www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Suppurative
labyrinthitis
associated
with
otitis
media:
26
years’
experience
夽
,
夽
André
Souza
de
Albuquerque
Maranhão
a,b,∗,
Valeria
Romero
Godofredo
c,
Norma
de
Oliveira
Penido
a,baDepartmentofOtorhinolaryngology,EscolaPaulistadeMedicina,UniversidadeFederaldeSãoPaulo(EPM-UNIFESP),SãoPaulo,
SP,Brazil
bDepartmentofHeadandNeckSurgery,EscolaPaulistadeMedicina,UniversidadeFederaldeSãoPaulo(EPM-UNIFESP),
SãoPaulo,SP,Brazil
cDepartmentofMedicine,EscolaPaulistadeMedicina,UniversidadeFederaldeSãoPaulo(EPM-UNIFESP),SãoPaulo,SP,Brazil
Received11July2014;accepted24December2014 Availableonline11December2015
KEYWORDS Otitismedia; Labyrinthitis; Hearingloss
Abstract
Introduction:Suppurativelabyrinthitiscontinuestoresultinsignificanthearingimpairment, despitescientificeffortstoimprovenotonlyitsdiagnosisbutalsoitstreatment.Thedefinitive diagnosisdependsonimagingoftheinnerear,butitisusuallyclinicallypresumed.
Objective:Toanalyzetheclinicalfactorsandhearingoutcomesinpatientswithlabyrinthitis secondarytomiddleearinfectionsandtodiscussfindingsbasedonimagingtestresults.
Methods:Retrospectivecohortstudy,basedonthechartsofpatientsadmittedwithmiddleear infection-associatedlabyrinthitis.
Results:Weidentified14patients,eight(57%)ofwhomwerefemalesandsix(43%)males.Mean agewas40years.Cholesteatomatouschronicotitismediawasdiagnosedinsixpatients(43%), acutesuppurativeotitismediainsix (43%),andchronicotitis mediawithoutcholesteatoma wasdiagnosedintwopatients(14%).Besideslabyrinthitis,24concomitantcomplicationswere identified:sixcases(25%)oflabyrinthinefistula,fivecases(21%)ofmeningitis,fivecases(21%) offacialparalysis,fivecases(21%) ofmastoiditis,twocases(8%)ofcerebellarabscess,and onecase(4%)oftemporalabscess.Therewasonedeath.Eight(57%)individualsbecamedeaf, whilesix(43%)acquiredmixedhearingloss.
夽
Pleasecitethisarticleas:MaranhãoASdA,GodofredoVR,PenidoNO.Suppurativelabyrinthitisassociatedwithotitismedia:26years’ experience.BrazJOtorhinolaryngol.2016;82:82---7.
夽
Institution:DepartmentofOtorhinolaryngologyandHeadandNeckSurgery,EscolaPaulistadeMedicina,UniversidadeFederaldeSão Paulo(EPM-UNIFESP),SãoPaulo,SP,Brazil.
∗Correspondingauthor.
E-mail:[email protected](A.S.d.A.Maranhão).
http://dx.doi.org/10.1016/j.bjorl.2014.12.012
Conclusion: Suppurativelabyrinthitiswasoftenassociatedwithothercomplications;MRIplayed arole inthedefinitivediagnosisintheacutephase; thehearing sequeloflabyrinthitiswas significant.
© 2015Associac¸ãoBrasileira de Otorrinolaringologiae CirurgiaCérvico-Facial. Publishedby ElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE Otitemédia; Labirintite; Perdaauditiva
Labirintiteassociadaàotitemédia:experiênciade26anos
Resumo
Introduc¸ão: Labirintitepermaneceresultandoemdeficiênciaauditivasignificativa,apesardos esforc¸oscientíficosparamelhorarnãosóodiagnóstico,comotambémotratamento.O diag-nósticodefinitivoédependentedeimagens daorelhainterna,masgeralmenteépresumido clinicamente.
Objetivo: Analisarosfatores clínicos eosresultadosauditivos empacientescomlabirintite secundáriaàotitemédiaediscutirosachadosdosexamesdeimagem.
Método: Estudodecoorteretrospectivo,combasenosprontuáriosdepacientesdiagnosticados comlabirintiteassociadaàinfecc¸ãodaorelhamédia.
Resultados: Foramidentificados14pacientes,oito (57%)dosexo femininoeseis(43%) mas-culino.Médiaetáriade40anos.Otitemédiacrônicacolesteatomatosafoidiagnosticadaem seis pacientes(43%),otite médiaagudaem seispacientes(43%) eotite médiacrônicasem colesteatomaem doispacientes(14%).Foramidentificadas 24complicac¸ões concomitantes: seiscasos(25%) defístulalabiríntica,cincocasos(21%) demeningite,cinco(21%) de paral-isiafacial,cinco(21%)demastoidite,doiscasos(8%)deabscessocerebelareumcaso(4%)de abcessotemporal.Houveumamorte.Oito(57%)indivíduostornaram-seanacústicos,enquanto seis(43%)evoluíramparaperdaauditivamista.
Conclusão:Labirintitefoifrequentementeassociadaaoutrascomplicac¸ões;RNMauxiliouno diagnóstico definitivo dalabirintite nasuafase aguda; a sequela auditivadalabirintite foi significativa.
©2015Associac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.Publicado por ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
The advent of antibiotics and immunizations in the last century ledto a considerable decline in the incidenceof complications from otitis media, and therefore a discus-siononsuppurativelabyrinthitisassociatedwithmiddle-ear infection may seem, at first glance, an outdated issue. However,complicationsstilloccur,particularlyin develop-ing countries,with significant morbidity (notably, hearing loss).1---6Leskinenetal.studied50patientstreatedforotitis mediacomplicationsand,amongtheseveralcomplications listedinthestudy,suppurativelabyrinthitiswasconsidered themostdisabling,inthatallaffectedindividualsdeveloped profoundorcompletehearingloss.2
The diagnosis of suppurative labyrinthitis secondary to otitis media is essentially a clinical one, through the observation of vertigo, nystagmus, tinnitus and hearing impairment in the presence of a middle ear infection. In many diseases of the inner ear,the inflammatory process that ensues is usually presumed, rather than effectively diagnosed, and corticosteroids are empirically prescribed as the treatment of choice.7 The identification of sup-purative labyrinthitis is usually more obvious, due to the magnitudeandseverity,ofthesymptoms,whereasinserous
labyrinthitissymptomsaremoresubtleandmanypatients experiencea satisfactory recovery withthe treatment of underlyingdisordersofthemiddleear.
The complex location of inner ear structures in the temporalbone, housedinthedensebone oftheotic cap-sule, represents a significant barrier for the access and identificationofanyalterationsinthisregion.Considering thatthe current knowledgeabout inner ear physiopathol-ogy is mainly derived from animal studies involving the collection of tissues and histological, molecular and inflammatory marker analyses, little is known about the mechanisms involved in diseases of the human inner ear
invivo.8
Figure1 TemporalbonesCT,axialview.Thearrowshows ero-sionofthelateralsemicircularcanalontheleft,inapatient withCCOM.Note:posteriorerosioninthemastoid,adjacentto thesigmoidsinus.
Theaimofthisresearchistoanalyzeclinicalfactorsand hearingoutcomes of patients withlabyrinthitis secondary tomiddleearinfections anddiscusstheresultsofimaging tests.
Methods
Aretrospectivecohortstudywascarriedoutbasedon medi-calrecordsofpatientstreatedattheOtology/Otoneurology departmentofatertiaryuniversityhospitalbetween1987 and 2013. The study included patients whose medical recordscontainedthe diagnosis of labyrinthitis secondary tootitis media.Medicalrecordswithincomplete informa-tionwereexcluded,aswellasthoseinwhichthediagnosis of suppurative labyrinthitiswasnot well established. The followingdata werecollected frommedicalrecords:age, gender,medicalhistory,typeofmiddleearinfection, asso-ciatedcomplications,audiometryandimagingtestresults. Allpatientsreceivedantibiotictherapyandsystemic corti-costeroids.ThestudywasapprovedbytheEthicsCommittee oftheinstitutionunderProtocolnumber0081/10.
Results
Atotalof14patientsdiagnosedwithlabyrinthitisassociated withotitismediawereidentified.Eightwerefemale(57%) andsix(43%)weremale.Themeanagewas40,withanage rangefrom9to67years(Table1).
All patients had otitis media before the diagnosis of labyrinthitis. Otitis media was classified as follows: cholesteatomatouschronicotitismedia(CCOM)insix(43%) patients,acuteotitismedia(AOM)insix(43%)patients,and non-cholesteatomatouschronicotitismedia(NCCOM)intwo (14%)patients.Thirteen(93%)patientshadoneormoreof thefollowingassociatedcomplications(totalof24recorded complications):labyrinthine fistula (Fig. 1)in six patients (25%,n=24);meningitis,facialparalysisandmastoiditisin fivepatientseach(21%,n=24);cerebellarabscess(Fig.2) intwopatients (8%,n=24), andtemporallobe abscessin onepatient(4%,n=24).Therewasonedeathinthisstudy (case7)(Table2).
Tinnituswas reportedin 14 patients(100%), vertigo in 10patients(71%),andnystagmusinfive(36%).Eight(57%)
Figure2 Brain CTwithcontrast,axialviewandsofttissue window.Itshowsacerebellarabscess ontheleft.Note:soft tissueedema,adjacenttothelefttemporalbone,consistent withmastoiditis.
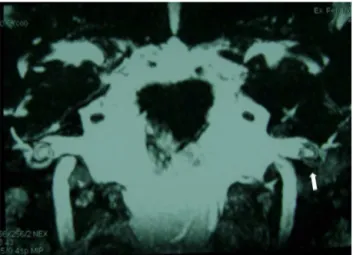
Figure 3 NMR weighted in T1 with gadolinium. Enhance-mentofcontrastintheleftcochlea(arrow)inapatientwith Wegener’sgranulomatosis.Note:enhancedcontrastinthe mid-dleear.Patientwithassociatedmastoiditis.
patients developed anacusis, and six (43%) progressed to mixedhearing loss(moderate tosevere). Innine patients (64%),thediagnosisoflabyrinthitiswasconfirmedwiththe aid of NMR: with contrast (Fig. 3) and with the FIESTA (fastimagingemployingsteadystateacquisition)sequence (Fig.4).ThetemporalboneCTscancorroboratedthe diag-nosisinthreepatients(cases2,3and4)(21%)throughthe observationofcochlearossification(Fig.5).
Discussion
Table1 Descriptionofcases. Case Gender Age Otologic
diagno-sis
Comorbidity Imaging test
Associated complication
Auditoryoutcome
1 F 59 CCOM Diabetesmellitus CT Labyrinthinefistula SevereMHL 2 F 20 NCCOM AIDS CT Meningitis Anacusis 3 M 9 CCOM --- CT
NMR
Labyrinthinefistula Meningitis
Cerebellarabscess
Anacusis
4 M 39 CCOM Chroniceosinophilic pneumonitis
CT --- Anacusis 5 M 43 CCOM --- CT Labyrinthinefistula SevereMHL 6 M 18 CCOM --- CT
NMR
Meningitis
Labyrinthinefistula Temporalabscess
Anacusis
7 F 31 CCOM --- CT Meningitis Facialparalysis Labyrinthinefistula
Anacusis
8 F 17 CCOM --- CT NMR
Meningitis
Labyrinthinefistula Mastoiditis Cerebellarabscess
Anacusis
9 M 31 AOM Wegener’s Granulomatosis
CT NMR
Facialparalysis Mastoiditis
Moderate---severe MHL
10 F 52 AOM Wegener’s Granulomatosis
CT NMR
Facialparalysis Mastoiditis
Moderate---severe MHL
11 F 42 AOM Wegener’s Granulomatosis
CT NMR
Facialparalysis Mastoiditis
Moderate---severe MHL
12 F 64 AOM Diabetesmellitus CT NMR
Facialparalysis ModerateMHL 13 F 41 AOM --- CT
NMR
Facialparalysis Meningitis
Anacusis 14 F 67 AOM Diabetesmellitus CT
NMR
Mastoiditis Anacusis
CCOM,cholesteatomatous chronic otitismedia;NCCOM,non-cholesteatomatous chronicotitismedia; AOM,acuteotitismedia; CT, computedtomography;NMR,nuclearmagneticresonance;AIDS,acquiredimmunodeficiencysyndrome;MHL,mixedhearingloss.
Figure 4 NMR FIESTA sequence, coronal view. The arrow showshypointensesignalinthecochleaandvestibular projec-tion.ThisisthesamepatientshowninFig.3.
Table2 Distributionofcomplications(n=24).
Complication N % Labyrinthinefistula 6 25 Meningitis 5 21 Facialparalysis 5 21 Mastoiditis 5 21 Cerebellarabscess 2 8 Temporalabscess 1 4
The predominant otologic diagnoses were CCOM and AOM; although thesample was small(n=14),similar pat-terns were reported in studies with a larger number of patients.4,5 The majority of patients with CCOM had labyrinthine fistula as an associated complication. It is assumedthatthephysiopathologicalprocessinthesecases occurs through close contact of the infected granulation tissuebelowthecholesteatoma matrixwiththeendosteal membrane and the underlying perilymph,1,3---5 whereas in casesofacuteotitismedia,itisbelievedthattheinfection extendsintothelabyrinththroughavulnerableordehiscent ovalwindowmembrane.2,12
Thereislittledirectevidenceofinflammationoccurring during labyrinthitis, and the knowledge of the inflamma-toryresponsedynamicswithinthehuman innerearis still limited.8 We believe that a better understanding of the inflammatory process and the possibility of defining its course in an affected individual will help to identify the typeand location of the cochlear lesion, resultingin the developmentof customizedtreatmentsaimed atreducing theharmfuleffectsonthedelicatestructuresoftheinner ear,thus changing the current paradigm of administering systemiccorticosteroidstoallcases.
Someanimalstudieshaveinvestigatedthemechanismsof inflammation-inducedinnereardisorders;however,studies in humans are limited. The reasons could be: the intral-abyrinthinefluids andtissues arehoused in the temporal bonecomplexandaredifficulttocollectforculture;acute hearing loss or vertigo arerarely fatal, making inner ear tissues rarely available for autopsies; the temporal bone is not usuallyremoved in routineautopsies, thus limiting histologicalanalysis.1,4
Imagingtestshelptoovercometheseobstaclesand cur-rentlyplayanimportantroleindiagnosis.Fewmedicalareas havebenefitedfromadvancesindiagnosticimagingasmuch asotology.8,9NMRwasperformedin64%ofpatientsinthis studyanditwasadecisivetooltoconfirmthediagnosisand toassesstheextentofdisease.
Previousstudies8---11 haveemphasizedtheimportanceof usinggadoliniuminNMRtodetect innerearinflammatory lesions. They also noted that incipient alterations in the disease process are detectable by nuclear magnetic res-onance imaging. It is believed that the enhancement by contrast results from a disruption of the blood---labyrinth barrier (BLB). The BLB maintains the composition of the innerearfluidsandprotectstheinnerearfromtoxic sub-stancesthroughitsselectivepermeabilitycharacteristic.9,13 Intheradiologicalliterature,threephasesoflabyrinthitis areusuallydescribed:acute,fibrousstage,and labyrinthi-tis ossificans14; it is important to mention that this is a
didactic divisionand that the concomitant occurrence of thephasesispossible.Intheacutephase,thereisintense enhancement of the inner ear structures at T1-weighted NMRimagesafterintravenousgadoliniuminjection(Fig.3). Webelieve itispreciselyat thisstageofthe diseasethat theNMRisessentialforthediagnosis,aslabyrinthitisoften hasunspecificsymptomsanditisnotpossible todiagnose itbyclinicalmeansalone.
CTstudies areof littlehelpin thisphase,aswellasin thefibrousstageoflabyrinthitis.Withthereplacement of intralabyrinthine fluids by fibrous tissue septa, which are characteristicofthefibrousphase,theremaystillbeinner earenhancementbygadolinium,althoughlesspronounced. AttheT2-weightedNMRandintheFIESTAsequence(Fig.4) itispossibletoobservethedecreasedsignalintheinnerear. In turn, at thelabyrinthitis ossificans stage,where debris andboneyspiculesareformed,thetemporalboneCTscan (Fig.5)isthebesttesttoidentifylesionextentandlocation. AttheNMRthereistypicallynocontrastenhancement,and intheFIESTAsequencesandT2,hypointensesignalcanbe observedinthelabyrinthineregion.
We emphasize that all patients (100%) complained of tinnitus and all of them developed some degree of sen-sorineuralhearingloss(withorwithoutanair-bonegap),and 71%complainedofvertigo,usuallycorrelatedwithinfection severity.Inamorecomprehensiveseriesofcases,2profound orcompletehearinglosswasnotedinallcases.Thatseries alsoreportedthatlabyrinthitis-associatedvertigowas com-pensated in all patients. We alsoobserved that after the acuteinfectiousconditionwasover,patientswithvestibular complaintsshowedasatisfactoryrecovery.Alsonoteworthy istheimportanceoftakingintoaccountthetinnitus com-plaint(ubiquitousinthisstudy),whichdespitebeingquite commoninotherotologicdiseasescanindicateanincipient invasionofthecochlearneuroepithelium.
It is pertinent to observe that labyrinthitis occurred in association with other complications in all except one patient(93%);thesecomplications usuallyreceive greater attention due to their more urgent clinical presentation, resulting in a delay in the labyrinthitis diagnosis. When it is finally identified, the hearing loss is already estab-lished.Withthecurrentavailabletreatment,evenifitwere possible to attain an early diagnosis, once the inflamma-tory process starts in the inner ear, it develops into an inevitable cell damage process. Unfortunately, the early diagnosis oflabyrinthitisstilldoes notchange thehearing prognosis, except in cases of immune-mediated diseases, such as Wegener’s granulomatosis, in which it is possible toimprovehearingthresholdswithspecifictreatment.15,16 Concomitant complications have been widely reported in theliterature,3---6whichshouldalertotorhinolaryngologists to the importance of a careful assessment of patients with complications of otitis media, in order to rule out associatedcomplications.
Conclusions
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.MaranhãoASA, AndradeJS,Godofredo VR,MatosRC, Penido NO.Intratemporalcomplicationsofotitismedia.BrazJ Otorhi-nolaryngol.2013;79:141---9.
2.LeskinenK,JeroJ.Acutecomplicationsofotitismediainadults. ClinOtol.2005;30:511---6.
3.DubeySP,LarawinV.Complicationsofchronicsuppurativeotitis mediaandtheirmanagement.Laryngoscope.2007;117:264---7. 4.OsmaU,CureogluS,HosogluS.Thecomplicationsofchronic oti-tismedia:reportof93cases.JLaryngolOtol.2000;114:97---100. 5.KangsanarakJ,FooanantS,RuckphaopuntK,NavacharoenN, TeotrakulS.Extracranialandintracranialcomplicationsof sup-purativeotitis media: reportof 102 cases. JLaryngol Otol. 1993;107:999---1004.
6.PenidoNO,AndreBorinA,IhaL,SuguriVM,OnishiE,Fukuda Y,et al. Intracranial complicationsofotitis media:15years of experience in 33 patients. Otolaryngol Head Neck Surg. 2005;132:37---42.
7.Haynes DS, O’Malley M, Cohen S, Watford K, Labadie RF. Intratympanicdexamethasonefor suddensensorineural hear-ing loss after failure of systemic therapy. Laryngoscope. 2007;117:3---15.
8.Floc’hJL,TanW,TelangRS,SrdjanMV,NuttallA,RooneyWD, etal.MarkersofcochlearinflammationusingMRI.JMagnReson Imaging.2014;39:150---61.
9.Hegarty JL, Patel S, Fischbein N, Jackler RK, Lalwani AK. The value of enhanced magnetic resonance imaging in the evaluationofendocochleardisease. Laryngoscope.2002;112: 8---17.
10.SoneM,MizunoT,NaganawaS,NakashimaT.Imaginganalysis incaseswithinflammation-inducedsensorineuralhearingloss. ActaOto-Laryngol.2009;129:239---43.
11.DubrulleF,KohlerR,VincentC,PuechP,ErnstO.Differential diagnosisandprognosisofT1-weightedpost-gadolinium intral-abyrinthinehyperintensities.EurRadiol.2010;20:2628---36. 12.Paparella MM, Sugiura S. The pathology of suppurative
labyrinthitis.AnnOtol.1967;56:4---86.
13.Juhn SK, Hunter BA, Odland RM. Blood---labyrinth barrier and fluiddynamics of the innerear. IntTinnitus J. 2001;7: 78---83.
14.LemmerlingMM,DeFoerB,VerbistBM,VandeVyverV.Imaging ofinflammatoryandinfectiousdiseasesinthetemporalbone. NeuroimagingClinNAm.2009;19:321---37.
15.Maranhão ASA, Testa JRG, Chen VG, Rossini BA, Penido NO. Mastoiditis and facial paralysis as initial manifesta-tions of Wegener’s granulomatosis. Braz J Otorhinolaryngol. 2012;78:80---6.