsforthe
Pre-matureBaby’’,27 ArticleVIIstates:‘‘Everyprematurebaby
hastherighttorestandoneshouldthereforecomplywith
itsperiodoflightanddeepsleep,whichwillhenceforthbe
takenasessentialtoitsproperpsychicdevelopmentandits
biologicalregulation.Interruptingrandomlyand
indicativeofabuse.’’AndintheArticleVIII:‘‘Every
prema-turebabyhas theinalienableright tosilence, thatallows
the baby to feel as close as possible to the intrauterine
soundenvironment,inrespecttoitsthresholdsand
sensi-tivity.Anysoundsourcethatdisrespectsthisrightshallbe
deemedcriminal,heinous,andrepugnant.’’
InnoiselevelmeasurementsintheNUstudied,the
maxi-mumlevelmeasuredwas71.2---83dBA.Thesemeasurements
occurredatmomentsofgreatestexcitementwithintheNU.
Againstthis,acontroloftheambientnoiselevelwas
rec-ommended,whichshouldbeapracticeadoptedbyallNUs,2
becauseofthevulnerabilityoftheassistedclientele.
Consideringthehighsoundpressurelevelsfoundinthis
studyandtheireffectonlow-weightNBsinincubators,the
resultsshowtheneedforinterventionsinordertoachieve
therecommendedsoundpatternsandimprovecare.
Some studies have been conducted in order to gain
awareness on the perception of professionals working in
the NICU and parents of hospitalized NBs, with respect
to the existing noise in these environments,28 and for
implementingeducationalprograms29intheseplaces;their
authorssuggestedtheimplementationofawarenessraising
programs.
Therefore, caretakers should rely on knowledge,
plan-ning, teamwork, motivation, lifelong learning, and
feed-back.Physicalchangesintheunitaftercarefulplanningmay
beoneofthemoreeasilyappliedaspects.Thebiggest
chal-lengeresides in humanactivity, themain noise-producing
factorwithintheNU.23
It is recommended that periodic monitoring of sound
pressurelevelsinthreeshiftsanddifferentdaysoftheweek
isconducted.
Importantly, thereis no adverse effect,known or
pro-posed, that would inhibit or limit the adoption of sound
controlmeasures.
In this study, it is possible to search for strategies for
improving the quality of life of high-risk NBs, both with
regard totheir hearing conservation andto minimize the
psychological and physiological effects from exposure to
noise.
The scientificproduction intheareainquestion isstill
in its infancy, because many studies measuring NU
envi-ronments,orassessingthedevelopmentoflow-weightNBs,
havebeenpublished,butlaterintheNBs’livesandoutside
the NU. Thus, this study may be important toencourage
investigatorstodeploynoisereductionprogramsinNUsin
ordertoimprovethequalityoflifeoftheNB.
Conclusion
Thisstudyshowedhighsoundpressurelevelsinthe
environ-mentoftheNICUandalsodemonstratedchangesobserved
inNBs,whichwerecausedbythenoisyenvironment.
It isconcludedthatNBsareaffectedby environmental
noiseasshownintheirphysiologicalorfunctionalchanges,
especiallyatmomentsofhighersoundproduction.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.BRASIL. MinistériodaSaúde. SecretariadeAtenc¸ãoàSaúde. Brasília:MinistériodaSaúde;2010.
2.NogueiraMFH.Mensurac¸ãoderuídoemunidadesneonataise incubadorascomrecém-nascidos.RiodeJaneiro:UERJ;2011. 3.OliveiraICS.Oadventodasincubadoraseoscuidadosde
enfer-magemaosprematurosnaprimeirametadedoséculoXX.Texto ContextoEnfermFlorianópolis.2004;13:459---66.
4.Santiago L. Humanizac¸ãoem UTI neonatal. São Paulo: UTC; 2009.
5.Aurélio SF, Tochetto TM. Mensurac¸ão do ruído em uma UTI neonatal.ActaPediátrPort.2010;41:64---8.
6.MunizLMN,StroppaMA.Desconfortodospacientesinternados naUTIquantoàpoluic¸ãosonora.RAHIS;2009.p.56---62. 7.ReichertAPS,LinsRNP,ColletN.Humanizac¸ãodocuidadoda
UTIneonatal.RevEletrônEnferm.2007;9:200---13.
8.Tamez RN, Silva MJ. Impacto do ambiente da UTI neonatal no desenvolvimento neuromotor.Rio de Janeiro: Guanabara Koogan;2006.p.147---54.
9.American Academy of Pediatrics,Joint Committee onInfant Hearing. Position statement: principles and guidelines for earlyhearingdetectionandinterventionprograms.Pediatrics. 2007;120:898---921.
10.NBR10152-Níveisderuídoparaconfortoacústico---ABNT;1987. 11.KamlinCO,O’DonnelCP,EverstNJ,DavisPG,MorleyCJ. Accu-racyofclinicalassessmentofinfantheartrateinthedelivery room.Resuscitation.2006;31:9---21.
12.MacedoISC.Avaliac¸ãodoruídoemunidadesdeterapia inten-siva.BrazJOtorhinolaryngol.2009;74:844---6.
13.PortariaMTBN◦3.214,DE08DEJUNHODE;1978.
14.GaívaMAM,MarquesiMC,RosaMKO.Osonodorecém-nascido internadoemunidadedeterapiaintensiva:cuidadosde enfer-magem.RevCiêncSaúde.2010;9:602---9.
15.PinheiroEM, Guinsburg R, NabucoMAA, Kakehashi TY. Ruído na unidade de terapia intensiva neonatal e no interior da incubadora.RevLatino-AmEnferm.2011;19:1---8.
16.NogueiraMFH,DiPieroKC,RamosEG,SouzaMN, DutraMVP. Mensurac¸ãoderuídosonoroemunidadesneonataise incubado-rascomrecém-nascidos;revisãosistemáticadeliteratura.Rev Latino-AmEnferm.2011;19:1---10.
17.Cardoso MVLML, Chaves EMC, Bezerra MGA. Ruídos e barul-hos na unidade neonatal. Rev Bras Enferm Bras. 2010;63: 561---6.
18.PeixotoPV,Araújo MAN,Kakehashi TY,PinheiroEM.Nívelde pressãosonoraemunidadedeterapiaintensivaneonatal.Rev EscolaEnfermUSP.2011;45:1309---14.
19.Zamberlan-AmorimNE,FujinagaCI,HassVJ,FonsecaLMM, For-tunaCM,ScohiCGS.Impactodeumprogramaparticipativode reduc¸ãodoruídoemunidadeneonatal.RevLatino-AmEnferm. 2012;20:109---16.
20.MinistériodaSaúdeCuidadoscomorecém-nascidopré-termo. Atenc¸ãoàSaúdedoRecém-Nascido.Guiaparaosprofissionais deSaúde.Brasília-DF;2011.
21.Gray L, Philbin MK. Effects of the neonatal intensive care unit on auditory attention and distraction. Clin Perionatol. 2004;24:3---60.
22.Phiblin MK,RobertsonA, HallJW. Recommendedpermissible noise criteriafor occupied, newly constructed or renovated hospitalnurseries.JPerinatol.2011;87:183---5.
23.WeichTM,OuriqueAC,TochettoTM,FranceschiCM.Eficácia deumprogramaparareduc¸ãoderuídoemunidadedeterapia intensivaneonatal.RevBrasTerapiaIntens.2011;23:327---34. 24.KakehashiTY,PinheiroEM,PizzarroG,GuilhermeA.Nívelde
25.GomesCF,CrivaraMM. Osruídoshospitalareseaaudic¸ãodo bebê.RevBrasOtorrinolaringol.1998;64:453---7.
26.D’ArcadiaMZ,NeriERF,AlvesSP.Estresseneonatal:osimpactos doruídoedasuperestimulac¸ãoauditivaparaorecém-nascido. RevMov.2012;5:217---22.
27.TavaresLAM.Umadeclarac¸ãouniversaldedireitosparaobebê prematuro.1sted.CamposdoGoytacazes:Autor;2011.
28.AurélioFS, TochettoTM.Ruído em umaUnidade de Terapia IntensivaNeonatal: mensurac¸ãoepercepc¸ãode profissionais epais.RevPaulPediatr.2010;28:162---9.