CHI LDBI RTH CARE: CONTRI BUTI NG TO THE DEBATE ON HUMAN DEVELOPMENT
Crist ina Maria Garcia de Lim a Parada1
Maria Ant oniet a de Barros Leit e Carvalhaes2
Par ada CMGL, Car v alhaes MABL. Childbir t h car e: cont r ibut ing t o t he debat e on hum an dev elopm ent . Rev Lat ino- am Enferm agem 2007 set em bro- out ubro; 15( núm ero especial) : 792- 8.
This study aimed to evaluate care during childbirth and neonatal development in the interior of São Paulo in order to support m anagers responsible for form ulating public policies on hum an developm ent and allocating public resources to the wom en’s healthcare. This epidem iological study focused on the evaluation of health services based on the observation of the assistance delivered by the Single Health System in 12 maternities and 134 delivers. The Brazilian Health Ministry or World Health Organization standards were adopted for com parison. The results revealed problems related to the structure of some maternities, where some well-proven practices in normal childbirth are still little used, whereas other prejudicial or ineffective ones are routinely used. Reversing this picture is essential in order to offer hum anized quality care to wom en with consequent reductions in m aternal and neonatal m ortality rates, in such a way that the region achieves the m illennium goals established for im proving hum an developm ent.
DESCRI PTORS: hum an developm ent ; healt h services evaluat ion; delivery
EVALUACI ÓN DE LA ESTRUCTURA Y DEL PROCESO DE ATENCI ÓN AL PARTO:
CONTRI BUCI ÓN AL DEBATE SOBRE DESARROLLO HUMANO
Con la finalidad de subsidiar a gestores responsables por la atención a la salud de la m ujer en la form ulación de políticas públicas dirigidas al desarrollo hum ano, se propone la presente investigación, cuyo objetivo es evaluar la estructura y proceso de atención al parto y al neonato desarrollada en una región del interior del Estado de São Paulo, Brasil. Se trata de un estudio epidem iológico caracterizado por la evaluación de la calidad de servicios de salud. Los resultados obtenidos fueron com parados con patrones establecidos por el Ministerio de la Salud y la Organización Mundial de Salud. Los resultados apuntan problem as con la estructura de algunas m aternidades y revelan que práct icas dem ost radam ent e út iles en el part o norm al aún son poco ut ilizadas, m ient ras que ot ras perjudiciales o ineficaces son rutinariam ente utilizadas. Modificar esa situación será esencial para ofrecer atención hum anizada y de calidad, con consecuente reducción en las tasas de m ortalidad m aterna y neonatal, de form a que la región alcance las m etas establecidas para la am pliación del desarrollo hum ano en el m ilenio.
DESCRI PTORES: desarrollo hum ano; evaluación de servicios de salud; part o
AVALI AÇÃO DA ESTRUTURA E PROCESSO DA ATENÇÃO AO PARTO: CONTRI BUI ÇÃO AO
DEBATE SOBRE DESENVOLVI MENTO HUMANO
Com a finalidade de subsidiar gestores da área de saúde da m ulher, na form ulação de políticas públicas, volt adas ao desenvolvim ent o hum ano, realizou- se est a invest igação, cuj o obj et ivo foi avaliar a est rut ura e o processo da atenção ao parto e ao neonato desenvolvido em região do interior paulista. Estudo epidem iológico, volt ado para avaliação dos serviços de saúde, baseou- se na observação da assist ência prest ada pelo Sist em a Único de Saúde em 12 m aternidades e 134 partos, adotando-se padrões estabelecidos pelo Ministério da Saúde ou Organização Mundial de Saúde para com paração. Os resultados apontam problem as relacionados à estrutura em algum as m aternidades, m ostrando que práticas úteis ao parto norm al ainda são pouco utilizadas, enquanto que out ras prej udiciais ou ineficazes ainda são ut ilizadas rot ineiram ent e. Revert er esse quadro será essencial para oferecer atendim ento de qualidade às m ulheres, com conseqüente redução nas taxas de m ortalidade m aterna e neonatal, para que a região atinja as m etas estabelecidas para am pliação do desenvolvim ento hum ano no m ilênio.
DESCRI TORES: desenvolvim ent o hum ano; avaliação de serviços de saúde; part o
1 PhD in Nursing, Professor, e- m ail: cparada@fm b.unesp.br; 2 PhD in Public Health, e- m ail: carvalha@fm b.unesp.br. Medical School of Botucatu, Universidade Est adual Paulist a “ Júlio de Mesquit a Filho”, Brazil
I NTRODUCTI ON
I
n r e ce n t d e ca d e s, t h e Un i t e d Na t i o n s Pr ogr am for Dev elopm en t ( UNPD) h as w or k ed n ot only w it h econom ic, but also w it h social indicat or s, especially in the health and educational areas. Am ong t he eight obj ect ives t his Program est ablished for t he m illen n iu m , w it h a v iew t o t h e decr ease of social inequalities on the planet, two are closely related with d eliv er y car e: t o d ecr ease ch ild m or t alit y an d t o im prove m at ernal healt h( 1). Brazil is am ong t he 189count ries t hat com m it t ed t o t hese obj ect ives. Cu r r en t l y, m o st o f ch i l d r en ’s d ea t h s a r e concentrated in the first m onth of life, evidencing the im port ance of fact ors relat ed t o pregnancy, delivery and puerperium . I t is em phasized that, in spite of the cont inuous post - neonat al m ort alit y decrease in Brazil as from t he 1990’s, neonat al m ort alit y has rem ained r elat iv ely st abilit y, r epr esent ing m or e t han 60% of children’s deaths in the country( 2). The sam e situation
is found in DI R XI ( form er Direção Regional de Saúde
[ Regional Healt h Board] of Bot ucat u/ SP) , where t his st udy w as per for m ed. I n 2005, t his sit e show ed a child m ortality coefficient of 12.1 per 1,000 live births, a little below that of the State of São Paulo ( 13.4 per 1,000 live birt hs) , while neonat al m ort alit y and post -neonatal coefficients were 8.3 and 3.8 per 1,000 live birt hs, respect ively( 3).
I n 2004 t he Nat ional Policy Plan for Wom en priorit ized t he prom ot ion of qualified and hum anized obstetric and neonatal care, an indispensable condition for Brazil to be able to reach the goals established by t he Millennium Hum an Developm ent Sum m it , relat ed t o t he decrease of m at ernal and neonat al indicat ors by 75% unt il 2015( 4). The act ions t o be per for m ed
in clu d e t h e ex p an sion of t h e Pr e- Nat al an d Bir t h Hum anization Program , also m aking financial transfers for cit ies t o com plet e t he expansion and qualificat ion pr ot ocols of car e act ions t o t he pr e- nat al, deliv er y and puerperal periods( 5).
For t he follow- up of UNDP goals orient ed t o i m p r o v e m a t e r n a l h e a l t h , t w o i n d i c a t o r s w e r e adopt ed: m at ernal m ort alit y rat e and percent age of d e l i v e r i e s a t t e n d e d b y a q u a l i f i e d h e a l t h c a r e p r o f e ssi o n a l( 1 ). Re a so n s f o r i n cr e a se d m a t e r n a l
m o r t a l i t y i n d i c a t e p o o r s o c i a l a n d e c o n o m i c condit ions, low degree of inform at ion and educat ional b a ck g r o u n d , f a m i l y d y n a m i cs w h e r e v i o l e n ce i s present and, above all, difficult ies of access t o qualit y healt hcar e ser v ices( 4).
Mat ernal m ort alit y is considered avoidable in 9 2 % of cases( 1 ), w h ich r ef lect s ser iou s p r ob lem s
r elat ed t o car e in t he pr egnancy- puer per al cycle, if any. I n the last official estim ate, regarding 2002, the Brazilian m aternal m ortality ratio corresponded to 74.8 deaths per 100,000 live births, m uch higher than the indicat or considered accept able by t he World Healt h Or g an izat ion ( WHO) : 2 0 d eat h s p er 1 0 0 , 0 0 0 liv e birt hs( 4).
However, as this is a rare event, the analysis of m at er n al m or t alit y r at es m u st con sider, t o t h e ex t ent possible, lar ge populat ions and t r ends ov er r e l a t i v e l y l o n g p e r i o d s, a v o i d i n g t h e si m p l e com parison of different rat es in sm all populat ions or fr om one year t o t he ot her. Consider ing t he per iod from 2001 to 2005, this indicator rem ained relatively st able in t he St at e of São Paulo, r anging bet w een 30.3 and 35.7 per 100,000 live births, a status different from t he region governed by Bot ucat u where, in t he sam e period, t he rat es range from zero t o 98.5 per 100,000 live birt hs( 6).
Maternal and neonatal deaths m ust be treated as a result of t he sam e precarious condit ion in pre-nat al, deliv er y and post - pre-nat al car e. Ther efor e, it is beyond doubt that the quality of wom en’s care in this phase of life also const it ut es an indicat or of hum an developm ent . To evaluat e ser v ice deliver y, in or der to identify its fragilities and strengths, prom oting care r e o r g a n i za t i o n w h e n e v e r r e q u i r e d , i s a w a y t o part icipat e in t he effort t o decrease t he inequalit ies expressed by t he UNDP.
This art icle shows and discusses, under t he UNDP focus, t he result s relat ed t o t he delivery care ev alu at ion ob t ain ed t h r ou g h a b r oad p r oj ect t h at ev al u at ed t h e Pr e- Nat al an d Bi r t h Hu m an i zat i o n Program ( PNHP) at t he DI R XI( 7) of t he St at e of São
Pau lo.
MATERI AL AND METHODS
Fr om a t ot al of 31 r egional cit ies, 20 w er e included in the study, with the city’s adherence to the PNHP unt il 2003 as t he only inclusion cr it er ion. All cit ies had basic healt hcar e unit s for pr e- nat al car e and 11 had m at er nit ies for low r isk deliv er y car e, how ev er, w it h a var iable num ber of beds: t hr ee in t h e h ospit als w it h t h e low est m on t h ly av er age of deliveries and 29 in the one with the highest average. Th er e w as on e sin g le ser v ice f or t er t iar y car e in obst et r ics.
The structure indicators used were: for hum an resources, t he presence of physicians and nurses in all shift s; for physical resources, t he possibilit y of a com panion in the pre-delivery period, the existence of PDP (pre-partum , delivery and puerperium ) room s and the adequacy of C-section and natural delivery room s, of the joint room and nursery to receive the parents; for the m aterial and equipm ent resources, the presence of com pr essed air, ox y gen, sur gical lam p, deliv er y t able, em ergency and anest hesia cart , st et hoscope, sphygm om anom et er, Pinard’s st et hoscope or Doppler sonar and heated cradle in the natural delivery and C-section room s and, in the joint room and nursery, the num ber of cradles and clot hes for m ot her and baby, and t he exist ence of a rest room before t he ent ry of the nursery; for rules and procedures, the availability of a j oint room , writ t en rules/ procedures, syst em at ic orientation activities to the m other, the use of nursing bot t les, feedin g bot t les an d ar t ificial m ilk an d t h e perm ission for the m other to rem ain in the nursery if the child’s hospitalization is required.
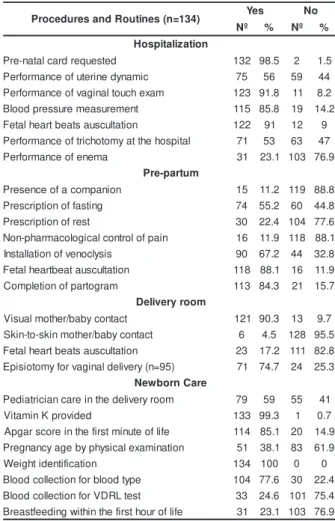
Th e p r o ce ss i n d i ca t o r s i n cl u d e d : a t hospit alizat ion, t he r equest for t he pr e- nat al car d, per for m ance of ut er ine dy nam ic and v aginal t ouch e x a m i n a t i o n , b l o o d p r e ssu r e m e a su r e m e n t , auscult at ion of fet al heart beat s and perform ance of t r i ch o t o m y a n d e n e m a ; i n t h e p r e - p a r t u m , t h e presence of a com panion, pr escr ipt ion of fast ing or rest , non- pharm acological cont rol of pain, inst allat ion of v enocly sis, auscult at ion of fet al hear t beat s and com pletion of partogram ; in the delivery room , visual and skin- t o- skin cont act of m ot her/ baby, auscult at ion of fet al heart beat s and perform ance of episiot om y in v agin al deliv er y ; for t h e n ew bor n car e, car e by a pediatrician at the delivery room , provision of vitam in K, establishm ent of Apgar score in the first m inute of life, pregnancy age by physical exam inat ion, weight identification, blood collection for blood type and VDRL ( Ven er eal Diseases Resear ch Labor at or y ) t est an d breast feeding in t he first hour of life.
Dat a Collect ion
Three instrum ents with closed questions were elaborat ed: t he first one, for t he int erview wit h t he m anager, considered as t he inform er who was m ost knowledgeable about the service structure; the second and the third, for follow- up of delivery care processes, consisted of a check- list type program to be com pleted b y t h e o b ser v er s, a l so i n cl u d i n g a sp ect s o f t h e m at er n it y st r u ct u r e, h ow ev er, accor d in g t o t h eir perspective. All derived from a broad instrum ent used i n a st u d y d ev el o p ed i n Ma r a n h ã o( 9 ), a n d sm a l l
changes were m ade t o adapt t o t he local realit y. Data were collected in 2004 and 2005, in two stages. I n the first stage, all m aternity m anagers were int er v iew ed ( n= 12) , usually t he clinical dir ect or. I n t he second, all deliv er ies m ade t hr ough t he Single Healt h Syst em for seven consecut ive days, 24 hours a d ay, w er e ob ser v ed in all r eg ion al m at er n it ies ( n = 1 3 4 ) ; t h i s o b se r v a t i o n w a s p e r f o r m e d b y h e a l t h ca r e p r o f e ssi o n a l s o r p r e v i o u sl y q u a l i f i e d st u den t s. Th e coor din at ion an d su per v ision of t h e obser v at ion w as per for m ed by one of t he aut hor s, upon m eetings with the observers held before, during and aft er dat a collect ion.
Dat a Analy sis
As already shown, when evaluating the PNHP st ruct ure and process, t he result s obt ained wit h t he st andards est ablished by t he Minist ry of Healt h( 10- 11)
or WHO( 2) were com pared, the practices known to be
Et hical Pr ocedur es
This research project was analyzed and approved by the Ethics Committee at Botucatu School of Medicine of the Universidade Estadual Paulista and complied with all rules established for research involving human beings.
RESULTS
I nform ation on the structure for delivery and newborn care are shown in table 1. Very low rates were found for all item s related to hum an resources. None of t he m at ernit ies had PDP room s, in m ore t han half of t hem t he phy sical space allow ed t he pr esence of a com panion in the pre- partum , and one delivery room was showed as inappropriate, due to its sm all size. The physical area of t he j oined room was appropriat e in two thirds of the institutions and in a little m ore than half the institutions the nursery was adequate to receive the parents. The use of nursing bottles and feeding bottles w as v er y high and t he dev elopm ent of sy st em at ic educational activity, infrequent (table 1).
Table 1 - Resources, rules and procedures available in t he DI R XI m at ernit ies, 2004/ 2005
Dat a about t he deliv er y and new bor n car e process are showed in t able 2.
Table 2 - Pr ocedu r es per f or m ed w it h t h e pr egn an t patient at the hospitalization, pre- partum , and delivery room , and newborn care in DI R XI m aternities, 2004/ 2005 ) 4 3 1 = n ( s e n i t u o R d n a s e r u d e c o r
P Yes No
º
N % Nº %
n o i t a z il a t i p s o H d e t s e u q e r d r a c l a t a n -e r
P 132 98.5 2 1.5
c i m a n y d e n ir e t u f o e c n a m r o f r e
P 75 56 59 44
m a x e h c u o t l a n i g a v f o e c n a m r o f r e
P 123 91.8 11 8.2
t n e m e r u s a e m e r u s s e r p d o o l
B 115 85.8 19 14.2
n o it a tl u c s u a s t a e b t r a e h l a t e
F 122 91 12 9
l a ti p s o h e h t t a y m o t o h c ir t f o e c n a m r o f r e
P 71 53 63 47
a m e n e f o e c n a m r o f r e
P 31 23.1 103 76.9
m u t r a p -e r P n o i n a p m o c a f o e c n e s e r
P 15 11.2 119 88.8
g n it s a f f o n o it p ir c s e r
P 74 55.2 60 44.8
t s e r f o n o it p ir c s e r
P 30 22.4 104 77.6
n i a p f o l o r t n o c l a c i g o l o c a m r a h p -n o
N 16 11.9 118 88.1
s i s y l c o n e v f o n o it a ll a t s n
I 90 67.2 44 32.8
n o it a tl u c s u a t a e b t r a e h l a t e
F 118 88.1 16 11.9
m a r g o t r a p f o n o it e l p m o
C 113 84.3 21 15.7
m o o r y r e v il e D t c a t n o c y b a b / r e h t o m l a u s i
V 121 90.3 13 9.7
t c a t n o c y b a b / r e h t o m n i k s -o t -n i k
S 6 4.5 128 95.5
n o it a tl u c s u a s t a e b t r a e h l a t e
F 23 17.2 111 82.8
) 5 9 = n ( y r e v il e d l a n i g a v r o f y m o t o i s i p
E 71 74.7 24 25.3
e r a C n r o b w e N m o o r y r e v il e d e h t n i e r a c n a i c ir t a i d e
P 79 59 55 41
d e d i v o r p K n i m a ti
V 133 99.3 1 0.7
e fi l f o e t u n i m t s r if e h t n i e r o c s r a g p
A 114 85.1 20 14.9
n o it a n i m a x e l a c i s y h p y b e g a y c n a n g e r
P 51 38.1 83 61.9
n o it a c if it n e d i t h g i e
W 134 100 0 0
e p y t d o o l b r o f n o it c e ll o c d o o l
B 104 77.6 30 22.4
t s e t L R D V r o f n o it c e ll o c d o o l
B 33 24.6 101 75.4
e fi l f o r u o h t s r if e h t n i h ti w g n i d e e ft s a e r
B 31 23.1 103 76.9
) 2 1 = n ( s e r u d e c o r P d n a s e l u R , s e c r u o s e
R Yes No
º
N % Nº %
) y a d / s r u o h 4 2 ( s e c r u o s e R n a m u H n a i c ir t e t s b
O 2 16.7 10 83.3
m o o R y r e v il e D n i e s r u n c ir t e t s b
O 0 0 12 100
n a i c ir t a i d e
P 1 8.3 11 91.7
t s i g o l o i s e h t s e n
A 1 8.3 11 91.7
m u ir e p r e u p t a e s r u
N 0 0 12 100
a e r a l a t a n o e n n i e s r u
N 1 8.3 11 91.7
s e c r u o s e r l a c i s y h P m u t r a p -e r p e h t n i n o i n a p m o c f o y ti li b i s s o
P 7 58.3 5 41.7
, m u t r a p -e r p ( s m o o r P D P f o e c n e t s i x E ) m u ir e p r e u p d n a y r e v il e
d 0 0 12 100
s m o o r y r e v il e d l a r u t a n d n a n o it c e s -C f o y c a u q e d
A 11 91.7 1 8.3
m o o r t n i o j f o y c a u q e d
A 9 75 3 25
s t n e it a p e h t e v i e c e r o t y r e s r u n f o y c a u q e d
A 7 58.3 5 41.7
s e c r u o s e R t n e m p i u q E d n a l a i r e t a M l a r u t a n d n a n o it c e s -C e h t n i t n e m p i u q E s m o o r y r e v il e
d 10 83.3 2 16.7
e h t n i r e t e m o n a m o m g y h p s / e p o c s o h t e t S m o o r y r e v il e
d 7 58.3 5 41.7
m o o r y r e v il e d e h t n i r a n o s r e l p p o D / d r a n i
P 1 8.3 11 91.7
m o o r y r e v il e d e h t n i e l d a r c d e t a e
H 4 33.3 8 66.7
m o o r t n i o j e h t n i s e l d a r c f o r e b m u n e h t n i y c a u q e d
A 10 83.3 2 16.7
e h t n i y b a b e h t d n a r e h t o m e h t r o f s e h t o l C y r e s r u n / m o o r t n i o
j 11 91.7 1 8.3
y r e s r u n e h t f o e c n a r t n e e h t t a m o o r t s e
R 7 58.3 5 41.7
y r e s r u n e h t n i s e l d a r c f o r e b m u n e h t n i y c a u q e d
A 10 83.3 2 16.7
s e r u d e c o r P d n a s e l u R m o o r t n i o j f o y ti li b a li a v
A 11 91.7 1 8.3
s e r u d e c o r p / s e l u r n e tt ir w f o e c n e t s i x
E 6 50 6 50
n o it a t n e ir o ' s r e h t o m f o s e it i v it c a c it a m e t s y
S 2 16.7 10 83.3
d e s u y l e n it u o r s e lt t o b g n i d e e f d n a g n i s r u
N 7 58.3 5 41.7
d e s u y l e n it u o r k li m l a i c if it r
A 1 8.3 11 91.7
y r e s r u n e h t r e t n e o t r e h t o m e h t r o f n o i s s i m r e
P 9 75 3 25
perform ance of t richot om y and regular perform ance of en em a w er e con sider ed u n sat isf act or y ; in pr e-partum , the prescription of fasting and the installation o f v e n o cl y si s w e r e u n sa t i sf a ct o r y, w h i l e t h e prescript ion of rest was usual. I n t he delivery room , t he per for m ance of episiot om y in vaginal deliver ies was unsat isfact ory ( t able 2) .
DI SCUSSI ON
This study shows an im portant characteristic: m ost of t he indicat ors used were m easured by direct observation of the m aternity structure and the delivery car e pr ocess. Ther efor e, it m ay be consider ed t hat t he result s show good reliabilit y, if com pared t o t he Brazilian st udies wit h sim ilar obj ect ives perform ed t o date, as they always collect data by checking patient f i l e s a n d i n t e r v i e w i n g p r e g n a n t p a t i e n t s a n d pr ofessionals.
According t o t he PNHP, all unit s int egrat ing t he SUS have t he responsibilit y t o have appropriat e hum an resources for delivery care( 11) and, in line with
W HO, t h e m i d w i f e- n u r se seem s t o b e t h e m o st a p p r o p r i a t e p r o f e ssi o n a l , w i t h b e t t e r co st -e f f -e ct i v -e n -e ss, t o b -e r -e sp o n si b l -e f o r ca r -e i n pregnancies and nat ural deliveries( 12). I n spit e of t he
abov e, none of t he hospit als in t his st udy hav e an act ing m idwife- nurse in t he Delivery Room t o at t end nat ural deliveries 24 hours a day. Only one hospit al has this expert to perform the delivery but, only during day shift s and in t he absence of a physician. Even a general nurse is not present very m uch: no hospit al had a nur se w or k ing ex clusiv ely in obst et r ics, and only one of t he hospit als had t his professional act ing specifically in neonat ology area in all shift s. I n m ost of t he cases, t he division of t he few nurses hired t o assist the whole hospital, and the presence of a single nurse per shift were com m on.
Regarding m edical work, the m ost frequently observed sit uat ion in t his st udy is t hat of t he on- call obst et rician, which is not rare in Brazil. According t o a st udy published in 2002, alm ost one t hir d of t he deliveries occurred in institutions with no obstetrician, not even on- call, and 74% did not have a pediatrician p r esen t( 1 3 ). Th is is an u n accep t ab le sit u at ion , as
legislation establishes that all units integrating the SUS m ust guarant ee t he presence of a pediat rician in t he delivery room( 11). Com paring the situation seen in the
DI R XI region wit h Brazilian dat a, a m ore favorable
condit ion was found, as t he pediat rician was present in 59% of t he deliveries.
St ill, t he need for effect ive m ult iprofessional action, reconsideration of on- calls, especially in larger m at ernit ies, and t he pert inence of t he developm ent o f p e r m a n e n t e d u ca t i o n a l a ct i v i t i e s m u st b e considered, so t hat a higher num ber of deliveries is assist ed by qualified professionals. This is a wom en’s right and a country’s obligation to im prove its hum an dev elopm ent indicat or s.
The situation in the physical space where the pre- part um occurs is inappropriat e in about 40% of the m aternities, as it is incom patible with the presence of a com panion. I n general, the physical areas of the m at ernit ies and nurseries were not built t o allow for ca r e h u m a n i za t i o n . I n a d d i t i o n , i n o n e o f t h e m aternities, there was no j oint room , essential to help in t he elabor at ion of t he m ot her - child r elat ion and m andat ory in SUS unit s since 1993( 14).
Most of t he hospit als st udied had deliv er y room s equipped with com pressed air, oxygen, surgical lam p, delivery t able, em ergency and anest hesia cart . How ev er, t he pr esence of basic inst r um ent s lik e a st e t h o sco p e / sp h y g m o m a n o m e t e r a n d Pi n a r d ’ s st et hoscope or Doppler sonar was not frequent . This form of organizat ion in m at ernit ies is relat ed t o t he m edicalizat ion of deliveries. This sit uat ion has been not iceable in Brazil since t he second half of t he 20t h cent ury. I n recent years, it has been reviewed since, in a low risk situation, there m ust be little intervention, wit h m easures t aken in consist ency wit h safet y( 12).
Fo r t h e o v e r a l l e v a l u a t i o n o f t h e c a r e pr ocess fr om hospit alizat ion t o deliver y, am ong t he p r a c t i c e s u s e f u l f o r n a t u r a l d e l i v e r y, o n l y t h e f ollow in g in d icat or s w er e sat isf act or y : r eq u est of pre- nat al card, perform ance of vaginal t ouch exam , com p let ion of p ar t og r am an d m ot h er / b ab y v isu al cont act . Alt hough posit ive for t he qualit y of care( 10-11), t he good per for m ance of t hese indicat or s does
The failur e t o m easur e t he m ot her ’s blood pressure and auscult at e t he fet al heart beat indicat es a m aj or technical failure in the care process, contrary t o t he purpose of decreasing m at ernal and neonat al m ort alit y. A sudden increase in blood pressure m ay indicate the need to hurry the delivery or transfer the patient to a m ore com plex care level, while heartbeat auscult at ion is essent ial for t he ev aluat ion of fet al vit alit y, wit h subsequent conduct s( 12).
A num ber of procedures allowing for a better p r o g n o si s o f n e w b o r n s sh o w e d u n sa t i sf a ct o r y perform ance, particularly the breastfeeding rate within the first hour of life, which scored only 23.1% , below t he 40% r ecent ly obt ained in a public m at er nit y in Rio de Janeiro( 16). I t m ust be rem em bered that favoring
br east feeding is also one of t he UNPD goals and a priorit y in t he Brazilian healt h policy.
Sin ce t h e 1 9 5 0 ’s, it h as been sh ow n t h at h u m a n d ev el o p m en t i n d i ca t o r s m u st i n cl u d e, i n addition to the econom ic dim ension, other dim ensions r elat ed t o people’s social life and qualit y of life. I n this effort, in the State of São Paulo, since 2000, such indicat or s hav e been consider ing t he per inat al and ch ild m or t alit y r at e, sig n alin g t h e im p or t an ce of m other- child care, as both rates keep a close relation t o t he qualit y of pre- nat al care and delivery( 17).
Considering the unfavorable results especially related to the quality indicators of the wom en’s health care process during labor and delivery and newborn car e, t ak ing t he PNHP as a r efer ence, it should be questioned if im proving m aternal and child health has been a priority of the local people in charge - m anagers, professionals, society - through the im plem entation of healt h and hum an developm ent policies.
CONCLUSI ONS
Practices markedly favorable to health, useful in natural delivery and advised by the PNHP, such as the presence of a com panion, non-pharm acological control of pain, skin-to-skin mother/ baby contact, and the early start of breastfeeding, among others, are still little practiced in the maternities studied, while other clearly harmful or in ef f ect iv e pr act ices, su ch as f ast in g, v en ocly sis, trichotomy and episiotomy, are still frequently used.
Revert ing t his condit ion w ill be essent ial t o deliver hum anized and quality care to wom en, with a su b se q u e n t d e cr e a se o f m a t e r n a l a n d n e o n a t a l m or t alit y r at es, goals of t h e h u m an dev elopm en t pr oj ect in t he new m illennium Br azilian healt hcar e services are com m it t ed t o.
REFERENCES
1. Wat kins K, Carvaj al L, Coppard D, Fuent es R, Ghosh A, Giam berardini C, et al. Relat ório do Desenvolvim ent o Hum ano 2 0 0 6 . Ne w Yo r k : Pr o g r a m a d a s Na çõ e s Un i d a s p a r a o Desen v olv im en t o; 2 0 0 6 .
2. Fundo das Nações Unidas par a a I nfância. Sit uação da cr ian ça b r asileir a 2 0 0 6 . O d ir eit o à sob r ev iv ên cia e ao desenvolvim ent o: crianças de at é 6 anos. Brasília: UNI CEF; 2 0 0 5 .
3. Fundação Sist em a Est adual de Análise de Dados [ Página na I nt ernet ] . Taxa de m ort alidade infant il por idade, segundo Dir eções Regionais de Saúde e m unicípios paulist as, 2005 [ Ace sso e m 0 6 a g o 2 0 0 7 ] . D i sp o n ív e l e m : h t t p : / / www.seade.gov.br/ produt os/ m ort inf/
4. Minist ério da Saúde ( BR) . Secret aria de At enção à Saúde. D ep a r t a m en t o d e Açõ es Pr o g r a m á t i ca s e Est r a t ég i ca s. Polít ica Nacional de At enção I nt egr al à Saúde da Mulher : pr in cípios e dir et r izes. Br asília( DF) : Min ist ér io da Saú de; 2 0 0 4 .
5. Fundação Sist em a Est adual de Análise de Dados [ Página n a I n t e r n e t ] . I n f o r m a çõ e s d o s Mu n i cíp i o s Pa u l i st a s. Mor t alidade m at er na no Est ado de São Paulo e r egião de governo de Botucatu no período de 2001 a 2005 [ Acesso em 0 8 ag o 2 0 0 7 ] . Disp on ív el em : h t t p : / / w w w. sead e. g ov. b r / pr odut os/ im p/ index.php
6 . Pr esidên cia da Repú blica ( BR) . Secr et ar ia Especial de Polít icas par a as Mulher es. Plano Nacional de Polít ica par a Mulheres. Brasília ( DF) : Presidência da República; 2004. 7. Parada CMGL. Avaliação do Program a de Hum anização do Pré- Nat al e Nascim ent o ( PHPN) na DI R XI - Bot ucat u. [ livre-docência] . Ribeir ão Pr et o ( SP) : Escola de Enfer m agem de Ribeir ão Pr et o/ USP; 2 00 6 .
8 . Don ab ed ian A. Th e q u alit y of car e - h ow com e it b e a sse sse d ? Jo u r n a l o f t h e Am e r i ca n Me d Asso c 1 9 8 8 ; 2 6 0 ( 1 2 ) : 1 7 4 3 - 8 .
9 . Alv es MTSSB, Silv a AAM. Av aliação d e q u alid ad e d e m at ernidades: assist ência à m ulher e ao seu recém - nascido no Sist em a Único de Saúde. São Luis ( MA) : UNI CEF; 2000. 1 0 . Min ist ér io da Saú de ( BR) . Secr et ar ia de Polít icas de Saúde. Part o, abort o e puerpério: assist ência hum anizada à m ulher. Brasília: Minist ério da Saúde; 2003.
11. Minist ério da Saúde ( BR) . Port aria nº 569 de 01 de j unho de 2000. I nst it uição do Program a de Hum anização do Pré-nat al e Nascim ent o no âm bit o do Sist em a Único de Saúde. Diário Oficial da República Federat iva do Brasil, Brasília 2000 j unho 8.
1 2 . Or gan ização Mu n dial de Saú de. Mat er n idade Segu r a. Assist ência ao part o norm al: um guia prát ico. Genebra: OMS; 1 9 9 6 . Pu b licação OMS/ SRF/ MSM/ 9 6 . 2 4 .
14. Minist ério da Saúde [ Página na I nt ernet ] . Norm as básicas para im plant ação do sist em a Aloj am ent o Conj unt o. Port aria MS/ GM. Nº 1 0 1 6 d e 2 6 d e a g o st o d e 1 9 9 3 . Br a síl i a : Mi n i st é r i o d a Sa ú d e ; 2 0 0 6 [ Ace sso e m 0 1 a b r 2 0 0 6 ] . Di sp o n ív el em : h t t p / / w w w . al ei t am en t o . o r g . b r / ar q u i v o s/ aloj a1.ht m
1 5 . Bezer r a MGA, Car doso MVLML. Fat or es cu lt u r ais qu e int erferem nas experiências das m ulheres durant e o t rabalho d e p a r t o e p a r t o . Re v La t i n o - a m En f e r m a g e m 2 0 0 6 ; 1 4 ( 3 ) : 4 1 4 - 2 1 .
16. D’Orsi E, Chor D, Giffin K, Ângulo-Test a A, Barbosa GP, Ga m a AS, e t a l . Qu a l i d a d e d a a t e n çã o a o p a r t o e m m at er nidades do Rio de Janeir o. Rev Saúde Pública 2005; 3 9 ( 4 ) : 6 4 6 - 5 4 .
17. Tor r es HG, Fer r eir a MP, Dini NP. I ndicador es sociais -porque const ruir novos indicadores com o o I PRS. São Paulo Per sp ec 2 0 0 3 ; 1 7 ( 3 - 4 ) : 8 0 - 9 0 .