w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Original
Article
Acute
physical
and
psychological
stress
effects
on
visceral
hypersensitivity
in
male
rat:
role
of
central
nucleus
of
the
amygdala
Hamideh
Afzali
a,
Fatemeh
Nabavizadeh
a,∗,
Seyed
Morteza
Karimian
a,
Hamid
Sohanaki
a,
Jalal
Vahedian
b,c,
Seyed
Mehdi
Mohamadi
b,caTehranUniversityofMedicalSciences,SchoolofMedicine,DepartmentofPhysiology,Tehran,Iran
bIranUniversityofMedicalSciences,SchoolofMedicine,DepartmentofPhysiology,Tehran,Iran
cIranUniversityofMedicalSciences,FirouzgarHospital,DepartmentofSurgery,Tehran,Iran
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received19November2016 Accepted21December2016 Availableonline27February2017
Keywords:
Abdominalwithdrawalreflex Amygdala
Physicalstress Psychologicalstress Visceralhypersensitivity
a
b
s
t
r
a
c
t
Objective:Theaimofthisstudywastoinvestigatetheeffectsofacutephysicaland
psycho-logicalstressandtemporarycentralnucleusoftheamygdala(CeA)blockonstress-induced visceralhypersensitivity.
Methods:FortytwomaleWistarratswereusedinthisstudy.Animalsweredividedinto7
groups(n=6);1–Control,2–physicalstress,3–psychologicalstress,4–sham,5–lidocaine, 6–lidocaine+physicalstressand7–lidocaine+psychologicalstress.Stressinductionwas doneusingacommunicationbox.
Results:Abdominalwithdrawalreflex(AWR)scorewasmonitoredonehourafterstress
expo-sure.AWRscoresignificantlyheightenedat20,40and60mmHginthepsychologicalstress groupcomparedwithcontrol(p<0.05),while,itwasalmostunchangedinothergroups.This scorewasstrikinglydecreasedat20,40and60mmHginlidocaine+psychologicalstress groupcomparedwithpsychologicalstresswithnotangibleresponseonphysicalstress. Totalstoolweightwassignificantlyincreasedinpsychologicalstressgroupcomparedwith control(0.72±0.15,0.1±0.06g)(p<0.05),butitdidnotchangeinphysicalstresscompared tocontrolgroup(0.16±0.12,0.1±0.06g)(p<0.05).Concomitantuseoflidocainewithstress followedthesameresultsinpsychologicalgroups(0.18±0.2,0.72±0.15g)(p<0.05),whileit didnothaveanyeffectonphysicalstressgroup(0.25±0.1,0.16±0.12g)(p<0.05).
Conclusions:Psychologicalstresscouldstronglyaffectvisceralhypersensitivity.Thiseffectis
statisticallycomparablewithphysicalstress.TemporaryCeAblockcouldalsoreducevisceral hypersensitivitypost-acutepsychologicalstress.
©2017PublishedbyElsevierEditoraLtda.onbehalfofSociedadeBrasileirade Coloproctologia.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
∗ Correspondingauthor.
E-mail:[email protected](F.Nabavizadeh). http://dx.doi.org/10.1016/j.jcol.2016.12.006
Efeitos
agudos
do
estresse
físico
e
psicológico
na
hipersensibilidade
visceral
em
rato
macho:
papel
do
núcleo
central
da
amídala
Palavras-chave:
Reflexoderetiradaabdominal Amídala
Estressefísico Estressepsicológico Hipersensibilidadevisceral
r
e
s
u
m
e
n
Objetivo: Oobjetivodesseestudofoiinvestigarosefeitosdoestressefísicoepsicológico
agudoebloqueio temporáriodonúcleocentral daamídala(CeA)nahipersensibilidade visceralinduzidaporestresse.
Métodos: QuarentaedoisratosWistarmachosforamempregadosnesseestudo.Osanimais
foramdivididosem7grupos(n=6):1–Controle,2–estressefísico,3–estressepsicológico,4 –simulacro,5–lidocaína,6–lidocaína+estressefísicoe7–lidocaína+estressepsicológico. Ainduc¸ãodoestressefoifeitacomousodeumacaixadecomunicac¸ão.
Resultados: Oescore doreflexode retiradaabdominal(RRA) foimonitoradouma hora
depoisda exposic¸ãoaoestresse.OescoreRRAaumentousignificativamentea20,40 e 60mmHgnogrupodeestressepsicológicoversuscontrole(p<0,05),enquantoque prati-camentepermaneceuinalteradonosdemaisgrupos.Esseescorediminuiudrasticamente a20,40e60mmHgnogrupodelidocaína+estressepsicológicoversusestressepsicológico, semrespostatangívelnoestressefísico.Opesototaldasfezesaumentousignificativamente nogrupodeestressepsicológicoversuscontrole(0,72±0,15,0,1±0,06g)(p<0,05),masnão houvemudanc¸anogrupodeestressefísicoversuscontrole(0,16±0,12,0,1±0,06g)(p<0,05). Ousosimultâneodalidocaínacomoestresseacompanhouosmesmosresultadosnos gru-pospsicológicos(0,18±0,2,0,72±0,15g)(p<0,05),enquantoquenãofoiobservadoqualquer efeitonogrupodeestressefísico(0,25±0,1,0,16±0,12g)(p<0,05).
Conclusões:Oestressepsicológicopodeafetarfortementeahipersensibilidadevisceral.Esse
efeitoéestatisticamentecomparávelcomoestressefísico.UmbloqueiotemporáriodoCeA tambémpodereduzirahipersensibilidadevisceralpós-estressepsicológicoagudo.
©2017PublicadoporElsevierEditoraLtda.ennombredeSociedadeBrasileirade Coloproctologia.Esteesunart´ıculoOpenAccessbajolalicenciaCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Visceralhypersensitivityisnowacommonhypothesisused toexplainthepainfulsymptomsinpatientssufferingfrom irritable bowel syndrome (IBS). IBSis aprevalent gastroin-testinaldisordercharacterizedbyabdominalpainandbowel habitchangeswithunexploredetiology.1 Almost22%ofthe populationexperiencesIBSsymptoms.2Difficultyin diagno-sisandinadequategoodtreatmenttogetherwithhighsocial andmedicalcostschangedIBSintoasocialconcern.3,4
Psychologicalandphysicalstressorshavebeenidentified asimportantfactors inIBSpathophysiology.5,6 Researchers havefoundarelationshipbetweencentralpathwaysofstress andanxietyandperipheralmechanismsmodulating gastroin-testinalsensitivity.Amygdala,especiallythecentralnucleus ofamygdala(CeA),whichhasapivotalroleonthis relation-ship;mainlyaffectsendocrineandautonomicreplytostress andcausesvisceralhypersensitivity.7Visceral hypersensitiv-ityiscommonlyexaminedviadifferentformsamongwhich communicationboxseemstobeanagreeabletoolfor con-comitantstudyofphysiologicalandbehavioralchangesunder psychologicalandphysicalstresses.8
However,tothebestofourknowledge,thisisthefirststudy whichfocusesonratvisceralhypersensitivitypostinduction inthecommunicationboxenvironment.Therefore,theaim ofthecurrentstudywastoinvestigatetheroleofCeAblock invisceralhypersensitivityresponsepostcommunicationbox inducedphysicalandpsychologicalstressmodelinmalerats.
Materials
and
methods
Animals
FortytwomaleWistarrats(250–325g)purchasedfrom phys-iologydepartmentofTehran UniversityofMedicalSciences (TUMS).Animalswerekeptunderstandardconditionsof 12-h:12-hlight/darkcyclewithunlimitedaccesstothestandard rat chowand water.All experimentswereperformed upon TUMSethicalcommitteeapprovalbetween8amupto3pm everyday.
Experimentalprotocol
Experimentswereperformedonsevenequallyassigned ani-malgroups(n=6)asperthefollowingclassification:
1. Control; animals placed in stress box 15min without receivingelectricfootshock.
2. Physicalstress;animalsplacedinstressboxandreceived 5selectricalshock(2mA),then55srestfor15min. 3. Psychologicalstress;animalsplacedinthesafe
compart-mentsfor15minwithout receivingfoot shockand then receivedvisual,auditoryandolfactorysensationcuesfrom theneighboringanimal,
(CeA)5minbeforeplacingintothestressboxfollowedby thesameprocedureasgroup1.
5. Lidocaine; animals received bilateral microinjections of lidocaine(0.5–1l,2%).intoCeA
6. Physical stress+lidocaine; animals received bilateral microinjectionsoflidocaineintoCeA5minbeforeplacing intothestressboxfollowedbythesameprocedureasgroup 2.
7. Psychologicalstress+lidocaine;animalsreceivedbilateral microinjectionsoflidocaineintoCeA5minbeforeplacing intothestressboxfollowedbythesameprocedureasgroup 3.
Stereotaxicsurgery
Animals anesthetized first with a mixture of ketamine (50mg/kg,ip)andxylazine(5mg/kg,ip)andplacedina stereo-taxicapparatus.Theskullwasclean shaved andamidline incisionmade.Connectivetissueswerethenremovedtohave thebestaccesstolambdabregmalandmarks.Twoholeswere madewithamicrodrillovertheskullaccordingtoratbrain anatomicalatlas(paxinos)coordinates(2.5mm posteriorto thebregma,4.4mmbilateraltomidlineand8mmfromthe top.Two23-gaugestainlesssteelguidecannulaswere bilater-allylowereduntiltheirtipsstood2mmaboveCeAandfixedto theskullsurfacewithdentalcement.Cannulasiteswere con-firmedviamethylenebluecolorinjectionandtissuesection studies.Uponcompletion,animalsbackedtotheircagesfora weekrecoverybeforehandlingstressaccommodation.9 Nor-malsaline(0.5–1l)andlidocaine(0.5–1l,2%)10,11delicately injectedwithaHamiltonsyringeconnectedtoa30-gauge can-nulaextended2mmbelowtheguidecannulatip.Lidocaine actedastemporaryblockerofbothneuronsandtractsinthe amygdalaregion.11Injectionsweremadeover1mintoallow maximaldiffusion.Thecannulawasalsoslowlywithdrawn duringthesametimeperiod.9
Body temperature kept at 37◦C with a homoeothermic
heatingpad.
Stressboxandelectricalshockdevice
Communicationboxapparatuswasdesignedforstress stimu-lusapplication.Theapparatusconsistsofninecompartments of 50cm×16cm×16cm, separated by transparent plastic walls.Toapplypsychologicalstress,eachratisindividually placedinto one compartmentand isolated from others by transparentwallswithnophysicalcontact,butfreetoreceive visual,auditoryandolfactorysensationcuesfromthe neigh-boringrat.Thefloorofeachcompartmentwascoveredwith metalgridsmadeupof5mmdiameter stainlesssteelrods placed1.3cmapartconnectedtoanelectricshockgenerator (currentof2mA)(BorjSanatCo.,Iran,sensitivity0.1–10mA) toapplyfootshockwith5sdurationand55sinterval.12Four compartmentsgridswereinsulatedwithplasticrollstoserve asshock-freecompartmentsforpsychologicalstressgroup.13
Totalstoolweightmeasurement
Eachratbackedtoanindividualcageimmediatelyafterstress exposurefor30minwithfreeaccesstostandardchowand
water. Feces were collected,weighed and reported astotal stoolweight.12
Behavioraltests
Visceral hypersensitivity wasmonitored1hourafterstress exposure using visual observation of animal response to graded colorectal distention (CRD), as previously described.14,15 Animals inhaled diethyl ether inhalation underaglassbellforalightanesthesia.A5cmballoonmade upofsurgicalglovefingerattachedtoatygontube,inserted into theanalcanalandadvanced8cmintothedescending colonandfixedtotheanimaltailwithanadhesivetape.The tubeendattachedtoasphygmomanometerviaaY-connector. Rats were then recovered from anesthesia and allowedto adaptforabout30min.CRDwascarriedoutthroughrapidly inflatingtheballoontodifferentpressureamountincluding 20,40,60and80mmHgfora20sfollowedby2minrest. Behav-ioralresponsestoCRDweremonitoredbyanobserverblindto theexperimentandrecordedasabdominalwithdrawalreflex (AWR) score as follows: 0, no behavioral response; 1, brief headmovement followedbyimmobilestatus;2,abdominal musclecontraction;3,abdominalwalllifting;4,bodyarching andpelvicstructureslifting.
Determinationofplasmacorticosteronelevel
Atthe end ofthe experiments, animalswere anesthetized withdiethylether.Bloodsampleswerecollectedbycardiac punctureandkeptinEDTAcoatedtubesforfurtherplasma separation.Samplesstoredat−70◦Ctillmorningassay.
Cor-ticosteroneELISAkit(DRG,Germany)wasusedtodetermine corticosteronelevel.
Histology
Attheendoftheexperiment,injectionsiteswereevaluatedfor accuracywithmethylenebluemicroinjections(0.25L/each side). Animals were then decapitated under diethyl ether inhalation.Brainswereremovedandfixedinformalin(10%) solution. Coronal sections (50m)were also prepared and examinedforCeAinjectionsite.16
Statisticalanalysis
Data represented as mean±SEM. Statistical analysis was performed by SPSS software, version 19.0. Nonparametric FriedmantestusedtoassesAWRscoresatrespective pres-sures withineachgroup. AveragedAWRscore ateach CRD pressurewerecomparedamonggroupsusingKruskal–Wallis one-wayanalysisofvariance.Hormonelevelsandtotalstools weight were compared with analysis of variance (ANOVA) followedbyTukeyposthoctest.p<0.05wasconsideredas sig-nificantstatisticallevel.
Results
4
3
2 ∗
∗
∗
#
#
#
1
0
20 mmHg 40 mmHg 60 mmHg 80 mmHg
Control Ph Control Control Control
y
Phy Phy Phy
Psy Psy Psy Psy
Sham Lid Sham Lid Sham Lid Sham Lid
Lid + Ph y
Lid + Psy Lid + PsyLid + Psy Lid + PsyLid + Psy Lid + PsyLid + Psy
A
WR score
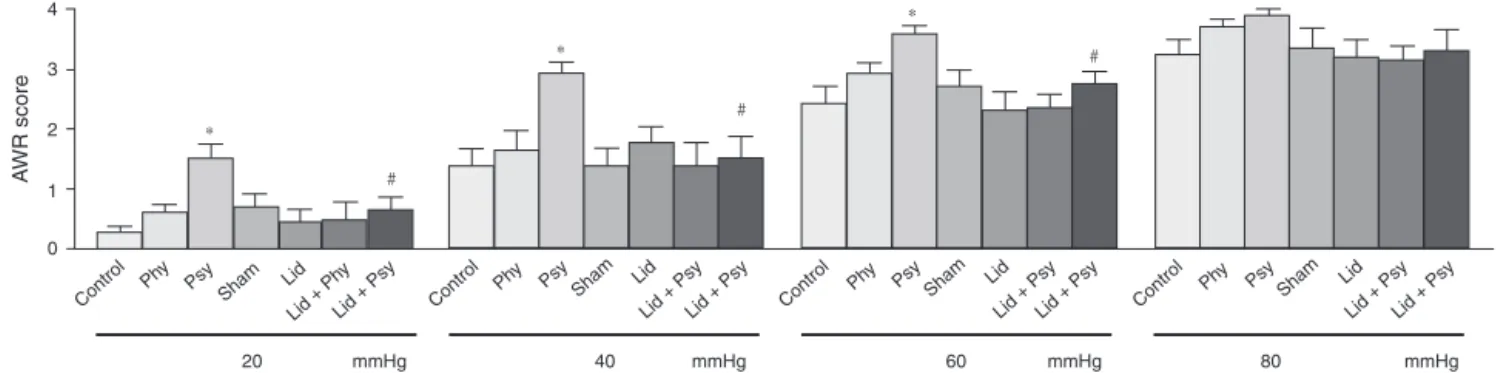
Fig.1–Effectofacutephysicalandpsychologicalstressesandtemporarycentralnucleusofamygdala(CeA)blockon withdrawalreflex(AWR)scores.Control,physical(phy),psychological(psy),sham,lidocain(lid),lidocain+physical (lid+phy),lidocain+psychological(lid+psy)stresses.*p<0.05comparisonofpsystressgroupwithcontroland#p<0.05
lid+psywithpsy.
AWRscoressignificantlyincreasedat20,40and60mmHgin psychologicalstressgroupcomparedwithcontrol(p<0.05). AWRscores in other groups were slightly increasedat 20, 40,60and80mmHgcomparedwithcontrol(p>0.05).These scoreswere significantlydecreased at20,40and 60mmHg inlidocaine+psychologicalstressgroupcomparedwiththe psychologicalstress group. Nosignificant differences were observedbetweenAWRscoresoflidocaine+physicalstress comparedwithphysicalstressgroup.
Total stool weight post stress exposure in psychologi-calstressgroupwassignificantlyhigherthancontrolgroup (0.72±0.15, 0.1±0.06g), but it did not statistically change in physical stress compared to control group (0.16±0.12, 0.1±0.06g) (Fig. 2). Rats in psychological+lidocaine stress
2000
Cor
ticosterone (ng/ml)
1500
$ ∗
∗
#
1000
500
Groups
0
Control Phy Psy Sh am Lid
Lid + ph y
Lid + psy
Fig.2–Effectofacutephysicalandpsychologicalstresses andtemporarycentralnucleusofamygdala(CeA)blockon totalstoolweightpoststressexposureduring30min. Control,physical(phy),psychological(psy),sham,lidocain (lid),lidocain+physical(lid+phy),lidocain+psychological (lid+psy)stresses(Mean±SE,n=6).*p<0.05comparisonof
psystressgroupswithcontroland#p<0.0505comparison
ofpsy+lidstresswithpsystressgroup.
groupshowedasignificantdecreaseintotalstoolweight com-paredwithpsychologicalstressgroup(0.18±0.2,0.72±0.15g). No significant difference wasobserved between totalstool weightsinlidocaine+physicalgroupcomparedwithphysical one(0.25±0.1,0.16±0.12g)(Fig.2).
The effect of acute physical and psychological stresses and temporary CeA block on plasma corticosterone level were shown in (Fig. 3). Significant differences were seen in plasma corticosterone levels of control, physical and psychological stress groups (1258.17±11.9, 1723.50±5.7, 1700.50±5.5ng/ml)(p<0.05).Plasmacorticosteronelevel sig-nificantly decreased in lidocainegroup comparedwith the shamanimals(1235.50±8.6,1622±1.6ng/ml)(p<0.05).
1.0
∗
# 0.8
0.6
0.4
0.2
0.0
Groups
To
tal w
eight of stools (g)
Control Ph y
Psy
Sham Lid
Lid + ph y
Lid + psy
Fig.3–Effectofacutephysicalandpsychologicalstresses andtemporarycentralnucleusofamygdala(CeA)blockon plasmacorticosteronelevel.Control,physical(phy), psychological(psy),sham,lidocain(lid),lidocain+physical (lid+phy),lidocain+psychological(lid+psy)stresses (Mean±SE,n=6).*p<0.05comparisonofphyandpsy
stressgroupswithControl,$lidwithshamp<0.05and
Plasma corticosterone level was significantly decreased inlidocaine+physicalgroup comparedwithphysicalgroup (1132.33±13.6, 1723.50±5.7ng/ml), whereas no significant changeswere observedbetweencorticosterone levelofthe lidocaine+psychologicalgroupcomparedwithpsychological group(1391.67±9.9,1700.50±5.5ng/ml)(Fig.3).
Discussion
In the present study, we investigated the acute physical andpsychologicalstresseffectsonvisceralhypersensitivity togetherwithtemporaryCeAblockresponsetostress-induced visceral hypersensitivity in male rat. One clinical study reportedwhenIBSpatientfacedwithacutestress,decreased significantlyrectalthresholdperceptionandpain,Asaresult ofincreasedvisceralsensitivityinthesepatients.17
Ourresultsshowedthatacutepsychologicalstresscould significantlyincreaseabdominalcontractionresponsestoCRD especiallyat20,40,and60mmHg.Thisisincongruentwith otherprecedingstudiesshowingincreasedvisceralsensitivity post-acutephysicalandpsychologicalstresses.17–19
Some studies have shown limbic system involvement includingamygdalainresponsetovisceralstimulation,20–22 alsothetechniquesthatexaminedbrainactivityhaveshown that inpatients with IBS activity oflimbic regions includ-ing the amygdala increased in response to rectosigmoid Stimulation.22,23
Amygdalaisacentralintegratorforemotion,nociception, emotionalpainbehavior,andemotionalevaluationofsensory stimuliandisvitalforfearandanxietysenses.20,24
Itconsistsofmanynucleiandreceivesversatile informa-tionfromdifferentsomatosensory,olfactory,auditory,visual, gustatoryandvisceralsenses.Thelateralnucleus(LA)isits maininputoftheamygdalawhilethecentralnucleus(CeA) actsastheoutput.CeAprojectsmainlytocortical, hypotha-lamic,andbrainstemregions.25Inthisstudywetemporary blockedtheoutputtracksandassessedstress-inducedcolonic hypersensitivityaftertemporaryCeAblock,especiallyatlower pressures.Inaddition, we notedthat temporaryCeA block could decreasevisceral hypersensitivity clearlyamong ani-malsexposedtopsychologicalstress.
Sever stress is outcomes life car and predis-pose to diseases such as IBS. Stress first activates hypothalamic–pituitary–adrenal (HPA) axis. This causes hypothalamiccorticotropin releasinghormone(CRH) secre-tionatthenextstepandfinallypituitaryadrenocorticotropin (ACTH)secretionandcorticosteronerelease.26
In this study, plasma corticosterone level was signifi-cantlyincreasedinphysicalandpsychologicalstressgroups incomparisontocontrol.Theseresultsareincongruentwith previousstudiesindicatingincreasedlevelofplasma corticos-teroneasthemostimportantsignsofphysical&psychological stress.27,28
StimulationofCeAhasbeenshowntoeasetheHPAaxis activation,29,30 while its lesions could block the axis and plasmacorticosteronesecretion.31
Inthis study increasedplasmacorticosterone levelpost physicalstresswasblockedbybilateralCeAlidocaine microin-jections,butitwasunaffectedpostpsychologicalstress.This
notablefindingmayraisetheprobabilitythatanalternative modulatorypathwayexceptthatCeAisinvolved.Sucha path-waymayrelateeithertoanothercentralintegrationcenter ortoshiftedperipheralresponsesofvisceralstimuli. Expres-sion of different subtypes of CRH receptors with versatile regulatoryresponseingutfunctionsmayalsoexplaindiverse responsepostpsychologicalstressapplication.Somestudies haveshown expressionoftwoCRH receptorsubtypeswith quiteoppositegutfunctionspostmaternalseparation.32
Studieshavedepictedthatautonomicimbalanceincluding lowvagaltoneandincreasedsympatheticactivitymayalso changevisceralsensitivity.33Ourdatashowedthatthe auto-nomicsystemmaybemorecontributedinvisceralperception toluminaldistensionthantheHPAaxissincecolonic hyper-sensitivitydecreasedaftertemporaryCeAblock,butincreased plasmacorticosteronelevelwasunaffected.
In the present study,wealso assessedthe acute physi-calandpsychologicalstresseffectsontotalstoolweightand foundasignificantincreasepostpsychologicalstress appli-cation. This finding is in agreement with previous results showing that both stressors could enhance colonic motor activityanddefecation.12,34However,totalstoolweightwas not significantly increased in animals exposed tophysical stress.
PreviousstudiesstatedthatmajorCeAoutputtosolitary tractnucleusandneuronsindorsalmotornucleusofthevagus regulates colonicmotility.35,36 Weobserved that temporary CeAblockcould significantlydecreasetotal stoolweightin ratsexposedtopsychologicalstress.
Inconclusion,thepresentstudyshowedtheeffectsofacute physical and psychological stress together with temporary CeAblockonvisceralhypersensitivity,plasmacorticosterone leveland,totalstoolweightinstudiedrats.Wealsodepicted thatpsychologicalstressismuchmoreeffectivethan physi-calstressonvisceralhypersensitivityandtotalstoolweight, whereasbothstresstypeshavesimilareffectsonplasma cor-ticosteronelevel.
Temporary CeA block could decrease plasma corticos-teronelevelinacutephysicalstress,withnoeffectonplasma corticosteronelevelinacutepsychologicalstress.
Visceral sensitivity and defecation clearly reduced after temporaryCeAblockinacutepsychologicalstressespecially atlowerpressuresbutremainedunchangedinacutephysical stress.
Visceral hypersensitivity iscommoninIBSpatients and stressisoneofthefactorsreinforcingvisceralsensitivity.In conclusion,visceralhypersensitivityisaninterestingtopicfor researchersandatargetforthediscoveryofanoveldrugfor thetreatmentofIBS.37
Ourfindingshighlightedtheimportanceofpsychological stressonvisceralhypersensitivityandmayhelpin evaluat-ingthepatientssufferingfromIBSunderpsychologicalstress ordesigningtherapeuticalmodalitieswithmoreemphasison theautonomicdysregulation.
Conflicts
of
interest
Acknowledgment
ThisresearchwassupportedbyTehranUniversityofMedical Sciences.
r
e
f
e
r
e
n
c
e
s
1. KeszthelyiD,TroostFJ,MascleeAA.Irritablebowelsyndrome: methods,mechanisms,andpathophysiology.Methodsto assessvisceralhypersensitivityinirritablebowelsyndrome. AmJPhysiolGastrointestLiverPhysiol.2012;303:G141–54. 2. FassovJ,LundbyL,WorsøeJ,BuntzenS,LaurbergS,KroghK.
Arandomised,controlledstudyofsmallintestinalmotilityin patientstreatedwithsacralnervestimulationforirritable bowelsyndrome.BMCGastroenterol.2014;14:1.
3. JungH-K,KimYH,ParkJY,JangBH,ParkS-Y,NamM-H,etal. Estimatingtheburdenofirritablebowelsyndrome:analysis ofanationwidekoreandatabase.JNeurogastroenterolMotil. 2014;20:242–52.
4. RicciJ-F,JhingranP,McLaughlinT,CarterEG.Costsofcarefor irritablebowelsyndromeinmanagedcare.JCOM–WaynePA. 2000;7:23–34.
5. MayerEA,NaliboffBD,ChangL,CoutinhoSVV.Stressand irritablebowelsyndrome.AmJPhysiolGastrointestLiver Physiol.2001;280:G519–24.
6. QinH-Y,ChengC-W,TangX-D,BianZ-X.Impactof psychologicalstressonirritablebowelsyndrome.WorldJ Gastroenterol.2014;20:14126–31.
7. MyersB,Greenwood-VanMeerveldB.Roleofanxietyinthe pathophysiologyofirritablebowelsyndrome:importanceof theamygdala.FrontNeurosci.2009;3:47.
8. EndoY,YamauchiK,FuetaY,IrieM.Changesofbody temperatureandplasmacorticosteronelevelinratsduring psychologicalstressinducedbythecommunicationbox.Med SciMonit.2001;7:1161–5.
9. RashvandM,KhajavaiA,ParvizM,HasaneinP,KeshavarzM. GABAAreceptorsareinvolvedintheanalgesiceffectsof morphinemicroinjectedintothecentralnucleusofthe amygdala.ClinExpPharmacolPhysiol.2014;41:338–44. 10.AhnS,PhillipsAG.Modulationbycentralandbasolateral
amygdalarnucleiofdopaminergiccorrelatesoffeedingto satietyintheratnucleusaccumbensandmedialprefrontal cortex.JNeurosci.2002;22:10958–65.
11.CarriveP,LeeJ,SuA.Lidocaineblockadeofamygdalaoutput infear-conditionedratsreducesFosexpressioninthe ventrolateralperiaqueductalgray.Neuroscience. 2000;95:1071–80.
12.HirataT,FunatsuT,KetoY,AkuzawaS,SasamataM,Miyata K.Inhibitoryeffectsoframosetron,apotentandselective 5-HT3-receptorantagonist,onconditionedfear
stress-inducedabnormaldefecationandnormaldefecation inrats:comparativestudieswithantidiarrhealand spasmolyticagents.JPharmacolSci.2008;106:264–70. 13.FatemehN,MohammadV,HedayatS,SoheilaA,EhsanS.
Physicalandpsychologicalstresshavesimilareffectson gastricacidandpepsinsecretionsinrat.JStressPhysiol Biochem.2011:7164–74.
14.Al-ChaerED,KawasakiM,PasrichaPJ.Anewmodelofchronic visceralhypersensitivityinadultratsinducedbycolon irritationduringpostnataldevelopment.Gastroenterology. 2000;119:1276–85.
15.GuoX,ChenJ,LuY,WuL,WengZ,YangL,etal.
ElectroacupunctureatHe-MupointsreducesP2X4receptor expressioninvisceralhypersensitivity.NeuralRegenRes. 2013;8:2069–77.
16.PaxinosG,WatsonC.Theratbraininstereotaxiccoordinates. SanDiego,CA:Academic;1986.
17.MurrayCD,FlynnJ,RatcliffeL,JacynaMR,KammMA, EmmanuelAV.Effectofacutephysicalandpsychological stressongutautonomicinnervationinirritablebowel syndrome.Gastroenterology.2004;127:1695–703.
18.BradesiS,EutameneH,Garcia-VillarR,FioramontiJ,BuenoL. Acuteandchronicstressdifferentlyaffectvisceralsensitivity torectaldistensioninfemalerats.NeurogastroenterolMotil. 2002;14:75–82.
19.SunY,LiuFL,SongGQ,QianW,HouXH.Effectsofacuteand chronicrestraintstressonvisceralsensitivityand
neuroendocrinehormonesinrats.ChinJDigDis. 2006;7:149–55.
20.DavisM.Neurobiologyoffearresponses:theroleofthe amygdala.JNeuropsychiatryClinNeurosci.1997;9:382–402. 21.FeliceVD,GibneySM,GosselinRD,DinanTG,O’MahonySM,
CryanJF.Differentialactivationoftheprefrontalcortexand amygdalafollowingpsychologicalstressandcolorectal distensioninthematernallyseparatedrat.Neuroscience. 2014;267:252–62.
22.NaliboffBD,DerbyshireSW,MunakataJ,BermanS,
MandelkernM,ChangL,etal.Cerebralactivationinpatients withirritablebowelsyndromeandcontrolsubjectsduring rectosigmoidstimulation.PsychosomMed.2001;63:365–75. 23.Wilder-SmithC,SchindlerD,LovbladK,RedmondS,Nirkko
A.Brainfunctionalmagneticresonanceimagingofrectal painandactivationofendogenousinhibitorymechanismsin irritablebowelsyndromepatientsubgroupsandhealthy controls.Gut.2004;53:1595–601.
24.StrobelC,HuntS,SullivanR,SunJ,SahP.Emotional
regulationofpain:theroleofnoradrenalineintheamygdala. SciChinaLifeSci.2014;57:384–90.
25.NeugebauerV,LiW,BirdGC,HanJS.Theamygdalaand persistentpain.Neurosci:RevJNeurobiolNeurolPsychiatry Neurosci.2004;10:221–34.
26.SmithSM,ValeWW.Theroleofthe
hypothalamic–pituitary–adrenalaxisinneuroendocrine responsestostress.DialoguesClinNeurosci.2006;8: 383–95.
27.ChrousosGP,GoldPW.Theconceptsofstressandstress systemdisorders.Overviewofphysicalandbehavioral homeostasis.JAMA.1992;267:1244–52.
28.JafariM,SalehiM,ZardoozH,RostamkhaniF.Responseof liverantioxidantdefensesystemtoacuteandchronic physicalandpsychologicalstressesinmalerats.EXCLIJ. 2014;13:161–71.
29.MaS,MorilakDA.Norepinephrinereleaseinmedial amygdalafacilitatesactivationofthe
hypothalamic–pituitary–adrenalaxisinresponsetoacute immobilisationstress.JNeuroendocrinol.2005;17:22–8. 30.RedgateES,FahringerEE.Acomparisonofthepituitary
adrenalactivityelicitedbyelectricalstimulationofpreoptic, amygdaloidandhypothalamicsitesintheratbrain. Neuroendocrinology.1973;12:334–43.
31.FeldmanS,ConfortiN,ItzikA,WeidenfeldJ.Differentialeffect ofamygdaloidlesionsonCRF-41,ACTHandcorticosterone responsesfollowingneuralstimuli.BrainRes.1994;658:21–6. 32.O’MalleyD,DinanTG,CryanJF.Alterationsincolonic
corticotropin-releasingfactorreceptorsinthematernally separatedratmodelofirritablebowelsyndrome:differential effectsofacutepsychologicalandphysicalstressors. Peptides.2010;31:662–70.
33.TougasG.Theautonomicnervoussysteminfunctionalbowel disorders.CanJGastroenterol.1999;13Suppl.A:15A–7A. 34.RaoSS,HatfieldRA,SulsJM,ChamberlainMJ.Psychological
35.LyubashinaOA.Possiblemechanismsofinvolvementofthe amygdaloidcomplexinthecontrolofgastricmotorfunction. NeurosciBehavPhysiol.2004;34:379–88.
36.VenkovaK,JohnsonAC,MyersB,Greenwood-VanMeerveldB. Exposureoftheamygdalatoelevatedlevelsofcorticosterone
alterscolonicmotilityinresponsetoacutepsychological stress.Neuropharmacology.2010;58:1161–7.
37.KanazawaM,HongoM,FukudoS.Visceralhypersensitivityin irritablebowelsyndrome.JGastroenterolHepatol.