SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Update
Article
Diffuse
pigmented
villonodular
synovitis
in
knee
joint:
diagnosis
and
treatment
夽
Eduardo
Frois
Temponi
a,∗,
Antônio
Augusto
Guimarães
Barros
a,
Vinícius
Oliveira
Paganini
a,
Victor
Atsushi
Kasuya
Barbosa
a,
Roger
Badet
b,
Lúcio
Honório
de
Carvalho
Júnior
a,caHospitalMadreTeresa,BeloHorizonte,MG,Brazil
bPôleOstéoArticulaireSantéetSport,BourgoinJallieu,France
cUniversidadeFederaldeMinasGerais,FaculdadedeMedicina,DepartamentodoAparelhoLocomotor,BeloHorizonte,MG,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received29May2016 Accepted25July2016 Availableonline24June2017
Keywords:
Synovitis,pigmentedvillonodular Knee
Radiotherapy
a
b
s
t
r
a
c
t
Pigmentedvillonodularsynovitisisarareproliferativeconditionofthesynovium.Although theconditioncanpresentinanyjoint,thekneeisthemostcommonlyaffectedsite.Despite beingabenigncondition,pigmentedvillonodularsynovitisisoftenaggressive,withmarked extra-articularextensioninsomecases.Monoarticularinvolvementoccursintwoforms: localizedanddiffuse.Thelatterismorecommon,withahighrecurrencerate.Thereisno standardmethodofmanagementofthislesion.Opensurgeryisaclassicalandeffective methodfortreatment.Arthroscopicsynovectomy,however,hasgainedpopularity,andhas severaladvantagesovertheopentechniqueparticularlyinexclusivelyarticularcases.The combinedapproachissuggestedincaseswithextra-articularinvolvement.Synovectomy throughanyapproachmaypreventsecondaryosteoarthritisandsubsequentjoint arthro-plasty.Internalirradiationorexternalbeamradiationasanadjuvanttreatmenttosurgical synovectomyappearstodecreasetherateoflocalrecurrenceindiffusecases.Theauthors observedagreatheterogeneityinreportingoffunctionalresults,andspecificconclusions shouldnotbedrawn.Eachpatientshouldbemanagedinaccordancewithhis/herparticular condition.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudyconductedatHospitalMadreTeresa,BeloHorizonte,MG,Brazil.
∗ Correspondingauthor.
E-mails:[email protected],[email protected](E.F.Temponi).
http://dx.doi.org/10.1016/j.rboe.2017.06.008
Sinovite
vilonodular
pigmentada
difusa
no
joelho:
diagnóstico
e
tratamento
Palavras-chave:
Sinovitepigmentadavilonodular Joelho
Radioterapia
r
e
s
u
m
o
Asinovitevilonodularpigmentadaéumararacondic¸ãoproliferativadamembranasinovial. Apesar de a doenc¸apoder estar presente em qualquerarticulac¸ão, o joelhoé olocal maisfrequentementeafetado.Aindaquedoenc¸abenigna,geralmentetemcomportamento agressivo,podeterextensãoextra-articularemalgunscasos.Oacometimento monoartic-ularocorreemduasformas:localizadaoudifusa.Aformadifusaémaiscomumetemalta taxaderecorrência.Nãohámétodopadronizadoparaomanejodessalesão.Otratamento cirúrgicoabertoéométodoclássicoeefetivo.Asinovectomiaartroscópica,entretanto,tem ganhadopopularidadeetemdiversasvantagenssobreatécnicaaberta,principalmente emcasosexclusivamentearticulares.Aabordagemcombinadaésugeridaemcasoscom envolvimentoextra-articular.Asinovectomiapodepreveniraosteoartrosesecundáriaeo subsequentetratamentoreconstrutivo.Aradioterapiausadacomotratamentoadjuvante àsinovectomiaparecediminuirataxaderecorrêncialocalnaformadifusadadoenc¸a. Osautoresencontraramgrandeheterogeneidadenaformacomoosresultadosfuncionais foramreportadosenãosedevechegaraconclusõesespecíficas.Cadapacientedeveser manejadodeacordocomsuasparticularidades.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Pigmentedvillonodularsynovitis(PVNS)is arare prolifera-tiveprocessthataffectsthesynovialjoints,tendonsheaths, and bursas. In 1852, Chassaignac1 reported the first case ofa lesion inthe flexor tendonsheath of the second and thirdfingers;thiswassubsequentlyreportedinotherjoints. In1941,Jaffeetal.2 coinedtheterm“pigmented villonodu-larsynovitis”;subsequently,Granowitzetal.3 expandedthe terminology, distinguishing the localized (LPVNS) and dif-fuse(DPVNS)formsfromothersynoviallesions.Recently,the WorldHealthOrganizationhasdefinedPVNSandgiantcell tumortobeequivalentterms.4,5
TheestimatedincidenceofPVNSranges around1.8per million.6,7 Itisusuallymonoarticular,affectinglargejoints. Thekneeisthemostaffectedsite(28%–70%),butcasesinthe hip,ankle,shoulder,andelbowareoftenobserved.5,6,8The dis-easepresentsintwoforms,localizedordiffuse,andbothtypes havesimilarappearance:asynovialmembranecharacterized by inflammation and presence of hemosiderin deposits.3,9 Microscopically,itischaracterizedbythepresenceof lipid-ladenmacrophages,multinucleatedgiantcells,hemosiderin deposits, and proliferation of fibroblastsand stromal cells. LPVNSischaracterizedbydiscreteorpedunculatednodular lesions.Inturn,DPVNS isthe mostcommonpresentation, involvingintra-articulartissues;it mayhaveextra-articular extension,behavingasachronicprocess.10–12
In the last 100 years, little progress has been made regardingtreatment.ThegoalofPVNStreatmentistoremove allsynovialtissueinordertorelievepain,decreasetheriskof jointdestruction,andpreventlocalrecurrence.Several treat-mentoptionshavebeenproposedforthisdiseaseincasesof genicularinvolvement,rangingfromobservationandradical localsurgerytototalkneearthroplasty(Fig.1).4,5,8,13,14
Etiology
and
pathophysiology
The etiology ofPVNS isstill unknown. Some authors sug-gest thatthe diseaseoccurs asaresultofbaselinetrauma andsubsequentbleedingintheaffectedjoint.13–20 This the-ory issupportedbythe factthat patientswith hemophilia present progressivedestruction of the cartilage during the natural course of the disease. However, studies that pro-duced PVNS-like histological findings by injecting iron or bloodintothejointwereunabletoreplicatetheclassic lipid-laden histiocytes and giant cells.15 However, most studies reportedahistoryoftraumainlessthanone-thirdofpatients. Abnormalmetabolic activityhas alsobeen indicatedasan adjuvant event intheinflammationobserved inPVNS,but this isan inconsistent finding.16 There are alsoreports in theliteraturethatPVNSmaybeaneoplasticprocess.Several authorssuggestedthepresenceofchromosome7trisomyand clonal rearrangementsasa cause.11,17 Somereports, albeit rare, indicate the occurrence of malignant transformation andmetastasesinpatientsinitiallydiagnosedwithPVNS.17,18 DespitethecasereportsofmalignantPVNSandaneuploidy, thereisevidenceagainstthetheorythatPVNSisa neoplas-ticprocess.Intheiranalysis,Oehleretal.9observedastrong evidenceofchronicinflammation.Theirfindingswerebased on thepresenceofacellularmarkerofinflammationwith aheterogeneouspopulationofmononuclearcells.Theyalso postulatedthatthepresenceoflargeamountsofironinthe lesionwouldstimulatesynoviocytesandfibroblaststodevelop macrophage-likecharacteristics.
Fig.1–Diffusepigmentedvillonodularsynovitisoftheknee–preoperativeperiodofopenanterioraccesssurgery.
commonsiteofinvolvementisthesynoviumintheanterior hornregionofthemedialmeniscus.Patientswithlesionsin thislocationmaypresentsignsandsymptomssuggestiveof meniscal disease.If left untreated,LPVNS may cause pain and discomfortand limitthe patient’s activities and func-tions.Nostudies haveassessedthe long-termoutcomes in patientswithuntreatedLPVNS,probablyduetothelowrate ofrecurrenceandthefactthattheyareeasilytreated,oreven duetothelargeproportionofasymptomaticpatients.4,12,20–25 Manyauthorsagreethatthemarginalexcisionofthelesion results in good or excellent results, especially if treated early.5,7,21
DPVNS is characterized by the involvement of almost theentiresynovialtissueintheknee. Edemaand painare more significant than in LPVNS, and are generally poorly localized. DPVNS tends tobe moredestructive and conse-quentlyhaveaworseprognosis;itmaypresentextra-articular extensionatthe timeofthe primarydiagnosis or incases of recurrence.21 Extra-articular lesions may also involve neurovascular structures, making surgical resection more challengingandhinderingcompleteexcision.22,25–30Despite treatment, the recurrence rate is high, reaching around 46%.13,14,23
Clinical
presentation
PVNSistypicallyamonoarticularprocessthatusuallyaffects largejoints.PVNSgenerallyaffectspatientsinthethirdand fourthdecadeoflife.10,19Historically,itwasbelievedthatthis conditionwasmorecommoninmales,butrecentstudies indi-cated nogenderpreference.6,19 Itsclinical courseisaslow and insidiousonset ofpain, swelling, and stiffness in the involved joint.Diagnosis isoftendelayed orconfusedwith initialosteoarthrosis,rheumatoidarthritis,andmeniscalor ligamentousinjury.InbothDPVNSandLPVNS,symptomsare usuallyintermittent.4,12,19,20,30–36
Diagnosis
ThediagnosisofDPVNSisnotalwaysobvious.Inthestudiesby Flandryetal.,19only17%ofpatientswerecorrectlydiagnosed beforereferral.19,24Severalimagingmodalitiesareneededto ruleoutotherconditionsandestablishthediagnosis. Syno-vial fluid can be collected and analyzed by arthrocentesis (Table1).33–36 Other specificdiagnoses shouldberuledout. DPVNSdemonstratesnormalviscositywithvariedbleeding
Table1–Classificationofthesynovialfluidoftheknee.33–36
Normal Non-inflammatory Inflammatory Infectious Hemorrhagic
Volume(mL) <3.5 >3.5 >3.5 >3.5 >3.5
Viscosity High High Low Variable Low
Color Light,colorless Lightyellowish Yellowish Variable(opaque) Red
Leuc(mm3) <200 <2000 5000–75,000 >50,000 Similarbloodlevel
Pols(%) <25 <25 50–70 >70 Similarbloodlevel
Gram Negative Negative Negative Often+ Negative
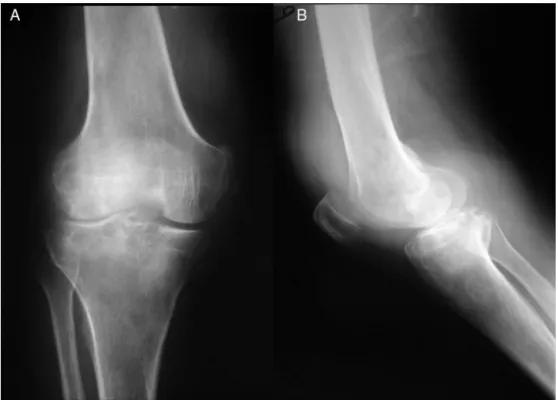
Fig.2–Kneeradiographofadiffusepigmentedvillonodularsynovitisofthekneein(A)antero-posteriorand(B)profile,
evidencingareasofbonedestruction.
Fig.3–Magneticresonanceimagingofakneewithdiffusepigmentedvillonodularsynovitisoftheknee.AandB,coronal
cutinT1;C,sagittalsectioninT1;D,T1axialcutwithareasofdiffusesynovitiswithtibialandfemoralboneinvasion,
resultinginsignificantjointdestruction.
patterns,andradiographscanbeuseful(Fig.2),astheymay showperiarticularerosionswithathinlayerofreactivebone. Thelateradiographicfindingofjointspacenarrowing indi-cates loss of articular cartilage, which may be difficult to differentiatefromprimaryosteoarthrosis.Radiographic find-ings can be observed in up to 30% ofpatients.4,19,20 More recently,magneticresonanceimaging(MRI)hasbecomethe imagingmodalityofchoicefordiagnosingDPVNS.25Thisisa
PVNS
DPVNS
DPVNS with low risk of recurrence
Total arthroscopic synovectomy
Without adjuvant radiotherapy
Assess the use of adjuvant radiotherapy due to recurrence risk
Assess the use of adjuvant radiotherapy due to recurrence risk Total arthroscopic synovectomy, total open synovectomy or combined
with arthroscopic (case -by-case assessment) Total arthroscopic
synovectomy, total open synovectomy or combined
with arthroscopic (case -by-case assessment)
DPVNS with high risk of recurrence
DPVNS with extra -articular involvement
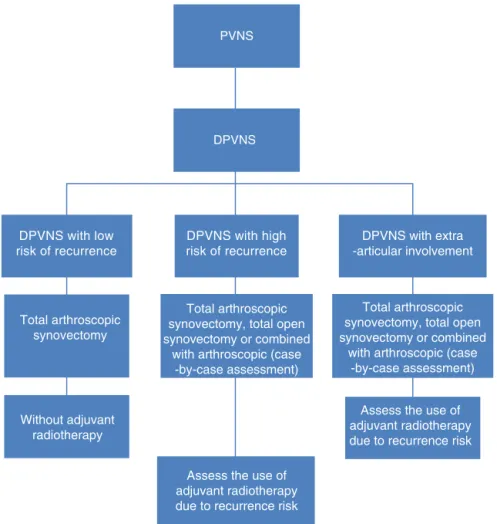
Fig.4–Flowchartofthetreatmentfordiffusedpigmentedvillonodularsynovitisoftheknee(theauthors’preferred
treatmentoption,basedonliteraturereview).7,14,33–36
Observation:Theriskofrecurrenceshouldbeassessedbasedonthedegreeofinvolvementoftheanteriorandposterior
compartmentsofthekneejoint,theeffectiveresectioncapacityofalllesions,andthesurgeon’sexperienceinthetreatment
oftheselesions.7,14,33–36
isdescribedas“darkondark”onT1andT2images,butinitial lesionswithlesshemosiderinmayhaveahighsignalonT2 sequences(Fig.3).4,25
Treatment
of
DPVNS
Historically,non-surgicalprocedures were the treatmentof choiceforDPVNS,andledtohighratesofrecurrence.26 How-ever,advancesinsurgicaltechniquesandpostoperativecare haveconsiderablyreducedthefrequencyofrecurrenceand complications,makingsurgicaltreatmentthefirstchoicein mostpatients.5,13
Non-surgical
Thehigh rates ofrecurrenceand complications associated withDPVNSmanagementledearlyinvestigatorstoadvocate observationuntiltotalarthroplastybecamenecessary. Recur-rentcasesdiagnosedonimagingtests,butwithoutprogressive synovitis,maynotrequireanewsynovectomy.However,such patientsshouldbefollowed-upmoreclosely.2,6,26
Radiotherapymaybeindicatedincaseswheretotal syn-ovectomy and complete resectionofextra-articular lesions cannot be performed, although some studies have dis-cussedthelong-termresultsofthisstrategywhenappliedin isolation.22,27,28
Surgicaltreatment
ManytreatmentoptionshavebeendescribedforDPVNSofthe knee.However,totalsynovectomyisconsideredthebasisof treatmenttopreventlocalrecurrence.Nospecificconclusions shouldbedrawnastowhichtechniqueshouldbeused,and eachpatientshouldbemanagedaccordingtotheirparticular case(Fig.4).
Arthroscopicapproach
DPVNS,theanterior compartmentistypicallyinvolvedand requires greater technical care from the surgeon, making complementaryportalstothetraditionalportalsmade ante-riorly,andusing30◦ and70◦ arthroscopes.33–36Patientswith
largemassesinthepoplitealfossaorextra-articular involve-mentgenerallyarenotcandidatesforexclusivelyarthroscopic approach. Arthroscopic treatment should be reserved for patientswithlimited,purelyintra-articulardisease.34–36 Dis-easeassessmentandchoiceofbesttreatmentscheduleshould be made with MRI before the definitive resection. If the arthroscopicapproachisselected,acomplete synovectomy, includingtheposteriorcompartments,shouldbeperformed inordertominimizetheriskofrecurrence.20,23,34
Twosimilar-sizedgroupsofpatientswereidentifiedinthe reviewbyAureganetal.34:localrecurrenceswere observed in28 of124 patients (23%)in the open surgerygroup and intwentyof124(16%)inthegroupthatunderwent arthro-scopicsurgery,inmeanfollow-upperiodsofsixandfiveyears, respectively. Thelower recurrencerate in the arthroscopic groupcan beexplained bythe shorterfollow-up period in thisgroup.Nonetheless,ahigherrateofpostoperative com-plicationswas reportedin the groupthat underwent open totalsynovectomywhencomparedwiththegroup submit-ted to arthroscopy. Functional scores appear to be better inthearthroscopic group;however,asdiscussedearlier,no convincingconclusioncanbedrawn.Thisstudy concluded thatposterioropentreatment,togetherwithanterior arthro-scopicsynovectomy,isaviableapproachforDPVNSofthe knee,withlowrecurrenceratesandfewpostoperative com-plications.Basedontheseresults,thearthroscopicapproach for arthroscopic synovectomy is recommended whenever technically possible. Colman et al.33 reported 48 cases of patientstreatedusingthearthroscopic,posterioropenwith anterior arthroscopic,or anterior open and posterior open synovectomytechniques.Recurrencerateswerelowerinthe open/arthroscopic group when compared with the arthro-scopic or with the open/open groups: 9% vs. 62% vs. 64%, respectively.Osteoarthrosisprogressionwasobservedin17% ofthetotalofpatients, 8%ofwhom underwent totalknee arthroplastyduringthefollow-upperiod.33
Althougharthroscopy is a less invasive procedure, it is notfreeofpotentialcomplications.Inadditiontotheriskof recurrence,arthroscopicexcisionpresentsthetheoreticalrisk ofjointtumordispersionandportalcontamination.Afailed arthroscopicapproachmaycauseextensivejointinvolvement andextra-articulardissemination.20,21,23,34–36
Openapproach
Theopenapproachfollowedbycompletesynovectomyisthe standardsurgicaltreatmentforDPVNSoftheknee.Patients withextensiveextra-articularinvolvementandlargemasses inthepoplitealfossaclearlyarenotsuitablecandidatesfor arthroscopicsynovectomy.Moreover,openproceduresshould be considered for patients with disease in hard-to-reach places,suchasthepoplitealtendonsheath,betweenthe gas-trocnemiusheads,and withinthe semimembranousbursa. Open treatment begins with an anterior approach, arthro-tomy,andaggressiveanterior synovectomy,followed byan S-shaped posterior approach, protecting the neurovascular
structures.Subsequently,jointandextra-articularexploration shouldbeconductedinordertoavoidanyremainingtumor tissue.9,21,23,24,34–36
Oldstudiesassessingopentreatmentreportedexcessively highratesofrecurrence.Nonetheless,inthesestudies recur-renceprobablyindicatedincompleteexcisionsofthelesions andlikelyreferredtoinadequatesurgicalexposure.Flandry etal.19reportedaseriesof25kneeswithbiopsyandproven DPVNS that were treated by double open approach. The authorsreportedarecurrencerateof8%inafollow-upof58 months.
Open treatment, however, isnot freeofrisks and com-plications.Comparedwiththearthroscopicprocedure,open synovectomy is associated with longer hospital stay and longer rehabilitation period. Oneof the maincriticisms of the open procedure ispostoperative stiffness, which often requires manipulation under anesthesia. In the study by Flandryetal.,19therateofpostoperativestiffnesswas24%. Therefore,manyexpertsadvocatetheuseoflessinvasiveand lessaggressiveprocedures.19,34
Combinedopenandarthroscopicapproach
Thecombinationofopenandarthroscopicapproachhasnot beenwelldescribedintheliterature.Patientswithposterior involvementassociatedwithminimalanteriorinvolvement may benefitfrom anterior arthroscopic synovectomy com-bined with posterior open synovectomy. Another suitable scenario for the combined approach is in cases in which totalsynovectomybyarthroscopicapproachaloneis impossi-ble. Inthis scenario,severalauthorssuggest acombination of anterior arthroscopic synovectomy and open posterior synovectomy.5,7,14Moreover,arthroscopymayplayan impor-tantroleinthepre-andpostoperativediagnosis,aswellasin thetreatmentofresidualdiseaseafteropensurgery.De Car-valho etal.14 reportedthatpatientsdiagnosedwithDPVNS treatedwithpartialarthroscopicsynovectomycombinedwith anterior open synovectomypresented arecurrence rate of 12.5%inameanfollow-upof8.6years;nomajorcomplications wereobservedduringfollow-up.14
Adjuvantradiotherapy
Radiotherapyhasbeenusedformanyyearsasanalternative to surgical synovectomyin patients with nonspecific syn-ovitis. Radiation-induced synovectomyin the treatment of DPVNShasbeenincreasinglydiscussed,butwithconflicting results.14,23,28,29 From1950onwards,goodresultshavebeen reported with use of adjuvant external radiation in the managementofrecurrentDPVNS.30Potentialcomplications are associatedwithexternalradiation,includingskin reac-tions, poor wound healing, joint stiffness, and neoplastic transformation.31–36
periodof8.6years.14Blancoetal.29described22patientswith knee DPVNS treated with arthroscopic synovectomy com-bined with postoperative external radiotherapy (total dose of2600cGy).Therecurrenceratewas13.62%;thesepatients underwent a second surgical procedure. Ustinova et al.31 describedtheirexperiencewith24patientswithDPVNS. Radi-ation(intwodoses,oneof1.2–1.5cGyinfivefractionsanda focaldoseof16–20cGy)wasapplied,sincetheaffected syno-vialtissuehadnotbeencompletelyremovedduringsurgery. Norecurrenceswereobservedinthefollow-upperiod,which rangedfromsixmonthstosixyears,andoccupational reha-bilitationwasachievedin87.5%ofthepatients.31O’Sullivan et al.22 also reported the cases of 14 patients with intra-andextra-articularlesionswhoreceivedadjuvantradiation. ThoseauthorsconcludedthatafterDPVNSremoval,theuse ofmoderateexternalradiationwasveryeffectivein preven-tingrecurrence,avoidingamputationinadvancedcasesand preservinglimbfunction.
Localradiotherapycanalsobeappliedwithintra-articular radioisotopeinjection.Chinetal.21assessedalargenumber ofpatients(n=40)withDPVNS,eachsubjectedtoeitheropen orarthroscopicsurgery,but whopresentedrecurrence.The numberofresiduallesionsinthegroupstreatedwith radio-therapywaslowerthanintheuntreatedgroup.Shabatetal., inameanfollow-upofsixyears,assessedtenpatientswith DPVNSwho underwent oneormorepartialsynovectomies andreceivedintra-articularinjectionofyttriumisotope(90Y; 15–25mCi)betweensixandeightweeksafterthelastsurgery. Inninepatients,noevidenceofrecurrencewasobserved dur-ingfollow-up,whereasinonepatientthediseasestabilized.32
Final
considerations
DPVNS of the knee is a rare condition in which treat-ment may be associated with a significant risk of local recurrence,postoperativecomplications,andfunctional lim-itations.Regardinglocalrecurrence,therewasnodifference intheliteraturebetweenopenorarthroscopictotal synovec-tomyforthetreatmentofDPVNS.However,alower rateof complicationswasreportedafterarthroscopicsynovectomy. IncompletesynovectomyforthetreatmentofDPVNSshould notbeperformedinisolation,duetothehighriskof recur-rence.Internalorexternalradiationasanadjuvanttreatment method to surgical synovectomy appears to decrease the rateoflocalrecurrenceincasesofDPVNS.CasesofDPVNS withextra-articularinvolvementshouldbetreatedwithtotal synovectomy, open excision of extra-articular lesions, and adjuvantradiotherapytreatment.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgments
ToallresearchersandtoDr.GuilhermeReisforhaving autho-rizedtheuseofthearchiveimagesinthisarticle.
r
e
f
e
r
e
n
c
e
s
1.ChassaignacEP.Cancerdelagainedestendons.GazHopCiv Milit.1852;25:185–6.
2.JaffeHL,LichtensteinI,SutroCJ.Pigmentedvillonodular synovitis,bursitisandtenosynovitis:adiscussionofthe synovialandbursalequivalentsofthetenosynoviallesion commonlydenotedasxanthoma,xanthogranuloma,giant celltumorormyeloplaxomaoftendonsheathwithsome considerationofthistendonsheathlesionitself.ArchPathol. 1941;31:731–65.
3.GranowitzSP,MankinHJ.Localizedpigmentedvillonodular synovitisoftheknee.Reportoffivecases.JBoneJointSurg Am.1967;49(1):122–8.
4.JendrissekKA,HotfielT,SwobodaB,SoderS,JankaR. Pigmentedvillonodularsynovitis:araredifferentialdiagnosis ofsynovialjointswelling.ZRheumatol.2016;75(2):157–65.
5.Rodriguez-MerchanEC.Reviewarticle:openversus arthroscopicsynovectomyforpigmentedvillonodular synovitisoftheknee.JOrthopSurg(HongKong). 2014;22(3):406–8.
6.MyersBW,MasiAT.Pigmentedvillonodularsynovitisand tenosynovitis:aclinicalepidemiologicstudyof166casesand literaturereview.Medicine(Baltimore).1980;59(3):223–38.
7.YangB,LiuD,LinJ,JinJ,WengXS,QianWW,etal.Surgical treatmentofdiffusepigmentedvillonodularsynovitisofthe knee.ZhongguoYiXueKeXueYuanXueBao.
2015;37(2):234–9.
8.SherryJB,AndersonW.Thenaturalhistoryofpigmented villonodularsynovitisoftendonsheaths.JBoneJointSurg Am.1955;37-A(5):1005–11.
9.OehlerS,FassbenderHG,NeureiterD,Meyer-ScholtenC, KirchnerT,AignerT.Cellpopulationsinvolvedinpigmented villonodularsynovitisoftheknee.JRheumatol.
2000;27(2):463–70.
10.deVisserE,VethRP,PruszczynskiM,WobbesT,VandePutte LB.Diffuseandlocalizedpigmentedvillonodularsynovitis: evaluationoftreatmentof38patients.ArchOrthopTrauma Surg.1999;119(7–8):401–4.
11.PerkaC,LabsK,ZippelH,ButtgereitF.Localizedpigmented villonodularsynovitisofthekneejoint:neoplasmorreactive granuloma?Areviewof18cases.Rheumatology(Oxford). 2000;39(2):172–8.
12.BouguennecN,MeyerA,GraveleauN.Localizedformof pigmentedvillonodularsynovitisoftheknee:themeniscal mime.OrthopTraumatolSurgRes.2014;100(2):251–4.
13.MollonB,GriffinAM,FergusonPC,WunderJS, TheodoropoulosJ.Combinedarthroscopicandopen synovectomyfordiffusepigmentedvillonodularsynovitisof theknee.KneeSurgSportsTraumatolArthrosc.
2016;24(1):260–6.
14.deCarvalhoLHJr,SoaresLF,GoncalvesMB,TemponiEF,de MeloSilvaOJr.Long-termsuccessinthetreatmentofdiffuse pigmentedvillonodularsynovitisofthekneewithsubtotal synovectomyandradiotherapy.Arthroscopy.
2012;28(9):1271–4.
15.SinghR,GrewalDS,ChakravartiRN.Experimentalproduction ofpigmentedvillonodularsynovitisinthekneeandankle jointsofrhesusmonkeys.JPathol.1969;98(2):137–42.
16.HirohataK.Lightmicroscopicandelectronmicroscopic studiesofindividualcellsinpigmentedvillonodularsynovitis andbursitis(Jaffe).KobeJMedSci.1968;14(4):251–79.
18.BertoniF,UnniKK,BeaboutJW,SimFH.Malignantgiantcell tumorofthetendonsheathsandjoints(malignantpigmented villonodularsynovitis).AmJSurgPathol.1997;21(2):153–63.
19.FlandryF,HughstonJC,McCannSB,KurtzDM.Diagnostic featuresofdiffusepigmentedvillonodularsynovitisofthe knee.ClinOrthopRelatRes.1994;(298):212–20.
20.AkgunI,OgutT,KesmezacarH,DervisogluS.Localized pigmentedvillonodularsynovitisoftheknee.Orthopedics. 2003;26(11):1131–5.
21.ChinKR,BarrSJ,WinalskiC,ZurakowskiD,BrickGW. Treatmentofadvancedprimaryandrecurrentdiffuse pigmentedvillonodularsynovitisoftheknee.JBoneJoint SurgAm.2002;84(12):2192–202.
22.O’SullivanB,CummingsB,CattonC,BellR,DavisA,Fornasier V,etal.Outcomefollowingradiationtreatmentforhigh-risk pigmentedvillonodularsynovitis.IntJRadiatOncolBiolPhys. 1995;32(3):777–86.
23.NassarWA,BassionyAA,ElghazalyHA.Treatmentofdiffuse pigmentedvillonodularsynovitisofthekneewithcombined surgicalandradiosynovectomy.HSSJ.2009;5(1):19–23.
24.FlandryFC,HughstonJC,JacobsonKE,BarrackRL,McCann SB,KurtzDM.Surgicaltreatmentofdiffusepigmented villonodularsynovitisoftheknee.ClinOrthopRelatRes. 1994;(300):183–92.
25.DaleK,SmithHJ,PausAC,RefsumSB.DynamicMR-imaging inthediagnosisofpigmentedvillonodularsynovitisofthe knee.ScandJRheumatol.2000;29(5):336–9.
26.ByersPD,CottonRE,DeaconOW,LowyM,NewmanPH, SissonsHA,etal.Thediagnosisandtreatmentofpigmented villonodularsynovitis.JBoneJointSurgBr.1968;50(2):290–305.
27.ParkG,KimYS,KimJH,LeeSW,SongSY,ChoiEK,etal. Low-doseexternalbeamradiotherapyasapostoperative treatmentforpatientswithdiffusepigmentedvillonodular synovitisoftheknee:4recurrencesin23patientsfollowed formean9years.ActaOrthop.2012;83(3):256–60.
28.HeydR,SeegenschmiedtMH,MickeO.Theroleofexternal beamradiationtherapyintheadjuvanttreatmentof pigmentedvillonodularsynovitis.ZOrthopUnfall. 2011;149(6):677–82.
29.BlancoCE,LeonHO,GuthrieTB.Combinedpartial
arthroscopicsynovectomyandradiationtherapyfordiffuse pigmentedvillonodularsynovitisoftheknee.Arthroscopy. 2001;17(5):527–31.
30.FriedmanM,SchwartzEE.Irradiationtherapyofpigmented villonodularsynovitis.BullHospJointDis.1957;18(1):19–32.
31.UstinovaVF,PodliashukEL,RodionovaSS.Combined treatmentofthediffuseformofpigmentedvillonodular synovitis.MedRadiol(Mosk).1986;31(3):27–31.
32.ShabatS,KollenderY,MerimskyO,IsakovJ,FlusserG,Nyska M,etal.Theuseofsurgeryandyttrium90inthe
managementofextensiveanddiffusepigmented
villonodularsynovitisoflargejoints.Rheumatology(Oxford). 2002;41(10):1113–8.
33.ColmanMW,YeJ,WeissKR,GoodmanMA,McGoughRL3rd. Doescombinedopenandarthroscopicsynovectomyfor diffusePVNSofthekneeimproverecurrencerates?Clin OrthopRelatRes.2013;471(3):883–90.
34.AureganJC,KloucheS,BohuY,LefevreN,HermanS,HardyP. Treatmentofpigmentedvillonodularsynovitisoftheknee. Arthroscopy.2014;30(10):1327–41.
35.NakaharaH,MatsudaS,HarimayaK,SakamotoA, MatsumotoY,OkazakiK,etal.Clinicalresultsofopen synovectomyfortreatmentofdiffusepigmentedvillonodular synovitisoftheknee:caseseriesandreviewofliterature. Knee.2012;19(5):684–7.