r e v b r a s o r t o p . 2016;51(4):478–481
SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Case
Report
Arthroscopic
surgical
treatment
of
pigmented
villonodular
synovitis
of
the
elbow:
case
report
夽
Marlon
Araujo
Ramos,
Niso
Eduardo
Balsini
∗,
Fernando
Ramos,
Luiz
Gustavo
Machado
InstitutoBalsini,Joinville,SC,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received22August2015 Accepted23September2015 Availableonline12July2016
Keywords:
Pigmentedvillonodularsynovitis Arthroscopy
Elbow
a
b
s
t
r
a
c
t
Thiscaseconcernsamalepatientcomplainingofpainanddiscomfortinhisrightelbow, associatedwithdecreasedrangeofmotion.Elbowradiographyshowedanosteolyticlesion inthemetaphysealregionofthedistalhumerusandmagneticresonanceimagingshowed intra-articulartumorformationwithswellingthatsuggestedpigmentedvillonodular syn-ovitis.Arthroscopictreatmentwasperformedinordertoobtainasynovialbiopsyandthen tocarryouttotalsynovectomy.Anatomopathologicalexaminationconfirmedthe diagno-sis.Thepatientpresentedexcellentprogressthroughthephysiotherapeuticrehabilitation proposedandcontinuedtobeasymptomatic12monthsaftertheoperation.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Tratamento
cirúrgico
artroscópico
de
sinovite
vilonodular
pigmentada
de
cotovelo:
relato
de
caso
Palavraschave:
Sinovitevilonodularpigmentada Artroscopia
Cotovelo
r
e
s
u
m
o
Ocasodizrespeitoaumpacientedosexomasculinocomqueixadedoredesconfortono cotovelodireitoassociadosadiminuic¸ãodaamplitudedemovimento.Apresentava radio-grafiadocotovelocomlesãoosteolíticadaregiãometafisáriadoúmerodistaleressonância magnéticaquemostravatumorac¸ãointra-articularcomaumentodevolumequesugeria sinovitevilonodularpigmentada.Foifeitotratamentoartroscópicoparabiópsiasinovial esinovectomiatotal.Oestudoanatomopatológico confirmouodiagnóstico.Opaciente apresentouótimaevoluc¸ãocomreabilitac¸ãofisioterápicaproposta,até12mesesde pós-operatorioapresentava-seassintomático.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevierEditora Ltda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudyconductedatInstitutoBalsini,Joinville,SC,Brasil.
∗ Correspondingauthor.
E-mail:[email protected](N.E.Balsini). http://dx.doi.org/10.1016/j.rboe.2016.07.001
r e v b r a s o r t o p . 2016;51(4):478–481
479
Introduction
Pigmentedvillonodularsynovitis(PVNS)isararelesionthat appears as a proliferative process, affecting the synovial joints,tendonsheaths,andbursalmembranes.In1852,itwas describedbyChassaignacapudByersetal.1attheflexor
ten-donsofthemiddleandindexfingers.Itpresentsmainlyas asingle-jointform;itismoreprevalentinthekneejointand hasdifferentprognoses.
Elbowinvolvementisuncommon,with24casesreported intheliterature2,3;thereisnoconsensusregardingtreatment,
whichcanbeconservative,openorarthroscopicsurgical syn-ovectomy,andsynovectomybyradiotherapy.2,4
Opensynovectomyhasbeenassociatedwithriskof infec-tion,suturedehiscence,andjointstiffnessduetothedifficulty ofrehabilitationcaused bypain or instability. Theauthors usedafullyarthroscopicmethodforthediagnosisofelbow PVNSandtreatmentwithsynovectomy.
Clinical
case
Malepatient,43yearsold,white,businessman,sought treat-mentforpainandmovementlimitationoftherightelbowthat hadinitiatedsixmonthsprior.Clinicalexaminationshowed no deformities, 30◦ ofextension and 120◦ of flexion
(con-tralateral0–140◦),painonpalpationofthelateralepicondyle
andolecranon,andanegativeCozentest.Valgusandvarus maneuversshowednoligamentinstabilityandaTinelsign wasnegativefortheulnarnerve.
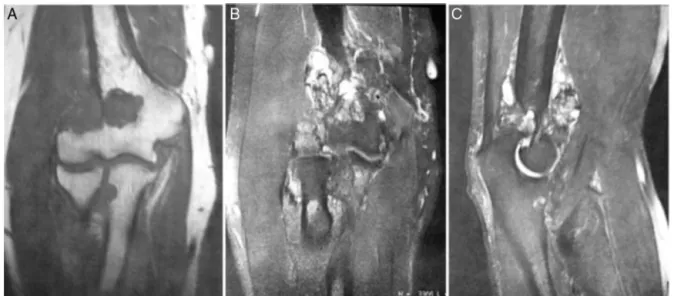
Radiographs(RX)weremadeonfirstpresentation,followed bymagneticresonanceimaging(MRI).RXinanteroposterior and lateral views (Fig. 1) indicated an osteolytic lesion of thedistalmetaphyseal regionofthehumerus. MRIshowed
extensivetissuewithhyposignalontheT1-weightedimage and sharp hyposignal on the T2-weighted intra-articular image that increased after contrast injection (gadolinium). Marginal erosions in the radius, ulna, and humerus were observed,aswellaselbowjointirregularity(Fig.2).
ThecharacteristicsoftheimagesledtosuspicionofPVNS. Thevideoarthroscopicmethodwasindicatedfordirect evalu-ation,fragmentcollectionforanalysis,andtotalsynovectomy, inasingleprocedure.
Thus,thepatientunderwentrightelbowarthroscopy.He waspositionedinthepronepositionwiththeelbowsupported and loosen for mobilization; the anteromedial, anterolat-eral, posterior, and posterolateral portals were used. The anteriorandposteriorcompartmentswereassessed.The syn-oviumhadanodularcharacteristic,withspongytextureand brownish-yellowcolor(Fig.3);afreebodywasremovedinthe posteriorcompartment.Materialforpathologicalanalysiswas harvested;asynovectomyandacapsulotomywereperformed aiminggainofrangeofmotion(Fig.4).Then,skinsuturingwas performedwithmononylonanddressing;immobilizationwas notused.Thecollectedmaterialwassenttohistologic analy-sis,whichconfirmedthepre-establisheddiagnosisofPVNS.
Thepost-operativerehabilitationwasinitiatedinthefirst week,focusingongainofpassiverangeofmotion.5 Patient
evolved with little pain, but showed local swelling that persistedfortwoweeks.Rangeofmotioninthethird postop-erativedaywas15◦degreesofextensionandevolvedto5◦at
theendofthesixthweekpostoperatively.Inthetwelfthweek aftersurgery,thepatientpresentedrangeofmotionof3◦of
extensionand140◦offlexion;hewasasymptomaticand
per-formedhisprofessionalactivitieswithoutdeficits.Anelbow MRIwasperformed14monthspostoperative,andpresented noevidenceofpathologicalsynovialtissueneoformation, sug-gestinglackofrecurrence.
480
r e v b r a s o r t o p . 2016;51(4):478–481Fig.2–Magneticresonanceimagingoftherightelbow.(A)coronalplaneinT1;(B)coronalplaneinT2;and(C)sagittalplane
inT2.
Fig.3–Arthroscopicimageoftheelbowshowing
villonodularsynovitisaspect.
Discussion
TheoriginsofPVNSarestillunclear.Thereareseveral theo-riesthataimtoexplainit,includingrecurrenthemarthrosis, inflammatoryresponseto anunknownagent, cancer,lipid metabolismdisorder,oraresponsetorepeatedtrauma.None havebeenprovenorareundisputed.6
Itcanbedividedinto twomajortypes:thediffuseform, whichismonoarticularand affectsthe knee,hip, ankle,or rarelytheelbow;andthelocalizedform,whichisrestrictedto thetendonsofthefingers.4
Itsincidenceis1.8casesper1,000,000,andaffects primar-ilythe knee. There are24 casesdescribed inthe literature involvingtheelbow.2,3
Symptomsdescribedarepain,swellingandjointeffusion, decreasedrangeofmotion,andevenpalpablemass, depend-ingontheextentionandvolumeofsynovitis.Thesesignsand symptomspresentaslowandprogressivedevelopment.6,7
Fig.4–Arthroscopicimageoftheelbowaftersynovectomy.
Presenceofboneerosioninthemetaphysealregionofthe
distalhumerus.
Thetreatmentprincipleisbasedontheremovalof patho-logical synovialtissuebytotal synovectomy,whichmaybe surgicalorthroughradiotherapytreatment.Inmoreadvanced caseswithjointdamage,arthroplastyorarthrodesismaybe necessary.8
Instudiesofthekneejointthatcomparedarthroscopic syn-ovectomywithopentechniquefortreatingdiffusePVNS,the recurrenceresultsareequivalent:16.1%forarthroscopic syn-ovectomy,22.6%foropensynovectomy,and25%forcombined synovectomy(arthroscopicandopen).9
Inthepresentcase,accordingtotheMRI,thepatienthad small jointalterationand itsinvolvementwasrestrictedto theintra-articularspace.Theauthorsoptedforacompletely arthroscopic synovectomyfordiagnosisand treatment,not associatedwithradiotherapymethods.
r e v b r a s o r t o p . 2016;51(4):478–481
481
nodular masses. The color varies from brownish-red (sec-ondarybleeding)toyellow-orange(secondarytothepresence oflipids).7Thedefinitivediagnosisisbyhistology,which
fea-turesinfiltratedpolyhedralhistiocyticcells,fibroblasts,giant cells,andmacrophagesfilledwithhemosiderinorlipids(foam cells). Hemosiderin is observed among cells, synovial lin-ing cells, and histiocytes. Although PVNS is considered a benigninflammatoryprocess,mitoticfiguresareeasilyfound inproliferatingfibroblasts,macrophages,andsynoviallining cells.6,7
Inconclusion,anextremelyrarecaseofPVNSoftheelbow wasdiagnosedandtreatedusingafullyarthroscopicmethod.
Total synovectomy and capsulotomy were performed; the
patient progressed with favorable evolution, full range of motion,andwithoutpain.Afollow-upwithMRIwillbe con-ductedeverysixmonthsforlocalrecurrencecontrol.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.ByersPD,CottonRE,DeaconOW,LowyM,NewmanPH,Sissons HA,etal.Thediagnosisandtreatmentofpigmented
villonodularsynovitis.JBoneJointSurgBr.1968;50(2): 290–305.
2.PimpalnerkarA,BartonE,SiblyTF.Pigmentedvillonodular synovitisoftheelbow.JShoulderElbowSurg.1998;7(1): 71–5.
3.KotoK,MurataH,SakabeT,MatsuiT,HorieN,SawaiY,etal. Magneticresonanceimagingandthallium-201scintigraphyfor thediagnosisoflocalizedpigmentedvillonodularsynovitis arisingfromtheelbow:acasereportandreviewofthe literature.ExpTherMed.2013;5(5):1277–80.
4.WyattMC,RoltonN,VealeGA.Pigmentedvillonodular synovitisoftheelbowwithafenestratedfossa:acasereport.J OrthopSurg(HongKong).2009;17(1):127–9.
5.WilkKE,ArrigoC,AndrewsJR.Rehabilitationoftheelbowin thethrowingathlete.JOrthopSportsPhysTher.
1993;17(6):305–17.
6.DorwartRH,GenantHK,JohnstonWH,MorrisJM.Pigmented villonodularsynovitisofsynovialjoints:clinical,pathologic, andradiologicfeatures.AJRAmJRoentgenol.
1984;143(4):877–85.
7.SparksL.Sinovitevilonodular.In:WeinsteinLS,BuckwalterAJ, editors.OrtopediadeTurek:princípiosesuaaplicac¸ão.5◦ed.
Barueri,SP:Manole;2000.p.195–7.
8.SekiyaH,OzawaH,SugimotoN,KariyaY,HoshinoY. Pigmentedvillonodularsynovitisoftheelbowina6-year-old girl:acasereport.JOrthopSurg(HongKong).2007;15(1): 106–8.