revbrashematolhemoter.2015;37(2):132–135
w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Case
Report
Hairy
cell
leukemia
variant:
the
importance
of
differential
diagnosis
Renata
Cristina
Messores
Rudolf-Oliveira,
Mayara
Marin
Pirolli,
Fernanda
Santos
de
Souza,
Juliana
Michels,
Maria
Cláudia
Santos-Silva
∗UniversidadeFederaldeSantaCatarina(UFSC),Florianópolis,SC,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received25August2014 Accepted4October2014 Availableonline11February2015
Introduction
Hairycellleukemiaisararediseasecomprisingabout2%of lymphoidneoplasms.1Thisneoplasmcanbeconfusedwith otherhematologicdiseases.Therefore,adifferentialdiagnosis mustbeperformedbetweenclassichairycellleukemia,hairy cellleukemiavariant,andsplenicmarginalzonelymphoma (SMZL).2AccordingtotheWorldHealthOrganization(2008), hairy cell leukemia variant was classified as a provisional entitybecauseithasclinicalandpathologicalfeaturesthat dif-ferfromclassichairycellleukemia.3Amongtheseaspectsare morphologicalandimmunophenotypicvariationsand resis-tancetoconventionaltreatment.1Furthermore,patientswith hairycellleukemiaare treatedwithnucleosideanalogsbut thesedrugshaveareducedresponseinhairycellleukemia variantandareevenineffectiveinsomecases.3,4An alterna-tiveforthesepatientsistheassociationofnucleosideanalogs withthemonoclonalantibodyrituximab(anti-CD20).5Thus, duetodifferential treatment, the aimofthis study was to reportacaseofhairycellleukemiavariantandcoversome aspectsrelatedtothedifferentialdiagnosisbetweenthe clas-sicandvariantformsofthediseaseandSMZL.Thisstudywas
∗ Correspondingauthorat:DivisãodeAnálisesClínicas,HospitalUniversitárioProfessorPolydoroErnanideSãoThiago,Universidade FederaldeSantaCatarina(UFSC),CampusUniversitário,s/n◦,Trindade,88036-800Florianópolis,SC,Brazil.
E-mailaddress:[email protected](M.C.Santos-Silva).
approvedbytheResearchEthicsCommitteeofthe Universi-dadeFederaldeSantaCatarina(#913/2010).
Case
report
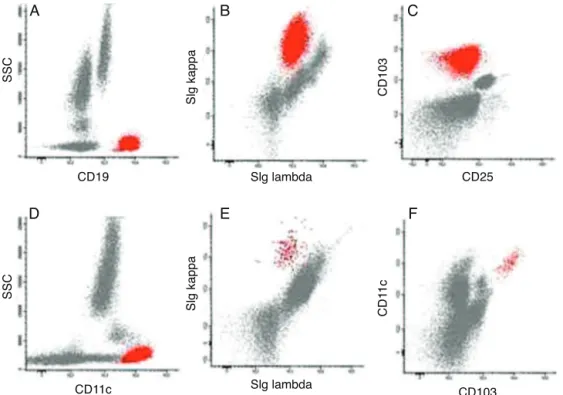
The case of a 74-year-old male patient is reported. The presence of splenomegaly was observed since 2011, with areas of infarction in the splenic periphery evidenced by cholangiography and computed tomography. In 2012, due tothepersistenceofsplenomegaly,acompletebloodcount andimmunophenotypingbyflowcytometrywererequested. At this time, there was no lymphadenopathy. The blood count showed alterations in red blood cells (poikilocyto-sis, acanthocytes and squizocytes), anemia (hemoglobin 10.1g/dL),thrombocytopenia(100×103/mL),andmild leuko-cytosis (11.03×103/mL). A white blood cell differential revealed the following: 2.86×103neutrophils/mL (25.9%), 4.67×103lymphocytes/mL (42.3%), 1.16×103monocytes/mL (10.5%), 1.73×103eosinophils/mL (15.7%), 0.07×103 basophils/mL (0.6%) and 0.55×103lymphocytes/mL (5.0%) withcytoplasmicprojections(Figure1).Immunophenotyping ofperipheralblood(Figure2)showed23.2%ofBlymphocytes
http://dx.doi.org/10.1016/j.bjhh.2015.01.003
revbrashematolhemoter.2015;37(2):132–135
133
Figure1–Small/intermediate-sizedcellswithmoderatepale-graycytoplasm,round/ovalnucleiwithsmoothnuclear
borders,stippledchromatin,occasionalnucleoli,cellshavecircumferentialhair-likeandshort,bluntcytoplasmic
projections.
(CD19+),monoclonal(sIg Kappa+), CD103+, CD11c+, CD20++, CD22+,IgM+/++FMC7++,CD79b++,BCL2+andnoexpressionof sIgLambda,CD3, CD4,CD5, CD8,CD10,CD23,CD24,CD25, CD27,CD38,CD43,andCD123.AssessmentofsIgD,sIgG,and sIgA expression on the pathological lymphocytes was not performed.Thebonemarrowwasnotevaluatedandstaging wasnotperformedduringdiagnosis.Thetreatmentwasfour intravenousdosesofrituximab600mg.Afterthefirstdose, thepatientwasdischargedandtheresponsewasmonitored in the outpatient clinic. At the end of the treatment, the patient returned to the hospital and underwent a bone marrowaspirationforimmunophenotyping,myelogram,and immunohistochemistry. Immunophenotyping showed 1.1% ofBlymphoid cellswithasimilarphenotypetothatfound
atdiagnosis (Figure2).Themyelogram showed hypercellu-larity for the age, normal myeloid:erythroid ratio, as well asnormalityforallothermyelogramparameters. Immuno-histochemistry revealed aggregates of small lymphocytes CD20+ and DBA44−/+ and the result ofTRAP staining was
indeterminate.Currently,thepatientisbeingtreatedinthe outpatientclinicand undergoesperiodiclaboratoryteststo monitorthedisease.
Discussion
Classichairycellleukemia,hairycellleukemiavariant,and SMZL share some common features, including malignant
SSC
SSC
Slg kappa
Slg kappa
CD103
CD1
1c
CD19
A
B
C
D
E
F
CD11c
CD25
CD103 Slg lambda
Slg lambda
Figure2–Representativedotplotsofperipheralbloodimmunophenotyping.(A)Pathologicalcells(red)CD19+atdiagnosis;
(B)pathologicalcells(red)sIgKappa+andsIgLambda−atdiagnosis;(C)pathologicalcells(red)CD103+andCD25−at
diagnosis;(D)pathologicalcells(red)CD11c+atdiagnosis;(E)pathologicalcells(red)sIgKappa+andsIgLambda−inminimal
134
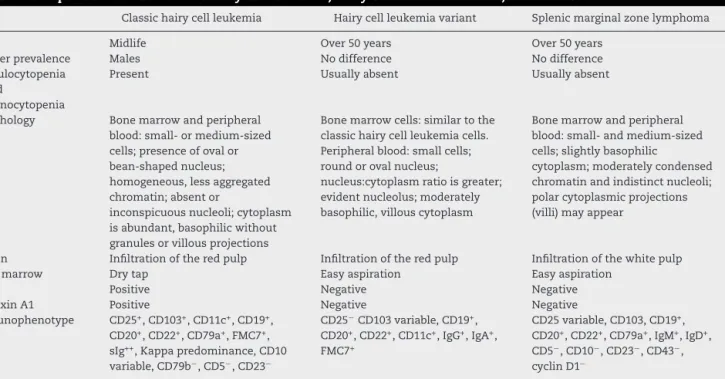
revbrashematolhemoter.2015;37(2):132–135Table1–Comparisonbetweenclassichairycellleukemia,hairycellleukemiavariant,andSMZL.
Classichairycellleukemia Hairycellleukemiavariant Splenicmarginalzonelymphoma
Age Midlife Over50years Over50years
Genderprevalence Males Nodifference Nodifference
Granulocytopenia and
monocytopenia
Present Usuallyabsent Usuallyabsent
Morphology Bonemarrowandperipheral
blood:small-ormedium-sized cells;presenceofovalor bean-shapednucleus; homogeneous,lessaggregated chromatin;absentor
inconspicuousnucleoli;cytoplasm isabundant,basophilicwithout granulesorvillousprojections
Bonemarrowcells:similartothe classichairycellleukemiacells. Peripheralblood:smallcells; roundorovalnucleus;
nucleus:cytoplasmratioisgreater; evidentnucleolus;moderately basophilic,villouscytoplasm
Bonemarrowandperipheral blood:small-andmedium-sized cells;slightlybasophilic
cytoplasm;moderatelycondensed chromatinandindistinctnucleoli; polarcytoplasmicprojections (villi)mayappear
Spleen Infiltrationoftheredpulp Infiltrationoftheredpulp Infiltrationofthewhitepulp
Bonemarrow Drytap Easyaspiration Easyaspiration
TRAP Positive Negative Negative
AnnexinA1 Positive Negative Negative
Immunophenotype CD25+,CD103+,CD11c+,CD19+,
CD20+,CD22+,CD79a+,FMC7+,
sIg++,Kappapredominance,CD10
variable,CD79b−,CD5−,CD23−
CD25−CD103variable,CD19+,
CD20+,CD22+,CD11c+,IgG+,IgA+,
FMC7+
CD25variable,CD103,CD19+,
CD20+,CD22+,CD79a+,IgM+,IgD+,
CD5−,CD10−,CD23−,CD43−, cyclinD1−
lymphocytic infiltration in bone marrow and peripheral blood, splenomegaly, and B lymphocytes with a similar immunophenotype.5 Unlike classichairycell leukemia,the variantformaffectsolderindividuals.1
Anemia and/or thrombocytopenia and leukocytosis are common atdiagnosis ofhairy cell leukemia variant, while pancytopenia, granulocytopenia, and monocytopenia are morecommoninclassichairycellleukemia.Thepatientin this study presented with anemia, thrombocytopenia, and mildleukocytosisduetomonocytosis,eosinophiliaandthe presenceofpathologicallymphocytes.
Immunophenotyping by flow cytometry contributes to differential diagnosis, although it must also be associated withimmunohistochemistryandclinicaldata(Table1). Clas-sic hairy cell leukemia cells are always positive for CD25 andCD103and hairycellleukemia variantcellsarealways negative for CD25 and occasionally positive for CD103. In SMZL,onthe otherhand,CD103isnegativeandCD25may be positive or negative.3,5 Classic hairy cell leukemia and the variant form are also differentiated bythe expression of CD123, which is positive in the classic form and neg-ative in the variant form.6 Evaluation of immunoglobulin heavy chain isotype expression is another way to possi-blydifferentiatehairy cellleukemiavariantfrom SMZL.An unusualfeatureofhairycellleukemiavariant,nottypically observedinotherB-celllymphoproliferativedisorders,isthe expressionofpre-switchedIgM/IgDandpost-switchedIgG/IgA immunoglobulinsbythesamecellsinapproximately40%of cases.Incontrast,SMZLcells characteristicallyexpressIgM withIgDandlackIgGorIgA.7Unfortunatelyinthiscasethe IgG,IgAandIgDimmunoglobulinswerenotavailablefor eval-uation. Thus,the resultsofimmunophenotypicanalysisof peripheralbloodherewereconsistentwithhairycellleukemia variant.
Inimmunohistochemistry,DBA44providesstrongstaining forlymphocyteswithcytoplasmicprojectionsintissues; how-ever,itmayalsobepresentinnormalBcells.3Moreover,cells from hairycellleukemiavariantpatientsrarelyshowTRAP reactivity(unliketheclassicform).1Inthepatientofthisstudy, TRAPstainingremainedindeterminate;hence,itdidnothelp inthediagnosis.Themorphologyandphenotypeconfirmed thediagnosisofhairycellleukemiavariant.
When the patient returned to the hospital of the Uni-versidade Federalde Santa Catarina (HU-UFSC)at the end oftreatment, themyelogramwas hypercellularforhisage, butthisalterationhasnoclinicalrelevancetohiscondition. The presenceof1.1% ofcells with a phenotypesimilar to thatfoundatdiagnosis,asevidencedbyimmunophenotyping ofabonemarrowaspirate, indicatesthepresenceof mini-malresidualdisease(MRD).MRDispresentinmanypatients treatedforhairycellleukemia;however,thesepatientsmay havelong-termsurvival.TreatmentwithRituximabisusedto achievecompleteremission,althoughtheresponseis depend-ent on how much bone marrow is involved and on the characteristicsoftheindividual.8
Conclusion
revbrashematolhemoter.2015;37(2):132–135
135
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.HsiehYC,ChangST,ChuangSS,LuCL,TsaoCJ,LiCN,etal. HairycellleukemiaandvariantinTaiwan:reportofavariant caseandliteraturereview.IntJClinExpPathol.2011;1(4): 183–9.
2.FinoP,FioramontiP,OnestiMG,PassarettiD,ScuderiN.Skin metastasisinpatientwithhairycellleukemia:casereportand reviewofliterature.InVivo.2012;2(26):311–4.
3.SwerdlowSH,CampoE,HarrisNL,JaffeES,PileriSA,SteinH, etal.WHOclassificationoftumoursofhaematopoieticand lymphoidtissues.4thed.Geneva:WHOPress;2008.
4.PalomeraL,DomingoJM,SolaC,AzacetaG,CalvoMT, GutierrezM.Cladribine(2-chlorodeoxyadenosine)therapyin hairycellleukemiavariant.Areportofthreecases.
Haematologica.2002;87(1):107–8.
5.RobakT.Hairy-cellleukemiavariant:recentviewondiagnosis, biologyandtreatment.CancerTreatRev.2011;37(1):
3–10.
6.VenkataramanG,AguharC,KreitmanRJ,YuanCM, Stetler-StevensonM.CharacteristicCD103andCD123 expressionpatterndefineshairycellleukemia:usefulnessof CD123andCD103inthediagnosisofmatureB-cell
lymphoproliferativedisorders.AmJClinPathol. 2011;136(4):625–30.
7.CessnaMH,HartungL,TrippS,PerkinsSL,BahlerDW.Hairy cellleukemiavariant:factorfiction.AmJClinPathol. 2005;123(1):132–8.