SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Case
Report
Total
knee
replacement
in
patients
with
diffuse
villonodular
synovitis
夽
Lucio
Flávio
Biondi
Pinheiro
Junior
a,∗,
Marcos
Henrique
Frauendorf
Cenni
a,
Rafael
Henriques
Soares
Leal
b,
Luiz
Eduardo
Moreira
Teixeira
caRedeMaterDeideSaúde,BeloHorizonte,MG,Brazil
bHospitaldaUnimed,BeloHorizonte,MG,Brazil
cUniversidadeFederaldeMinasGerais,HospitaldasClínicas,BeloHorizonte,MG,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received8July2016 Accepted16August2016 Availableonline14August2017
Keywords:
Villonodularpigmentedsynovitis Arthroscopy
Knee
Giantcelltumors
a
b
s
t
r
a
c
t
Thispaperreportsacaseofdiffusepigmentedvillonodularsynovitis(DPVNS),associated withadvancedgonarthrosis,submittedtototalkneereplacement.Thepatienthad progres-sivepainandswelling.Shehadtwoprevioussurgeries,firstlyarthroscopicsynovectomyand subsequentlyopensynovectomyassociatedwithradiotherapy,withrecurrenceofthe dis-ease.Magneticresonanceimagingrevealeddiffusesynovitis,advancedarthrosis,andbone cysts.Thepatientwassubmittedtoatotalkneereplacementandsynovectomy.Therewas agoodpostoperativeclinicalcourse,withimprovementofpain,function,andjointedema onexamination.Thepatientwillbefollowedregardingthepossibilityofdiseaserecurrence andimplantsurvival.
©2017PublishedbyElsevierEditoraLtda.onbehalfofSociedadeBrasileiradeOrtopedia eTraumatologia.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Artroplastia
total
do
joelho
em
paciente
com
sinovite
vilonodular
pigmentada
forma
difusa
Palavras-chave:
Sinovitepigmentadavilonodular Artroscopia
Joelho
Tumoresdecélulasgigantes
r
e
s
u
m
o
Estetrabalhorelataumcasodesinovitevilonodularpigmentadaformadifusa(SVNPD), associadaa genoartrose avanc¸ada, que foi submetida a artroplastiatotal dojoelho. A pacienteapresentavadoreedemaemjoelhodecaráterprogressivo,jásubmetida previ-amenteaduassinovectomias,umaporviaartroscópicaeoutraporviaaberta,alémde radioterapia,comrecidivadadoenc¸a.Asradiografiasdemonstravamobliterac¸ãodosespac¸os
夽
PaperdevelopedatthenetworkMaterDeideSaúde,BeloHorizonte,MG,Brazil. ∗ Correspondingauthor.
E-mail:[email protected](L.F.PinheiroJunior).
http://dx.doi.org/10.1016/j.rboe.2017.08.002
articulares,alémdeerosõesecistosintraósseosnatíbiaenofêmur.Ressonânciamagnética evidenciousinovitedifusaextensa,alémdeartroseavanc¸adaecistosósseos.Apacientefoi submetidaaartroplastiatotaldojoelhocombinadacomsinovectomiaampla.Ela apresen-touboaevoluc¸ãoclinicapós-operatória,commelhoriadador,dafunc¸ãoedoedema.A pacienteseráacompanhadaquantoàpossibilidadederecorrênciadadoenc¸aesobrevida doimplante.
©2017PublicadoporElsevierEditoraLtda.emnomedeSociedadeBrasileirade OrtopediaeTraumatologia.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Pigmentedvillynodularsynovitisisarare, benignand pro-liferativediseaseofthesynovialtissueofuncertainetiology thatcandeterminethedestructionofjointcartilageandresult inosteoarthrosis.1Simondescribedthelocalizedtypeofthe knee andMoser, in1909,described the diffusetypeofthe disease.Jaffeetal.2proposedthetermpigmented villonodu-larsynovitisforthesemanifestations,butthenomenclature proposedbyGranowitzdefinedthatthetermpigmented vil-lonodularsynovitisshouldbeusedforintra-articularlesions, pigmented villonodular bursitis for lesions located in the bursaeandpigmentedvillonodulartenosynovitisforlesions originatingfromtendinoussheaths.
Thispathologycanbedividedintotwotypes:localizedand diffuse.Themostcommontypeisthediffuseone.Itismore frequentbetween20and50yearsofagebutcanreachanyage, withaslightprevalenceinfemales.Thetreatmentaimsatthe resectionofthelesion,botharthroscopicallyand/orviaopen surgery,withlocalrecurrencebetween10%and56%.3
Fig.1–Clinicalaspect(A),magneticresonanceimaging(B)andradiographs(C),whichdemonstratediffusesynovitis, arthrosis,andbonecysts.
This work describes a case of diffuse villonodular pig-mentedsynovitisaffectingtherightknee,thatwasassociated with advanced gonarthrosis and underwent total replace-ment.
Clinical
case
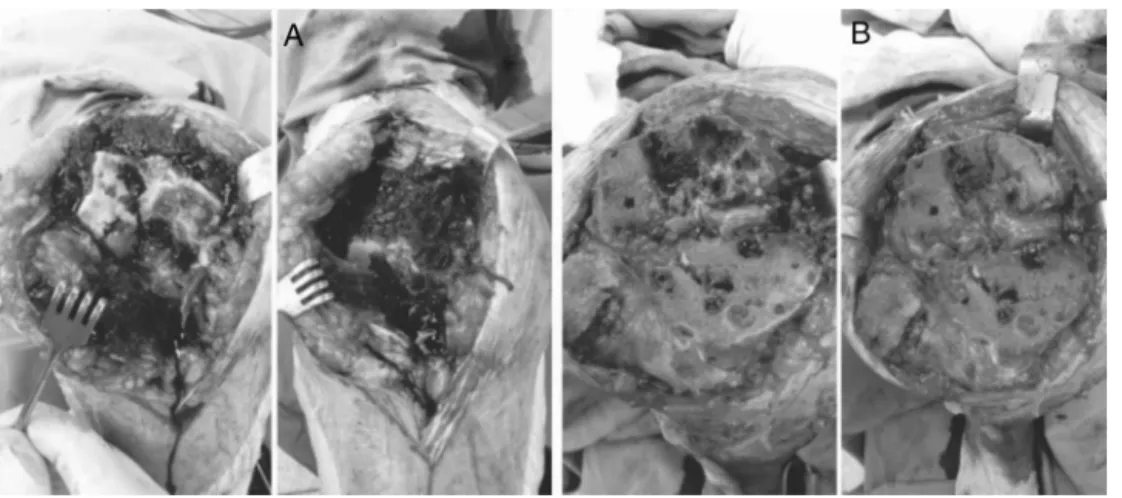
Fig.2–Imageswhichdemonstratepreoperativeaspect–DPVNS,boneflawsandbonesectionsbefore(A)andafter(B) graftingandwidesynovectomy.
110◦.Thekneeradiographshowedadvanced
tricompartmen-talarthrosis,grade4ofKellgrenandLawrence,asignificant lossof joint space and the presenceofvarious epiphyseal bonecystsinthetibiaandfemur.Magneticresonanceimaging demonstratedadvancedtricompartmentalarthrosis,aswell asexuberantdiffusesynovitisthroughoutthejoint, includ-ingpoplitealfossaandextra-articularextensionsintendinous sheaths,inadditiontovariousbonecystsinthefemurand tibia(Fig.1).
The patient underwent total joint replacement of the knee,associatedwithawideperioperativesynovectomy.Bone defects resulting from the cysts, which formed contained defects, were found; bone grafts were put in the defects (Fig.2). Theposteriorcruciateligament wassacrificedwith aposteriorsacrificefemoralcomponent(PS),and,inthiscase, non-replacementof the patella was chosen. We also used intravenous tranexamic acid in anesthetic induction and 15min before releasing the tourniquet due to the risk of increasedbleedingfrom surgery. Thepatientleft the oper-atingroomingoodconditions,andremainedintheICUon thedayofsurgery,beingtransferredtotheroomonthefirst postoperativeday(POD).Shewasdischargedonthesecond POD.
Non-weightbearingwasmaintainedfor30daysduetobone graftingonthemedialfemoralcondyle.Thepatienthadagood postoperativeevolution,despitetheshortfollow-up.Shehas goodlimbalignment,fullextensionand100◦flexion.Shealso
reportsimprovementofpainandregressionofkneeedema (Figs.3and4).
Discussion
Pigmentedvillonodular synovitisisarare disease,with an incidenceof1.8casespermillion,andshouldbesonamed whenfound inintra-articularlocations.This lesioncan be foundinoneineach2500arthroscopies.4Themostcommon locationisintheknee,about80%,followedbytheankle. Intra-articulardiseasemaybelocalizedordiffuse,withthefirsttype beingalmostexclusivelyfoundintheknee.DPVNSis char-acterizedbysynovialortendinoussheathhyperplasia,with
markedproliferationofstromalcells,largeamountsofintra andextracellularhemosiderinandmultinucleatedgiantcells. Thediseaseismoreprevalentinpatientsbetweentheagesof 20and50,butitcanaffectanyage.Thelocalizedtype repre-sents6%ofthetotalofthisdiseaseandhasamildpreference forfemales.5AccordingtoDinesetal.,6Hoffafat, suprapatel-larrecess,intercondyleand posteriorcapsuleare themost commonlocations,thelattertherarer.
DPVNShasunknownetiology,althoughtrauma, inflamma-toryprocesses,neoplasmsandlipidmetabolicdiseaseshave beenimplicatedasthecauseofthedisease.Recent cytoge-neticstudiessuggestevidencemorerelatedtoneoplasia.3,7
In diffusetypes, repetitivejoint effusion, limited range of motion and pain are common symptoms. In the local-izedtypesthemechanicalsymptomsthatsimulatemeniscal lesionsandinstability,palpablemassesandpainarefrequent complaints andoften makediagnosis difficult. Inposterior lesions,painisoftenreportedwithkneeflexion.8Pain and tumorareusuallyprogressive.Thetimefromonsetof symp-tomstodiagnosisisonaverage19monthsinthelocalized typesand15monthsinthediffuseones.Thecorrelationof symptomonsetandtraumaispresentin44–53%ofpatients.5 Complementarytestsaidinthediagnosis,andmagnetic resonanceimagingisthemostsensitive.3,4,7Radiographsare
Fig.4–ClinicalaspectandROMofthepatientwithonemonthaftersurgery.
usuallynormal,butdegenerationofthejointsurfacemaybe presentandismorefrequentinthehipandshoulderjoints. Intheknee,thesechangesarerare,butthenarrowingofjoint spaceandosteophytesarefindingsrelatedtoDPVNS,asfound inthiscase.Recentstudiessuggestthatproteolyticenzymes producedbygiantcellswithinthehyperplasticsynovialtissue couldplay arole inthisjoint degradation.4 Magnetic reso-nanceimagingisanimportanttesttoestablishthediagnosis anddirecttreatment.AreasoflowsignalonT1andT2are observedinthesynovialmembrane,whichisirregular,and theassociationwithjointeffusionisfrequent.7
Thehistologicalfindingsareofawell-differentiatedlesion, withdestructive proliferation ofsynovial-like mononuclear cells,associatedwithmultinucleatedgiantcells, xanthoma-tous macrophages, presence of hemosiderin, lipids and lymphoplasmacytic inflammatorycells.In localizedlesions thereisthepresenceofapseudocapsule.4,7
DPVNS is a progressive benign lesion, and malignancy israre.1 The recommended treatment forDPVNS islesion resection.Itcan bearthroscopicalor open.In diffusetype, arthroscopyhasagoodindicationwiththe useofmultiple portals.Theuseofposteriorarthrotomymaybenecessaryin casesofposteriorfossadisease.Inthelocalizedtype,the par-tialarthroscopicsynovectomyinwhichthelesionisremoved isless invasive,but intumorswell-delimited bya pseudo-capsule,open resectionisa goodoption.6,7 Relapsesrange from10%to56%,andaremorecommonindiffusetypeand maytakeyearstooccur.5Therecurrenceinlocalizeddisease isaround3%.9Radiotherapy isusedincaseswithmultiple recurrences.Malignancyoccursin3%ofcasesandcorrelates withmultiplerecurrencesandradiotherapy.Patientfollow-up isdonewithperiodicmagneticresonanceimagingeverysixto 12months.7
Hamlinetal.10 followed 18patients atMayo Clinicwho were diagnosed with DPVNS, and underwent total knee arthroplasty,14withthediffusetype–activein11andinactive inthree–andfourwiththelocalizedtype.Themean follow-upwas9.9years.Allpatientswiththediffuseactivetypealso underwenttotalsynovectomy.Attheendofthefollow-up,in 14ofthe18patientsthereplacementwasfixedandwitha sat-isfactoryfunction.Thefourfailuresoccurredinpatientswith
thediffuseandactivetypeofthedisease,aspresentedinour case.Three failureswere duetoasepticloosening andone wasduetorelapseofthedisease.Theseauthorsrecommend abroadsynovectomy,associatedwithposteriorcruciate lig-amentreplacementforbettersynovialmembraneexposure, whichwasdoneinthiscase.
Total knee arthroplasty (TKA) in patients with VNS is not a complication-free procedure. In cases of recurrence ofthe disease afterTKA and dependingon functional sta-tus, a newsynovectomymay beattempted. Other options wouldberadiotherapy,arthrodesisorevenamputation.Many patientsalsohavedifficultyingainingrangeofmotion(ROM) intheinitialpostoperativeperiodandtheauthorsrecommend attentiontoavoidstiffness.10
TKA is a viable option for patients with DPVNS when thereisassociatedadvancedsecondaryosteoarthrosis.Itcan providepainrelieveandbetterlimbfunction.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.OdaY,TakahiraT,YokoyamaR,TsuneyoshiM.Diffuse-type giantcelltumor/pigmentedvillonodularsynovitisarisingin thesacrum:malignantform.PatholInt.2007;57(9):627–31.
2.JaffeHL,LichtensteinL,SutroCJ.Pigmentedvillonodular synovitis,bursitisandtenosynovitis.ArchPathol. 1941;31:731–65.
3.KimSJ,ShinSJ,ChoiNH,ChooET.Arthroscopictreatmentfor localizedpigmentedvillonodularsynovitisoftheknee.Clin OrthopRelatRes.2000;(379):224–30.
4.MuscoloDL,MakinoA,Costa-PazM,AyerzaMA.Localized pigmentedvillonodularsynovitisoftheposterior compartmentoftheknee:diagnosiswithmagnetic resonanceimaging.Arthroscopy.1995;11(4):482–5.
5.MurpheyMD,RheeJH,LewisRB,Fanburg-SmithJC,Flemming DJ,WalkerEA.Pigmentedvillonodularsynovitis:
6. DinesJS,DeBerardinoTM,WellsJL,DodsonCC,ShindleM, DiCarloEF,etal.Long-termfollow-upofsurgicallytreated localizedpigmentedvillonodularsynovitisoftheknee. Arthroscopy.2007;23(9):930–7.
7. GodoyFAC,FaustinoCAC,MenesesCS,NishiST,GóesCEG, CantoAL.Sinovitevilonodularpigmentada:relatodecaso. RevBrasOrtop.2011;46(4):468–71.
8. ChaeDJ,ShettyGM,KangKH,KimJH,NhaKW.Localized pigmentedvillonodularsynovitisoftheposteriorcapsuleof theknee.JKneeSurg.2009;22(3):267–9.
9.HernandezAJ,CamanhoGL,LarayaMH,FávaroE,Martinelli FilhoM.Sinovitevilonodularpigmentadalocalizadado joelho:tratamentoporviaartroscópica.ActaOrtopBras. 2005;13(2):76–8.