w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Original
Article
Mechanical
technology
effect
in
the
treatment
of
anorectocele
using
transanal
repair
of
rectocele
and
full
rectal
mucosectomy
with
one
circular
stapler
procedure
Carlos
Sardi ˜nas
a,∗,
Dilia
Díaz
Arreaza
b,
Héctor
Osorio
caHospitalUniversitariodeCaracas,UnidaddeColoproctología,LaboratoriodeFisiologíaAnorrectal,Caracas,Venezuela
bUniversidadCentraldeVenezuela,InstitutoAnatomopatológico“Dr.JoséAntonioO’Daly”,Caracas,Venezuela cInstitutoVenezolanodeInvestigacionesCientíficas(IVIC),Caracas,Venezuela
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received25September2016
Accepted21December2016
Availableonline2February2017
Keywords:
Treatment Anorectocele TRREMS Staplers Comparison
a
b
s
t
r
a
c
t
Objective:Transanalrepairofrectoceleandfullrectalmucosectomywithonecircularstapler
isaproceduredesignedforthetreatmentofObstructiveDefecationSyndromebydoctorFco.
SergioRegadasin2005.Wecomparetheuseofmultipleinstrumentsandtheirmechanical
technologyeffectinthetreatmentofanorectocele.
Patientsandmethods:Femalepatientscomplainingaboutsensationofincomplete
evacua-tion,agesbetween40and55.Theevaluationwasmadewiththefunctionofevacuation
protocol: colonic transit time, colon radiology, ecodefecography, anorectal manometry
andpsychological test.The technique used was transanal repairof rectoceleand full
rectalmucosectomywithonecircularstapler,usingstaplersCPH-34,CPH-34HVand
EEA-3135-HEM,withmeasurementoftherectalwallresected:verticallengthincentimetres,
horizontallengthincentimetres,weightingramsandvolumeincubiccentimetres;
after-wardshistologicalstudyofthetissuethickness,andappliedtheANOVAandSPSS12tests
forthestatisticalanalysis.
Results:TheresultsobtainedbycomparingtheresectionsmadewiththeCPH-34,the
CPH-34HVandtheEEA-3135-HEMinrespectofverticallength,horizontallength,weightand
volume,werefoundtohavenosignificantdifferences;neitherinthehistologicalstudyof
thetissuethicknessinrespectofcharacteristicsandstructure.
Conclusion:The effectof mechanicaltechnology in thetreatment of anorectocele with
transanalrepairofrectoceleandfullrectalmucosectomywithonecircularstapler
proce-dureusingtheCPH-34,theCPH-34HVandtheEEA-3135-HEM,doesnotshowanydifference.
Leavingtheapplicationofeachtotheoperatorcompetencies.
©2017SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.This
isanopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/
licenses/by-nc-nd/4.0/).
∗ Correspondingauthor.
E-mail:carloseduardosardinas@gmail.com(C.Sardi ˜nas).
http://dx.doi.org/10.1016/j.jcol.2016.12.003
2237-9363/©2017SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.ThisisanopenaccessarticleundertheCC
Efeito
mecânico
da
tecnologia
no
tratamento
da
anorretocele
com
o
uso
do
procedimento
TRREMS
Palavras-chave:
Tratamento Anorretocele TRREMS Grampos Comparac¸ão
r
e
s
u
m
o
Objetivo: TRREMS(TransanalRepairofRectoceleandfullrectalMucosectomywithonecircular Stapler,Reparotransanalderetoceleemucosectomiaretaltotalcomumgrampocircular)
éumprocedimentoquevisaotratamentodaSíndromedaDefecac¸ãoObstrutivapeloDr.
FranciscoSergioRegadasem2005.Comparamosousodediversosinstrumentoseoefeito
mecânicodatecnologianotratamentodaanorretocele.
Pacientesemétodos: Pacientesdogênerofemininocomqueixadesensac¸ãodeevacuac¸ão
incompleta(SEI),comidadesentre40e55anos.Aavaliac¸ãofoiefetuadacomoprotocolo
defunc¸ãodeevacuac¸ão:tempodetrânsitocolônico,radiologiadocólon,ecodefecografia,
manometriaanorretaletestepsicológico.AtécnicaempregadafoiTRREMS,comousode
grampeadoresCPH-34,CPH-34HVeEEA-3135-HEM,commedic¸ãodaparederetalressecada:
comprimentoverticalemcentímetros,comprimentohorizontalemcentímetros,pesoem
gramas evolumeemcentímetroscúbicos; subsequentemente,foirealizadoestudo
his-tológicodaespessuradotecido,comaplicac¸ãodeANOVAedoprogramaSPSS12paraa
análiseestatística.
Resultados: Observamosqueosresultadosobtidoscomacomparac¸ãodasressecc¸ões
real-izadas comCPH-34, CPH-34HVe EEA-3135-HEMcomrelac¸ão aocomprimento vertical,
comprimentohorizontal,pesoevolume,bemcomoosresultadosdoestudohistológicoda
espessuradotecidocomrelac¸ãoàscaracterísticaseestrutura,nãoapresentavamdiferenc¸as
significativas.
©2017SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda.Este
´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/
licenses/by-nc-nd/4.0/).
Introduction
Anatomicalstructuresareaconjunctionofrelations,between
eachother,ofanorganpartsfromhumanbody.The
distri-butionandorderoforganpartsprovidethesupportstructure
thathelpstotransmitalltheefforts andloads resultingof
theirexistenceanduse.
Describingtheanatomicalstructuresthatcontributeinthe
regulatorymechanismsofcontinenceanddefecationcanbe
donebyexplainingthatthesigmoidcolonhasapropulsive
function,therectumactsasacontaineroffaecalmaterialand
theanusisanorgan withflowresistanceand,atthesame
time,sensoryanddiscriminativecapacities.
Thestaggeredarrangementofthethreeorgansthatplay
relatedfunctionsistypicalofourbody.Thearrangementofthe
terminalbowelelementsensuresthecontinence,periodical
andvoluntary,alsoselective,withtheabilitytodiscriminate
solid,liquid andgaseous contents.So, the analcontinence
dependsonabarriereffect,whichdevelopsintheanorectal
andanaljunction.Intheanus,thisbarriereffectisproduced
bythecombinationofforcesthatareduetotheanatomical
configurationofthepelvicfloorandthemuscleaction;this
complexmechanismisactivatedinresponsetosensory
infor-mationobtainedfromthiszone.
Thepelvicfloorandanalcanalstructuresformananatomic
regiontraditionallypoorlyknown.Thereareresearchpapers,
inthelastyears,inwhichnewmorphostructuralapproaches
oftheanalsphinctermechanismaredumped.In2006Regadas
et al.,1 showed discrepancies inthe definition of the anal
canal,aswellasnewdataintheirextensionandstructural
elements,whattheycallanorectoceleandwhatprovides
mod-ifications to the anatomic, the surgical and the functional
canal,consideringtheideaofanorectocelebeingpartofthe
morphostructuralandfunctionalalterations.
Thedifficultyofdefiningaconceptisgenerallyin
propor-tiontothenumberofvariablesthatcaninfluenceit.Inthe
caseofobstructivedefecationsyndrome(ODS),whichcould
arisefromtheanorectocele,itisespeciallydifficultbecauseof
theimpossibilityofallcomponentsinvolvedintheabsence
of an effective defecation clumping. Therefore we believe
thatthefactorsinvolvedindefecationcouldbedividedinto
three types: structuralfactors, muscle factors and sensory
factors.
On the basis of considering that the anorectocele is a
morphostructural alterationthat comprisestheevacuation,
thesurgicalcorrectionwouldbethesolutiontothe
difficul-ties.Therearealotofpapersthatprovideevidences,where
thesurgicalcorrectionoftherectovaginalseptumalterations
significantlyimprovesthe patientswithobstructive
defeca-tion syndrome (ODS),but it takes multipletechniques and
mechanicaltechnologiestocutandstapletheaffectedtissues,
andthereistheproposalofLealandRegadasin2010,2thatto
optimizethesurgicaltechniquestaplersshouldbemodified
orusingjustone.
Thepurposeofthispaperwastousethetechniquecreated
byRegadasin2004,3knownasTransanalRepairofRectocele
andRectalMucosectomywithoneCircularStapler(TRREMS)
tocomparetheeffectofvariousmechanicaltechnologiesfor
Patients
and
methods
Inthisexperimentalstudywereincluded21femalepatients
withincompleteevacuationsensation,agesbetween40and
55.Thepatients wereevaluated withtheEvacuation
Func-tionProtocolusedintheColoproctologyUnitofI.A.Hospital
Universitario de Caracas,4 inwhich studies were practiced
topatients as:colonic transittime, colonradiology,
ecode-fecography, anorectal manometry and psychological test.5
This allowed to determine the presence of an obstructive
defecationsyndrome(ODS)relatedtothepresenceof
anorec-tocele.Theexperimenterintroducedascontrolthreefemale
groupswithODSandanorectocele,theassignmentwas
ran-dom.ThetechniqueusedfortheirtreatmentwasTRREMS,3
inwhichthesurgeoncoloproctologystappliedalternating
sta-plers,CPH-34,CPH-34HV(FrankenmanInternationalLtd.)and
EEA-3135-HEM(CovideanUSA).Thehypothesisisthatstaplers
havedifferentcapacitiesofresectionastheyareappliedfor
theanorectoceletreatmentinTRREMS.Theeffectof
mechan-icaltechnologyisevaluatedwithsubsequentmeasurementof
therectalwallresection.Thesampleswherefixedwith
forma-lin10%andplacedonacorktopreventdeformation.During
themacroscopicstudy wereobtainedthehorizontallength
incentimetres,theverticallengthincentimetres,theweight
ingramsandthevolumeincubiccentimetres,makingcuts
ofthewall.Theywereprocessedwithroutinetechniquesto
obtainthehistologicalslidesstainedwithhematoxylin–eosin.
They were analyzedwithan OlympusCX31 microscope to
determinethe thicknessin millimetresof each rectal wall
layer. After two moths exploring the patients reports we
verifytheirclinicalimprovementanddegreeofsatisfaction.
Was employed for the statistical analysis the ANOVA and
SPSS21.
Table1–Horizontallengthdescriptivestatistics.
Groups N Minimum Maximum Average D.T.
CPH34 7 8 9.7 9.243 0.588 CPH34HV 7 6 11.5 8.786 1.729 EEAHEM3335 7 8 10 8.714 0.756
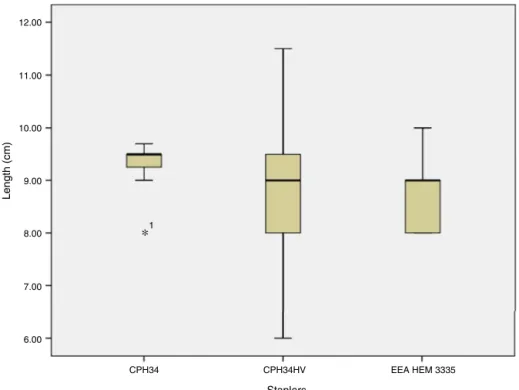
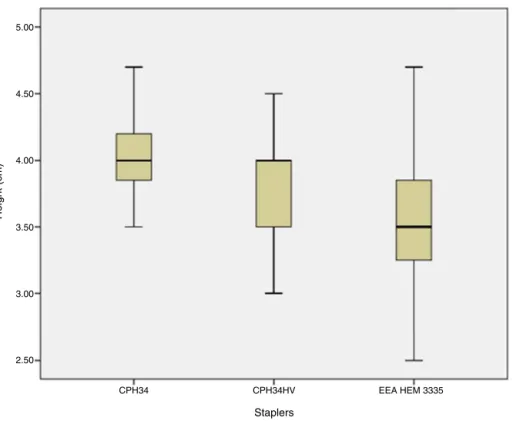
Table2–Verticallengthdescriptivestatistics(cm).
Groups Total Minimum Maximum Average D.T.
CPH34 7 3.5 4.7 4.04 0.4
CPH34HV 7 3 4.5 3.79 0.4 EEAHEM3335 7 2.5 4.7 3.56 0.8
Results
Horizontallength(cm)
By comparing the staplers CPH-34, CPH-34HV
(Franken-man InternationalLtd.) and EEA-3135-HEM(Covidean USA) with the resected tissue horizontal length in centimetres, the resultsdidnotshow statisticallysignificant differences (F2,18=0.442;p>0.05)(Table1andFig.1).
Verticallengthorheight(cm)
By comparingthestaplers CPH-34,CPH-34HV (Frankenman
International Ltd.) andEEA-3135-HEM (Covidean USA)with
the resectedtissueverticallengthorheightincentimetres,
the resultsdidnotshow statisticallysignificant differences
(F2,18=1.408;p>0.05)(Table2andFig.2).
12.00
11.00
10.00
9.00
8.00
7.00
6.00
CPH34 1
∗
CPH34HV EEA HEM 3335
Staplers
Length (cm)
5.00
4.50
4.00
3.50
3.00
2.50
CPH34 CPH34HV
Staplers
Height (cm)
EEA HEM 3335
Fig.2–Horizontallengthorheightdescriptivestatistics.
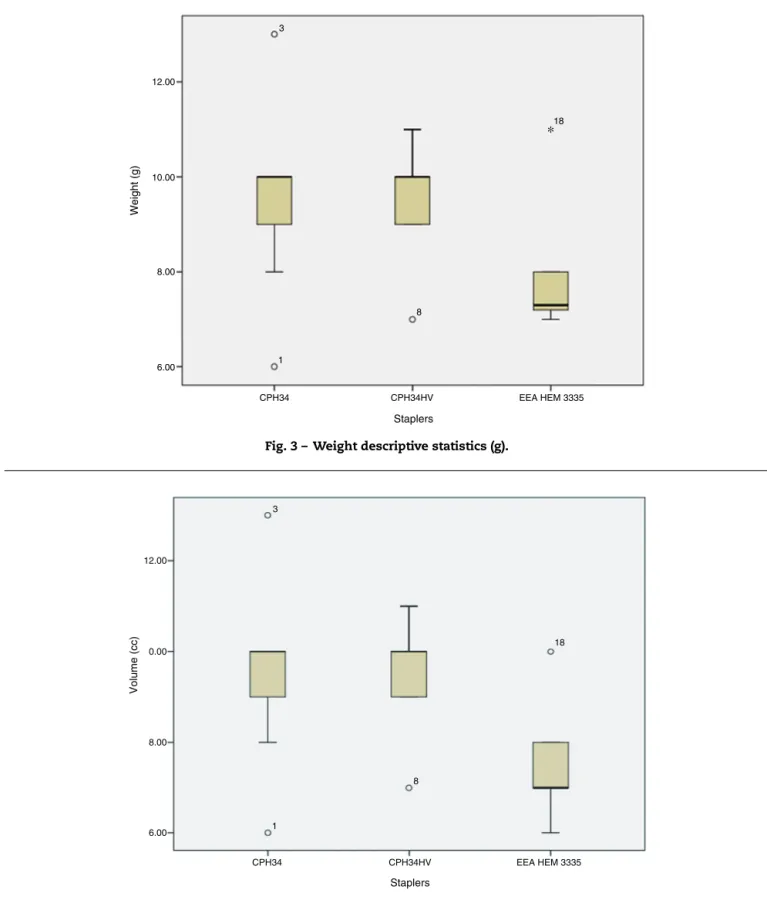
Table3–Weightdescriptivestatistics(g).
Groups Total Minimum Maximum Average D.T.
CPH34 7 6 13 9.57 2.3
CPH34HV 7 7 11 9.43 1.5
EEAHEM3335 7 7 11 7.96 1.5
Weight(g)
Bycomparingthe staplersCPH-34,CPH-34HV (Frankenman
International Ltd.)and EEA-3135-HEM(Covidean USA) with the resected tissue weight in grams, the results did not showstatisticallysignificantdifferences(F2,18=2.046;p>0.05) (Table3andFig.3).
Volume(cc)
Bycomparingthe staplersCPH-34,CPH-34HV (Frankenman
International Ltd.)and EEA-3135-HEM(Covidean USA) with
theresectedtissuevolumeincubiccentimetres,theresults
didnotshowstatisticallysignificantdifferences(F2,18=3.327;
p>0.05)(Table4andFig.4).
Table4–Volumedescriptivestatistics(cc).
Groups Total Minimum Maximum Average D.T.
CPH34 7 6 13 9.57 2.34
CPH34HV 7 7 11 9.43 1.51
EEAHEM3335 7 6 10 7.57 1.37
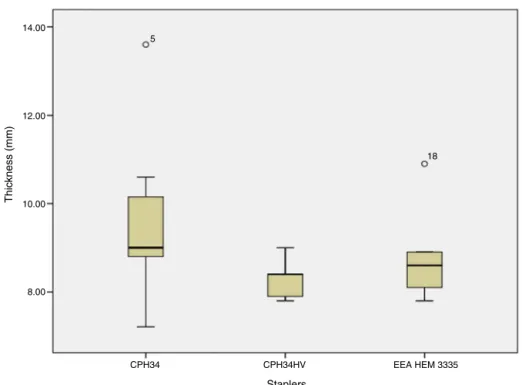
Table5–Thicknessdescriptivestatistics(mm).
Groups Total Minimum Maximum Average D.T.
CPH34 7 7.2 13.6 9.67 2.2 CPH34HV 7 7.8 9 8.26 0.5 EEAHEM3335 7 7.8 10.9 8.76 1.1
Thickness(mm)
By comparingthestaplers CPH-34,CPH-34HV (Frankenman
International Ltd.)and EEA-3135-HEM (Covidean USA)with theresectedtissuethicknessinmillimetres,theresultsdidnot showstatisticallysignificantdifferences(F2,18=2.031;p>0.05) (Table5andFig.5).
Explorationofpatientsreport
The improvement levels two months after the treatment
where marked in eleven patients and complete in seven
patients.
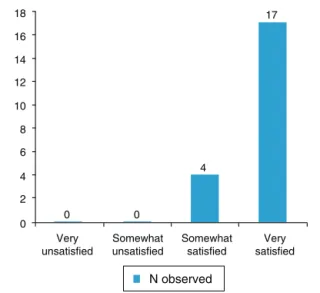
Thesatisfaction degreetwomonthsafterthe treatment
wassomewhatsatisfiedinfourpatientsandverysatisfiedin
seventeenpatients.
Discussion
Boccasantaestablishedin2004,6thatithasbeenintroduced,
since1998,thecircularstaplersfortransanalhaemorrhoids
ormucosalprolapsestreatment,openinganewhorizonfor
theobstructiveevacuationtreatment.Boccasantaproposesto
12.00
3
18
∗
8
1 10.00
8.00
6.00
CPH34 CPH34HV EEA HEM 3335
Staplers
Weight (g)
Fig.3–Weightdescriptivestatistics(g).
12.00
0.00
8.00
6.00 1
8
18 3
CPH34 CPH34HV
Staplers
Volume (cc)
EEA HEM 3335
Fig.4–Volumedescriptivestatistics(cc).
withvaginalorperineallevartoplasty,Delorme’stransrectal
excision,laparotomy olaparoscopy withresections or
rec-topexybytwoprocedureswithtransanalstapled(STAPL)and
perineallevartoplastywithdoubletransanalstapledforrectal
resection(STARR),theycouldbeeffectivealternativesto
con-ventionalsurgeriesintheobstructiveevacuationtreatment.
Inboth,STAPLandSTARR,wasemployedthePPH-01(Ethicon
endosurgery USA), making reference to the mechanical
technologyeffect,obtainingthathistologicalexaminationof
resectedtissuesfoundrectalsmoothmusclefibresin64%of
thegroups,withoutanyotherfindings,causingdoubtsin26%
Fig.5–Thicknessdescriptivestatistics(mm).
Boccasantapublishedinaugust20047asecondpaperwith
STARRintheobstructiveevacuationtreatment.Usingthe
PPH-01 (Ethicon endosurgery USA), in this opportunity offering
dataaboutthemechanicaltechnologyeffectofstapled,
deter-miningananteriorsegmentoftissuewithanhorizontallength
of6.2±1.6cmandawidthof5.7±1.2cm. Fortheposterior
segment ahorizontallengthof4.8±1.4cm and awidth of
4.8±1.4cm. Hereportsthe findingofsmoothmusclefibres
in100%ofthepatients.Thusthefirstvaluesofthetechnology
effectsintissuesare set.Weobtainedvaluesforhorizontal
lengthfrom6to11.5cmasshowninTable1andFig.1,
verti-callengthorheightfrom2.5to4.7cmasshowninTable2and
Fig.2.Howeverthereisnosignificantevidencecomparingthe
staplersCPH-34,CPH-34HV(FrankenmanInternationalLtd.)
andEEA-3135-HEM(CovideanUSA).
InNovember2004, Regadas3 publishedanewtechnique
fortherectoceletreatment,usingatransanalstapler,labelling
it“transanalrepairofrectoceleandfullrectalmucosectomy
withonecircularstapler”(TRREMS),beingconsideredbythe
authorasanewtechniqueinthe existingspectrumofthe
alreadyknown.FortheTRREMSexecutionineightpatients
they used two types of staplers, the EEA-34-stapler (Tyco
healthcare USA) n seven patients and the PPH-03 33mm
(EthiconendosurgeryUSA)inone.Themechanicaltechnology
effectresultsarepublished,reportingonemucosalbandwith
athicknessof5.2cm, averagefrom4.5to6.5cm,
neverthe-lesstheydonotdiscriminatebetweenstaplersintheresults.
Thehistologicevaluationreportsfindingrectalsmooth
mus-clefibresineverypatient.IntheresultsdiscussionRegadas
emphasizestheneedforstapledsuturebeinglocatedbetween
the normalanterior wallof therectus and the anal canal,
0.5cmabovethepectinealline.Thiswaytheanorectovaginal
septumwillberesectedandreinforced,andwillbepromoted
thescarringofhealthytissue.Kleemanin20058publisheda
reviewandupgradeofrectocelesandanatomyofthe
vagi-nalposteriorwall,wheretheycouldgetthestructureofthe
multiplelayersandestablishedthatthethicknessin
anorec-tocelescouldreach16.6mm.InFig.6couldbeappreciatethe
width reachedbythestaplers CPH-34,CPH-34HV
(Franken-manInternationalLtd.)andEEA-3135-HEM(Covidean USA),
fromderectalmucosauntiltheadventicia,thethickness
val-uesrangefrom7.2to13.6mm,withoutsignificantdifferences
comparingthestaplersasshowninTable5andFig.5.
In 2005, Regadas9 published a multicentre experience,
whereitispresentedthe evaluationoftheuseofnew
rec-tal mucosectomy equipmentwith stapled.In this occasion
thestaplerusedisthecircularEEA-34-mm(Tycohealthcare
USA).Themechanicaltechnologyeffectswherethecleavage
ofa4.7cm mucosalband withoutanyhistologicalstudyof
the samples. Inthis paper theycomment the existenceof
twodifferenttypesofstaplers,asthePPH-01andthePPH-03
(EthiconendosurgeryUSA)andthecircularEEA-34-mm(Tyco
healthcareUSA),theyhavebeenusedforthemucosalband
resections;linkingthemucosalprolapse,nottothetechnical
principlesofthesurgicalprocedure,butthestaplersbeinguse
untilthen.Regadasconsidersthattheidealresection,because
ofthesizeandshapeprovidedbystaplers,shouldbea5cm
widemucosalband,butthemechanicaltechnologycapacity
justallowsanaverageof4.5cmwide, supportinghisclaim
intheLatin-Americanmulticentreworkin2003,headedby
Habr-Gama10wheretheypublishedthefirstexperiencesofthe
stapledhaemorrhoidectomy.Themucosalbands,astermed
byRegadas,didnotexceed4.7cmasshown inTable2and
Fig.2.Regardlessofthestaplerusedforthetechnique.
In2008,Lehur11publishedamulticentrepaperwherethey
applySTARRfortheobstructiveevacuationtreatment,using
PPH-01(EthiconendosurgeryUSA),reportingthedoughnuts
resection,understoodascircumferentialtissue,thesewhere
subjectedtohistologicalstudies.Theydonotreport
dimen-sionsorhistologicalcharacteristicsofthedoughnuts,sothat
there is no evidence ofthe mechanical technology effect,
reportedbyotherauthorswiththeuseofthePPH-01(Ethicon
endosurgeryUSA),whichcouldmeanthattheresection
pro-portions would notberelevantinthe technologiceffectof
stapled.Itseemstobedemonstratedbyresultsnotshowing
anystatisticallysignificantdifferencesintablesandfigures.
Renzi,12in2008,publishedamulticentrestudywherewas
usedanewstaplerforthe STARRintheobstructive
evacu-ationtreatment.ThisstapleristheCCS-30contourtranstar
(EthiconendosurgeryUSA),reportingthemechanical
14.00
5
18 12.00
10.00
8.00
CPH34 CPH34HV EEA HEM 3335
Staplers
Thic
kness (mm)
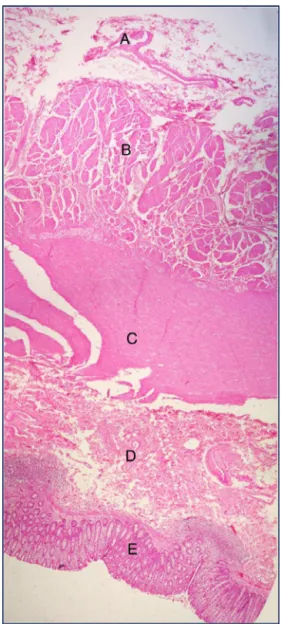
Fig.6–Anorectocelehorizontalsection.Hematoxilineosinstained.Resectedtissueshowsrectalwallcomponents. Adventicia(A),outermusclelayer(B),innermusclelayer(C),submucosa(D)andrectalmucosa(E).
and10.1±2.2cmlong,therebeingnoreportofthetissue
his-tologicanalysis.Oneimportantelementofthepaperisthe
comment where is compared the CCS-30contour transtar
(Ethicon endosurgeryUSA) withthe PPH-01(Ethicon
endo-surgeryUSA).IsaffirmedthatthemajorcapacityoftheCCS-30
contourtranstar(EthiconendosurgeryUSA)istheresection
ofa greater tissuevolume. Thisparameter, the volume, is
referred for the first time inthe literature reviewed,so is
addedanewdimensiontothemechanicaltechnologyeffect,
thathasbeendescribedintheresectedsamplesaswidthand
lengthofthemucosa,andatthismomentwasconsideredof
5cm.However,Renzidoesnotreportvaluesofthe
mechan-icaltechnologyeffectwiththeexceptionthatthisisgreater
thanthepreviousobtainedwithothertechnologies.Table4
andFig.4allowtodemonstratevolumesvaryingbetween6
and13cm3,butagainnosignificantdifferencesbetween
sta-plersCPH-34,CPH-34HV(FrankenmanInternationalLtd.)and
EEA-3135-HEM(CovideanUSA).
Lenisa13in2008,publishedamulticentreprospectivepaper
of the results applying STARR technique with the stapler
CCS-30contourtranstar (Ethiconendosurgery USA)forthe
obstructive evacuation treatment. Itestablishes the
limita-tionsthatthePPH-01(EthiconendosurgeryUSA)hasforthe
rectalwallresection,aswellasbeingablindprocedureafter
the insertionofthe transanalstapler. Oneofthe new
ele-ments that Lenisa introduces in the study is the resected
tissueweightvalue,asameasureofthemechanical
technol-ogyeffect,besidesoftheheightandthehistologicevaluation,
alreadyestablishedbyotherauthors,tryingtoshowthe
thick-nessoftherectalwallthathasbeenresected,aswellasthe
presenceorabsenceofperitoneum.Theresultsobtainedin
the evaluationofthe specimenswere an averagewidth of
8.1cmandalengthof4.8cm,anaverageweightof30g.Itwas
alsoestablishedthetotalresectionoftherectalwallreaching
totheperirectaladiposetissueinallthecases.Lenisa
con-cludesthatSTARRusingthenewinstrumentismuchmore
effective,astheeliminationofthewholerectalwallthickness
isobtained,it duplicatestheaverageofthetissueresected
sizeandweightcomparingitwiththeweightaverage
accom-plished witha PPH-01(Ethicon endosurgery USA)that had
been 15g.Thetissueweightintheresectionswasbetween
6and13g,butagainnosignificantdifferencesbetween
sta-plersCPH-34,CPH-34HV(FrankenmanInternationalLtd.)and
EEA-3135-HEM(CovideanUSA)asshowninTable3andFig.3.
Reboa14in2009publishesananalysisoftheSTARRresults
inthetreatmentofobstructiveevacuation, consideredasa
modern alternative inthe transanal treatment techniques.
Reboa employsthePPH-01(Ethicon endosurgeryUSA),
pre-sentingaselementsfortechniqueevaluationthemechanical
technologyeffectsintheresectedmucosalspecimens,being
necessarytorememberthatinSTARRtechniqueareobtained
twosegments,anteriorandposterior.Theaveragevaluesthat
werereachedwereverticalof4.3±1.1cmfortheanterior
seg-mentand3.6±1.2cmfortheposteriorsegment,horizontalof
5.8±1.4cmfortheanteriorsegmentand4.5±1.3cmforthe
posteriorsegment.Reboadoesnotconsidertheparameters
ofweightorvolume,neitherthehistologicevaluationofthe
thickness.Fromdeanalysisofthemultipleauthorsuntilnow,
themostimportantvariablesarethehorizontalandvertical
lengths,thisisnotbeingshowninourtablesandfigures,as
therearenoresultswithstatisticallysignificantdifferences.
In 2009, Isbert15 presents a comparative study between
STARR andTRANSTARforthe obstructiveevacuation
treat-ment. In their study is expressed that surgical techniques
promoted in that moment looked for the distal rectus
12 3 7 11 0 10 8 6 4 2 0 No improvement Some improvement Marked improvement Full improvement N observed
Fig.7–Improvementlevels.
associated,even when it have notbeen proved,an
exten-sivesuppressionoftherectuscouldimprovetheevacuation
function.Isbert compares the PPH-01 (Ethiconendosurgery
USA)withtheCCS-30contourtranstar(Ethiconendosurgery
USA)allowingustorescuethemechanicaltechnologyeffects
values of both machines, with the resected tissue
vol-ume, being 46±10.68cm3 for the CCS-30 contour transtar
(EthiconendosurgeryUSA)and27±4.86cm3 forthePPH-01
(Ethiconendosurgery USA).Regarding the width ofthe
tis-suebandsresecteditshowedanaverageof4.5cmand3.5cm
respectively.IsbertsustainsthattheCCS-30contourtranstar
(Ethiconendosurgery USA)hasa greater capacitythan the
PPH-01 (Ethicon endosurgery USA), as the last one shows
limitationsfortheresectionofrectaltissueduetothe
restric-tions in accommodating to the tissue appropriatevolume
inthestapled cylinder.Howeverit establishesthat besides
theacceptancethatobtainingthecompletetissueprolapsed
wouldimprove the function,it isnotdemonstrated bythe
studywhentheresultsofbothstaplersarecomparedafter12
monthsoffollowing.Isbertconsiderationsarevery
interest-ing,inourstudywereachedimportantlevelsofimprovement
andsatisfaction,showninFigs.7and8,butthiswasobtained
inagreaterfollowingtimethanIsbert’s.
Wadhawan16 in 2010 shows an study where is tried to
established if the CCS-30 contour transtar (Ethicon
endo-surgery USA) increases the results because of its better
mechanical technology effect, compared to the PPH-01
(EthiconendosurgeryUSA),sincethislastonepresents
limita-tionsinthetissueresectionsassaidbyIsbert.Thecapacitiesof
bothstaplerswerereachedwiththemeasureoftheextended
tissueonatableand fixedwithtweezers,without
stretch-ingit,themeasureofthespecimenwasmadeinthecentral
portionwithvaluesof4.2cmforthePPH-01(Ethicon
endo-surgery USA), and 5.3cm for the CCS-30 contour transtar
(EthiconendosurgeryUSA),thecircumferencemeasureswere
takenasequal.Ontheotherhanditestablishesthatevenif
thereisnosignificantdifferenceintherectalwallresection
capacity it cannot be established the improvement. One
critique to the method for obtaining the measures of the
18 16 14 12 10 8 6 4 2 0 Very unsatisfied 0 0 4 17 Somewhat unsatisfied Somewhat satisfied Very satisfied N observed
Fig.8–Degreeofsatisfaction.
mechanical process is the tissues elasticity, being
recom-mended, asa moresuitable variable,the tissueweight, as
previouslyproposedbyLenisain2008,eventhoughthe
accu-racycouldbecompromised.Thatiswhyitisrecommended
to individualize the technique for each patient. The data
obtainedhasdemonstrated thatthereisno significant
dif-ference in the mechanical technology effects where it is
valuedthemucosalresectionmeasures:horizontaland
ver-ticallengthsincentimetres,weightingramsandvolumein
cubic centimetres, accompaniedby the histologic study of
the tissuethicknessinmillimetresofall thestaplers inall
the groups, alsoduringa periodoftimethe patientswere
followedforreportingimprovementandsatisfaction.17 Itis
mandatorytheindividualizationofeach patient,coinciding
withWadhawan,applyingsomethingsimilartothe
Evacua-tionFunctionProtocolandrecordingthecolonictransittime,
radiology of the colon, ecodecografy, anorectal manometry
andpsychologicaltest.4
Leal,2 in 2010 presented the results of evaluating the
TRREMStechniquefortheobstructiveevacuationtreatment,
developed byRegadas3 in Brazil in 2005for the treatment
ofrectoceleandmucosalprolapsewithonecircularstapler.
Leal2 withthecollaborationofRegadasusesthestapler
34-mmEEAcircularstapler(CovideanUSA)forTRREMSobtaining
theresectionoftheanorectaljunctionanteriorwall,mucosa
andsubmucosainthewholecircumference,thismechanical
techniqueeffectisdemonstratedbythereductionofthe
rec-tocelesize,withaveragevalues,obtainedbyecodefecografy,
restingbetween19.2mmand6.6mmandwitheffortbetween
34.8mmand 10.9mm, after treatment. There are noother
parametersinthepaperofeffortmeasure,butthereisthe
pro-posalthatforoptimizingthesurgicaltechniqueitshouldbe
modifiedthestaplersoruseasingleone.Theyhavepresented
theresultsoftheanalysisofthreestaplersdesignedwiththe
purposeofmaking transanalresectionswithdiverse
thera-peutic indications,in this case,anorectocele withTRREMS
technique. The staplers were CPH-34, CPH-34HV
(Franken-manInternationalLtd.)andEEA-3135-HEM(CovideanUSA)an
allegedevolutionofdesignofthePPH-01(Ethiconendosurgery
isstatisticallynotsignificantonthepreviousvaluespublished
bythereviewedliterature.
Cruz18 in 2011, published a multicentre investigation
whereisevaluatedtheTRREMStechnique.Inthis
opportu-nitytheyuse twostaplers,the34-mmEEAandthe 31-EEA
circumferentialstapler(CovideanUSA)inordertoremove
cir-cumferentiallytheanorectalmucosaandtostrengthenthe
anorectalanteriorwalljunction,butwithoneofthestaplers.
Thereisnoassessmentofthestapler’seffectsexceptthe
men-tionaboutthe10.6%ofpatientshavingaresidualanorectocele
gradeI. ItismentionedthatTRREMStechniquemadewith
onestaplerproducedarectocelesuppressionfollowedbya
complete mucosectomyand anopexy,whereadditionally it
rectifiesthe rectovaginalwalland itstrengthen thefibrous
tissueproducedinthehealingprocess.
Allthisleadsustoconcludethatinthepresenceof
obstruc-tive defecation syndrome (ODS), the selection criteria for
patientsareessential,4sothat,withatechnique3andastapler
appliedbyacoloproctologist19importantimprovementlevels
andsatisfactiondegreeswillbeobtained.4,17
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. RegadasFS,Murad-RegadasSM,WexnerSD,RodriguesLV, SouzaMH,SilvaFR,etal.Anorectalthree-dimensional endosonographyandanalmanometryinassessinganterior rectoceleinwomen:anewpathogenesisconceptandthe basicsurgicalprinciple.ColorectalDis.2007;9:80–5.
2. LealVM,RegadasFSP,MuradRegadasSM,VerasLR.Clinical andfunctionalevaluationofpatientswithrectoceleand mucosalprolapsetreatedwithtransanalrepairofrectocele andrectalmucosectomywithasinglecircularstapler (TRREMS).TechColoproctol.2010;14:329–35.
3. RegadasFS,RegadasSM,RodriguesLV,MisiciR,SilvaFR, RegadasFilhoFS.Transanalrepairofrectoceleandfullrectal mucosectomywithonecircularstapler:anovelsurgical technique.TechColoproctol.2005;9:63–6.
4. VargasE,PérezL,MeloI,BravoP,Sardi ˜nasC.Curade rectoceleporvíatransanal.ExperienciadelaUnidadde ColoproctologíadelHospitalUniversitariodeCaracas.Rev VenezCir.2009;62:103–6.
5. PescatoriM,SpyrouM,Pulvirentid’UrsoA.Aprospective evaluationofoccultdisordersinobstructeddefecationusing the“icebergdiagram”.ColorectalDis.2007;9:452–6.
6. BoccasantaP,VenturiM,SalaminaG,CesanaBM,Bernasconi F,RoviaroG.Newtrendsinsurgicaltreatmentofoutlet
obstruction:clinicalandfunctionalresultsoftwonovel transanalstapledtechniquesfromarandomizedcontrolled trial.IntJColorectalDis.2004;19:359–69.
7.BoccasantaP,VenturiM,StutoA,BottiniC,CavigliaA, CarrieroA,etal.Stapledtransanalrectalresectionforoutlet obstruction:aprospective,multicentertrial.DisColon Rectum.2004;47:1285–96.
8.KleemanSD,WestermannC,KarramMM.Rectocelesand anatomyofposteriorvaginalwall:revisited.AmJObstet Gynecol.2005;193:2050–5.
9.RegadasFS,RegadasSM,RodriguesLV,MisiciR,TramujasI, BarretoJB,etal.Newdevicesforstapledrectalmucosectomy: amulticenterexperience.TechColoproctol.2005;9:243–6.
10.Habr-GamaA,eSousAHJr,RovelóJM,SouzaJV,BenícioF, RegadasFS,etal.Stapledhemorrhoidectomy:initial experienceofaLatinAmericangroup.JGastrointestSurg. 2003;7:809–13.
11.LehurPA,StutoA,FantoliM,VillaniRD,QueraltoM, LazorthesF,etal.Outcomesofstapledtransanalrectal resectionvs.biofeedbackforthetreatmentofoutlet obstructionassociatedwithrectalintussusceptionand rectocele:amulticenter,randomizedcontrolledtrial.Dis ColonRectum.2008;51:1611–8.
12.RenziA,TalentoP,GiardielloC,AngeloneG,IzzoD,DiSarno G.Stapledtransanalrectalresection(STARR)byanew dedicateddeviceforthesurgicaltreatmentofobstructed defecationsyndromecausedbyrectalintussusceptionand rectocele:earlyresultsofmulticenterprospectivestudy.IntJ ColorectalDis.2008;23:999–1005.
13.LenisaL,SchwandnerO,StutoA,JayneD,PigotF,TuechJJ, etal.STARRwithContour® TranstarTM:prospective multicenterEuropeanstudy.ColorectalDis.2009;11:821–7.
14.ReboaG,GipponiM,LigorioM,MarinoP,LantieriF.The impactofstapledtransanalrectalresectiononanorectal functioninpatientswithobstructeddefecationsyndrome. DisColonRectum.2009;52:1598–604.
15.IsbertC,ReibetanzJ,JayneDG,KimM,GermerCT,BoenickeL. ComparativestudyofContourTrastaranSTARRprocedure forthetreatmentofobstructeddefaecationsyndrome(ODS) feasibility,morbidityandearlyfunctionalresults.Colorectal Dis.2010;12:901–8.
16.WadhawanH,ShorthouseAJ,BrownSR.Surgeryfor obstructeddefaecation:doestheuseoftheContourdevice (Trans-STARR)improveresults?ColorectalDis.
2009;12:885–90.
17.MurthyVK,OrkinBA,SmithLE,GlassmanLM.Excellent outcomeusingselectivecriteriaforrectocelerepair.DisColon Rectum.1996;39:374–8.
18.CruzJV,RegadasFSP,Murad-RegadasSM,RodriguesLV, BenicioF,LealR,etal.TRREMSprocedure(TransanalRepairof RectoceleandrectalMucosectomywithonecircularStapler). Aprospectivemulticentertrial.ArqGastroenterol.
2011;48:3–7.