REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
PublicaçãoOficialdaSociedadeBrasileiradeAnestesiologiawww.sba.com.br
SCIENTIFIC
ARTICLE
Impact
of
postoperative
cognitive
decline
in
quality
of
life:
a
prospective
study
Joana
Borges
a,
Joana
Moreira
a,
Adriano
Moreira
a,
Alice
Santos
a,
Fernando
J.
Abelha
a,b,∗aCentroHospitalardeSãoJoão,Servic¸odeAnestesiologia,Porto,Portugal
bFaculdadedeMedicinadaUniversidadedoPorto,DepartamentodeCirurgia,UnidadedeAnestesiologiaeMedicina Perioperatória,Porto,Portugal
Received17September2015;accepted20July2016 Availableonline29August2016
KEYWORDS
Postoperativecare; Postoperative cognitivedecline; Qualityoflife
Abstract
Background: Regardless the progress in perioperative care postoperative cognitive decline (PCD)hasbeenacceptedunequivocallyasasignificantandfrequentcomplicationofsurgeryin olderpatients.Theaimofthisstudywastoevaluatetheincidenceofpostoperativecognitive declineanditsinfluenceonqualityoflifethreemonthsaftersurgery.
Methods:Observational,prospectivestudyinaPost-AnesthesiaCareUnit(PACU)inpatients agedabove45years,afterelectivemajorsurgery.CognitivefunctionwasassessedwithMontreal Cognitive Assessment (MOCA);Qualityof life(QoL) was assessedusing SF-36Health Survey (SF-36).Assessmentswereperformedpreoperatively(T0)and3monthsaftersurgery(T3). Results:Forty-onepatients werestudied. TheincidenceofPCD3months aftersurgerywas 24%.AtT3MOCAscoreswerelowerinpatientswithPCD(median20vs.25,p=0.009).When comparingthemedianscoresforeachofSF-36domains,therewerenodifferencesbetween patientswithandwithoutPCD.In patientswithPCD,andcomparingeachofSF-36domains obtainedbefore andthreemonthsafter surgery,hadsimilarscoresfor everyofthe8SF-36 areaswhilepatientswithoutPCDhadbetterscoresforsixdomains.AtT3patientswithPCD presentedwithhigherlevelsofdependencyinpersonalactivitiesofdailyliving(ADL). Conclusion:ThreemonthsaftersurgerypatientswithoutPCDhadsignificantimprovementin MOCAscores.PatientswithPCDobtainednoincreaseinSF-36scoresbutpatientswithoutPCD improvedinalmostallSF-36domains.PatientswithPCDpresentedhigherratesofdependency inpersonalADLaftersurgery.
©2016PublishedbyElsevierEditoraLtda.onbehalfofSociedadeBrasileiradeAnestesiologia. Thisisanopenaccess articleundertheCCBY-NC-NDlicense(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
∗Correspondingauthor.
E-mail:[email protected](F.J.Abelha).
http://dx.doi.org/10.1016/j.bjane.2016.07.012
0104-0014/©2016PublishedbyElsevierEditoraLtda.onbehalfofSociedadeBrasileiradeAnestesiologia.Thisisanopenaccessarticle
PALAVRAS-CHAVE
Cuidado pós-operatório; Declíniocognitivo pós-operatório; Qualidadedevida
Impactododeclíniocognitivopós-operatórionaqualidadedevida:estudo prospectivo
Resumo
Justificativaeobjetivo: Independentedoprogressodotratamentonoperíodoperioperatório, odeclíniocognitivonopós-operatório(DCPO)éinequivocamenteaceitocomoumacomplicac¸ão importanteefrequentedacirurgiaempacientesmaisvelhos.Oobjetivodesteestudofoiavaliar aincidênciadeDCPOesuainfluêncianaqualidadedevidatrêsmesesapósacirurgia. Métodos: EstudoprospectivoobservacionalconduzidoemSaladeRecuperac¸ãoPós-anestesia (SRPA)compacientesdeidadesuperiora45anos,apóscirurgiaeletivadegrandeporte.Afunc¸ão cognitivafoiavaliadacomotestedeAvaliac¸ãoCognitivadeMontreal(MOCA)eaqualidadede vida(QV)comoQuestionáriosobreQualidadedeVida(SF-36).Asavaliac¸õesforamrealizadas nopré-operatório(T0)etrêsmesesapósacirurgia(T3).
Resultados: Foramavaliados41pacientes. Aincidência deDCPOtrêsmesesapósacirurgia foide24%.EmT3,osescoresMOCAforammenoresnospacientescomDCPO(mediana20vs. 25, p=0,009).Ao compararas medianasdos escorespara cada um dosdomíniosdo SF-36, não observamos diferenc¸asentreos pacientescome semDCPO.Aocomparar cadaumdos domíniosdoSF-36obtidosanteseapóstrêsmesesdecirurgia,ospacientescomDCPO apre-sentaramresultadossemelhantesparacadaumadasoitoáreasdoSF-36,enquantopacientes semDCPOapresentaramresultadosmelhoresemseisdomínios.EmT3,ospacientescomDCPO apresentaramníveismaiselevadosdedependêncianarealizac¸ãodeatividadescotidianas. Conclusão:Três mesesapósacirurgia,os pacientessemDCPO apresentarammelhora signi-ficativa dosescores MOCA.OspacientescomDCPO não apresentaram aumentodosescores SF-36,masospacientessemDCPOapresentarammelhoraemquasetodososdomíniosdo SF-36.OspacientescomDCPOapresentaramtaxasmaiselevadasdedependêncianarealizac¸ão deatividadescotidianasapósacirurgia.
©2016PublicadoporElsevierEditoraLtda.emnomedeSociedadeBrasileiradeAnestesiologia. Este ´eum artigo Open Access sob umalicenc¸aCC BY-NC-ND(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
Introduction
Regardlesstheprogressinperioperativecare,postoperative
cognitivedecline(PCD)hasbeenacceptedunequivocallyas
asignificantandfrequentcomplicationofsurgeryinolder
patients.1---12 However,thereisstillnoconsensusdefinition
ofPCDinthemedicalcommunity,andbroadly,itrefersto
atemporarydeclineincognitionassociatedwithsurgery.13
Ifitlastlongerthanthreemonthsis definedaslong-term
postoperativecognitivedecline,13,14andaconsiderable pro-portionofpatientsdonotrecoverthreemonthsaftersurgery (7---69%incardiacsurgery).15
The exactetiologyofPCDremainsunclearandis
prob-ablymultifactorial.15,16 Complicationsintheperioperative periodmayanticipateearlyPCD,butincreasingagehasbeen
shown to bea significant and independent risk factor for
PCD.The incidenceof PCDisexpectedtoincrease asthe
populationofoldersurgicalpatientsgrows.11,17
Patients submitted to cardiac surgery have been
pro-fusely studied, however, the incidenceand prevalence of
thiscomplicationafterothertypesofsurgeryhasnotbeen
so exhaustively reported.16,18 The International Study of
Postoperative Cognitive Dysfunction (ISPOCD) group
stud-ied 1218 patients aged 60 years old or older, undergoing
majorgeneralsurgeryandreportedanincidenceofPCDof
25.8---9.9%, oneweek andthreemonths followingsurgery,
respectively.6 However,theestimationofthefrequencyof
PCDstillvariesfrom25%to80%.4
The diagnosis of PCD requires valid and accurate
pre-operativeandpostoperativeneuropsychologicaltestingand
thedeterminationofacut-offpointbetweenPCDand
nor-malvariationincognitiveperformance.PCDdiagnosisisnot easytoperformandithasnoapparentclinicalsymptoms
---patientsmaypresentanimpairmentinoneorvarious
cog-nitive abilities suchas memory,attention, concentration,
speedofmotorandmentalresponse,informationprocessing
and learn after surgery and anesthesia that is different
fromdelirium.4,13,19Ithasasubtlemannerofmanifestation,
commonlymany daysor weeks aftersurgery.2,4 Numerous
cliniciansfail torecognizethe subject’s cognitivedecline
followingsurgery;butalsothepatientsthemselves,dueto
inattentionor embarrassment,may notbeawareof their
PCDor bereluctant toreport any alteration.4 Until now,
thereis no standard accepted approach for its diagnosis,
anditisessentialuseseveralvalidandhighlysensitive
neu-ropsychologicaltests,whichallowassessingmanycognitive
areas.4,19---21
Althoughcognitivechangesarenotmanifestedclinically
insomepatients,recentstudiesshowthatPCDmayleadto
aprolongedhospitalstay,elevatedmedicalcosts,increased
morbidityand readmission tohospital.PCDhas long-term
consequencesintermsofincreasedall-causemortalityand
declined in Quality of Life (QoL), associatedwith
impair-mentsin dailyfunctioning,prematuredeparturefromthe
labormarket,anddependencyoneconomicassistanceafter
Thepurposeofthisstudywastoassesstheincidenceof
PCDandcognitiverecovery3monthsfollowingnon-cardiac
andnon-neurologicalsurgeryandtodeterminetheimpact
ofcognitivedeclineinQoLanddependencyinactivitiesof
thedailyliving.
Methods
Ethics
Ethicalapprovalforthisstudy(EthicalCommitteeapproval
n◦
127/12)wasprovidedbyComitédeÉticaparaaSaúdedo
CentroHospitalardeSãoJoão,Porto,Portugal(Chairperson:
ProfessorFilipeAlmeida)onMay25,2012.Writtenconsent
wasobtainedfromallpatients.
Thecohort
Atotal of221 patients undergoingelective majorsurgery
wereenrolled in the study, conductedfrom 18thJune to
15th July 2012, in the multidisciplinary Post-Anesthesia
Care Unit (PACU). The inclusion criteria involved adult
Portuguese-speaking patients submittedtomajor elective
surgery(definedassurgerythatrequirestwoormoredays
of hospital stay) requiring anesthesia, aged 45 years old
and older. Patients could not be included twice, even if
theyhadanunrelatedsecondprocedure.Patientswerealso
excludedif they(1)hadcognitiveimpairment atbaseline
assessmentconsideredforpatientswithaMini-MentalState
Examination(MMSE)score22oflessthan24;(2)hadnot
pro-videdorwereincapableofprovidinginformedconsent;(3)
wereunabletounderstandthelanguageusedorwere
illit-erate; (4) were unwilling tocomply withthe protocol or
procedures;(5)hadbeensubmittedtourgentoremergent
surgery;(6)hadbeen admittedforobstetric,neurological
orcardiacsurgery;and(7)wereadmittedtointensivecare
units for postoperative vigilance. All patients were
inter-viewed either on the eve or the day of the surgery (at
least3h before). Itwasthen conductedasmall
consulta-tiontoobtainconsent,toperformMMSEtestandtocollect
the medical history. Patients completed
neuropsychologi-caltestsatentrytothestudy(T0)andthreemonthsafter
surgery(T3). These testsincluded the Montreal Cognitive
Assessmenttest(MOCA),23 theMedicalOutcomesStudy36
items Short Form Health Survey test (SF-36),24 the
Law-toninstrumentalactivitiesofthedailylivingscale(Lawton
scale)25 and the Katz Index of Independence in activities
ofthe daily living(Katz’s Index).26 Anesthesiologistswere
blinded to patient involvement in the study. Conduct of
anesthesia,includingthechoice ofthetypeof anesthesia
wasatthediscretionoftheanesthesiologist.
Patientassessment
The recordedpatients’ characteristics were:age, weight,
height, body mass index (BMI) and American Society of
Anaesthesiologists Physical Status (ASA-PS). The Revised
CardiacRiskIndex(RCRI)wasalsocalculated,usingthe
clas-sificationsystem reportedby Lee etal.,27 which includes
high-risk surgery (i.e., intraperitoneal, intrathoracic, or
suprainguinalvascularprocedures)andclinicalriskfactors:
history of ischemic heart disease, compensated or prior
heart failure, cerebrovascular disease, diabetes mellitus
andrenalinsufficiency.Thesevariablesareincludedinthe
Cardiac Risk Stratification for Non-cardiac Surgical
Proce-duresofthe2007guidelinesonPerioperativeCardiovascular
EvaluationandCarefor Non-cardiacSurgeryof the
Ameri-canCollegeofCardiology/AmericanHeartAssociationTask
ForceonPracticeGuidelines.28
Intraoperative details, including type and duration of
anesthesiaandsurgicalprocedures,lengthofPACUstayand
any cardiorespiratory events in this unit were also
docu-mented.
EvaluationofPCDandqualityoflife
Each participantunderwent neuropsychological testing at
two-timepoints:preoperatively(T0)andthreemonthsafter
surgery(T3).
Allpatientscompletedbaselineassessmentsof general
cognitive functioning assessed by the Mini-Mental State
Examination.MMSEisavalidandrecognizedtest,performed
in5---10min;thatevaluatescognitivestatus.Itgrossly
evalu-atesexecutivecognitivefunctionbymeasuringorientation,
calculations,memory, readingandwriting capacities,
lan-guage andvisuospatialability. Even so,patients withmild
forms of cognitivedecline frequently scorein the normal
rangeintheMMSE.22
Montrealcognitiveassessment testis aone-page
ques-tionnaire that takes 10min to perform and is suitable to
evaluateshort-termmemory,executivefunctions, working
memory, concentration, visuospatial abilities, attention,
language,andtemporalandspatialorientation.The score
rangevariesfrom0to30,andhigherscoresindicatebetter
cognitive performance. To adjust for educational effects,
subjects with 12 or fewer years of education receive
an extra point.23,29,30 Several studies were conducted in
Portugal concerning the Portuguese experimental version
oftheMOCA,andthestudies’conclusionsappeartoassure
thevalidityandclinical utilityofthistool.30 Adopting the
criterion usedby Baracchini et al.1 a decline of at least
2 points in MOCA test at T3 was considered as clinically
relevantanddefinedasPCD.
TheMedicalOutcomesStudy36ItemShortFormHealth
Survey24aimstoquantifygeneralhealthconditionand
con-sistsofeightsectionsordomains, whicharetheweighted
sums of thequestionsin their section.The eightdomains
arevitality,physicalfunctioning,bodilypain,generalhealth
perceptions,physicalrolefunctioning,emotionalrole
func-tioning, social role functioning, and mental health. This
questionnairehasalsobeenculturally adaptedtothe
Por-tugueseandvalidatedinastudybyFerreiraetal.31,32 Evaluationoffunctionalcapacitywasbasedontheability ofthepatienttoundertakepersonalandinstrumental activ-itiesofdailyliving.Todoso,twoquestionnairesthatassess
thefunctional independenceof thesubjecttoaccomplish
instrumental ADL (I-ADL) and personal ADL (P-ADL) were
used:theLawtonI-ADLscale25andtheKatz’sIndexof
Inde-pendence in ADL, respectively.26 The Lawton I-ADL scale
is easy to perform and provides self-reported knowledge
about the functional skills needed to live in the
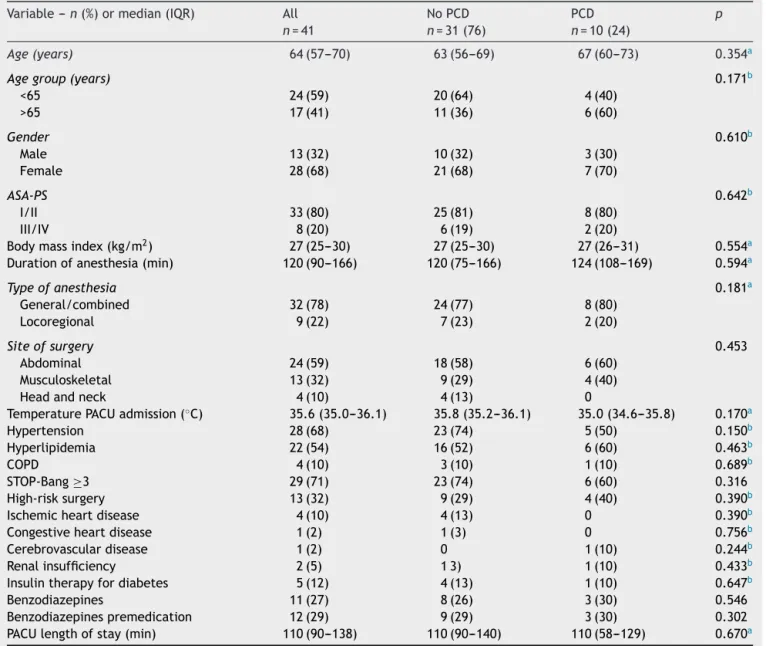
Table1 Pre-admissionpatientcharacteristicsandoutcomes(n=41).
Variable---n(%)ormedian(IQR) All n=41
NoPCD n=31(76)
PCD n=10(24)
p
Age(years) 64(57---70) 63(56---69) 67(60---73) 0.354a
Agegroup(years) 0.171b
<65 24(59) 20(64) 4(40)
>65 17(41) 11(36) 6(60)
Gender 0.610b
Male 13(32) 10(32) 3(30)
Female 28(68) 21(68) 7(70)
ASA-PS 0.642b
I/II 33(80) 25(81) 8(80)
III/IV 8(20) 6(19) 2(20)
Bodymassindex(kg/m2) 27(25---30) 27(25---30) 27(26---31) 0.554a
Durationofanesthesia(min) 120(90---166) 120(75---166) 124(108---169) 0.594a
Typeofanesthesia 0.181a
General/combined 32(78) 24(77) 8(80)
Locoregional 9(22) 7(23) 2(20)
Siteofsurgery 0.453
Abdominal 24(59) 18(58) 6(60)
Musculoskeletal 13(32) 9(29) 4(40)
Headandneck 4(10) 4(13) 0
TemperaturePACUadmission(◦C) 35.6(35.0---36.1) 35.8(35.2---36.1) 35.0(34.6---35.8) 0.170a
Hypertension 28(68) 23(74) 5(50) 0.150b
Hyperlipidemia 22(54) 16(52) 6(60) 0.463b
COPD 4(10) 3(10) 1(10) 0.689b
STOP-Bang≥3 29(71) 23(74) 6(60) 0.316
High-risksurgery 13(32) 9(29) 4(40) 0.390b
Ischemicheartdisease 4(10) 4(13) 0 0.390b
Congestiveheartdisease 1(2) 1(3) 0 0.756b
Cerebrovasculardisease 1(2) 0 1(10) 0.244b
Renalinsufficiency 2(5) 13) 1(10) 0.433b
Insulintherapyfordiabetes 5(12) 4(13) 1(10) 0.647b
Benzodiazepines 11(27) 8(26) 3(30) 0.546
Benzodiazepinespremedication 12(29) 9(29) 3(30) 0.302
PACUlengthofstay(min) 110(90---138) 110(90---140) 110(58---129) 0.670a
PCD,postoperativecognitivedecline;IQR,interquartilerange;ASA-PS,AmericanSocietyofAnesthesiologistsphysicalstatus;COPD,
chronicobstructivepulmonarydisease;PACU,Post-AnesthesiaCareUnit.
a Mann---WhitneyUtest.
b Pearson
2.
finances,shopping,housekeeping,foodpreparation,public
transportationandresponsibilityforownmedications.25The
KatzADLscaleevaluatesbasicpersonalADLandranks
capa-bilityofperformancein6areas:bathing,dressing,goingto
the toilet,transferring frombed tochair, continence and
feeding.25Thepatients’answerswerecategorizedintotwo
classes: capable or incapable toperform each activity or
groupofactivities.Theywereconsideredtobedependentif
theywereincompetenttoperformatleastoneinstrumental
orpersonalADL.
Statisticalanalysis
Descriptive analysis of variables was used to summarize
data. Ordinal and continuous data found not to follow a
normaldistribution,basedontheKolmogorov---Smirnovtest
for normalityof the underlyingpopulation, arepresented
as median and interquartile range (IQR). Normally
dis-tributeddataarepresentedasmeanandstandarddeviation
(SD).Non-parametrictestswereperformedforcomparisons
(WilcoxsignedranktestandtheMann---WhitneyUtest).The
chi-squaretestorFisher’sexacttestwereusedtocompare
proportions between twogroups of subjects. The related
samplesWilcoxonsignedranktestwasusedtocompare
SF-36 scores before surgery and three-months after surgery.
Differenceswereconsideredstatisticallysignificantwhenp
was<0.05. SPSS softwarefor Windows Version 20.0 (SPSS
Inc.,Chicago,IL,USA)wasusedforallstatisticalanalyzes.
Results
Fromthe221patientsconsecutivelyadmittedinthePACU
Table2 SF-36inpatientswithPCD.
T0(median) T3(median) p
Physicalfunction 83 75 0.779
Rolephysical 59 56 0.635
Bodilypain 43 67 0.314
Generalhealth 53 49 0.674
Vitality 40 44 0.905
Socialfunctioning 75 69 0.918
Roleemotional 79 75 0.921
Mentalhealth 52 58 0.818
SF-36,36-Item ShortFormHealth Survey;PCD,postoperative cognitivedecline;T0,beforesurgery;T3,3monthsaftersurgery.
Table3 SF-36inpatientswithnoPCD.
T0(median) T3(median) p
Physicalfunction 70 65 0.289
Rolephysical 50 63 0.021a
Bodilypain 62 74 0.022a
Generalhealth 57 65 0.016a
Vitality 46 50 0.208
Socialfunctioning 75 100 <0.001a
Roleemotional 67 92 0.014a
Mentalhealth 52 68 <0.001a
SF-36,36-Item ShortFormHealth Survey;PCD,postoperative
cognitivedecline;T0,beforesurgery;T3,3monthsaftersurgery.
aStatisticallysignificant,p<0.05.
One-hundredsixty-threepatientswereexcluded,according
totheexclusioncriteria:21couldnotperformpreoperative assessment,112hadlessthan45yearsold,12patientswere
admittedtoasurgicalintensivecareunit,8patientswere
unabletoprovideinformedconsentorhadanMMSE<24,2
patientsdidnotundergosurgery,2patientsunderwent
neu-rosurgery,3patientsdidnotspeakPortugueseand3patient
refusedtoparticipate.Fromtheremaining57patients,only
41 patients have completed all evaluations for cognitive
assessmentandqualityoflifeatthreemonthsfollow-up.
The characteristics of the population are summarized
in Table1. The median age was 64years old.78% of the
patientsunderwent generalor combinedanesthesia
(gen-eralpluslocoregionalanesthesia,andthemediantimefor
itsdurationwas120min.Gastrointestinalsurgeryaccounted
for)49%ofthecases,plasticandreconstructivesurgeryto
15%,gynecologicsurgeryandorthopedics,each10%,
urol-ogyto8%,vascularto4%,headandnecksurgeryto3%and
otorhinolaryngologyto1%ofthecases.Nostatistically
sig-nificantdifferencesbetweenpatientswithandwithoutPCD
wererecordedforthestudiedvariables.
The incidenceofPCD,3monthsaftersurgery,was24%
(n=10).AtT0,nodifferencesemergedfortheMOCAscores
between patients withand without cognitive impairment
(median25vs.21,p=0.139).AtT3,however,patientswith
PCDhadworsemedian MOCAscores(20vs.25,p=0.009).
ComparingtopreoperativeMOCAscores,PCDpatientshad
worseMOCAmedianscoresatT3(20vs.25,p=0.001),while patientswithoutPCDhadbetterscores(25vs.21,p<0.001).
Tables2 and3presentmedianscores ofSF-36domains
forbothgroupsofpatients,comparingT0andT3score.For
Table4 Comparinggroups withandwithout PCDbefore
surgeryforSF-36(T0).
SF-36domains WithoutPCD WithPCD p
Physicalfunction 70 83 0.772
Rolephysical 50 59 0.561
Bodilypain 62 43 0.407
Generalhealth 57 53 0.465
Vitality 46 40 0.562
Social 75 75 0.736
Roleemotional 67 79 0.288
Mentalhealth 52 52 0.513
SF-36, 36-ItemShort FormHealth Survey;PCD,postoperative cognitivedecline;T0,beforesurgery.
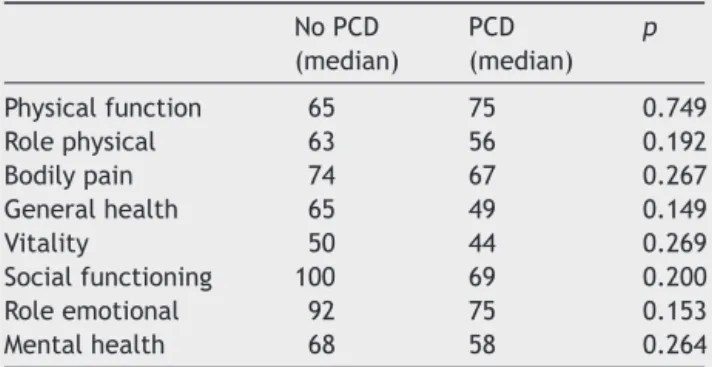
Table5 ComparinggroupswithandwithoutPCDforSF-36
3monthsaftersurgery(T3).
NoPCD (median)
PCD (median)
p
Physicalfunction 65 75 0.749
Rolephysical 63 56 0.192
Bodilypain 74 67 0.267
Generalhealth 65 49 0.149
Vitality 50 44 0.269
Socialfunctioning 100 69 0.200
Roleemotional 92 75 0.153
Mentalhealth 68 58 0.264
SF-36, 36-ItemShort FormHealth Survey;PCD,postoperative cognitivedecline;T3,3monthsaftersurgery.
patientswithPCD,andcomparingeachofSF-36domainsat T0and T3,therearesimilarscores for everyof theeight SF-36domains(Table 2).Patientswithout PCDhad better scoresatT3insixdomains(Table3):rolelimitationscaused
by physicalproblems (median 63vs.50, p=0.021),bodily
pain(median74 vs.62,p=0.022), generalhealth
percep-tion(median65vs.57,p=0.016),socialfunctioning(median 100vs.75,p<0.001),rolelimitationscausedbyemotional
problems (median 92vs. 67, p=0.014)and mentalhealth
(median68vs.52,p<0.001)andtheyhadsimilarscoresfor vitality(p=0.208)andphysicalfunction(p=0.289)domains.
Tables4 and5 present themedian scores for allSF-36
domains obtained before and after surgery, respectively,
comparingpatientswithandwithoutPCD.Asexhibited,at
T0andT3allscoresforSF-36domainsweresimilar.
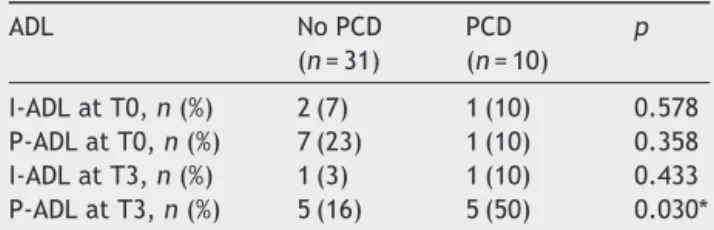
InTable6itisshownthatatT0thereweresimilarrates
ofdependencyinP-ADLandI-ADL,whencomparingpatients
with and without PCD; however, at T3 patients with PCD
presented withhigherlevelsofdependency inP-ADL (50%
vs. 16%, p=0.030). Comparing their rates of dependency
at T0withT3and forpatients withPCDthereis ahigher
dependencescoresinI-ADL(50%vs.10%,p=0.037)butnot
for P-ADL (10% vs. 10%, p=1.0).In the samecomparison,
patients withoutPCDhad nodifferencesinI-ADL(29% vs.
Table6 Independencyinactivitiesofdaily livingbefore andaftersurgery.
ADL NoPCD
(n=31)
PCD (n=10)
p
I-ADLatT0,n(%) 2(7) 1(10) 0.578 P-ADLatT0,n(%) 7(23) 1(10) 0.358 I-ADLatT3,n(%) 1(3) 1(10) 0.433 P-ADLatT3,n(%) 5(16) 5(50) 0.030*
ADL, instrumental activities of daily living; P-ADL, personal activitiesofdailyliving;T0,beforesurgery;T3,3monthsafter surgery.
Discussion
WereportanincidenceofPCDof24%,threemonths follow-ingsurgery.Inliterature,theincidenceofPCDisnotclearly definedandmayvarybetween25%and80%.4,13Manycurrent reportsestablishthatsurgery,particularlycardiacsurgery,
mayresultinPCDandthatitsincidenceincreaseswithage,
independentlyoftheanesthetictechnique.11
PCD can have a considerable impacton qualityof life
andmayresultinwithdrawalfromsociety.11,13,15,17Inrecent
years, PCDafter non-cardiac surgery has been
systemati-callystudied.InparticulartheISPOCD(InternationalStudy
groupofPostoperativeCognitiveDysfunction)was
success-fulinuncoveringtheextentoftheproblemanddefiningrisk
factors.EarlyPCDoccursinapproximately25%ofpatients
oneweekaftersurgery,andthendeclinestolessthan10%
afterthreemonths.6
PCD refers to deterioration in cognition temporally
associated with operation; thus, the growing number of
elderly patients undergoing surgery should aware
anes-thesiologists and surgeons to its serious repercussions.11
Nevertheless,thereisnoexplicitinformationifanychange
in procedures would change the incidence of PCD,but it
is possible that preoperative medication, anticholinergic,
catecholamine’s, and some events such as hypotension,
hypothermia,hypoxia,cerebralatheroembolismor
hypoper-fusion, poorglycemic controland carotidendarterectomy
maycontributetohighincidencelevelsofPCD.2Inourstudy,
wedidnotfounddifferencesrelatedtopatientdemographic
variablesoranesthesiaorsurgicalcharacteristics.
InthemultiplePCDstudiestherehasnotbeenastandard
methodology used33 and the choice of neuropsychological
testinstruments,thecriteriatoconsider,thetimingof test-ingandretesting,andinclusionandexclusioncriteriahave allvaried.34
The use of highly sensible and specific
neuropsycholo-gicaltests allowsfortheidentification of subtlecognitive deficitswithexcellenttest/retestvalidity,butwithhighest riskoftypeIIerrors(failingtodetectPCD).Forthisstudy,
theMOCAtestwaschosen becauseit iseasy andquickto
perform and enables the evaluation of several functional
domainsofcognition.Evenso,itmayfailtoidentifysome
patientswithmilderformsofPCD.35,36
Perioperative interventions have long-range effects on
theindividual,sostrategiestopreservelong-termcognitive performanceandqualityoflifearerequired.37
The risk of cognitivedecline increaseswith ageand is
furtherenhanced after hospitalizationfor surgery,
result-ing in significant morbidity and reduced quality of life.38 Actually,thereisnoindividualapproachtoavoidcognitive
deterioration2 but the maintenanceand/or restorationof
functionalindependence,includingcognition,intheelderly
hospitalizedpatientconstitutesamajorchallengefor the
healthcaresystem.
The postoperative cognitive decline may diminish
improvements in QOL and strategies to reduce
cogni-tive decline mayallow patients toachieve the maximum
improvementinQOLaftersurgery. Thishasbeen the
sub-ject of various studies7 and like them the present study
demonstratedthat cognitivedecline limitedimprovement
inQOL.
Even mild cognitive deficits before surgery may be a
markerforincreasedriskofcognitivedecline39 andalsoit
hasbeen accepted that PCDgenerally resolvewithin 1---3
monthsinmostpatientsinwhomnewcognitivesymptoms
developduringpostoperativeperiod.33,39,40
Threemonthsaftersurgeryasignificantimprovementin
qualityof life in patients without PCD wasdemonstrated
byan increase in almost all scores of SF-36domains, but
amongstpatientswithPCD,noimprovementwasseeninany
oftheSF-36scores.Thislimitationinqualityimprovement
isalsodemonstratedinPCDpatientsbyasignificantmore
dependencyinP-ADLthreemonthsaftersurgerycomparing
withpatientswithoutPCD.
Thisstudyhasseverallimitations.Itisanobservational study,withasmallsampleofpatients.Ithasmanydropouts andlossestothefollow-up(explained,inpart,bytheneed
tohavecomplete interviewsbeforeandafterthesurgery,
forfollow-upconsultation).Furthermore,wedidnot
stud-iedclinicalvariablesaftersurgery,includingcomplications
andmedicationsthatmayhaveaffectednotonlythelosses
tofollow-upbutalsotheresultsincognitiveperformance,
qualityoflifeandindependenceinADL.
Conclusions
Theprincipalfindingsofthisstudywereasfollow:(1)the
incidenceofPCDwasof24%;(2)patientswithPCDshown
noimprovementsinqualityoflifescores;and(3)patients
withoutPCDshownbetterscoresinalmostallSF-36domains
andanincreaseindependency,aftersurgery.
PCD is a real event, with realcomplications and
con-sequences in the quality of life, which requires a better
understanding, especially in terms of etiologic factors in
ordertoprevent them.It shouldnotbe overestimatedas
itdecreasesthequalityoflifeandenhancesthedegreeof
dependencefor activities of daily living, andhigh-quality
perioperativecareandsupportaresocialandfinancialare
essential.
Authorship
Allauthorsconfirm thattheyhaveread andapprovedthe
paper.
Allauthorsconfirm that theyhavemet thecriteriafor
paperrepresentshonestwork, andcan verifythe validity oftheresultsreported.
All persons designated, as authors are qualified for
authorship.
Eachauthorparticipatedsufficientlyintheworktotake
publicresponsibilityforappropriateportionsofthecontent.
Allauthorshavesubstantialcontributionstoconception
anddesign,acquisitionofdata,analysisandinterpretation ofdata,draftingthearticleorrevisingitcriticallyfor impor-tantintellectualcontent.
Allauthorsmadetheirfinalapprovaloftheversionifis
tobepublished.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
TheauthorswouldliketothanktheStaffofCentro Hospita-lardeSãoJoãoPost-AnesthesiaCareUnitfortheirassistance withthestudy.
References
1.BaracchiniC,MazzalaiF,GruppoM,etal.Carotid endarterec-tomy protects elderly patients from cognitive decline: a prospectivestudy.Surgery.2012;151:99---106.
2.BekkerAY,WeeksEJ.Cognitivefunctionafteranaesthesiainthe elderly.BestPractResClinAnaesthesiol.2003;17:259---72.
3.BergerM,NadlerJW, BrowndykeJ,etal.Postoperative cog-nitive dysfunction: minding thegaps in our knowledge of a commonpostoperativecomplicationintheelderly.Anesthesiol Clin.2015;33:517---50.
4.Funder KS, Steinmetz J, Rasmussen LS. Cognitive dys-function after cardiovascular surgery. Minerva Anestesiol. 2009;75:329---32.
5.HudetzJA,IqbalZ,Gandhi SD,etal.Postoperativecognitive dysfunctioninolderpatientswithahistoryofalcoholabuse. Anesthesiology.2007;106:423---30.
6.Moller JT, Cluitmans P, Rasmussen LS, et al. Interna-tionalStudyofPost-OperativeCognitiveDysfunction.Lancet. 1998;351:857---61.
7.Phillips-ButeB,Mathew JP,BlumenthalJA,etal.Association of neurocognitive function and quality of life 1 year after coronaryarterybypassgraft(CABG)surgery.PsychosomMed. 2006;68:369---75.
8.RasmussenLS,JohnsonT,KuipersHM,etal.Investigatorsdoes anaesthesiacausepostoperativecognitivedysfunction?A ran-domised study ofregional versus generalanaesthesia in438 elderlypatients.ActaAnaesthesiolScand.2003;47:260---6.
9.RasmussenLS,O’BrienJT,SilversteinJH,etal.Isperi-operative cortisolsecretionrelatedtopost-operativecognitive dysfunc-tion?ActaAnaesthesiolScand.2005;49:1225---31.
10.SteinmetzJ,ChristensenKB,LundT,etal.Long-term conse-quencesofpostoperativecognitivedysfunction.Anesthesiology. 2009;110:548---55.
11.SteinmetzJ,SiersmaV,KessingLV,etal.Ispostoperative cogni-tivedysfunctionariskfactorfordementia?Acohortfollow-up study.BrJAnaesth.2013;110Suppl.1:i92---7.
12.van Harten AE, Scheeren TW, Absalom AR. A review of postoperative cognitive dysfunction and neuroinflammation associatedwithcardiacsurgeryandanaesthesia.Anaesthesia. 2012;67:280---93.
13.DeinerS,SilversteinJH.Postoperativedeliriumandcognitive dysfunction.BrJAnaesth.2009;103Suppl.1:i41---6.
14.SelwoodA,OrrellM.Longtermcognitivedysfunctioninolder peopleafternon-cardiacsurgery.BMJ.2004;328:120---1.
15.XuT,BoL,WangJ,etal.Riskfactorsforearlypostoperative cog-nitivedysfunctionafternon-coronarybypasssurgeryinChinese population.JCardiothoracSurg.2013;8:204.
16.AbildstromH,RasmussenLS,RentowlP,etal.Cognitive dys-function 1---2 years after non-cardiac surgery in the elderly. ISPOCDgroup.Internationalstudyofpost-operativecognitive dysfunction.ActaAnaesthesiolScand.2000;44:1246---51.
17.TsaiTL,SandsLP,LeungJM.Anupdateonpostoperative cogni-tivedysfunction.AdvAnesth.2010;28:269---84.
18.MonkTG,WeldonBC,GarvanCW,etal.Predictorsofcognitive dysfunction after major noncardiac surgery. Anesthesiology. 2008;108:18---30.
19.Jungwirth B, Zieglgänsberger W, Kochs E, et al. Anesthesia andpostoperativecognitivedysfunction(POCD).MiniRevMed Chem.2009;9:1568---79.
20.RudolphJL, SchreiberKA, Culley DJ, et al. Measurementof post-operativecognitive dysfunctionaftercardiac surgery: a systematicreview.ActaAnaesthesiolScand.2010;54:663---77.
21.GornallBF,MylesPS,SmithCL,etal.Measurementofquality ofrecoveryusingtheQoR-40:aquantitativesystematicreview. BrJAnaesth.2013;111:161---9.
22.FolsteinMF,FolsteinSE,McHughPR.‘‘Mini-mentalstate’’. A practicalmethodforgradingthecognitivestateofpatientsfor theclinician.JPsychiatrRes.1975;12:189---98.
23.NasreddineZS,PhillipsNA,BédirianV,etal.TheMontreal cogni-tiveassessment,MoCA:abriefscreeningtoolformildcognitive impairment.JAmGeriatrSoc.2005;53:695---9.
24.WareJEJr,SherbourneCD.TheMOS36-itemshort-formhealth survey(SF-36). I.Conceptual frameworkand itemselection. MedCare.1992;30:473---83.
25.Lawton MP, Brody EM. Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist.1969;9:179---86.
26.KatzS.Assessing self-maintenance:activities ofdaily living, mobility,andinstrumentalactivitiesofdailyliving.JAmGeriatr Soc.1983;31:721---7.
27.Lee TH, Marcantonio ER, Mangione CM, et al. Derivation and prospective validation of a simple index for predic-tionofcardiacriskofmajornoncardiacsurgery.Circulation. 1999;100:1043---9.
28.Fleisher LA, Beckman JA, Brown KA, et al. ACC/AHA 2007 guidelinesonperioperativecardiovascularevaluationandcare for noncardiacsurgery: a reportofthe American Collegeof Cardiology/AmericanHeartAssociationTaskForceonPractice Guidelines (Writing Committee to Revise the 2002 Guide-linesonPerioperativeCardiovascularEvaluationforNoncardiac Surgery):developedincollaborationwiththeAmericanSociety ofEchocardiography,AmericanSocietyofNuclearCardiology, HeartRhythmSociety,SocietyofCardiovascular Anesthesiolo-gists,SocietyforCardiovascularAngiographyandInterventions, SocietyforVascularMedicineandBiology,andSocietyfor Vas-cularSurgery.Circulation.2007;116:e418---99.
29.FreitasS,SimõesMR,MarôcoJ,etal.Constructvalidityofthe Montrealcognitiveassessment(MoCA).JIntNeuropsycholSoc. 2012;18:242---50.
30.DuroD, Simões MR,Ponciano E,et al. Validation studiesof the Portuguese experimental version of the Montreal cogni-tiveassessment(MoCA):confirmatoryfactoranalysis.JNeurol. 2010;257:728---34.
31.FerreiraPL.DevelopmentofthePortugueseversionofMOS SF-36.PartI.Culturaland linguisticadaptation. ActaMedPort. 2000;13:55---66.
33.Newman S, Stygall J, Hirani S, et al. Postoperative cogni-tivedysfunctionafternoncardiacsurgery:asystematicreview. Anesthesiology.2007;106:572---90.
34.Rasmussen LS, Larsen K, Houx P, et al. The International StudyofPostoperativeCognitiveDysfunction.Theassessment ofpostoperativecognitivefunction.ActaAnaesthesiolScand. 2001;45:275---89.
35.GögenurI,MiddletonB,BurgdorfS,etal.Impactofsleepand circadian disturbancesin urinary 6-sulphatoxymelatonin lev-els,on cognitive function aftermajorsurgery. JPineal Res. 2007;43:179---84.
36.Newman MF, Grocott HP, Mathew JP, et al. Report of the substudyassessing theimpact ofneurocognitive function on
qualityoflife5yearsaftercardiacsurgery.Stroke. 2001;32: 2874---81.
37.BedfordPD.Adversecerebraleffectsofanaesthesiaonold peo-ple.Lancet.1955;269:259---63.
38.EhlenbachWJ,HoughCL,CranePK,etal.Associationbetween acutecareandcriticalillnesshospitalizationandcognitive func-tioninolderadults.JAMA.2010;303:763---70.
39.SelnesOA,GottesmanRF,GregaMA,etal.Cognitiveand neu-rologicoutcomesaftercoronary-arterybypasssurgery.NEnglJ Med.2012;366:250---7.