w w w . r b o . o r g . b r
Original
article
Q-angle
in
patellofemoral
pain:
relationship
with
dynamic
knee
valgus,
hip
abductor
torque,
pain
and
function
夽
Gabriel
Peixoto
Leão
Almeida
a,b,∗,
Ana
Paula
de
Moura
Campos
Carvalho
e
Silva
a,
Fábio
Jorge
Renovato
Franc¸a
a,
Maurício
Oliveira
Magalhães
a,
Thomaz
Nogueira
Burke
a,
Amélia
Pasqual
Marques
aaDepartmentofPhysiotherapy,SpeechTherapyandOccupationalTherapy,FaculdadedeMedicina,UniversidadedeSãoPaulo,SãoPaulo,
SP,Brazil
bDepartmentofPhysiotherapy,FaculdadedeMedicina,UniversidadeFederaldoCeará,Fortaleza,CE,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received22March2015 Accepted28May2015
Availableonline9February2016
Keywords: Knee
Patellofemoralpainsyndrome Manualstrengthdynamometer
a
b
s
t
r
a
c
t
Objective:Toinvestigatetherelationshipbetweentheq-angleandanteriorkneepain sever-ity, functionalcapacity, dynamickneevalgus andhip abductortorque inwomen with patellofemoralpainsyndrome(PFPS).
Methods:Thisstudyincluded22womenwithPFPS.Theq-anglewasassessedusing goniom-etry:theparticipantswerepositionedindorsaldecubituswiththekneeandhipextended, andthehipandfootinneutralrotation.Anteriorkneepainseveritywasassessedusinga visualanalogscale,andfunctionalcapacitywasassessedusingtheanteriorkneepainscale. Dynamicvalguswasevaluatedusingthefrontalplaneprojectionangle(FPPA)oftheknee, whichwasrecordedusingadigitalcameraduringstepdown,andhipabductorpeaktorque wasrecordedusingahandhelddynamometer.
Results:Theq-angledidnotpresentanysignificantcorrelationwithseverityofkneepain (r=−0.29;p=0.19),functionalcapacity(r=−0.08;p=0.72),FPPA(r=−0.28;p=0.19)or isomet-ricpeaktorqueoftheabductormuscles(r=−0.21;p=0.35).
Conclusion: Theq-angledidnot presentanyrelationshipwithpain intensity,functional capacity,FPPA,orhipabductorpeaktorqueinthepatientswithPFPS.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
夽
WorkperformedintheLaboratóriodeInvestigac¸ãoFisioterapêuticaClínicaeEletromiografia,UniversidadedeSãoPaulo,SãoPaulo, SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](G.P.L.Almeida). http://dx.doi.org/10.1016/j.rboe.2016.01.010
Ângulo-q
na
dor
patelofemoral:
relac¸ão
com
valgo
dinâmico
de
joelho,
torque
abdutor
do
quadril,
dor
e
func¸ão
Palavras-chave: Joelho
Síndromedadorpatelofemoral Dinamômetrodeforc¸amanual
r
e
s
u
m
o
Objetivo: Investigararelac¸ãoentreoângulo-qeintensidadeda doranteriornojoelho, capacidadefuncional,valgodinâmicodejoelhoetorqueabdutordoquadrilemmulheres comsíndromedadorpatelofemoral(SDPF).
Métodos: Participaram doestudo 22 mulheres comSDPF. Oângulo-qfoi avaliado pela goniometria,asparticipantesforamposicionadasemdecúbitodorsalcomjoelhoequadril estendidoequadrilepéemrotac¸ãoneutra.Aintensidadedadoranteriordojoelhofoi avaliadapelaescalavisualanalógicadedoreacapacidadefuncionalcomaescaladedor anteriornojoelho.Ovalgodinâmicofoiavaliadopeloângulodeprojec¸ãonoplanofrontal dojoelho(APPF),registradocomcâmeradigitaldurantestepdown,eopicodetorquedos abdutoresdoquadrilcomdinamômetromanual.
Resultados: Oângulo-qnãoapresentoucorrelac¸ãosignificativacomaintensidadedador nojoelho(r=−0,29;p=0,19),capacidadefuncional(r=−0,08;p=0,72),ângulodeprojec¸ão noplanofrontaldojoelho(r=−0,28;p=0,19)epicodetorqueisométricodosmúsculos abdutores(r=−0,21;p=0,35).
Conclusão: Oângulo-qnãoapresentourelac¸ãocomaintensidadedador,capacidade fun-cional,ângulodeprojec¸ãonoplanofrontaldojoelhoepicodetorquedosabdutoresdo quadrilempacientescomSDPF.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Theq-anglewasfirstdescribed byBrattstroem.1 Thisangle isformedbythe intersectionoftwolinesthatcross atthe centerofthepatella:onegoingfromtheanterosuperioriliac spine(ASIS)tothecenterofthepatellaandtheotherfrom theanteriortuberosityofthetibiatothecenterofthepatella; andtheotherfromtheanteriortuberosityofthetibiatothe centerofthepatella.1Theq-angleiswidelyusedfor evalu-atingpatientswithkneeproblems,especiallypatellofemoral painsyndrome(PFPS).Thelargertheq-angleis,thegreater the lateralizationforce onthe patella, which increasesthe retropatellarpressurebetweenthelateralfacetofthepatella andthelateralfemoralcondyle.2Thecontinuouscompressive forcesbetweenthesestructuresmaygiverisetoPFPSand,over thelongterm,causedegenerationofthejointcartilageofthe patella.2,3HubertiandHayes4reportedthata10%increasein theq-angleincreasedthestressonthepatellofemoraljoint by45%.
However,therearedivergencesintheliteratureregarding therelationshipbetweentheq-angleandPFPSincase–control studies.5,6 Moreover,prospectivestudieshavenotsupported thehypothesisthatgreaterq-anglesareariskfactorfor devel-opmentofPFPS.7–9
Notonlydoestheq-angleaffectthestaticalignmentofthe lowerlimbinthe frontalplane, butalsothe lever-arm dis-tancebetweenthecentersofthehipandknee jointsalters thecapacityofthehipabductormusclestogeneratetorque.10 However,itisquestionablewhetherthestaticvalgus(q-angle) affects the dynamic valgus of the knee and the peak iso-metrictorqueofthehipabductormuscles.Furthermore,few
studieshavecorrelatedtheq-anglewithkneepainintensity andfunctionalcapacityamongwomenwithPFPS.11,12
Thus,theobjectiveofthisstudywastoascertainthe rela-tionshipoftheq-anglewithkneepainintensity, functional capacity,projectionangleinthefrontalplaneandpeak iso-metric torqueofthe hip abductormuscles, amongwomen withpatellofemoralpain.Ourhypothesiswasthattheq-angle wouldhavepositivecorrelationswiththedynamicvalgusof thekneeandwiththeintensityofanteriorkneepain;andthat itwouldpresentnegativecorrelationswiththepeakisometric torqueofhipabductionandwithfunctionalcapacity,among womenwithPFPS.
Materials
and
methods
Participants
A cross-sectional study was conductedon 22 womenwith PFPS,ofages19–45years.Womenwereselectedforthisstudy becauseofthehighincidenceofPFPSinthispopulation,in comparisonwithmen,andbecauseofthestructural, strength-relatedandkinematicdifferencesinthehipsbetweenthetwo sexes.Theagegroupwaschosensoastoexcludepossible degenerative alterationstothekneeand hip.13 The partici-pantswererecruitedbymeansofpersonalcommunication, throughorthopedicclinicsandthroughleafletsdisseminated withinouruniversity.
Thepatientsincluded inthe patellofemoralgroup (PFG) presented patellofemoral pain that was reproduced in at leasttwoofthefollowingactivities:goingupordownstairs, squatting,kneeling, remainingseated foralong time, per-formingisometrichipcontraction,jumpingandrunning.They reported feeling pain upon palpation ofthe lateral and/or medialfacetofthepatella;insidiouspainthathadlastedfor atleastthreemonths;painscoringatleastthreeonavisual analogscale(VAS)forpain;14painuponcompressionofthe patellawiththekneeflexedat15◦orwithpalpationofthe
lat-eralretinaculumagainsttheposteriorsurfaceofthepatella;15 andatleast86pointsonthepainscaleforanteriorkneepain (maximum=100points).16
Thefollowingwomen were excluded from bothgroups: those with previous surgery on their knees, hips, ankles and/orspine;historiesofpatellardislocation;clinicalevidence ofknee instability;meniscallesions orotherintra-articular lesions; evidence of edema; Osgood-Schlatter or Sinding-Larsen-Johanssen; patellar tendinopathy; chondral lesions; osteoarthritis;bodymassindex(BMI)greaterthan28kg/m2; structural abnormalities in the spine; discrepancy of leg length of 2cm, evaluated by means of real and apparent measurement; neurologicalinvolvementthat compromised the abilityto walk; lumbarpain formore than two weeks over the last six months; or muscle or joint injuries in thehip.
Procedures
Alltheevaluationsweremadebythesameinvestigator,who hadfiveyearsofclinicalexperience.Onlythesymptomatic limb(orthemostsymptomaticlimb)wasevaluatedineach patient.
Q-angle
Theq-anglewasevaluatedbymeansofauniversal goniome-ter, with the participant in dorsal decubitus and with the hipandknee completelyextended,hip intheneutral rota-tionpositionandfeetintheneutralposition.Theanglewas calculatedbymeansoftheintersectionformedbytwolines crossing at the center of the patella. The first line went from the ASISto the centerof thepatella and the second fromtheanteriortuberosityofthetibiatothecenterofthe patella.17Theintraandinter-evaluatorreliabilityofq-angle measurementsusingagoniometerhasbeenwellestablished intheliterature18andthecorrectionthroughMRIevaluation ismoderate.18
Functionalcapacityandpain
TheintensityofthepainwasevaluatedbymeansofaVAS. Thisscalerangedfrom0(absenceofpain)to10(maximum pain) and is reliable and valid for pain complaints in the knee.19 Functional capacity was evaluated using the ante-riorkneepainscale(AKPS),whichisaquestionnairewith13 itemsandscoringbetween0(worstpossible) and100(best possible).20
Dynamickneevalgus
Kneekinematicsduringstep-downwasevaluatedbymeans offilmingin2Dusingadigitalcamera(SonyCyber-shot DSC-W35;7.2megapixels).Thefrontalplaneprojectionangle(FPPA) oftheknee wasdefined.Threeself-adhesivemarkerswere placed:atthemidpointbetweenthemedialandlateral malle-oli;atthemidpointbetweenthemedialandlateralfemoral condyles;andataposition30cmabovethekneemarker, fol-lowingastraightlinefromthismarkertotheanterosuperior iliacspine(ASIS).15
The heightofthe stepwas standardizedby takinginto account10% oftheheightofeach individual.Each partici-pant’sfootwaspositionedonastandardlineandthepoint atwhichthe heeltouchedthegroundwas standardizedat a distance of 5cm from the step. The digital camera was atadistanceof2mfromthe step,atthelevel ofthe knee that wastobeevaluated.Before thesubjectsdidthe tests, they were given verbal guidance about how to do them properly, witha demonstration of the depth and speed of the test, but without specifying the orientation ofthe hip andknee.
Alltheparticipantsperformedthreetests,with60sof res-ting between them,as the effective start ofthe test. Each step-downwasdonefor5s,referringtotheeccentricand con-centricphases,and weremarkedusingachronometer.The foot participants (1s) were instructed toperformthe step-downslowlyuntiltheheelofthesuspendedfoottouchedthe ground(3s).Thiswasfollowedbyaslowreturntothe ini-tialposition(5s).Afteraperiodofadaptationtothetest,the meanfromfivetestswasusedfortheanalysisoneachlower limb.15
AsequenceofimageswascapturedusingtheVirtualDub software(copyright1998–2009AveryLee).TheFPPAwas cal-culated through the postural assessmentsoftware (PAS) v. 0.68,basedondigitizingspatiallydefinedpointsthatenabled measurementofbodyangles.ThevaluesoftheFPPAwere con-sideredtobenegativewhenthekneemarkerwasmedialto thethighandankle(dynamicvalgus),andwereconsideredto bepositivewhenthekneemarkerwaslateraltotheothertwo (dynamicvarus).15
Abductortorqueofthehip
Musclestrengthwasevaluatedusingamanualdynamometer (NicholasManualMuscleTester,LafayetteInstrument Com-pany, Lafayette,Indiana, USA). Studies have demonstrated thatthisequipmenthasexcellentreliabilityinintraand inter-observerevaluation.21,22
theeventofanycompensationthatmighthavecompromised thetest result,or anyoccurrence ofdiscrepant values,the testwasdisregardedandwasrepeatedafter20s.Toanalyze thedata,theforce (N)wasconvertedintotorque(Nm)and wasnormalizedwithbodyweight(kg),throughthefollowing formula:(Torque[Nm]/Weight[kg])×100.
Thetorqueofthehipabductorswasevaluatedwiththe patientinlateraldecubitusonanexaminationbed.Thelimb tobeevaluatedwaspositionedathipabductionof20◦,
exten-sionof10◦andneutralrotation,withthekneeextended.The
non-evaluatedlimbwas positionedathipand kneeflexion of45◦.Thecenterofthedynamometerwaspositioned5cm
proximallytothecenterofthelateralmalleolus.Theleverarm wasmeasuredasthedistancefromthecenterofthegreater trochantertothecenterofapplicationofthedynamometeron thelowerlimb.
Statisticalanalysis
TheShapiro–Wilktestwasusedtoascertainwhetherthedata showednormaldistribution.Descriptiveanalyses(meanand standarddeviation)wereperformedonallthevariables.
Pearson’scorrelationcoefficientwasusedtoanalyzethe associationsbetweentheq-angle(independentvariable)and thepainintensity,functionalcapacity,dynamickneevalgus and hip abductor torque(dependentvariables).The values ofrwereinterpretedasfollows:0–0.19=none;0.2–0.39=low; 0.4–0.69=moderate;0.7–0.89=high;and0.9–1=veryhigh.For allthe statisticalanalyses,the SPSS17.0 softwarefor Win-dowswas used (Statistical Package forthe Social Sciences Inc.,Chicago,IL,USA),andthesignificancelevelwastakento be5%.
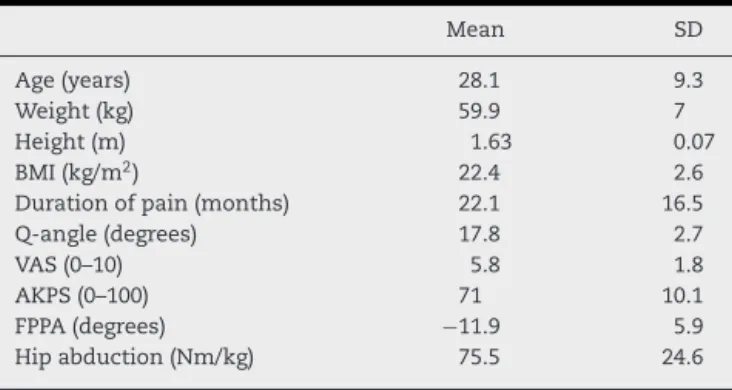
Table1–Clinicalandanthropometriccharacteristicsof thepatientswithpatellofemoralpainsyndrome (mean±SD).
Mean SD
Age(years) 28.1 9.3
Weight(kg) 59.9 7
Height(m) 1.63 0.07
BMI(kg/m2) 22.4 2.6
Durationofpain(months) 22.1 16.5 Q-angle(degrees) 17.8 2.7
VAS(0–10) 5.8 1.8
AKPS(0–100) 71 10.1
FPPA(degrees) −11.9 5.9 Hipabduction(Nm/kg) 75.5 24.6
BMI,bodymassindex;VAS,visualanalogscaleforpain;AKPS, ante-riorkneepainscale;FPPA,frontalplaneprojectionangle.
Results
Thedemographicandclinicalcharacteristicsofthepatients withPFPSareshowninTable1.
The q-angle did not present any significant correlation with pain intensity (r=−0.29; p=0.19), functional capacity (r=−0.08;p=0.72),dynamickneevalgus(r=−0.28;p=0.19)or hipabductortorque(r=−0.21;p=0.35)(Fig.1).
Discussion
Theobjectiveofthisstudywastoascertaintherelationship betweentheq-angleandthevariablesofpainintensity, func-tionalcapacity,FPPAofthekneeandpeakisometrictorqueof
10
8
6
4
2
0
100
80
60
40
20
0
15
10
5
0 30
40
20
10
0
0 10 20
q-angle (degrees)
30 0 10 20
q-angle (degrees)
30
0 10 20
q-angle (degrees)
30 0 10 20
q-angle (degrees)
30
FPPA (degrees)
VAS (0-10)
AKPS (0-100)
Hip abduction (Nm/kg)
A
B
C
D
thehipabductormuscles.However,thepresentstudydidnot findanyrelationshipbetweentheq-angleandthedependent variablesanalyzed.
Ithasbeentheorizedthatanexcessiveq-angleisrelated todevelopmentofPFPS,throughincreasedcompressiveforces betweenthelateralfacetofthepatellaandthelateralfemoral condyle.2,4 Nevertheless,this hypothesishasnotbeen con-firmedthroughprospectivestudies.Thijsetal.8andRamskov et al.9 prospectively monitored novice street runners and foundthattheq-angledidnotdifferbetweentheathleteswho developedPFPSand thosewho didnot.Thus, theydidnot considerittobeariskfactor.Similarfindingswerereported byBoling et al.7 from a prospectivestudy on 1319 partici-pants,withthreeyearsoffollow-up. Furthermore,arecent systematicreviewwithmeta-analysis23confirmedthelackof relationshipbetweenanexcessiveq-angleanddevelopment ofPFPS.
Excessivedynamickneevalgusisanabnormalityof neu-romuscularcontroloverthelowerlimb.Thiscreatesalateral force vector on the patella and increases the compressive loadsbetweenthelateralfaceofthepatellaandthelateral femoralcondyle.24Studiershavedemonstratedthatpatients withPFPSpresentgreaterdynamickneevalgusthando con-trols without PFPS.15,25 Theoretically, an excessive q-angle mayfavorexcessivedynamickneevalgusbecauseofthemore medialorientation of the knee in the frontal plane. How-ever,ourresultsshowthatpatientswithanexcessiveq-angle donothavegreaterdynamickneevalgus.Corroboratingour findings,ithasbeensuggestedthatthemagnitudeofthe q-anglehasminimaleffectonalterationsofthekinematicsof thelowerlimbanddoesnotincreasethekneejointanglein thesagittalandtransverseplanesduringrunning.26Pantano etal.27reportedthatindividualsclassifiedashavingalarger q-angle(≥17◦)didnotpresentagreaterkneevalgusangle,in
comparisonwiththosewithsmallerq-angles(≤8◦).
Interest-ingly,thenegativecorrelationbetweenthe q-angleandthe kneeabductionmoment indicatesthatgreaterq-anglesare associatedwithsmallerdynamicvalgus.10
Weaknessofthe hip abductor muscles hasconsistently beenfoundinpatientswithPFPS,withdeficitsrangingfrom 21to29%,incomparisonwithcontrolswithoutPFPS.28 The capacityofthehipmusclestocontrolexcessivedynamicknee valgusdependsontheircapacitytogeneratetorque.Factors thatmodifytheleverarmofthelower limbsmayalterthe capacityofthehipmusclestogeneratetorque.Studieshave shownthatanatomicalalterationsofthehip inthe frontal plane,suchasfemoraloffset,arecorrelatedwiththestrength of the hip abductor muscles.29 However, we did not find anystudiesinvestigatingtherelationshipbetween anatom-icalalterationsinthefrontalplaneoftheknee(q-angle)and thestrengthofthehipmuscles.Ourresultsdonotsupport thehypothesisthattheq-anglehasarelationshipwiththe capacityofthehipmusclestogeneratetorque.
Increased patellofemoral stress may result in increased intensity of anterior pain in the knee, with consequent diminutionoffunctionalcapacityandanearlydegenerative processinthepatellofemoraljoint.2However,wedidnotfind any relationship between the q-angle and the intensity of anterior knee pain and functional capacity among women withPFPS.SimilarresultswerefoundbyPivaetal.,11whodid
notfindanyevidenceforarelationshipbetweentheq-angle andpainandfunctionalcapacity.LivingstonandMandigo12 did not fundant correlation between the q-angle and the intensityofkneepainamongpatientswithPFPS.
Theabsenceofprospectivestudiessupportingthe hypoth-esis that the q-angle is a risk factor for PFPS6–8 and the lackofrelationshipbetweentheq-angleandpainintensity, functionalcapacity11andvariablethatarepotentially modifi-ablethroughphysiotherapy(dynamicvalgusandhipmuscle strength)diminishtheclinicalrelevanceofevaluatingthe q-angleasthefocusofpreventionandtreatmentofPFPS.
It is important to highlight that the present study has some limitations. The cross-sectional nature of this study didnotallowcause-and-effectrelationshipstobeestablished betweenthevariablesanalyzedandPFPS.Patellofemoralpain is of multifactorial origin, and other possible anatomical, biomechanical,neuromuscularandpsychologicalfactorsthat werenotstudiedmayvaryaccordingtotheq-angle.
Conclusion
Theq-angledidnotpresentanyrelationshipwithpain inten-sity,functionalcapacity,frontalplaneprojectionangleofthe kneeorpeakisometrictorqueofthehipmuscles.Itcanbe sug-gestedthatevaluatingtheq-anglemaynotbringadditional informationfortreatingpatientswithPFPS.Thus, physiother-apeuticassessmentandtreatmentshouldbedirectedtoward otherpotentiallymodifiablevariables.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
Research Support Foundation of the State of São Paulo (Fundac¸ão de Amparo à Pesquisa doEstado de São Paulo, FAPESP),no.2012/10768-0.
r
e
f
e
r
e
n
c
e
s
1.BrattstroemH.Shapeoftheintercondylargroovenormally andinrecurrentdislocationofpatella.Aclinicaland X-ray-anatomicalinvestigation.ActaOrthopScandSuppl. 1964;68:1–148.
2.HeinoBrechterJ,PowersCM.Patellofemoralstressduring walkinginpersonswithandwithoutpatellofemoralpain. MedSciSportsExerc.2002;34(10):1582–93.
3.LeeTQ,MorrisG,CsintalanRP.Theinfluenceoftibialand femoralrotationonpatellofemoralcontactareaandpressure. JOrthopSportsPhysTher.2003;33(11):686–93.
4.HubertiHH,HayesWC.Patellofemoralcontactpressures.The influenceofq-angleandtendofemoralcontact.JBoneJoint SurgAm.1984;66(5):715–24.
6. LankhorstNE,Bierma-ZeinstraSM,vanMiddelkoopM. Factorsassociatedwithpatellofemoralpainsyndrome:a systematicreview.BrJSportsMed.2013;47(4):193–206. 7. BolingMC,PaduaDA,MarshallSW,GuskiewiczK,PyneS,
BeutlerA.Aprospectiveinvestigationofbiomechanicalrisk factorsforpatellofemoralpainsyndrome:theJoint UndertakingtoMonitorandPreventACLInjury(JUMP-ACL) cohort.AmJSportsMed.2009;37(11):2108–16.
8. ThijsY,PattynE,VanTiggelenD,RombautL,WitvrouwE.Is hipmuscleweaknessapredisposingfactorforpatellofemoral paininfemalenovicerunners?Aprospectivestudy.AmJ SportsMed.2011;39(9):1877–82.
9. RamskovD,JensenML,OblingK,NielsenRO,ParnerET, RasmussenS.Noassociationbetweenq-angleandfoot posturewithrunning-relatedinjuries:a10weekprospective follow-upstudy.IntJSportsPhysTher.2013;8(4):
407–15.
10.ParkSK,StefanyshynDJ.GreaterQanglemaynotbearisk factorofpatellofemoralpainsyndrome.ClinBiomech(Bristol, Avon).2011;26(4):392–6.
11.PivaSR,FitzgeraldGK,IrrgangJJ,FritzJM,WisniewskiS, McGintyGT,etal.Associatesofphysicalfunctionandpainin patientswithpatellofemoralpainsyndrome.ArchPhysMed Rehabil.2009;90(2):285–95.
12.LivingstonLA,MandigoJL.BilateralQangleasymmetryand anteriorkneepainsyndrome.ClinBiomech(Bristol,Avon). 1999;14(1):7–13.
13.RussellKA,PalmieriRM,ZinderSM,IngersollCD.Sex differencesinvalguskneeangleduringasingle-legdrop jump.JAthlTrain.2006;41(2):166–71.
14.BolglaLA,MaloneTR,UmbergerBR,UhlTL.Hipstrengthand hipandkneekinematicsduringstairdescentinfemaleswith andwithoutpatellofemoralpainsyndrome.JOrthopSports PhysTher.2008;38(1):12–8.
15.WillsonJD,DavisIS.Utilityofthefrontalplaneprojection angleinfemaleswithpatellofemoralpain.JOrthopSports PhysTher.2008;38(10):606–15.
16.WatsonCJ,ProppsM,RatnerJ,ZeiglerDL,HortonP,SmithSS. Reliabilityandresponsivenessofthelowerextremity functionalscaleandtheanteriorkneepainscaleinpatients withanteriorkneepain.JOrthopSportsPhysTher.
2005;35(3):136–46.
17.SmithTO,HuntNJ,DonellST.Thereliabilityandvalidityof theQ-angle:asystematicreview.KneeSurgSportsTraumatol Arthrosc.2008;16(12):1068–79.
18.DraperCE,ChewKT,WangR,JenningsF,GoldGE,Fredericson M.Comparisonofquadricepsanglemeasurementsusing short-armandlong-armgoniometers:correlationwithMRI. PMR.2011;3(2):111–6.
19.CrossleyKM,BennellKL,CowanSM,GreenS.Analysisof outcomemeasuresforpersonswithpatellofemoralpain: whicharereliableandvalid?ArchPhysMedRehabil. 2004;85(5):815–22.
20.daCunhaRA,CostaLO,HespanholJuniorLC,PiresRS,Kujala UM,LopesAD.Translation,cross-culturaladaptationand clinimetrictestingofinstrumentsusedtoassesspatients withpatellofemoralpainsyndromeintheBrazilian population.JOrthopSportsPhysTher.2013;43(5):332–9. 21.PivaSR,GoodniteEA,ChildsJD.Strengtharoundthehipand
flexibilityofsofttissuesinindividualswithandwithout patellofemoralpainsyndrome.JOrthopSportsPhysTher. 2005;35(12):793–801.
22.RobinsonRL,NeeRJ.Analysisofhipstrengthinfemales seekingphysicaltherapytreatmentforunilateral patellofemoralpainsyndrome.JOrthopSportsPhysTher. 2007;37(5):232–8.
23.LankhorstNE,Bierma-ZeinstraSM,vanMiddelkoopM.Risk factorsforpatellofemoralpainsyndrome:asystematic review.JOrthopSportsPhysTher.2012;42(2):81–94. 24.PowersCM.Theinfluenceofabnormalhipmechanicson
kneeinjury:abiomechanicalperspective.JOrthopSports PhysTher.2010;40(2):42–51.
25.LevingerP,GilleardW,ColemanC.Femoralmedialdeviation angleduringaone-legsquattestinindividualswith patellofemoralpainsyndrome.PhysTherSport. 2007;(8):163–8.
26.HeiderscheitBC,HamillJ,CaldwellGE.InfluenceofQ-angle onlower-extremityrunningkinematics.JOrthopSportsPhys Ther.2000;30(5):271–8.
27.PantanoKJ,WhiteSC,GilchristLA,LeddyJ.Differencesin peakkneevalgusanglesbetweenindividualswithhighand lowQ-anglesduringasinglelimbsquat.ClinBiomech (Bristol,Avon).2005;20(9):966–72.
28.PrinsMR,vanderWurffP.Femaleswithpatellofemoralpain syndromehaveweakhipmuscles:asystematicreview.AustJ Physiother.2009;55(1):9–15.