Doppler Sonographic Findings in Testicular Microlithiasis
Selim Serter, Sebnem Orguc, Bilal Gumus, Veli Ayyildiz, Yuksel Pabuscu
Department of Radiology (SS,SO,YP) and Department of Urology (BG), Celal Bayar University, Manisa, Turkey, and Manisa Military Hospital (VA), Manisa, Turkey
ABSTRACT
Objective:The aim of this prospective study was to compare the resistive index (RI) values, which is a parameter of tes-ticular parenchymal perfusion, in testes-ticular microlithiasis (TM) cases and normal cases.
Materials and Methods:YROXQWHHUVDOOKHDOWK\PHQ\HDUVRIDJHIURPWKH$QQXDO$UP\5HVHUYH2I¿FHU Training Corps training camp were included in the study. A screening scrotal ultrasound was performed and all men di-agnosed with TM underwent a scrotal Doppler ultrasonography scan (US). US examinations were performed for subjects with TM and without TM as a control group and RI was determined.
Results:PHQZLWK70ZHUHLGHQWL¿HGLQWKH866SHFWUDO'RSSOHUH[DPLQDWLRQZDVDSSOLHGWRUDQGRPO\VH
-OHFWHGFDVHVWHVWLFOHVZLWKRXW70DQGWHVWLFOHVZLWK70FDVHVWHVWLFOHVZLWKELODWHUDODQGFDVHVZLWK XQLODWHUDOLQYROYHPHQW+RZHYHUQRUPDOWHVWLFOHVELODWHUDODQGXQLODWHUDODQGWHVWLFOHVZLWK70ELODWHUDO DQGXQLODWHUDORIZKLFKZHUHFDVHVZLWKELODWHUDO70ZKHUHÀRZIURPWKHFHQWULSHWDODUWHU\FRXOGEHREWDLQHGDQG DQDO\]HGZHUHLQFOXGHGLQWKHVWDWLVWLFDODQDO\VLVIRUUHVLVWLYHLQGLFHV7KHUHZDVQRVLJQL¿FDQWGLIIHUHQFHUHJDUGLQJWKH 5,DQGVSHFWUDOH[DPLQDWLRQVEHWZHHQVXEMHFWVZLWKDQGZLWKRXW70$QLQWHUHVWLQJ¿QGLQJZDVWKHWZLQNOLQJDUWLIDFW
observed in three cases.
Conclusion:0LFUROLWKVGLGQRWDOWHUWKH5,YDOXHVDQGWKXVKDGQRLQÀXHQFHRQWHVWLFXODUSHUIXVLRQRQ'RSSOHU86H[ -amination.
Key words: testis, ultrasonography, lithiasis, Doppler
Int Braz J Urol. 2008; 34: 477-84
INTRODUCTION
Testicular microlithiasis (TM) is an uncom-mon condition characterized by intratubular
cal-FL¿FDWLRQV ZLWKLQ D PXOWLOD\HUHG HQYHORSH XVXDOO\
discovered incidentally at ultrasonography (US) (1,2).
$OWKRXJKPLQRUPLFURFDOFL¿FDWLRQZLWKLQDWHVWLVLV
considered normal, the typical US appearance of TM is of multiple nonshadowing echogenic foci measur-ing 2-3 mm and randomly scattered throughout the
WHVWLFXODUSDUHQFK\PD7KHFOLQLFDOVLJQL¿FDQFHRI
testicular microlithiasis remains unclear. Currently
there is no evidence that TM is either a premalignant condition or a causative agent in testicular neoplasia; however, it has been associated with testicular
neopla-VLDLQRIFDVHV6RPHDXWKRUVFRQFOXGHG WKDWWKHLQFUHDVHLQWKHUHODWLYHULVNRIWHVWLFXODUFDQFHU
in the group with TM suggests that the presence of
70LQV\PSWRPDWLFPHQLVFOLQLFDOO\VLJQL¿FDQW,Q
WHVWLFXODUVHOIH[DPLQDWLRQLQPHQDWULVN,WLVE\
no means certain that microlith on its own is predic-tive of tumor.
Doppler US features of the testes, especially
UHVLVWLYHLQGH[5,ZKLFKLVDUHÀHFWLRQRIDUWHULDO
impedance, have been used to evaluate several tes-ticular disorders, such as varicocele, orchitis, scrotal hernias, and others (9-11). Currently, RI has become
DGLDJQRVWLFWRRORIWHVWLFXODUEORRGÀRZLQPDQ\GLV -eases as established by Middleton et al. (12). Among numerous Doppler US studies of the testes previously published, only two case reports attempted to identify Doppler ultrasonographic parameters for TM,
how-HYHUHQFRXQWHUHGQRVSHFL¿F¿QGLQJV7KLV LVWKH¿UVWVWXG\WRRXUNQRZOHGJHWRLQYHVWLJDWH
the Doppler parameters of TM in a large cohort and comparing them with a control group.
The aim of this prospective study was to com-pare the RI values, which is a parameter of testicular parenchymal perfusion in subjects with or without TM.
Many new studies have addressed the fact that hypoxic stress contributes to many (patho) bio-logical disorders and hypoxic control of cell growth and death may be of general pathophysiological importance (15,16). On these bases, we attempted to evaluate the possible vascular alterations in TM with the hypothesis of compression of microliths leading to increased local pressure in the testicular parenchyma and the possible association of microliths and tumor formation.
MATERIALS AND METHODS
%HWZHHQ$XJXVWDQG0D\ KHDOWK\ YROXQWHHUV IURP 5HVHUYH 2I¿FHU7UDLQLQJ
Corps annual training camp were included in the study. A total of 2,179 white male subjects were evaluated by US. The age of the subjects (mean ± SD) was 22.4 ± 3.6 years (range 17-42 years). There was no racial variation in our study cohort. Informed consent was obtained from all participants. The study was approved by the Institutional Review Board and met all guidelines of our institution. A medical history was obtained from all volunteers, who also underwent a genitourinary physical examination. None of the
subjects had a urinary disease or any other pathology. Subjects underwent screening scrotal ultrasound with
6LHPHQV6RQROLQH*XOWUDVRXQGPDFKLQH,VVDTXDK
WA). Examinations were performed with the patient in supine position and the scrotum was supported by a towel placed between the thighs and the penis was placed on the abdomen and covered with a towel. The ultrasound gel was warmed with a heated towel before sonography to avoid cremasteric muscle con-traction. All examinations were performed using a
0+]OLQHDUDUUD\WUDQVGXFHULQORQJLWXGLQDO
and transversal sections to document the presence or absence of TM. Four different radiologists perform
WKHVFUHHQLQJ%PRGXOWUDVRXQG6XEVHTXHQWO\WKH
same experienced radiologist (SS) performed the Doppler US examination for cases with TM and the selected control group.
$V SUHYLRXVO\ GH¿QHG D WHVWLFXODU PLFUR
-OLWKLDVLVGLDJQRVLVZDVFRQ¿UPHGZKHQPRUHWKDQ
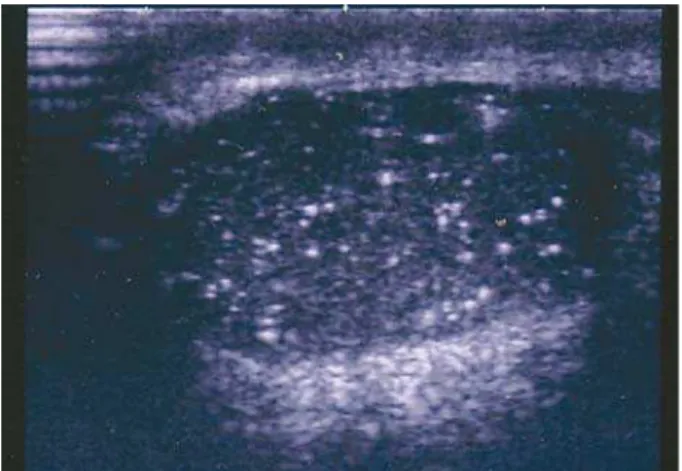
5 high intensity signals 1 to 2 mm in size without acoustic shadowing was detected by US in a tes-ticle (Figure-1). We recorded if the testes-ticles were
LQYROYHGZLWKFDOFL¿FDWLRQVXQLODWHUDOO\RUELODWHU -ally. The cases with TM were not graded according to the severity of microliths. All men diagnosed with TM underwent testicular Doppler US examination, complete clinical evaluation including a detailed genitourinary history and physical examination and
GHWHUPLQDWLRQRIWXPRUPDUNHUV%HWD+&*$)3
and lactate dehydrogenase). Color Doppler US of
WKH VFURWXP ZDV SHUIRUPHG ZLWK WKH VDPH HTXLS -ment. All Doppler examinations were performed using the same linear array transducer with a range
RI'RSSOHUIUHTXHQF\0+]&RORUJDLQWKUHVK -old) was maximized for optimal sensitivity while avoiding excessive color noise. The Doppler scale
UDQJHRIGLVSOD\DEOH'RSSOHUIUHTXHQF\VKLIWVZDV
decreased to its lowest value to maximize sensitivity
WRVORZÀRZ7KH'RSSOHUVFDOHZDVGLVSOD\HGRQ
the right side of all images as a bar containing the red and blue color assignment for different
Dop-SOHUIUHTXHQF\VKLIWV:DOO¿OWHUVZHUHDGMXVWHGWR
the lowest possible value. In Doppler examinations resistive indices were obtained from the centripetal artery or its recurrent rami, whichever was visualized
GLYLGHGE\SHDNV\VWROLFYHORFLW\7KH5,ZDVPHD -sured three times on each testicle.
'DWD ZHUH DQDO\]HG XVLQJ 6366 IRU
Windows commercially available computer software.
:HXVHGLQGHSHQGHQWVDPSOHVWWHVWDQGSZDV DFFHSWHGDVVWDWLVWLFDOO\VLJQL¿FDQW
RESULTS
)LIW\WKUHHPHQZLWK70ZHUHLGHQWL¿HGLQ PHQZLWKDSUHYDOHQFHRIIRU70LQWKLV
asymptomatic population. The mean age ± SD of subjects with TM was 23.9 ± 4.2 years old (range
WRRIWKHVXEMHFWVKDGELODWHUDO
microlithiasis. All cases with microliths displayed diffuse type of TM and no cases of focal TM were detected. All subjects with TM had a normal genito-urinary history and physical examination. The tumor
PDUNHUVZHUHZLWKLQQRUPDOOLPLWVIRUDOOVXEMHFWV
Spectral Doppler examination was applied
WRUDQGRPO\FKRVHQFDVHVWHVWLFOHVZLWKRXW 70DQGWHVWLFOHVZLWK70FDVHVWHVWLFOHV
with bilateral and 14 cases with unilateral
involve-PHQW+RZHYHUQRUPDOWHVWLFOHVELODWHUDODQG
14 unilateral) and 47 testicles with TM (15 bilateral
DQGXQLODWHUDORIZKLFKZHUHFDVHVZLWKELODW
-HUDO70LQZKLFKÀRZIURPWKHFHQWULSHWDODUWHU\
could be obtained and analyzed were included in the statistical analysis for resistive indices. The percent-age of cases where RI could be obtained from the centripetal arteries were approximately the same in both TM and control groups. Resistive indices of subjects with and without TM are shown in Table-1.
1R¿QGLQJVSHFL¿FWR70ZDVGHWHFWHGRQVSHFWUDO
Doppler ultrasound examination. There was no
sig-QL¿FDQWGLIIHUHQFHUHJDUGLQJWKH5,¶VDQGVSHFWUDO
examinations between subjects with or without TM. Figure-2 demonstrates Doppler spectral analysis of cases with testicular microlithiasis. An additional
LQWHUHVWLQJ¿QGLQJGHWHFWHGGXULQJWKH&RORU'RSSOHU H[DPLQDWLRQ ZDV WKH WZLQNOLQJ DUWLIDFW FDXVHG E\
testicular microliths (Figure-3). These artifacts were
REVHUYHGLQRQO\WKUHHRIDOOFDVHVZLWK70
These artifacts also complicated the examination by
PLPLFNLQJYDVFXODUVWUXFWXUHVZKLOHREWDLQLQJWKH
Doppler spectrum.
Figure 1 – Longitudinal sonogram of the testicle shows QXPHURXVVPDOOHFKRJHQLFIRFLRIFDOFL¿FDWLRQZLWKRXW posterior shadowing.
Figure 2 – Spectral Doppler analysis of testicular artery demonstrates resistive index value.
Table 1 – Resistive index values of centripetal artery or its recurrent rami transmediastinal testicular artery in subjects with or without testicular microlithiasis.
Resistive Indices (mean ± SD)
:LWKPLFUROLWKLDVLVQ WHVWHV
Without microlithiasis (n = 47 testes)
p Value !
COMMENTS
TM is a rare, asymptomatic disease, suspected to be associated with various benign and malignant urological pathologies and genetic anomalies, usu-ally found incidentusu-ally on ultrasound examinations performed for other reasons. TM has a characteristic appearance, classically consisting of multiple, often bilateral microliths scattered throughout the testicular parenchyma. Histologically microliths consist of a
FHQWUDOFDOFL¿HGFRUHVXUURXQGHGE\FRQFHQWULFODPL -nations of cellular debris, glycoprotein and collagen (17).
Many new studies have reported that hypoxic stress contributes to many (patho) biological disorders and hypoxic control of cell growth and death may be of general pathophysiological importance (15,16). On these bases, we attempted to evaluate the possible vascular alterations in TM with the hypothesis of compression of microliths leading to increased local pressure in the testicular parenchyma and the possible association of microliths and tumor formation.
7KLVVWXG\LVWKH¿UVWVHULHVWKDWHYDOXDWHG70
using Doppler ultrasound in a large cohort. There are only two case reports in the literature regarding the
'RSSOHUXOWUDVRQRJUDSKLF¿QGLQJVRI70
Knowledge of the arterial supply of the testis is
re-TXLUHGIRULQWHUSUHWDWLRQRIFRORUÀRZ'RSSOHUVRQRJ -raphy of the testis. The testicular arteries arise from the anterior aspect of the aorta just below the origin of the renal arteries. They course through the inguinal canal with the spermatic cord to the postero-superior aspect of the testis. Upon reaching the testis, the testicular artery divides into branches, which pierce the tunica albuginea and divides over the surface of
WKHWHVWLVLQDOD\HUNQRZQDVWKHWXQLFDYDVFXORVD
Centripetal branches arise from these capsular arteries; these branches course along the septula to converge on the mediastinum. From the mediastinum these branches form recurrent rami that course centrifugally within the testicular parenchyma, where they branch
LQWR DUWHULROHV DQG FDSLOODULHV 7KH YHORFLW\
waveforms of the normal intratesticular arteries show
KLJKOHYHOVRIDQWHJUDGHGLDVWROLFÀRZWKURXJKRXWWKH FDUGLDFF\FOHUHÀHFWLQJWKHORZYDVFXODUUHVLVWDQFH
of the testis (12). In this study cohort we evaluated the intratesticular artery (centripetal arteries and its
UHFXUUHQWUDPLÀRZSDUDPHWHUV,WLVVXJJHVWHGWKDW
the resistive indices could be higher in patients with TM due to compression of the intratesticular arteries
E\WKHPLFUROLWKV+RZHYHUZHGLGQRW¿QGDQ\GLI -ferences regarding the Doppler parameters between subjects with or without TM, as reported by Kutlu et al. (14). All Doppler parameters and spectral examination
¿QGLQJVZHUHZLWKLQQRUPDOOLPLWVLQERWKJURXSV $Q LQWHUHVWLQJ ILQGLQJ ZDV WKH WZLQNOLQJ DUWLIDFWVHHQLQWKUHHFDVHV7ZLQNOLQJDUWLIDFWZDV
described by Rahmouni et al. (19) as an artifact
JHQHUDWHG E\ D VWURQJO\ UHÀHFWLQJ PHGLXP7ZLQ
-NOLQJDUWLIDFWDSSHDUVDVDUDSLGO\DOWHUQDWLQJUHGDQG
blue color Doppler signal behind certain stationary objects, which gives the appearance of movement.
6LQFHLWVLQLWLDOGHVFULSWLRQWKHWZLQNOLQJDUWLIDFWKDV
been reported mainly in association with urinary tract
FDOFXOL5HFHQWO\WZLQNOLQJDUWLIDFWKDVEHHQ GHVFULEHGEHKLQGFDOFL¿FDWLRQVLQYDULRXVWLVVXHVVXFK
as gallbladder stones, encrustated indwelling ureteral
VWHQWVVWURQJO\UHÀHFWLQJRUELWDOVWUXFWXUHVDFDOFL¿HG
liver mass, intestinal pneumatosis and an intracranial
K\SHUHFKRLFPLFUROLWKVKDYHFUHDWHGGLI¿FXOWLHVLQ
obtaining the Doppler spectral analysis of intrates-ticular branches.
All subjects with TM were followed-up throughout their military service. At 6 and 12 months of follow-up, the subjects with TM were re-evaluated
ZLWKDSK\VLFDOH[DPLQDWLRQWHVWLFXODUWXPRUPDUN -ers and scrotal US examination. None of the subjects with TM underwent the biopsy procedure since there
ZHUHQR¿QGLQJVVXJJHVWLQJDWHVWLFXODUWXPRUVXFK
as a hypoechoic area or an irregularity on testicular contour. No testicular tumor was detected during the diagnosis or follow-up.
In conclusion, Doppler ultrasound in TM, previously reported only as case studies in the litera-ture, did not alter the spectral analysis parameters,
DQGWKXVKDGQRLQÀXHQFHRQWHVWLFXODUSHUIXVLRQLQ
Doppler US examination. Additionally we described
WKHWZLQNOLQJDUWLIDFWDPLVOHDGLQJ¿QGLQJFUHDWLQJ GLI¿FXOW\LQVSHFWUDODQDO\VLVVHFRQGDU\WRPLFUROLWKV
which has not been reported in TM in the literature.
CONFLICT OF INTEREST
None declared.
REFERENCES
-DQ]HQ'/0DWKLHVRQ-50DUVK-,&RRSHUEHUJ3/ GHO5LR3*ROGLQJ5+HWDO7HVWLFXODUPLFUROLWKLDVLV
sonographic and clinical features. AJR Am J
Roent-JHQRO
%DFNXV0/0DFN/$0LGGOHWRQ:'.LQJ%):LQ
-WHU7&UG7UXH/'7HVWLFXODUPLFUROLWKLDVLVLPDJLQJ
appearances and pathologic correlation. Radiology.
-DUDPLOOR'3HUH]$WD\GH$7HHOH5/6RQRJUDSK\ RI WHVWLFXODU PLFUROLWKLDVLV 8URO 5DGLRO
55-7.
+|EDUWK.6XVDQL06]DER1.UDW]LN&,QFLGHQFHRI WHVWLFXODUPLFUROLWKLDVLV8URORJ\ 0LGGOHWRQ:'7HHIH\6$6DQWLOODQ&67HVWLFXODU
PLFUROLWKLDVLVSURVSHFWLYHDQDO\VLVRISUHYDOHQFHDQG DVVRFLDWHGWXPRU5DGLRORJ\ 3DWHO0'2OFRWW(:.HUVFKPDQQ5/&DOOHQ3:
*RRGLQJ *$ 6RQRJUDSKLFDOO\ GHWHFWHG WHVWLFXODU
microlithiasis and testicular carcinoma. J Clin
Ultra-VRXQG
6HUWHU6*PV%8QO07XQo\UHN27DUKDQ 6$\\LOGL]9HWDO3UHYDOHQFHRIWHVWLFXODUPLFUROL -thiasis in an asymptomatic population. Scand J Urol
1HSKURO
'H&DVWUR%-3HWHUVRQ$&&RVWDELOH5$$\HDU
followup study of asymptomatic men with testicular
PLFUROLWKLDVLV-8UROGLVFXVVLRQ
1423.
9. Tanriverdi O, Miroglu C, Horasanli K, Altay B,
Cal-LVNDQ.&*XPXV(7HVWLFXODUEORRGÀRZPHDVXUH -ments and mean resistive index values after micro-surgical and high ligation varicocelectomy. Urology.
2]WXUN$2]WXUN(=H\UHN)2QXU.6LUPDWHO2 .DW1&RPSDULVRQRIEUXFHOODDQGQRQVSHFL¿FHSL
-GLG\PRUFKLWLVJUD\VFDOHDQGFRORU'RSSOHUXOWUDVR
-QRJUDSKLFIHDWXUHV(XU-5DGLRO
11. Turgut AT, Olçücüoglu E, Turan C, Kiliçoglu B, Kosar
3 *H\LN 32 HW DO 3UHRSHUDWLYH XOWUDVRQRJUDSKLF HYDOXDWLRQRIWHVWLFXODUYROXPHDQGEORRGÀRZLQSD
-WLHQWVZLWKLQJXLQDOKHUQLDV-8OWUDVRXQG0HG TXL]
0LGGOHWRQ :' 7KRUQH '$ 0HOVRQ */ &RORU
Doppler ultrasound of the normal testis. AJR Am J
5RHQWJHQRO
<DJFL & 2]FDQ +$\WDo 6$\GRV .$WDVR\ & 7HVWLFXODUPLFUROLWKLDVLVDVVRFLDWHGZLWKVHPLQRPD *UD\VFDOH DQG FRORU 'RSSOHU XOWUDVRXQG ¿QGLQJV 8URO,QW
.XWOX56LJLUFL$%D\VDO7$ONDQ$6DUDF.(IIHFWV RI WHVWLFXODU PLFUROLWKLDVLV RQ 'RSSOHU SDUDPHWHUV UHSRUWRIWKUHHFDVHV%0&8URO
6KDUL¿1)DUUDU:/3HUWXUEDWLRQVLQK\SR[LDGHWHF
-WLRQDVKDUHGOLQNEHWZHHQKHUHGLWDU\DQGVSRUDGLF WXPRUIRUPDWLRQ"0HG+\SRWKHVHV
5.
&DUPHOLHW3'RU<+HUEHUW-0)XNXPXUD'%UXV
-VHOPDQV.'HZHUFKLQ0HWDO5ROHRI+,)DOSKD
in hypoxia-mediated apoptosis, cell proliferation and
WXPRXUDQJLRJHQHVLV1DWXUH 9HJQL7DOOXUL 0 %LJOLDUGL (9DQQL 0*7RWD *
7HVWLFXODUPLFUROLWKVWKHLURULJLQDQGVWUXFWXUH-8URO
0LGGOHWRQ:'%HOO0:$QDO\VLVRILQWUDWHVWLFXODU
arterial anatomy with emphasis on transmediastinal
DUWHULHV5DGLRORJ\
19. Rahmouni A, Bargoin R, Herment A, Bargoin N, Vasile
&KHOIRXK1*UHQLHU1+LJXHUHW'7ULOODXG+/HYDQ
-WDO23DULHQWH-/HWDO&KDUDFWHUL]DWLRQRIXULQDU\ FDOFXOLLQYLWURVWXG\RI³WZLQNOLQJDUWLIDFW´UHYHDOHG E\ FRORUÀRZ VRQRJUDSK\$-5$P - 5RHQWJHQRO
/HH-<.LP6+&KR-<+DQ'&RORUDQGSRZHU 'RSSOHU WZLQNOLQJ DUWLIDFWV IURP XULQDU\ VWRQHV
clinical observations and phantom studies. AJR Am J
5RHQWJHQRO
$\WDo6.2]FDQ+(IIHFWRIFRORU'RSSOHUV\VWHPRQ WKHWZLQNOLQJVLJQDVVRFLDWHGZLWKXULQDU\WUDFWFDOFXOL -&OLQ8OWUDVRXQG
8VW\PRZLF]$.UHM]D-0DULDN=7ZLQNOLQJDUWLIDFW
in color Doppler imaging of the orbit. J Ultrasound
0HG
.KDQ+**DLOORXG30DUWLQ-%.KDZ16SDGROD / 5IHQDFKW '$ HW DO7ZLQNOLQJ DUWLIDFW RQ LQ -tracerebral color Doppler sonography. AJNR Am J
1HXURUDGLRO
7ULOODXG+3DULHQWH-/5DELH$*UHQLHU1'HWHFWLRQ
of encrusted indwelling ureteral stents using a
twin-NOLQJDUWLIDFWUHYHDOHGRQFRORU'RSSOHUVRQRJUDSK\ $-5$P-5RHQWJHQRO
*KHUVLQ(6RXGDFN0*DLWLQL'7ZLQNOLQJDUWLIDFW
in gallbladder adenomyomatosis. J Ultrasound Med.
2NWDU62<FHO&(UEDV*2]GHPLU+8VHRI WZLQNOLQJ DUWLIDFW LQ VRQRJUDSKLF GHWHFWLRQ RI LQ
-WHVWLQDO SQHXPDWRVLV$EGRP ,PDJLQJ
293-6.
Accepted after revision: April 20, 2008
Correspondence address: Dr. Selim Serter
VRN
8F\ROé]PLU7XUNH\ )D[ (PDLOVHUWHUVHOLP#JPDLOFRP
EDITORIAL COMMENT
Testicular microlithiasis (TM) corresponds to
LQWUDWXEXODUFDOFL¿FDWLRQVUHVXOWLQJIURPGHJHQHUDWLQJ
cells within the seminiferous tubules. They can be located in the lumen or beneath the epithelium under a thin layer of connective tissue (1). They are well seen with Ultrasound, and occasionally and
depend-LQJRQWKHQXPEHURIFDOFL¿FDWLRQVRQ&RPSXWHG
Tomography.
2QHRIWKH¿UVWUHSRUWVRQWHVWLFXODUPLFUROL -thiasis was found in the context of pulmonary alveolar
PLFUROLWKLDVLVLQ0LFUROLWKLDVLVKDVEHHQ
found in the adult general population with a reported
YDULDEOHLQFLGHQFHRIDQGLQFKLOGUHQ
(4). It has also been observed in association with
several other pathologies such as infertility (5), post-orchiopexy (6), orchialgia (7), torsion of appendix
WHVWLV0F&XQH$OEULJKWV\QGURPHDQG'RZQ V\QGURPH7KHPDLQFRQFHUQRIWHVWLFXODUPLFUR -lithiasis is its association with germ cell neoplasia and carcinoma in situ (11).
:KLOHPLFURFDOFL¿FDWLRQVGRH[LVWLQURXJKO\ RIJHUPFHOOWXPRUVWKHPDMRULW\RIPHQZLWK
testicular microlithiasis will not develop testicular cancer. Increased emphasis on testicular examination
LV WKH UHFRPPHQGHG IROORZXS IRU PHQ LGHQWL¿HG ZLWKWKLV¿QGLQJ)ROORZXSDWWKLVWLPHVKRXOG EHGLFWDWHGEDVHGRQULVNIDFWRUVIRUGHYHORSLQJWHVWLV
The recent study on Doppler Sonographic Findings in Testicular Microlithiasis by Serter et al. published in the current issue of the Journal expands the understanding of TM.
REFERENCES
6PLWK :6 %UDPPHU +0 +HQU\ 0 )UD]LHU + 7HVWLFXODUPLFUROLWKLDVLVVRQRJUDSKLFIHDWXUHVZLWK
pathologic correlation. AJR Am J Roentgenol. 1991;
&RHW]HH7 3XOPRQDU\ DOYHRODU PLFUROLWKLDVLV ZLWK
involvement of the sympathetic nervous system and
JRQDGV7KRUD[
6HUWHU6*Pú%8QO07XQo\UHN27DUKDQ 6$\\LOGL]9HWDO3UHYDOHQFHRIWHVWLFXODUPLFUROL -thiasis in an asymptomatic population. Scand J Urol
1HSKURO
'DJDVK+0DFNLQQRQ($7HVWLFXODUPLFUROLWKLDVLV ZKDWGRHVLWPHDQFOLQLFDOO\"%-8,QW
6FKDQW]$0LOVWHQ57HVWLFXODUPLFUROLWKLDVLVZLWK VWHULOLW\)HUWLO6WHULO
0XOOLQV7/6DQW*58FFL$$-U'RKHUW\)-7HVWLFX -lar microlithiasis occurring in postorchiopexy testis.
8URORJ\
7. 0DF.LQQRQ-7HVWLFXODUPLFUROLWKLDVLVHFKRJUDSKLF diagnosis of a new cause for orchialgia and infertility.
5HY0HG&KLO
.ZDQ'-.LUVFK$-&KDQJ'7*ROXERII(7%HUGRQ :(+HQVOH7:7HVWLFXODUPLFUROLWKLDVLVLQDFKLOGZLWK WRUVLRQRIWKHDSSHQGL[WHVWLV-8URO :DVQLHZVND0'H/XFD)%HUWHOORQL60DWDUD]]R3
:HEHU*&ULVDIXOOL*HWDO7HVWLFXODUPLFUROLWKLDVLV
an unreported feature of McCune-Albright syndrome
LQPDOHV-3HGLDWU
9DFKRQ/)DUHDX*(:LOVRQ0*&KDQ/67HVWLFX -lar microlithiasis in patients with Down syndrome. J
3HGLDWU
3DUHQWL*&=DJR6/XVD0&DPSLRQL30DQQHOOD 3$VVRFLDWLRQEHWZHHQWHVWLFXODUPLFUROLWKLDVLVDQG SULPDU\PDOLJQDQF\RIWKHWHVWLVRXUH[SHULHQFHDQG UHYLHZRIWKHOLWHUDWXUH5DGLRO0HG7RULQR
6KLFKLMR76DNDPRWR+6DLWR.2JDZD<<RVKLGD +.XVKLPD05HOHYDQFHRIWHVWLFXODUPLFUROLWKLDVLV
to the testicular carcinoma in situ in the contralateral
WHVWLFOH1LSSRQ+LQ\RNLND*DNNDL=DVVKL
541-6.
5DVKLG++&RV/5:HLQEHUJ(0HVVLQJ(07HV
-WLFXODUPLFUROLWKLDVLVDUHYLHZDQGLWVDVVRFLDWLRQZLWK WHVWLFXODUFDQFHU8URO2QFRO
Dr. Eugenio O. Gerscovich University of California Davis Medical Center Sacramento, California, USA E-mail: [email protected]
EDITORIAL COMMENT
In clinical practice, the greatest concern re-garding testicular microlithiasis (TM) is whether TM is a premalignant condition. The authors prospectively showed that the prevalence of testicular microlithiasis
70ZDVRIKHDOWK\PHQZKLFKPD\EH WKHPRVWLPSRUWDQW¿QGLQJLQWKLVVWXG\EHFDXVHWKH
true prevalence of TM in the general population has not yet been established. This study also showed that TM was not associated with the development of
tes-ticular tumors during the 12-month follow-up period. Moreover, the authors compared the resistance index (RI) between men with and without TM in order to evaluate the relationship between TM and testicular perfusion, while also showing that TM did not alter
WHVWLFXODUSHUIXVLRQZKLFK¿UVWO\VKRZHGEDVHGRQ WKH¿QGLQJVRIDODUJHFRKRUW
However, this study had some limitations
criteria were used in different studies including this
VWXG\ZKLFKPD\WKXVKDYHLQÀXHQFHGWKHSUHYDOHQFH
of TM. 2) While the etiology of TM has not yet been
YHUL¿HG70PD\RULJLQDWHIURPWKHGHJHQHUDWLRQRI
seminiferous tubules. Therefore, TM itself may be associated with an alteration of testicular perfusions. Moreover, the number and distribution of microliths may be related to testicular perfusion. 3) The number of men with TM is small. In addition, a failure to measure the RI was observed in about one-half of all males with and without TM. These factors may thus
KDYHLQÀXHQFHGWKHUHVXOWVDQGWKH\PD\DOVREHUHODWHG
to the impairment of testicular perfusion. Therefore, further study is necessary to verify the relationship between testicular perfusion and TM. 4) Few studies
have so far shown what the measurement of RI means in healthy men. Unfortunately, comparisons of the RI
¿QGLQJVEHWZHHQPHQZLWKDQGZLWKRXW70LQRUGHUWR
elucidate the relationship between TM and testicular
SHUIXVLRQPD\QRWEHLQIRUPDWLYHIRUUHDGHUV,WKLQN
that a study, which evaluates the testicular function
LQFOXGLQJWKHVHPHQSUR¿OHVPD\EHPRUHXVHIXOIRU
elucidating the relationship between TM and testicular perfusion.
Finally, TM itself and testicular tumors have
QRW\HWEHHQYHUL¿HGDVDSUHPDOLJQDQWFRQGLWLRQ
while TM has been reported to be associated with testicular tumors and carcinoma in situ. Therefore, the necessity of regular follow-up in normal men with TM has not yet been conclusively proven.