RevBrasAnestesiol.2015;65(5):367---370
REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiologywww.sba.com.br
SCIENTIFIC
ARTICLE
Ketamine---propofol
sedation
in
circumcision
Handan
Gulec
∗,
Saziye
Sahin,
Esra
Ozayar,
Semih
Degerli,
Fatma
Bercin,
Osman
Ozdemir
KeciorenTrainingHospital,Ankara,Turkey
Received23January2014;accepted10March2014 Availableonline31March2014
KEYWORDS
Ketamine---propofol; Sedation;
Circumcision
Abstract
Backgroundandobjective: Tocomparethetherapeuticeffectsofketaminealoneorketamine pluspropofolonanalgesia,sedation,recoverytime,sideeffectsinpremedicatedchildrenwith midazolam---ketamine---atropinwhoarepreparedcircumcisionoperation.
Methods:60AmericanSocietyofAnaesthesiologistsphysicalstatusI---IIchildren,agedbetween 3and9years,undergoingcircumcision operationsundersedation wererecruitedaccording toarandomizeanddouble-blindinstitutionalreviewboard-approvedprotocol.Patientswere randomizedintotwogroupsviasealedenvelopeassignment.Bothgroupswereadministered amixtureofmidazolam0.05mg/kg+ketamine3mg/kg+atropine0.02mg/kgintramuscularly in the presence ofparents in the pre-operative holding area. Patients were induced with propofol---ketamineinGroupIorketaminealoneinGroupII.
Results:Inthebetween-groupcomparisons,age,weight,initialsystolicbloodpressure,a dif-ferenceintermsoftheinitialpulseratewasobserved(p>0.050).Initialdiastolicbloodpressure andsubsequentserialmeasurementsof5,10,15,20thmin,systolicbloodpressure,diastolic bloodpressureandpulserateinketaminegroupweresignificantlyhigher(p<0.050).
Conclusion: Propofol-ketamine (Ketofol) provided better sedation quality andhemodynamy than ketamine alone in pediatric circumcision operations. We did not observe significant complicationsduringsedationinthesetwogroups.Therefore,ketofolappearstobeaneffective andsafesedationmethodforcircumcisionoperation.
© 2014SociedadeBrasileirade Anestesiologia.Publishedby ElsevierEditoraLtda.Allrights reserved.
PALAVRAS-CHAVE
Cetamina-propofol; Sedac¸ão;
Circuncisão
Sedac¸ãocomcetamina-propofolemcircuncisão
Resumo
Justificativaeobjetivo: Compararosefeitosterapêuticosdacetaminaisoladaoucombinac¸ão decetamina-propofolem analgesia,sedac¸ão,tempoderecuperac¸ãoeefeitoscolateraisem crianc¸aspré-medicadascommidazolam-cetamina-atropina programadasparaprocedimentos decircuncisão.
∗Correspondingauthor.
E-mail:[email protected](H.Gulec). http://dx.doi.org/10.1016/j.bjane.2014.03.002
368 H.Gulecetal.
Métodos: Sessentacrianc¸as,estadofísicoASAI-II(deacordocomaclassificac¸ãodaSociedade AmericanadeAnestesiologistas),comidadesentretrêsenoveanos,submetidasa procedimen-tosdecircuncisãosobsedac¸ão,foramrecrutadasdeacordocomumprotocoloderandomizac¸ão duplo-cegoaprovadopeloConselhodeRevisãoInstitucional.Ospacientesforamrandomizados ealocadosemdoisgruposcomousodométododeenvelopeslacrados.Ambososgrupos rece-beramumamisturademidazolam0,05mgkg−1+cetamina3mgkg−1+atropina0,02mgkg−1por viaintramuscular,napresenc¸adospaisnaáreadeintervenc¸õespré-operatórias.Ainduc¸ãofoi realizadacompropofol-cetaminanoGrupoIoucetaminaisoladanoGrupoII.
Resultados: Nascomparac¸ões entreos gruposforam observadasaidade, opeso,apressão arterialsistólicainicialeadiferenc¸aemrelac¸ãoàtaxadepulsoinicial(p>0,050).Apressão arterialdiastólicainicialeasmensurac¸õesseriadassubsequentesnosminutos5,10,15e20da pressãoarterialsistólica,pressãoarterialdiastólicaetaxadepulsodogrupocetaminaforam significativamentemaiores(p<0,050).
Conclusão:Cetamina-propofol(cetofol)proporcionoumelhorqualidadedesedac¸ãoe estabil-idadehemodinâmicaquecetaminaisoladaemcirurgiaspediátricasdecircuncisão.Nãoforam observadascomplicac¸õessignificativasduranteasedac¸ãonosdoisgrupos.Portanto, cetofol pareceserummétododesedac¸ãoeficazeseguroparaprocedimentosdecircuncisão. ©2014SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
Introduction
Circumcisionisapainfulandstressfuloutpatientprocedure in children.1 An ideal anesthetic agent for this
opera-tionshouldprovideadequateanalgesia,amnesia,sedation,
immobilityand shortrecovery timewhile shouldbeavoid
cardiovascularandrespiratorydepression,nausea-vomiting
andagitation.
The combination of propofolandketamine (ketofol)in
the same syringe successfully produced adequate action
for oncologic procedures,2 interventional radiology,3
car-diaccatheterization,4 hematologicaldiseases5 inchildren.
Opiods, midazolam, ketamine, propofol and
dexmedeto-midinearethegenerallypreferredsedoanalgesic agents.6
Propofol, as an intravenous anesthetic, is applied as an
intermittentinfusion for sedation inspinal anesthesia.7 If
the long infusion duration is ignored, waking is provided
atthetimeofterminatingtheinfusion.8 Nonetheless,the
use of propofol may causecardiovascular and respiratory
system depression.9 Ketamine may be considered
effec-tivewithdirectsympatheticstimulationandnorepinephrine
byreuptakeinhibitionfromthepostganglionicsympathetic
system.10Italsoinducesfunctionaldissociationbetweenthe
limbic andcortical system often referred to as
‘dissocia-tiveanesthesia’.Protectiveairwayreflexesaremaintained
duringsedationandthehightherapeuticindexofketamine
makesthisdrugsuitableforregionalanesthesia.11
Ketofol is prepared as a 1:1 mixture of ketamine
10mg/mLandpropofol10mg/mLmixedina10mLor20mL
syringeandisconstitutedasolutionwhichis 5mgeachof
ketamineandpropofolineachmililiters.
Inthisstudyweaimedtoevaluatetheeffectsofketamine
alone or ketamine plus propofol on analgesia, sedation,
recovery time,and side effects in premedicated children
withmidazolam---ketamine---atropinwhoareundergoing
cir-cumcisionoperation.
Materials
and
methods
60 ASA physical status I---II children, aged between 3 and
9years,undergoingcircumcisionoperationsundersedation
wererecruitedaccordingtoarandomizeanddouble-blind
institutionalreviewboard-approvedprotocol.Patientswith
clinicallysignificantneurological,respiratory,
cardiovascu-larandpsychiatricdiseaseswereexcludedfromthestudy.
Patients were randomized into two groups via sealed
envelopeassignment.Bothgroupswereadministereda
mix-tureofmidazolam0.05mg/kg+ketamine3mg/kg+atropine
0.02mg/kg intramuscularly in the presence of parents
in the pre-operative holding area. After 5min, children
were included in the operating room. Monitoring for the
procedure consistedof threeleadECG, SpO2 with
plethy-smographyandnoninvasivebloodpressure.Afterplacement
of an intravenous cannula, patients were induced with
propofol---ketamine inGroup Ior ketamine aloneinGroup
II. Medication dosages, administrationtimes, total
proce-duretime,vitalsigns(non-invasivebloodpressure,oxygen
saturationviapulseoxymetry,heartrate,respirationrate),
side effects, and sedation scores were recorded by the
same anesthesiologist at the beginning of the procedure
andafterinductionat5minandthenevery5minuntilthe
end ofthe procedure.The sedation levelsofthe patients
were assessed by Ramsay sedation score; induction and
maintenancewereappliedtotargetscoreof 2or 3.
Prilo-caine was injected for the dorsal penile nevre block by
the surgeon and the procedure wasstarted. Through the
circumcisionprocedure,whenthedrugdoseswerenot
Ketamine---propofolsedationincircumcision 369
thepatientmoved,additionalbolusesofpropofol---ketamine
wasadministeredinGroupIorketaminewasadministered
in Group II. Supplemental drugrequirements were noted.
Wealsonotedtheadversesymptomsincludingdesaturation
(SpO2<%90), apnea (>15s), rash, agitation,vomiting, and
increasedsecretions.All patientsreceivedoxygen
supple-mentationvianasalcannulaorbyblow-bywithagasflow
rate of 2L/min throughout the procedure. All operations
wereperformedbythesamesurgeon.
The Ramsay sedation scale used to determine the
responsetosedationandanalgesiaisgradedas5,deep
seda-tion:1,patientawake:6,patientasleepwithnoresponse
toanystimuli.
When the procedure was complete, the patients were
transferredtotherecovery roomandtheir levelsof
seda-tion,dischargetime,andadverseevents wereassessedat
5min intervals.Discharge criteriawereasfollows:airway
patentwithadequateoxygenation;awakeoreasilyaroused
(minimaltactileor vocal stimulationmightbenecessary);
swallowingreflexpresent,demonstratingabilitytoswallow
clearliquidswhileprotectingtheairway;presedationlevel
ofresponsivenessachieved.
Statistical analysis was made using Statistical Package
fortheSocialSciences15.0 (SPSS15.0,SPSSInc.,Chicago,
IL) software. All quantitative data were analyzed with
the Kolmogorov---Smirnov test to show distribution. Data
withnormaldistributionwereexpressedasmean±standard
deviationanddatawithnon-normaldistributionasmedian
(inter quartile range). According to the distribution
sta-tus of quantitative data independent sampling t-test or
Mann---Whitney U-test was used. The Chi-square test was
usedtocomparecategoricaldata.Aconfidenceintervalof
95% was defined anda value of p<0.05 was accepted as
statisticallysignificant.
Results
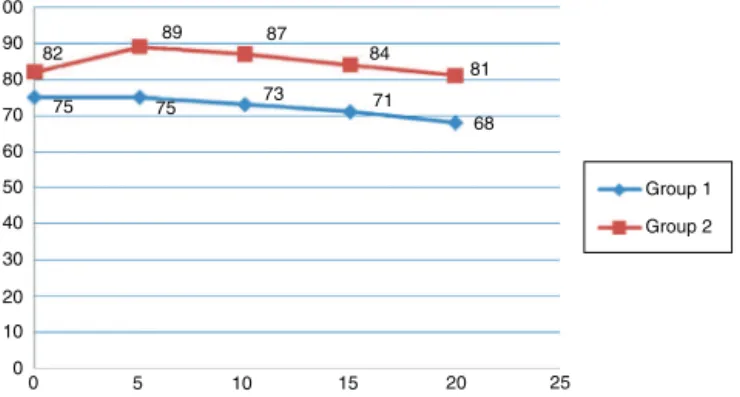
Inthebetween-groupcomparisons,age,weight,initial
sys-tolic blood pressure, a difference in terms of the initial
pulserate wasobserved (p>0.050). Initial diastolicblood
pressureandsubsequentserialmeasurementsof5,10,15,
20thmin, systolic blood pressure (Fig. 1), diastolic blood pressure(Fig.2)andpulserate(Fig.3)in ketaminegroup weresignificantlyhigher(p<0.050).Follow-uptimeinterms
ofthe need foradditionalanalgesic in ketofolgroupused
132 130 128 126 124 122 120 118 116 114 112
0 5 10 15 20 25
113 115
115 118
121 124
131
129 128
127
Group 1 Group 2
Figure 1 Comparison of systolic blood pressure levels betweengroups.
100 90 80 70 60 50 40 30 20 10 0
0 5 10 15 20 25
68 81 84 87 89
82
75 75 73 71
Group 1 Group 2
Figure 2 Comparison of diastolic blood pressure levels betweengroups.
160
140
111 108
106
122 129
109 109
136 138
115 120
100
80
60
40
20
0
0 5 10 15 20 25
Group 1 Group 2
Figure3 Comparisonofheartratesbetweengroups.
significantlyfeweranalgesics(p<0.050).Bothgroupswere similarintermsofcomplications(p>0.050).
Discussion
AccordingtoAmericanSociety of Anaesthesiologists(ASA)
data(2006),highdosesofsedationhave beenreportedto
lead torespiratory depression and are an important
rea-sonforunexplained malpractice.12 Anesthesiaisabalance
betweenthe patient’s state of wakefulness and the need
foranestheticmedication.Ifaninsufficientdoseis adminis-tered,thepatient’swakefulnessincreaseswhileahighdose
causeshemodynamicinstability, prolongedtimetowaking
and other complications.13 In relation tothe response to
sedationandanalgesia,it wasdecidedtouse theRamsay
scalein thecurrent study becauseitis easytoapply.14---16
Theidealsedativeagentforregionalanesthesiashouldhave
a rapid onset of action, produce a level of sedation
suf-ficient for patientcomfort, and have a short duration of
action.10 Generally, the intermittent intravenous
applica-tioninsedation does notallow for theadjustment ofthe
plasmaconcentrationlevelofthemedicationandextends
thetimetowaking.17
A pharmacological disadvantage of propofol is its
rel-atively narrow therapeutic range. Unlike opioids and
benzodiazepines,an antagonistisnotavailable toreverse
theeffects.Despiteitshighpotentialtoinducerespiratory depressionandcardiovascularinstability,propofolhasbeen routinelyadministeredbyanesthesiologist.18
In this prospective, randomized study, we compared
370 H.Gulecetal.
(ketofol) and ketamine alone for circumcision operation
underlocalanesthesiavia penileblock.Ourstudyshowed
that ketofol supplied more effective and safety sedation
thanketaminealoneinchildren.
Circumcisionisapainfuloperationanditusuallyis
per-formed in children.1 Many studies are performed on the
methodof anesthesiain this operation andmost of them
involvedpenileblockandcaudalblockwithorwithout seda-tion/generalanesthesia.11
The clinicaleffectsof propofolandketamineare
com-plementary. While propofol provides hypnosis, ketamine
performsanalgesiaandstablehemodynamicactivity,19 the
combinationofketamineandpropofolisrenamed‘‘ketofol’’
andiscurrentlypopularagentforproceduralsedation.2---5
David and Shipp20 comparedthe frequency of
respira-tory depression during emergency department procedural
sedation with ketamine plus propofol versus propofol
alone. Ketamine was applied only one as a 0.5mg/kg
via intravenous route at the beginning procedure, not
was prepared ketofol. And they arrived at the
conclu-sion of ketamine/propofol did not reduce the incidence
of respiratorydepression but resulted in greater provider
satisfaction,lesspropofoladministrationandperhaps
bet-ter sedation quality. In a study by Shah et al.,21 which
compared with ketamine alone and the combination of
ketamineandpropofolforpediatricorthopedicreductions,
itwasshownthatketamine/propofolcombinationproduced
slightlyfasterrecoverieswhilealsodemonstratingless
vomi-ting, higher satisfaction scores and similar efficacy and
airwaycomplications.Bothgroups didnotexperience
sig-nificantrespiratorydepressionandketofolgrouphadbetter
sedationlevelsthanketaminegroupinourstudy.Wefound
thatketofol providedmore acceptable hemodynamy than
ketaminealone. Butwe did notstudy for thesedation or
recoverytime.
In conclusion, ketofolprovided better sedation quality
andhemodynamythanketaminealoneinpediatric
circumci-sionoperations.Wedidnotobservesignificantcomplications
during in these two groups. Ketofol obtained by mixing
ketaminewithpropofolprovidedappropriateanalgesiaand
sedation.
Our results indicate that intravenously administered
ketofolproducesfasterrecoverytimeandsafesedation.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.ChoiWY,IrwinMG,HuiTW, etal.EMLAcream versusdorsal penilenerveblockforpostcircumcisionanalgesiainchildren. AnesthAnalg.2003;96:396---9.
2.AouadMT,MoussaAR,DagherCM,etal.Additionofketamine topropofolforinitiationofproceduralanesthesiainchildren
reducespropofolconsumptionandpreserveshemodynamic sta-bility.ActaAnaesthesiolScand.2008;52:561---5.
3.AydinErdenI,GulsunPamukA,AkinciSB,etal.Comparisonof propofol---fentanylwithpropofol---fentanyl---ketamine combina-tioninpediatricpatientsundergoinginterventionalradiology procedures.PediatrAnesth.2009;19:500---6.
4.Akin A, Esmaoglu A, Guler G, et al. Propofol and propofol---ketamine in pediatric patients undergoing cardiac catheterization.PediatrCardiol.2005;26:553---7.
5.daSilvaPSL,deAguiarVE,WaisbergDR,etal.Useofketofol forproceduralsedationandanalgesiainchildrenwith hemato-logicaldiseases.PediatrInt.2011;53:62---7.
6.Demiraran Y, Korkut E, Tamer A, et al. The comparison of dexmedetomidineandmidazolamusedforsedationofpatients duringupperendoscopy:aprospective,randomizedstudy.Can JGastroenterol.2007;21:25---9.
7.Murphy PG, Myers DS, Davies MJ, et al. The antioxidant potential of propofol (2,6-diisopropylphenol). Br J Anaesth. 1992;68:613---8.
8.MikawaK,AkamatsuH,NishinaK,etal.Propofolinhibitshuman neutropilfunctions.AnesthAnalg.1998;87:695---700.
9.Ozkan-Seyhan T, Sungur MO, Senturk E, et al. BIS quided sedation with propofol during spinal anaesthesia: influence ofanaesthetic level onsedation requirement. Br JAnaesth. 2006;6:645---9.
10.IkedaT,KazamaT,SesslerDI,etal.Inductionofanesthesiawith ketaminereducesthemagnitudeofredistributionhypothermia. AnesthAnalg.2001;93:934---8.
11.SerourF,CohenA,MandelbergA,etal.Dorsalpenilenerveblock inchildrenundergoingcircumcisioninaday-caresurgery.Can JAnaesth.1996;43:954---8.
12.BhanankerSM,PosnerKL,CheneyFW,etal.Injuryand liabil-ityassociatedwithmonitoredanesthesiacare:aclosedclaims analysis.Anesthesiology.2006;104:228---34.
13.BruhnJ,MylesPS,SneydR,etal.Depthofanaesthesia moni-toring:what’savailable,what’svalidatedandwhat’snext?BrJ Anaesth.2006;97:85---94.
14.HesselgardK,LarssonS,RomnerB,etal.Validityandreliability oftheBehaviouralObservationalPainScaleforpostoperative painmeasurementinchildren1---7years ofage.Pediatr Crit CareMed.2007;8:102---8.
15.Suraseranivongse S, Santawat U, Kraiprasit K, et al. Cross-validationofcompositepainscaleforpreschoolchildrenwithin 24hoursofsurgery.BrJAnaesth.2001;87:400---5.
16.DeJongheB, CookD,Appere DeVecchiC,et al.Usingand understandingsedationscoringsystems:asystematicreview. IntensiveCareMed.2000;26:275---85.
17.HohenerD,BlumenthalS,BorgeatA.SedationandregionalIin theadultpatient.BrJAnaesth.2008;100:8---16.
18.FredetteME, LightdaleJR. Endoscopic sedation in pediatric practice.GastrointestEndoscClinNAm.2008;18:739---51. 19.SakaiT,SinghH,MiWD,etal.Theeffectofketamineon
clin-icalendpoints ofhypnosisand EEGvariables duringpropofol infusion.ActaAnaesthesiolScand.1999;43:212---6.
20.DavidH,ShippJ.Arandomizedcontrolledtrialofketamine/ propofolversuspropofolaloneforemergencydepartment pro-ceduralsedation.AnnEmergMed.2011;57:435---41.