Revista
Portuguesa
de
Estomatologia,
Medicina
Dentária
e
Cirurgia
Maxilofacial
ww w . e l s e v i e r . p t / s p e m d
Research
Shear
bond
strength
of
orthodontic
brackets
to
fluorosed
enamel
Mónica
Mendes
a,∗,
Jaime
Portugal
b,
Sofia
Arantes-Oliveira
b,
Pedro
Mesquita
a aFaculdadedeMedicinaDentáriadaUniversidadedoPorto,PortugalbFaculdadedeMedicinaDentáriadaUniversidadedeLisboa,Portugal
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:Received10August2013 Accepted23October2013 Availableonline24February2014
Keywords: Dentalfluorosis Acidetching Orthodonticbrackets Shearstrength Dentalbonding
a
b
s
t
r
a
c
t
Objectives: Toevaluatetheinfluenceofdentalfluorosisandetchingtimeontheshearbond strengths(SBSs)oforthodonticbracketstohumanenamel.
Methods:Atotalof48humanmaxillarycentralincisors,extractedforperiodontalreasons wereused.Thesamplewasdividedintothreeexperimentalgroups(n=16):groupH30with healthyteethandgroupF30andF60withfluorosedteeth(ThylstrupandFejerskovIndex scores3–4).Afteretchingthedentalenamelwith35%phosphoricacidfor30s(groupsH30 andF30)orfor60s(groupF60),metalorthodonticbracketswerebondedwithTransbond XT adhesivesystem andlightcured(1200mW/cm2 for10s).The specimenswerethen thermocycled (5–55◦C,500cycles),storedindistilled water(37◦C/7days),andtestedin shear(Instron,1KN,1mm/min).Failuremodewasclassified,withastereomicroscope(20× magnification),accordingtotheadhesiveremnantindex(ARI).SBSdatawerestatistically analyzedwith1-wayANOVA,followedbyTukeyposthoctests(˛=0.05).Kruskal–Wallisand Mann–Whitneynonparametrictestswereusedtoanalyzefailuredata(˛=0.05).
Results:Nostatisticallysignificant(p=0.763)differenceswerefoundbetweenF30andF60, butthesegroupsshowedastatistically(p<0.05)lowerbondstrengthvaluesthanH30.The non-fluorosedgroupshowedasignificantly(p<0.05)higherARIscorethantheothergroups.
Conclusion: Orthodonticbracketsadhesiontoenamelisnegativelyinfluencedbydental fluo-rosis.Doublingtheetchingtimeinfluorosedteethwasnotenoughtoproducesimilarresults tothoseobservedinthehealthyones.
©2013SociedadePortuguesadeEstomatologiaeMedicinaDentária.Publishedby ElsevierEspaña,S.L.Allrightsreserved.
Resistência
adesiva
a
tensões
de
corte
de
brackets
ortodônticos
colados
a
esmalte
de
dentes
com
fluorose
Palavras-chave:
Fluorosedentária Condicionamentoácido
r
e
s
u
m
o
Objetivos:Avaliarainfluênciadafluoroseedotempodecondicionamentoácidosobrea resistênciaadesivaaocortedebracketsortodônticoscoladosaoesmalte.
Métodos:48incisivoscentraismaxilareshumanos,extraídosporrazõesperiodontais,e divi-didosemtrêsgruposexperimentais(n=16):grupoH30comdentessemfluoroseegrupos
∗ Correspondingauthor.
E-mailaddresses:[email protected],[email protected](M.Mendes).
1646-2890/$–seefrontmatter©2013SociedadePortuguesadeEstomatologiaeMedicinaDentária.PublishedbyElsevierEspaña,S.L.Allrightsreserved.
Bracketsortodônticos Resistênciaaocorte Adesãoaodente
F30eF60comdentescomfluorose(ÍndicedeThylstrupeFejerskov,classificac¸ão3–4).Após ocondicionamentodoesmaltecomácidofosfóricoa35%durante30segundos(H30eF30) oudurante60segundos(F60),foramcimentadosbracketsmetálicoscomosistema ade-sivoTransbondXTefotopolimerizados(1200mW/cm2durante10segundos).Osespécimes foramtermociclados(5–55◦C,500ciclos),armazenadosemáguadestilada(37◦C/7dias),e testadosaocorte(Instron,1KN,1mm/min).Afalhafoiclassificada,comum estereomi-croscópio(ampliac¸ão20x),deacordocomoÍndicedeAdesivoRemanescente(ARI).Osdados deresistência adesivaforamanalisadoscomANOVAecomparac¸õesmúltiplas segundo Tukey(␣=0,05).OstestesdeKruskal-WalliseMann-Whitneyforamutilizadosparaanalisar osdadosdafalha(␣=0,05).
Resultados:Nãoforamencontradasdiferenc¸asestatisticamentesignificativas(p=0,763)entre F30eF60,masestesgruposapresentaramvaloresderesistênciaadesivaestatisticamente (p<0,05)maisbaixosqueosobtidosemH30.OgrupoH30apresentouumaclassificac¸ãoARI estatisticamente(p<0,05)superioraosgruposF30eF60.
Conclusões: Aadesãodebracketsortodônticosaoesmalteénegativamenteinfluenciada pelafluorosedentária.Aduplicac¸ãodotempodecondicionamentoácidonosdentescom fluorosenãofoisuficienteparapromoverresultadossimilaresaosobservadosnosdentes semfluorose.
©2013SociedadePortuguesadeEstomatologiaeMedicinaDentária.Publicadopor ElsevierEspaña,S.L.Todososdireitosreservados.
Introduction
Duetothefluorideionanticariogenicproperties,adecrease indental cariesprevalenceoccurred,inthelast decades.1–3
Whenenamelremineralizationcycleshappeninthepresence offluorideions,the hydroxylgroupsofthe hydroxyapatite arereplacedbyfluorideleadingtoastrongerandless solu-blestructure, thefluoroapatite.4 However,asaresultofits
widespreaduse, there wasalsoan exponentialincrease in fluorosisprevalence.3,5–10
Dentalfluorosis isadevelopmentaltooth enamellesion resultingfromafluorideoverdoseandchronicingestion dur-ing early childhood.8,11 This condition leads to metabolic
changesinameloblasts,resultinginapoormatrixformation andtoothcalcification.11,12Thefluorosedenamelis
character-izedbyahypermineralizedouterlayerandahipomineralized andporoussublayer.13–16
Etching the enamel surface with acids such as phos-phoric acid is an important step to promote adhesion to dental enamel. The acid etching technique, introduced by Buonocore17 in 1955, causes a selective decalcification of
enamel, creating a rough surface and increasing the con-tact area and surface energywhich provides the substrate for infiltration of the bonding agent making possible the micromechanical union between the adhesive/restorative materialsandtheenamelsurface.4However,theadhesionto
enameloffluorosedteethmaybecompromised,duetothe etchingprocedure thathasbeenproventobelesseffective inthesehypermineralizedsurfaces.18–20Someauthors
advo-catetheincreaseofetchingtimeinordertoovercomesuch limitation.20–22
Orthodontictreatmentwithfixedappliancesrequiresan adequatebondbetweenbracketsandtoothenamel,andmay beaclinicalchallengeinendemicfluorosisregions.Ifbond strengthvaluesaretoolow,earlierdebondingofbracketsmay occurasaresultofnormalclinicalstress,forcingadelayand increasingtreatmentcosts.23
Theavailablestudiesthatassesstheadhesionof orthodon-tic brackets to teeth with fluorosis are scarce and show differentresults.20,22,24–27
Theaimofthisstudyistoevaluatetheinfluenceof den-talfluorosisandtheetchingtimeontheshearbondstrength of metal orthodontic brackets to humanenamel. The null hypothesestestedwerethatfluorosisdoesnotdecreasethe bondstrengthanddoublingtheetchingtimedoesnotincrease theadhesionoforthodonticbracketstofluorosedenamel.
Materials
and
methods
Thesamplesize(n=16)wasestimatedwithapoweranalysis toprovidestatisticalsignificancealpha=0.05atan80%power. Thesampleconsistedof48humanuppercentralincisors extractedforperiodontalreasons,andthestudywasapproved bytheInstitutionalResearchEthicsCommittee.Teethwere collected after receiving verbalconsent and storedin0.5% chloraminesolutionat4◦Cforaweekfollowedbyimmersion indistilled waterat4◦Cuntilbondingprocedures.The cri-teriaforstudy inclusionwereabsenceofpreviouschemical treatment,cariesandbuccalsurfacecracksandrestorations. HealthyteethcomposedgroupH30.Mildtomoderated fluo-rosedteethwereselectedbyconsensusbetweentwoobservers accordingtotheThylstrup andFejerskovIndex(ITF)scores 3–4,andrandomlyallocatedtogroupsF30andF60.28
Beforebonding,buccalsurfaceswerecleanedwitha mix-tureofwaterandnon-fluoridepumice,thoroughlyrinsedwith watersprayandair-dried.
Theenamelofbuccalsurfacespecimenswasetchedwith 37% phosphoric acid gel (TransbondTM XT EtchingGel, 3M
Unitek,Monrovia,EUA),for30sforgroupH30andF30,and 60sforgroupF60.Allteethwererinsedwithwatersprayfor 15sanddriedwithoil-freecompressedairfor5s,until charac-teristicfrostywhiteenameletchedappearancewaspresent.
Metalbrackets(VictorySeriesTMStandartedgewiseBracket
Table1–Adhesiveremnantindex(ARI).
Index Definition
0 Noadhesiveremainedonthetoothinthebondingarea 1 Lessthan50%oftheadhesiveremainedonthetooth 2 50%ormoreoftheadhesiveremainedonthetooth 3 100%oftheadhesiveremainedonthetooth,witha
distinctimpressionofthebracketmesh
TransbondXT (3MUnitek,Monrovia,USA)accordingtothe
manufacturer’sinstructions.Athinuniformlayerofadhesive
primerwas appliedwith amicrobrush onthe etched
buc-calenamelsurface.Thelightcuredorthodonticadhesivewas
appliedonthebaseofthebracketandthiswasimmediately
positionedontothetoothsurfaceandpressedfirmlyinthe
desiredposition.Excessiveresinwasgentlyremovedwitha
dentalprobeand thereaftercured(LED CV-218,Technoflux,
Barcelona,Spain)withanoutputof1200mW/cm2for10s(5s
ateachofthemesialanddistalbracketedge).
Thespecimenswere setinself-curedacrylicblock,
ther-mocycled(5–55◦C,500cycles),andstoredindistilledwaterat
37◦Cfor7days,beforetestedinshear.
Bond strengths were measured on a universal testing
machine(Instronmodel4502,InstronLtd.,Bucks,England),
using awire loop applied under the gingival wings ofthe
bracket,inordertoinducegingival-oclusalshearstressatthe
adhesiveinterface.Shearbondstrength(SBS)testswere
per-formedatacrossheadspeedof1mm/minandloadcellof1kN,
untilfailureoccurred.Failureloadvalues(N)wererecorded
and convertedinto megapascals(MPa), dividingthe failure
loadbythesurfaceareaofthebracketbase.
Afterdebonding,teethandbracketswereexaminedwith
a stereomicroscope (Meiji Techno, model EMZ-8TR, Meiji
TechnoCo.Lda, Saitama,Japan)atmagnificationof20×,to
assesstheamountofadhesiveremainingontheteethandthe
failuremodewasscoredaccordingtotheadhesiveremnant
index(ARI)(Table1).29,30
DatawerestatisticallyanalyzedusingIBMSPSSStatistics 20software(SPSSInc.,Chicago,IL,USA).Afterassessing nor-malityandhomoscedasticitywithKolmogorov–Smirnovand Levene’stests,SBSdataweresubmittedtoone-wayANOVA, followed by Tukey post hoc tests. Kruskal–Wallis followed byMann–Whitney withBonferroni correction nonparamet-rictestswere usedtoanalyzefailuremodedata.Statistical significancewasidentifiedatalpha=0.05.
Results
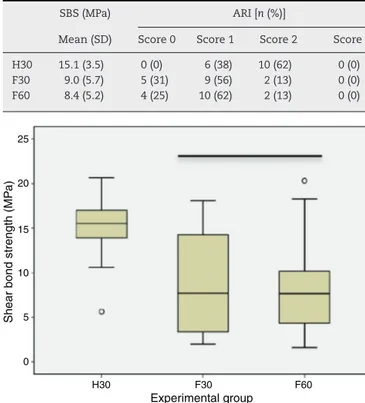
ThemeanSBSrangedfrom 8.4MPaforthe fluorosedteeth etchedfor60s(F60),to15.1MPaforH30withhealthy
speci-mens(Table2).Accordingto1-wayANOVAandTukeyposthoc
tests,meanSBSyieldedinbothgroupswithfluorosedteeth (F30andF60)weresignificantly(p<0.05)lowerthanthatwith non-fluorosedteeth(H30).Nosignificant(p=0.978)difference wasfoundbetweenF30andF60,thetwogroupswithfluorosed teeth(Fig.1).
The distribution of failure ARI score by experimental groupsispresentedinTable2andFig. 2. Nocohesive fail-ures(score3)wereobserved.Failuremodewaspredominantly
Table2–Shearbondstrengthandadhesiveremnant
index(ARI)data.
SBS(MPa) ARI[n(%)]
Mean(SD) Score0 Score1 Score2 Score3 H30 15.1(3.5) 0(0) 6(38) 10(62) 0(0) F30 9.0(5.7) 5(31) 9(56) 2(13) 0(0) F60 8.4(5.2) 4(25) 10(62) 2(13) 0(0) 25 20 15 10
Shear bond strength (MP
a) 5 0 H30 F30 Experimental group F60
Fig.1–Box-plotofshearbondstrengths(MPa)[horizontal lineindicatesstatisticalsimilargroups(p≥0.05)].
mixed(scores1and2)buttheARIscoreofH30non-fluorosed
teethwassignificantly(p<0.05)higherthanthoseachievedin
fluorosedteeth(F30andF60).Adhesivefailureswerefound
onlyforF30andF60.
Discussion
Bondingorthodontic brackets to fluorosedteethremains a
difficulttaskdue tothe loweracidic solubility of
fluoroap-atite,present athigh concentrationintheexternalenamel
layer.18–20Thereductionofenamelsolubilityisrelatedtothe
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100% H30 F30 F60 ARI scores 3 2 1 0
Fig.2–Adhesiveremnantindex(ARI)scoresdistribution byexperimentalgroups[horizontallineindicatesstatistical similargroups(p≥0.05)].
presenceoflargerapatitecrystals,bettercrystallinity,andthe bufferingactionoffluoridereleasedbyenamelcrystalsduring initialstagesofetching.31
Thepresent study was designed toevaluatethe effects of fluorosis and etching time on shear bond strengths of orthodonticbrackets.
Thermalcyclingwasperformed,accordingtotheISO11405 specificationsfortestingadhesiontotoothstructure.This pro-cedurecouldbecontroversialbutallspecimensweretreated inthesameway,althoughithasbeenstatedthat500cycles donotstandforasufficientamountofaging.32,33
Significantly lower bracket bond strength values were foundinthefluorosedenamelthanthoseachievedin non-fluorosedteeth.Consequently,thefirstnullhypothesistested wasrejected.These resultsare inagreementwithprevious studies18,20,24;neverthelesssomeothersshowednoeffectof
fluorosisonbondstrength.22,26 Thisinconsistencyand
con-flictingresultsmaybeexplainedbythedifferencesobserved betweenthefluorosisseverityoftheteethusedinthe differ-entstudies.Itwasshownthattheincreaseoffluorosisseverity leadstoalowerbondstrength.20,34Forthisstudy,mildto
mod-eratefluorosedteeth(TFI=3–4)werecollectedintheAzores Islands(São Miguel),afluorosis endemic area,where fluo-ridecontentsindrinkingwaterreachesconcentrationshigher than1ppm.35
Inordertoovercomethelowerenamelsolubilityinteeth withfluorosis,someauthorsadvocatetheextensionofetching time.20–22Ithasbeenrecommendedtoetchhealthyteethfor
15–30s,enamelwithmildandmoderatefluorosisfor30s,and etchingenamelwithseverefluorosisatleastfor60–90s.13,36,37
Inthe present investigation,the second nullhypothesis testedcouldnotberejected.Anincreaseinetchingtime,from 30to60s,onmildtomoderatefluorosedteethwasnotenough toachieve bondstrengths ashigh astheonesyieldedwith non-fluorosedteeth.Apreviousstudy,alsofoundnoincrease inbracketbondstrengthtoteethwithmoderateandsevere fluorosis,byextendingtheetchingtimefrom15sto150s.20
However, obtaining higher bond strengths may not be a critical issue. The adhesion achieved should be enough towithstandthe stressproduced inclinical situations,but extremely high bond values may induce enamel fractures duringbracketdebondingand increasethedifficulty ofthe adhesiveremnantsremoval, atthe endofthetreatment.20
Ithasbeen suggestedthatobtainingbracketbondstrength valuesrangingfrom 6to8MPawillbesufficientto ensure agoodclinicalperformance.38Regardlessofthelowerbond
strengthobservedwithfluorosedteethwhencomparedwith non-fluorosedteeth,themeanbracketbondvaluesachieved inallexperimentalgroupswerehigherthanthosementioned above. Nonetheless, it is known that several factors may influencethebondvalues,suchasthemechanicaltest config-urationsused.39–41Thelackofuniformityinthemethodology
ofpreviouspublicationslimitsthecomparabilityofthebond values between studies and their extrapolation to clinical behavior.
ThefailuremodeobservedwasinaccordancewiththeSBS values.The25–30%ofadhesive failuresfoundin fluorosed groupsmaysuggestthatinthesegroupstheunionbetween theenamelandtheorthodonticadhesiveisnotsostrongas inhealthyteeth.Thisresultwasalsoconsistentwithprevious
studieswherehigherARIscoresareobservedwithincreased bondstrengthvalues.20,24,27
Further studies should be performed to evaluate the influence ofdifferent types of fluorosis, etching time and orthodonticadhesivesonbracketbondstrength,andto eval-uatelong-termdurabilityofthebond.Clinicalstudiesarealso desirable.
Conclusion
Orthodonticbracketsadhesiontotoothenamelisnegatively influencedbydentalfluorosis.Doublingtheetchingtimedoes notincreasetheadhesionoforthodonticbracketstofluorosed enamel.
Ethical
disclosures
Protectionofhumanandanimalsubjects.Theauthorsdeclare thatnoexperimentswereperformedonhumansoranimals forthisinvestigation.
Confidentiality ofdata.Theauthors declarethatnopatient dataappearinthisarticle.
Righttoprivacyandinformedconsent.Theauthorsdeclare thatnopatientdataappearinthisarticle.
Conflicts
of
interest
Theauthorshavenoconflictsofinteresttodeclare.
Acknowledgments
Theauthorswishtothank3MUnitekforprovidingthe mate-rialsforthisstudy.ThisworkwasperformedatUICOB,R&D unitno.4062ofFCT.
r
e
f
e
r
e
n
c
e
s
1.BuzalafMA,LevySM.Fluorideintakeofchildren:
considerationsfordentalcariesanddentalfluorosis.Monogr
OralSci.2011;22:1–19.
2.PetersenPE,LennonMA.Effectiveuseoffluoridesforthe
preventionofdentalcariesinthe21stcentury:theWHO
approach.CommunityDentOralEpidemiol.2004;32:
319–21.
3.WheltonH,CrowleyE,O’MullaneD,DonaldsonM,KelleherV,
CroninM.Dentalcariesandenamelfluorosisamongthe
fluoridatedandnon-fluoridatedpopulationsintheRepublic
ofIrelandin2002.CommunityDentHealth.2004;21:
37–44.
4.SakaguchiRL,PowersJM.Craig’srestorativedentalmaterials.
13thed.Philadelphia:ElsevierMosby;2012.
5.SarvaiyaBU,BhayyaD,AroraR,MehtaDN.Prevalenceof
dentalfluorosisinrelationwithdifferentfluoridelevelsin
drinkingwateramongschoolgoingchildreninSaradatehsil
ofUdaipurdistrict,Rajasthan.JIndianSocPedodPrevDent.
2012;30:317–22.
6.AkpataES.Occurrenceandmanagementofdentalfluorosis.
7. WangC,GaoY,WangW,ZhaoL,ZhangW,HanH,etal.A
nationalcross-sectionalstudyoneffectsoffluoride-safe
watersupplyontheprevalenceoffluorosisinChina.BMJ
Open.2012;2:e001564.
8. Beltrán-AguilarED,BarkerL,DyeBA.Prevalenceandseverity
ofdentalfluorosisintheUnitedStates,1999–2004.NCHSData
Brief.2010;53:1–8.
9. MeneghimMdeC,TagliaferroEP,TenganC,MeneghimZM,
PereiraAC,AmbrosanoGM,etal.Trendsincariesexperience
andfluorosisprevalencein11-to12-year-oldBrazilian
childrenbetween1991and2004.OralHealthPrevDent.
2006;4:193–8.
10.KhanA,MoolaMH,Cleaton-JonesP.Globaltrendsindental
fluorosisfrom1980to2000:asystematicreview.SAfrDentJ.
2005;60:418–21.
11.DenbestenP,LiW.Chronicfluoridetoxicity:dentalfluorosis.
MonogrOralSci.2011;22:81–96.
12.AobaT,FejerskovO.Dentalfluorosis:chemistryandbiology.
CritRevOralBiolMed.2002;13:155–70.
13.Al-SugairMH,AkpataES.Effectoffluorosisonetchingof
humanenamel.JOralRehabil.1999;26:521–8.
14.WaidyasekeraK,NikaidoT,WeerasingheD,WatanabeA,
IchinoseS,TayF,etal.Whydoesfluoroseddentineshowa
highersusceptibilityforcaries:anultra-morphological
explanation.JMedDentSci.2010;57:17–23.
15.FejerskovO,LarsenMJ,RichardsA,BaelumV.Dentaltissue
effectsoffluoride.AdvDentRes.1994;8:15–31.
16.BronckersAL,LyaruuDM,DenBestenPK.Theimpactof
fluorideonameloblastsandthemechanismsofenamel
fluorosis.JDentRes.2009;88:877–93.
17.BuonocoreMG.Asimplemethodofincreasingtheadhesion
ofacrylicfillingmaterialstoenamelsurfaces.JDentRes.
1955;34:849–53.
18.AdanirN,TürkkahramanH,Yalc¸inGüngörA.Effectsof
adhesionpromotersontheshearbondstrengthsof
orthodonticbracketstofluorosedenamel.EurJOrthod.
2009;31:276–80.
19.Torres-GallegosI,Zavala-AlonsoV,Pati ˜no-MarínN,
Martinez-Casta ˜nonGA,AnusaviceK,Loyola-RodríguezJP.
Enamelroughnessanddepthprofileafterphosphoricacid
etchingofhealthyandfluoroticenamel.AustDentJ.
2012;57:151–6.
20.Silva-BenítezEL,Zavala-AlonsoV,Martinez-CastanonGA,
Loyola-RodriguezJP,Pati ˜no-MarinN,Ortega-PedrajoI,etal.
Shearbondstrengthevaluationofbondedmolartubeson
fluoroticmolars.AngleOrthod.2013;83:152–7.
21.AteyahN,AkpataE.Factorsaffectingshearbondstrengthof
compositeresintofluorosedhumanenamel.OperDent.
2000;25:216–22.
22.Ng’ang’aPM,OgaardB,CruzR,ChindiaML,AasrumE.Tensile
strengthoforthodonticbracketsbondeddirectlytofluorotic
andnonfluoroticteeth:aninvitrocomparativestudy.AmJ
OrthodDentofacialOrthop.1992;102:244–50.
23.MandallNA,MillettDT,MattickCR,HickmanJ,Worthington
HV,MacfarlaneTV.Orthodonticadhesives:asystematic
review.JOrthod.2002;29:205–10.
24.GungorAY,TurkkahramanH,AdanirN,AlkisH.Effectsof
fluorosisandselfetchingprimersonshearbondstrengthsof
orthodonticbrackets.EurJDent.2009;3:173–7.
25.NobleJ,KaraiskosNE,WiltshireWA.Invivobondingof
orthodonticbracketstofluorosedenamelusinganadhesion
promotor.AngleOrthod.2008;78:357–60.
26.IsciD,SahinSaglamAM,AlkisH,Elekdag-TurkS,TurkT.
Effectsoffluorosisontheshearbondstrengthoforthodontic
bracketsbondedwithaself-etchingprimer.EurJOrthod.
2011;33:161–6.
27.SumaS,AnitaG,ChandraShekarBR,KalluryA.Theeffectof
airabrasionontheretentionofmetallicbracketsbondedto
fluorosedenamelsurface.IndianJDentRes.2012;23:230–5.
28.ThylstrupA,FejerskovO.Clinicalappearanceofdental
fluorosisinpermanentteethinrelationtohistologicchanges.
CommunityDentOralEpidemiol.1978;6:315–28.
29.ArtunJ,BerglandS.Clinicaltrialswithcrystalgrowth
conditioningasanalternativetoacid-etchenamel
pretreatment.AmJOrthod.1984;85:333–40.
30.GodinhoJ,OliveiraSSA,JardimL.Comparisonoftwo
self-etchingprimersandeffectofsalivacontaminationon
shearbondstrengthoforthodonticbrackets.RevPort
EstomatolCirMaxilofac.2007;48:197–203.
31.ClarksonJJ,HardwickK,BarmesD,RichardsonL.
Internationalcollaborativeresearchonfluoride.JDentRes.
2000;79:893–904.
32.GaleMS,DarvellBW.Thermalcyclingproceduresfor
laboratorytestingofdentalrestorations.JDent.1999;27:89–99.
33.DeMunckJ,VanLanduytK,PeumansM,PoitevinA,
LambrechtsP,BraemM,etal.Acriticalreviewofthe
durabilityofadhesiontotoothtissue:methodsandresults.J
DentRes.2005;84:118–32.
34.WeerasingheDS,NikaidoT,WettasingheKA,AbayakoonJB,
TagamiJ.Micro-shearbondstrengthandmorphological
analysisofaself-etchingprimeradhesivesystemtofluorosed
enamel.JDent.2005;33:419–26.
35.CordeiroS,CoutinhoR,CruzJV.Fluoridecontentindrinking
watersupplyinSãoMiguelvolcanicisland(Azores,Portugal).
SciTotalEnviron.2012;432:23–36.
36.JohnstonCD,BurdenDJ,HusseyDL,MitchellCA.Bondingto
molars–theeffectofetchtime(aninvitrostudy).EurJ
Orthod.1998;20:195–9.
37.JohnstonCD,HusseyDL,BurdenDJ.Theeffectofetch
durationonthemicrostructureofmolarenamel:aninvitro
study.AmJOrthodDentofacialOrthop.1996;109:531–4.
38.ReynoldsIR.Areviewofdirectorthodonticbonding.BrJ
Orthod.1975;2:171–8.
39.KlockeA,Kahl-NiekeB.Influenceofforcelocationin
orthodonticshearbondstrengthtesting.DentMater.
2005;21:391–6.
40.KatonaTR,LongRW.Effectofloadingmodeonbondstrength
oforthodonticbracketsbondedwith2systems.AmJOrthod
DentofacialOrthop.2006;129:60–4.
41.KlockeA,Kahl-NiekeB.Effectofdebondingforcedirectionon
orthodonticshearbondstrength.AmJOrthodDentofacial
Orthop.2006;129:261–5.
View publication stats View publication stats