w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Original
Article
Laparoscopic
cytoreductive
surgery
for
metastatic
colon
cancer
–
how
to
improve
treatment
strategy
Andrey
Atroshchenko
∗,
Igor
Khatkov,
Stepan
Pozdnyakov,
Mikhail
Danilov
MoscowClinicalScientificCenter,Moscow,Russia
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received2December2016 Accepted15February2017 Availableonline10March2017
Keywords:
Laparoscopicsurgeryforcolorectal cancer
Cytoreductivesurgery Metastaticcolorectalcancer
a
b
s
t
r
a
c
t
Background:Coloncancer(CC)oneofthemostcommononcologicaldiseaseinWorld.Up to30%patientsinRussiahavemetastaticCCatfirstvisitingtooncologist.Thetreatment resultsstillcontroversial.Nowadays,minimallyinvasivelaparoscopicprecisiontechnique allowedextendingtheindicationforcytoreductivesurgeryeveninpatientswithsevere comorbidities.
Materialsandmethods:89patientswithcoloncancer(T1-4a)andcurablesynchronousdistant metastasesincludeinstudy.Allpatientsunderwentcytoreductivesurgerywithprimary tumorresection.Instudy group(44)weperformedlaparoscopicsurgery,inmaingroup (45)–opensurgeryprocedure.Thegroupsweresimilarbysex,age,tumorlocalizationand histologicalstructure,comorbidities.
Results:R0resectionperformed27%patients.Theaveragenumberoflymphnoderemoval wassimilar13and12respectively.Averageoperationtimewassignificantlylongerinstudy group210vs120min.Instudygroupbloodlosswaslower:300mLvs1200mL.Postoperative patientrecoveryshorterafterlaparoscopicsurgery(p<0.05):timetoactivation2.2vs3.9 days;timetofirstperistalsis–1.8vs4.5days;firstbowelmovement–3.4vs4.8days;first foodtaken–2.9vs3.9days.Shortertimeofanalgesicsintake–2.3vs4.4days,p<0.05. Hospitalstayshorter:9.3vs13.4days,p=0.05.Timetostartchemotherapyreducedsince 27.5to14.7days,p<0.05.Postoperativecomplicationslowerinstudygroup:6.8vs17.8%,
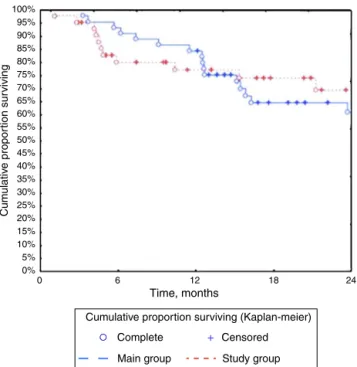
p=0.05.Kaplan–Meier2-yearoverallsurvivalweresimilar:69.5%vs61.6%,p=0.96.
Conclusion:LaparoscopiccytoreductivesurgeryformetastaticCCissafe,minimizedsurgical traumaandspeeduppatientrecovery.
©2017PublishedbyElsevierEditoraLtda.onbehalfofSociedadeBrasileirade Coloproctologia.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
∗ Correspondingauthor.
E-mail:[email protected](A.Atroshchenko). http://dx.doi.org/10.1016/j.jcol.2017.02.003
Cirurgia
laparoscópica
citorredutora
para
câncer
de
cólon
metastático
–
como
melhorar
a
estratégia
de
tratamento
Palavras-chave:
Cirurgialaparoscópicapara câncercolorretal
Cirurgiacitorredutora Câncercolorretalmetastático
r
e
s
u
m
o
Fundamento:Câncerdecólon(CC)éumadasdoenc¸asoncológicasmaiscomunsnomundo. Até30%dos pacientesnaRússiatêmCCmetastáticonaprimeiravisitaaooncologista. Osresultadosdotratamentoaindasãocontroversos.Atualmente,atécnicadeprecisão laparoscópicaminimamenteinvasivapermitiuestenderaindicac¸ãoparaacirurgia citorre-dutoramesmoempacientescomcomorbidadesgraves.
Materiaisemétodos: 89pacientescomcâncerdecólon(T1-4a)emetástasesdistantes sín-cronascuráveisforamincluídosnoestudo.Todosospacientesforamsubmetidosàcirurgia citorredutoracomressecc¸ãodotumorprimário.Nogrupodeestudo(44)realizamoscirurgia laparoscópica,nogrupoprincipal(45),acirurgiaaberta.Osgruposeramsemelhantesem relac¸ãoàsexo,idade,localizac¸ãoeestruturahistológicadotumor,ecomorbidades.
Resultados: Aressecc¸ãoR0foirealizadaem27%dospacientes.Onúmeromédioderemoc¸ão delinfonodosfoisimilar,13e12,respectivamente.Otempomédiodecirurgiafoi signi-ficativamentemaislongonogrupodeestudo,210versus120min.Aperdadesanguefoi menornogrupodeestudo:300mLversus1200mL.Arecuperac¸ãopós-operatóriafoimais curtaapósacirurgialaparoscópica(p<0,05):tempodeativac¸ão-2,2vs.3,9dias;tempoaté oprimeiroperistaltismo-1,8vs.4,5dias;primeiromovimentointestinal-3.4vs.4.8dias; primeiroalimentoconsumido-2.9vs.3.9dias.Menortempodeingestãodeanalgésicos -2,3versus4,4dias,p<0,05;menortempodehospitalizac¸ão:9,3vs.13,4dias,p=0,05.O tempoparainiciaraquimioterapiafoireduzidode27,5para14,7dias,p<0,05.Complicac¸ões pós-operatóriasmenoresnogrupodeestudo:6,8vs.17,8%,p=0,05.Asobrevivênciaglobal deKaplan–Meieraos2anosfoisemelhante:69,5%vs.61,6%,p=0,96.
Conclusão: AcirurgiacitorredutoralaparoscópicaparaCCmetastáticoésegura,minimizao traumacirúrgicoeaceleraarecuperac¸ãodopaciente.
©2017PublicadoporElsevierEditoraLtda.emnomedeSociedadeBrasileirade Coloproctologia.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Background
Coloncancer(CC)oneofthemostcommononcological dis-easeintheWorld.Morethan30,000newcaseswereregistered and12,000havedieannuallyinRussia,upto30%patientshave metastaticCCatfirstvisitingtooncologist.1
InRussiatreatmentofmetastaticCCisinfocusofinterests becausethereisahugepartofpatientswithanadvanced dis-ease.Newtreatmentstrategyandmedicaltechnologyallowed expandingindicationsforsurgeryinpatientswithmetastatic CCevenwithsevercomorbidities.Recentstudiesshowedthe improvementoftreatmentresultsaftercytoreductivesurgery eveninpatientswithmultipleliverandlungmetastases.2–5
Nowadays,introductionofinnovationminimallyinvasive surgery,advantagesinmoleculartechnologyandnewscheme ofchemotherapyallowedextendingtheindicationfor cytore-ductive surgeryformetastatic CC because it could help to optimizetreatment strategy and achieve the improvement of quality of life and long-term results. The laparoscopic precisiontechnique in cytoreductive surgerycould achieve theminimallevelofmorbidityandmortality,shorterperiod ofrehabilitation and time to adjuvant chemotherapy after surgery.6,7
Recently, the results of multiple multicenter random-izedcontrolledtrials(COST,Barcelonatrial,CLASSIC,COLOR,
COLOR-2), confirming thatthereisno differencesin short-term and long-term results between the laparoscopic and openaccesssurgeryforpatientswithCC.8–17
Inmodernliteraturethereisonlysinglearticlesreflecting laparoscopiccytoreductivesurgeryformetastaticCC.
Materials
and
methods
We analysis 89 patients treatment results with CC (T1-4a,Nany,M1a-b).Inclusioncriteriainstudy:coloncarcinoma with curable synchronous distant metastases (except the patientswithtotalperitonealcarcinomatosis);metastasesno more than 2 organs, ECOG<2. Exclusion criteria: ECOG>2, brainandbonemetastases,retroperitoneallymphnodes inva-sion, metastasesmorethan 2organs,tumoror metastases destruction,acutebowel obstruction,multiplesynchronous ormetachronousmetastases.Allpatientsunderwent simul-taneous or staged cytoreductive surgery and adjuvant chemotherapy.Thepatientsweredividedinto2groups:study group (44patients)– underwentlaparoscopic cytoreductive surgery;maingroup–cytoreductivesurgerybyopenaccess(45 patients).Thegroupsweresimilarbysex,age,tumorspread andlocalizationandhistologicalstructure,comorbidities.
68% 2% 11%
5% 5%
9%
68%
2% 13%
9%
9%
7%
Study group, %
Main group, %
Caccum
Right flexure
Descending colon
Ascending colon
Transverse colon
Sigmoid colon
Caccum
Right flexure
Descending colon
Ascending colon
Transverse colon
Sigmoid colon
Fig.1–Tumorlocalizationandmetastasesspread.
Table1–Thenumberandmetastaseslocalization.
Metastaseslocalization Studygroup N(%)
Maingroup N(%)
Liverall 38(86.4) 35(77.8)
Solitarylivermetastases 6(14.6) 5(13.2) Singlelivermetastases 11(26.8) 11(28.9) Multiplelivermetastases 24(58.5) 22(57.9)
Lung 2(4.6) 3(6.7)
Solitarylungmetastases 1(20) 0
Singlemetastasesofthelung 2(40.0) 2(33.3) Multiplelungmetastases 2(40.0) 4(66.7)
Leftlungmetastases 1(20.0) 1(16.7)
Rightlungmetastases 2(40.0) 1(16.7) Bilaterallungmetastases 2(40.0) 4(66.7)
Liverandlung 3(6.8) 3(6.7)
Metastasesinotherorgans 1(2.3) 4(8.8)
M1a–metastases 39(88.6) 38(84.4)
M1b–metastases 5(11.4) 7(15.6)
All patients had histologically verified colon adenocar-cinoma: high gradedifferentiated adenocarcinoma– 10.1% patients,moderate–76.4%,low-grade–6.7%and6,7%patients had mucousadenocarcinoma. Mainpartofthe patients in ourstudyhadmoderate–differentiatedcarcinomawithT3 invasion.
Thelymphnodemetastasesweredetectedin75%patients studygroup,and82.2%–inmaingroup.
Thedistributionofaffectedorgansmetastasesand local-izationispresentedinTable1.
Themainpartofpatientsinbothgrouphadmultiple bilat-erallivermetastasesandmultiplebilaterallungmetastases (Figs.2and3).
Differentsymptomsoftheprimarytumorinthecolonwere observedmorethanin50%ofpatients(Table2).
Almost91%patientsinstudy groupand82%patientsin maingrouphadseverecomorbidities(Table3).
Results
All patients(89)underwent cytoreductive surgerywith pri-mary tumor or primary tumor and distant metastases resection(Table4).
Fig.2–Livermetastases.
Table2–Primarytumorcomplications.
Typeofcomplications Studygroup, N(%)
Maingroup,N (%)
Bowelobstructionsubclinical 14(31.8) 15(33.3)
Bloodinstool 7(15.9) 7(15.6)
Toxicoanemicsyndrome 3(6.8) 5(11.1)
Total 24(54.6) 27(60.0)
Table3–Comorbidities.
Comorbidities Study
group,N
Maingroup, N
Coronaryheartdisease 28 25
ArterialhypertensionoftheIst 31 29
Arrhythmia 2 1
Diabetes 5 4
Obesity(BMI25–39.9) 30 34
Chronicobstructivepulmonarydisease 2 3 Gastrointestinaltractbenigndisease 12 8
Table4–Characteristicofcolonsurgeryprocedure.
Typeofsurgery Study
group,N(%)
Maingroup, N(%)
Righthemicolectomy 9(20.5) 13(28.9)
Lefthemicolectomy 4(9.1) 4(8.9)
Sigmoidresection 24(54.6) 18(40.0)
Rectalresection 3(6.8) 2(4.4)
Hartmanprocedure 4(9.1) 8(17.8)
Total 44(100) 45(100)
Hartmann’sprocedureunderwent4patientsinstudygroup and8patientsinmaingroupbecausehadsubclinicalsights ofbowelobstructionandcolonwallhypertrophy.Colon anas-tomosisformedin90.9%casesinstudygroupand82.2%–in maingroup.
SimultaneousR0resectionperformedincaseswhenthe generalcondition(ECOG0–2;APACHEII–0–14score)ofpatient, numberandlocalizationofmetastasesallowedtodoitwith lowriskofmorbidityandmortality(Table5).
R-0resectionperformed29.6%ofpatientsinstudygroup and24.4%–inmaingroup(Fig.4).
Table5–Characteristicsofsurgeryprocedurefor metastases.
Surgeryformetastases Study group,N(%)
Maingroup, N(%)
SimultaneusR-0resection
Liverresection 1(2.3) 0(0)
Salpingo-oophorectomy 1(2.3) 0(0)
Hysterectomy 0(0) 1(2.2)
Omentumresection 0(0) 1(2.2)
StagedR-0resection
Lungresection 1(2.3) 2(4.4)
Liverresection: 10(22.7) 7(15.6)
Righthemihepatectomy 4(9.1) 2(4.4)
Lefthemihepatectomy 2(4.5) 1(2.2)
Atypicalliverresection 4(9.1%) 4(8.9%)
TotalR-0resection 13(29.6%) 11(24.4%)
Fig.4–Atypicalliverresection.
Theaveragenumberoflymphnoderemovalwassimilarin bothgroups(13and12respectively,p<0.05(Fig.5).
Theaveragetimedurationoftheoperationinstudygroup was210min,inmaingroup–120min.Surgerytimedepends onsurgeonslearningcurve,andhavetendedtodeclineafter 30laparoscopicprocedures.
Inobesepatientsthetimeofsurgerysignificantlylonger especially in laparoscopicaccess group because it so diffi-cult to do the navigation and visualization of anatomical structures:obesityIdegree–234.4min;IIdegreeofobesity– 295min.Incontrolgroup:Idegreeobesity–163.6min;obesity IIdegree–226.7min.
Weanalyzedintraoperativebloodlossasafactorof surgi-caltrauma.Theaveragebloodlossinstudygroupwas300mL, incontrolgroup–1200mL,p<0.05.Thedatashowsthat,the laparoscopicprocedurecouldhelptoreducedoperativeblood losssignificantlyand,consequently,reducedthenumberof transfusioncomplicationsandspeeduppatients rehabilita-tion.
Surgicalcomplicationsweresimilarinbothgroup:5%in laparoscopic accessgroupand 4%– inopen surgerygroup
p>0.60.Themainsurgicalcomplicationwashemorrhage. We studded several indicators during early postopera-tiveperiod:timetoperistalsisrecoveryfirststool,firstfood taken,timetopatientactivation,painkillersintake, postop-erativecomplications,hospitalstay,andtimetostartadjuvant
Left colic artery
Arteria mesenteric inferior
Hypogastric nerve plexus
Right common iliac artery
Table6–Timetobowelmovementrestoration.
Settings Studygroup,(days) Maingroup(days) p
Firstperistalsis 1.8±0.7 4.51±1.5 <0.05
Firststool 3.4±1.3 4.78±1.4 0.05
Table7–Qualityoflifeinearlypostoperativeperiod.
Settings Studygroup,
days(median)
Maingroup, days,(median)
p
Averagetimeto patientactivation
2.2±1.1(2) 3.9±0.9(4) <0.05
Painkillersintake 2.3±1.4(2) 4.4±1.4(4) 0.05 Firstfoodtaken 2.9±0.7(3) 3.9±1.3(4) <0.05
chemotherapy.Allofthisparametershadimprovedinstudy group:timetoperistalsisrestorationwasshorterin2.5times (p<0.05),andadmittedreductiontimeoffirststoolin1.4times (p=0.05)(Table6).
Thequalityoflifeinearlypostoperativeperiodisan impor-tant parameter, which determined bythe first food taken, bowelmovementrestoration,andtimetopainkillersintake. The results also confirm the improvement quality of life inearlypostoperativeperiodinpatientsundergoing laparo-scopicprocedures(Table7).
Precisionlaparoscopictechniqueallowssignificantlyspeed upthepostoperativepatientrehabilitationincomparisonwith opensurgery.
Postoperativecomplicationsinmaingrouphavenotedin8 (17.8%)patients,3patientsofthemwasre-operated.Instudy groupcomplicationswerenotedin3patients(6.8%),2ofthem –re-operated.Theresultsshowedthatthelaparoscopicaccess couldminimizepostoperativecomplications.
Hospital stay afterlaparoscopic surgery were shorter: 9 daysinstudygroupversus13daysinmaingroup(p<0.05).
100% 95% 90% 85% 80% 75% 70% 65% 60% 55% 50% 45% 40% 35% 30% 25% 20% 15% 10% 0% 0 6 Time, months Cum u lativ e propor tion sur viving
12 18 24
5%
Main group Study group Cumulative proportion surviving (Kaplan-meier)
Complete + Censored
Fig.6–Kaplan–Meyer2-yearsurvival.
Thelaparoscopicprecisiontechniquecouldspeeduppatients rehabilitationupto1.5times.
Adjuvant chemotherapy plays a key role in treatment strategy for patients with metastatic CC. Time to start chemotherapyaftersurgery–oneofthemostimportant indi-cator,which oftendependsonpostoperativerehabilitation. The surgicalprocedures and postoperative complications– mainfactorsthatprolongedtimetostartadjuvant chemother-apy. Well known that the early start of chemotherapy after cytoreductive surgery is beneficial to the long-terms outcomes. Short periodof rehabilitation afterlaparoscopic surgery, improving thequality oflife,lower percentagesof postoperativecomplicationsallowedtoreducetimetostart the adjuvantchemotherapy:14.7 days–study group;27.5– maingroup(p<0.05).
Theresultsof2-yearoverall survivalaftercytoreductive surgerybylaparoscopicaccessandopensurgeryare compa-rable(69.5%and61.6%,respectively,p=0.96(Fig.6).
During2yearsfollowupwedidnotregisteredanycasesof localrecurrence.
Conclusion
Theresultsofourstudyshowedthatthelaparoscopic cytore-ductive surgery for patients with metastatic CC is safe, could minimize surgical trauma and speed up postopera-tiverecoveryeveninpatientswithmultiplemetastasesand severe comorbidity. The laparoscopic access indicated for patients withmetastatic coloncancer stageT1-4aNdifferent M1a-b.Contraindicationsforlaparoscopicsurgeryarelocally advancedhugetumorswhichinvadesintotheadjacentorgans aor structures(T4b) and advanced peritoneal carcinomato-sis or adhesions. The introduction of minimally invasive laparoscopictechnologyallowsextendingtheindicationsfor cytoreductivesurgeryeveninpatientswithmetastaticCCand severecomorbidities.
Conflict
of
interest
Theauthorsdeclarenoconflictofinterest.
r
e
f
e
r
e
n
c
e
s
1.AleksandrovVB.Laparoscopictechnologyincolorectal surgery;2003.
2.DavydovMI,AkselEM.Statisticsofmalignantneoplasmsin RussiaandCIScountriesin2007.VestnRONCNNBlokhinaof theRussianAcadMedSci.2009;20:1–158.
3.LutsevichOE,VtorenkoIV,GallyamovEA.Laparoscopyin emergencysurgery:currentstateoftheproblem.Thehealth ofthecapital.VIIMoscowAssembly.SBScientific.Works; 2008.
4.KhatkovIE,TsvirkunVV,AgapovVK,IzrailovRE.Laparoscopic pancreatoduodenectomy.AnnalsSurgHepatol.2008;13:78. 5.BajettaE,FlorianiI,BartolomeoMD,LabiancaR,LandiL,
postoperativetreatmentforradicallyresectedgastriccancer. JClinOncol.2012;30:LBA4001.
6. BangYJ,KimYW,YangHK,ChungHC,ParkYK,LeeKH,etal. Adjuvantcapecitabineandoxaliplatinforgastriccancerafter D2gastrectomy(CLASSIC):aphase3open-label,randomized controlledtrial.Lancet.2012;379:315–21.
7. GouvasN,AgalianosC,PapaparaskevaK.Surgeryalongthe embryologicalplanesforcoloncancer:asystematicreviewof completemesocolicexcision.IntJColorectalDis.
2016;31:1577–94.
8. HohenbergerW,WeberK,MatzelK,PapadopoulosT,MerkelS. Standardizedsurgeryforcoloniccancer:completemesocolic excisionandcentralligation–technicalnotesandoutcome. ColorectalDis.2009;11:354–64,discussion364-5.
9. LeungKL,LeeJFY,YiuRY,SimonSM,JimmyCM.Simultaneus laparoscopicresectionofrectalcancerandlivermetastasis.J LaparoendoscAdvS.2006;16:486–8.
10.LiangJ,FazioV,LaveryI,RemziF,HullT,StrongS,etal. Primacyofsurgeryforcolorectalcancer.BrJSurg. 2015;102:847–52.
11.MarksJH,KawunUB,HamdanW,MarksG.Redefining contraindicationstolaparoscopiccolorectalresectionfor high-riskpatients.SurgEndosc.2008;22:1899–904.
12.MoriS,KitaY,BabaK,YanagiM,TanabeK,UchikadoY,etal. Laparoscopiccompletemesocolicexcisionviacombined medialandcranialapproachesfortransversecoloncancer. SurgToday.2016;47:643–9.
13.MilsomJW,KimSH.Laparoscopicversusopensurgeryfor colorectalcancer.WorldJSurg.1997;27:702–5.
14.MiyamotoY.Laparoscopicresectionofprimarytumorfor stageIVcolorectalcancer.In:19thInternationalCongressof theEAES.2011.A:0133.
15.NgDC,CoCS,CheungHY,ChungCC,LiMK.Theoutcomeof laparoscopiccolorectalresectioninT4cancer.ColorectalDis. 2011;13:e349–52.
16.SoopM,NelsonH.Islaparoscopicresectionappropriatefor colorectaladenocarcinoma?AdvSurg.2008;42:205–17. 17.KuhryE,SchwenkWF,GaupsetR,RomildU,BonjerHJ.