1 St udy ext r act fr om Mast er Thesis; 2 Mast er st udent , CNPq scholar ship holder - Brazil; 3 PhD in Public Healt h, Pr ofessor. São Car los Federal Univer sit y, Brazil
D isponible e n ca st e lla no/ D isponíve l e m língua por t ugue sa SciELO Br a sil w w w .scie lo.br / r la e
I NSTRUCTI ON, SOCI AL ECONOMI C STATUS AND EVALUATI ON OF SOME DI MENSI ONS OF
OCTOGENARI ANS’ QUALI TY OF LI FE
1Keik a I n ou y e2
Eliset e Silv a Pedr azzani3
I nouye K, Pedrazzani ES. I nst r uct ion, social econom ic st at us and evaluat ion of som e dim ensions of oct ogenar ians’
qualit y of life. Rev Lat ino- am Enfer m agem 2 0 0 7 set em br o- out ubr o; 1 5 ( núm er o especial) : 7 4 2 - 7 .
Obj ect iv es: To descr ibe t h e pr of ile of a sam ple of oct ogen ar ian s ( n = 8 0 ) at t en ded at t h e m u n icipal
healt h net w or k of a cit y in t he int er ior of São Paulo, Br azil; ev aluat e t heir per cept ion r egar ding qualit y of life
d im en sion s ( QoL) ; id en t if y cor r elat ion s b et w een socio econ om ic st at u s, ed u cat ion lev el an d QoL. I t is an
ex plor at or y descr ipt iv e st udy w it h a quant it at iv e analy sis of dat a. The r esult s r ev ealed t hat t his populat ion is
p r e d o m i n a n t l y f e m a l e , w i d o w e d , i l l i t e r a t e , se d e n t a r y a n d p o o r , w h o n e e d h e a l t h se r v i ce s a n d l e i su r e
op p or t u n it ies, an d w h ose m ain su p p or t is r elig ion . Th e socio econ om ic st at u s d id n ot in t er f er e in t h e QoL
per cept ion, t hough, higher educat ion and par t icipat ion in phy sical act iv it ies r esult in higher sat isfact ion.
DESCRI PTORS: aged; aging; healt h of t he elder ly ; qualit y of life; pov er t y
N Í VEL DE I N STRUCCI ÓN , SOCI OECON ÓMI CO Y EVALUACI ÓN DE ALGUN AS
DI MENSI ONES DE LA CALI DAD DE VI DA DE OCTOGENARI OS
Obj et ivos: descr ibir el per fil de una m uest r a de oct ogenar ios ( n= 80) at endidos en la r ed m unicipal de
salud de una ciudad del int er ior del Est ado de São Paulo, Br asil; ev aluar su per cepción sobr e las dim ensiones
de la calidad de vida ( CV) ; e ident ificar cor r elaciones ent r e el st at us socioeconóm ico, nivel de inst r ucción y CV.
Se t r at a de un est udio explor at or io descr ipt ivo de apr oxim ación cualit at iva de los dat os. Los r esult ados r evelar on
q u e est a p ob lación es p r ed om in an t em en t e f em en in a, v iu d a, an alf ab et a, sed en t ar ia y p ob r e, q u e le f alt an
ser vicios de salud y opor t unidades de ocio, adm it iendo la r eligión com o el m ayor apoyo. El st at us socioeconóm ico
n o in t er f ir ió en la p er cep ción d e la CV. Sin em b ar g o, ob ser v am os t en d en cia d e q u e m ay or es n iv eles d e
inst r ucción y par t icipación en act iv idades físicas r esult an en m ay or sat isfacción.
DESCRI PTORES: anciano; env ej ecim ient o; salud del anciano; calidad de v ida; pobr eza
N Í VEL DE I N STRUÇÃO, STATUS SOCI OECON ÔMI CO E AVALI AÇÃO DE ALGUMAS
DI MENSÕES DA QUALI DADE DE VI DA DE OCTOGENÁRI OS
Os obj et ivos dest e t r abalho for am : descr ever o per fil de um a am ost r a de oct ogenár ios ( n= 80) , at endidos
n a r ede m u n icipal de saú de de u m a cidade do in t er ior do Est ado de São Pau lo, Br asil; av aliar a per cepção
desses acer ca das dim ensões da qualidade de vida ( QV) e ident ificar cor r elações ent r e o st at us socioeconôm ico,
nív el de inst r ução e QV. Tr at a- se de est udo ex plor at ór io descr it iv o, de abor dagem qualit at iv a dos dados. Os
r esu lt ad os r ev elar am q u e essa p op u lação é p r ed om in an t em en t e f em in in a, v iú v a, an alf ab et a, sed en t ár ia e
pobr e que car ece de ser v iços de saúde e opor t unidades de lazer , adm it indo a r eligião com o o m aior apoio. O
st at u s socioecon ôm ico n ão in t er f er iu n a p er cep ção d a QV, con t u d o, ob ser v a- se q u e h á t en d ên cia d e q u e
m aior es nív eis de inst r ução e par t icipação em at iv idades físicas r esult em em m aior sat isfação.
I NTRODUCTI ON
T
h e Wor ld Healt h Or gan izat ion est im at es a 2 2 3 % i n cr e a se , b e t w e e n 1 9 7 0 a n d 2 0 2 5 , i n t h enum ber of people aged six t y or m or e( 1). Consider ing
t h at old er p eop le d o n ot com p r ise a h om og en eou s
g r o u p , t h e d i v e r si t y a m o n g i n d i v i d u a l s t e n d s t o
incr ease. Fr om t his per spect ive, t he concer n w it h t he
developm ent of act ions t hat shar e values, despit e t he
differences, involves an inclusive, flexible and dynam ic
significat ion t hat values people( 2). This process should
suppor t t he opt im izat ion of know ledge and t alent s t hat
e n co u r a g e u n d e r - sk i l l e d p e o p l e , sa t i sf y i n g t h e i r
i n d i v i d u a l n eed s, so t h a t t h ey a l l f eel w el co m ed ,
u n d er st ood an d r esp ect ed r eg ar d in g t h eir d if f er en t
for m s of being, lear ning and liv ing( 3,4).
We ar e cur r ent ly under going a dem ogr aphic
revolut ion, in which adult s aged over 80 com prise t he
group with the (proportionally) highest growth in the world.
Today, the total num ber of octogenarians is approxim ately
sixt y- nine m illion; t hat is, 1% of t he planet populat ion,
and 3% of dev eloped count r ies’ populat ion( 1). I n t his
cont ext , governm ent s, int ernat ional organizat ions and
civ il societ y ar e called upon t o pr om ot e healt h in it s
b r o a d e st p e r sp e ct i v e , su r p a ssi n g t h e si m p l i st i c
r e m e d i a t i o n v i e w , a n d a ssu r e a cce ss t o m e d i ca l
appointm ents, hospitalizations and m edications(5). Healthy
aging should hav e a br oader char act er. I t should be
recognized t hat healt h care and physical int egralit y are
as im portant as an active participation in social, econom ic,
cultural, spiritual and civil relationships that aim at elders’
autonom y and independence. These activities should take
place through a continuous process of education, growth,
updat ing and per sonal fulfillm ent ; and should include
elders as effective m em bers in the construction of society.
Br oad, w ell fou n ded k n ow ledge abou t agin g
sh o u l d b e i n co r p o r a t e d i n cu r r i cu l a a n d t r a i n i n g
p r og r am s, so t h at st u d en t s an d w or k er s f r om t h e
s o c i a l , h e a l t h , r e c r e a t i o n , u r b a n p l a n n i n g a n d
archit ect ure areas w ork in collaborat ion and have t he
condit ions needed t o per for m funct ions in agr eem ent
w it h t he new dem ogr aphic dem ands( 1).
I n t h i s p e r s p e c t i v e , p u b l i c p o l i c i e s a r e
ch allen ged t o open n ew h or izon s t o t h e elder ly age
gr oup, w hich is ex pect ed t o r each 1. 2 billion people
in 2025( 1). There is an ur gent need for cir cum st ances
f av or ab le t o in cr easin g sit u at ion s of sh ar in g , liv in g
t o g e t h e r, a s w e l l a s t h e p o s s i b i l i t i e s o f c h o i c e .
I n d i s p e n s a b l e a d j u s t m e n t s t o a c c e s s i b i l i t y a r e
m a n d a t o r y a s w e l l . Th e i n t e g r a t i o n b e t w e e n
pr eser v at ion and im pr ov em ent in ev er y com m unit y ’s
w e l l b e i n g s h o u l d b e t h e f o c u s o f r e f l e c t i o n s ,
qu est ion in gs, discu ssion s an d act ion plan s in ev er y
dim ension, so t hat aging can be a posit ive exper ience
f o l l o w e d b y i n f i n i t e p o s s i b i l i t i e s , r e s o u r c e s a n d
o p p o r t u n i t i e s . O t h e r w i s e , w e r e a c h a m e r e l y
quant it at iv e adv ant age, adding y ear s t o liv es w it hout
a qualit at ive concern t o also add “ life” t o t he years( 6).
Qualit y of life depends on several det erm ining
fact ors t hat derive from a hist ory of int erpersonal and
environm ent al int eract ions in a cont inuous int erplay of
past an d pr esen t ex t er n al an d in t er n al in flu en ces( 7 ).
Br on f en b r en n er ’s b iolog ic ap p r oach ap p oin t s t h at a
developing person’s characteristics are strongly entwined
w i t h t h e so ci a l t i ssu e. Acco r d i n g t o t h i s sy st em i c
concept ion, t he pr oposals w ill only m ake sense if t he
exchange processes that take place in as well as am ong
t he syst em s com prised by individuals, t heir caregivers,
fam ilies and other contexts are taken into consideration(8).
Differ ent fr om w hat happens in int er nat ional
l i t e r a t u r e , t h e r e a r e s t i l l f e w s t u d i e s i n o u r
env ir onm ent t hat specifically addr ess elder ly ’s qualit y
o f l i f e . Th e l a c k o f i n f o r m a t i o n r e g a r d i n g t h e i r
per cept ion s, obj ect iv es, ex pect at ion s, con cer n s an d
m ain dif f icu lt ies n eed f u r t h er in v est igat ion so as t o
bet t er under st and t he t r acks w e m ust follow in t er m s
of public policies and im plem ent ing services t hat m eet
t he t r ue needs and ex pect at ions of old age( 9).
Therefore, we elected people aged 80 or m ore
as the target population of our study, which aim ed to: (a)
descr ibe t heir socioeconom ic pr ofile; ( b) assess t heir
percept ion regarding qualit y of life dim ensions; and ( c)
identify correlations between their socioeconom ic status,
education level and total score obtained on the Alzheim er’s
quality of life scale (QOL-AD)(10). At this m om ent, it should
be clarified that we adopted the following quality of life
dim ensions to be investigated: physical health, eagerness,
m ood, housing, m em ory, fam ily, m arriage, friends, t he
overall you, abilit y t o accom plish t asks, abilit y t o carry
out leisure activities, m oney, and life in general* .
METHODS
We p er f o r m ed a n ex p l o r a t o r y, d escr i p t i v e
s t u d y, w i t h a q u a n t i t a t i v e a p p r o a c h . D a t a w e r e
co l l e ct e d f r o m Au g u st 2 0 0 6 t o Ma r ch 2 0 0 7 , a t a
m edium - sized m unicipalit y in Cent ral Sao Paulo St at e,
Br azil, w it h a populat ion of 210,000, 12% of w hich is
aged 60 y ear s or m or e( 11).
St udy subj ect s w er e 80 elder ly people, user s
of t he m unicipal healt h syst em in 2006, w ho m et t he
in clu sion cr it er ion : b ein g at least eig h t y y ear s old .
The eligible part icipant s w er e select ed t hr ough a dr aw .
Th e f i r st 8 0 su b j e ct s w h o a g r e e d t o p a r t i ci p a t e
com pr ised t he st udy sam ple.
Dat a collect ion inst r um ent s w er e:
( a) char act er izat ion for m and sem ist r uct ur ed int er view
scr ipt : elaborat ed by t he r esearcher t o collect per sonal
in f or m at ion an d dat a abou t social liv in g, r ecen t lif e
ev en t s, f a m i l y co m p o si t i o n , h o b b i es a n d p h y si ca l
act iv it ies;
( b ) Br azi l Cr i t er i o n Qu est i o n n ai r e( 1 2 ): a scal e t h at
div ides t he populat ion int o sev en social classes ( A1,
A2, B1, B2, C, D, and E) by m eans of an ev aluat ion
of t he fam ily pur chase pow er, based on t he num ber
of durable consum er goods, inst ruct ion level of fam ily
head and som e ot her fact or s, such as having a house
m aid. People w it h t he highest pur chase pow er w er e
cat egor ized as “A1”, and t hose w it h low est as “ E” ;
( c ) Th e q u a l i t y o f l i f e w i t h Al z h e i m e r ’ s D i s e a s e
assessm ent scale ( QOL- AD)( 10): a t ranslat ed and
cross-cult ur ally adj ust ed inst r um ent v alidat ed for Br azil t o
assess t h e q u alit y of lif e of car eg iv er s an d eld er ly
w it h Alzheim er’s. The t hirt een scale aspect s evaluat ed
b y t h e p ar t icip an t ar e: p h y sical h ealt h , eag er n ess,
m ood, housing, m em or y, fam ily, m ar r iage, fr iend, t he
overall you, abilit y t o accom plish t asks, abilit y t o car r y
out leisur e act iv it ies, m oney, and life in general.
The follow ing scor es w er e used: 1 for “ bad” ;
2 for “ r egu lar ” ; 3 for “ good” ; an d 4 for “ excellen t ”.
The over all m inim um scor e w as 13 and t he m axim um
52. This inst rum ent w as chosen since it w as elabor at ed
f or eld er ly w it h cog n it iv e alt er at ion s an d p r ob ab le
Alzheim er’s Disease, but also for t heir caregivers, w ho
do n ot n ecessar ily pr esen t an y h ealt h pr oblem s n or
ar e aged over 60. Ther efor e, it is appr opr iat e for any
p er son . Mor eov er, sin ce t h e av er ag e p r ev alen ce of
Alzheim er’s Disease in t he w orld populat ion is 16.22%
a m o n g p e o p l e a g e d b e t w e e n 8 0 a n d 8 4 y e a r s ,
r eaching 54.83% for individuals over 95( 13), w e sought
an inst r um ent t hat w ould not exclude any per son w ho
m et t he research inclusion crit eria, so t hat t he result s
w ould show an ov er all pr ofile of oct ogenar ians.
Af t e r b e i n g a p p r o v e d b y t h e I n st i t u t i o n a l
Review Boar d at Sao Car los Federal Univer sit y, elder ly
w ho m et t he inclusion crit eria, along w it h t heir law fully
r e sp o n si b l e ca r e g i v e r s, w e r e i n f o r m e d a b o u t t h e
r esear ch an d i t s o b j ect i v es. Th o se w h o ag r eed t o
p ar t icip at e p r ov id ed w r it t en con sen t an d an sw er ed
t he inst r um ent s m ent ioned in t he pr evious par agr aph.
A single m eet ing w it h each par t icipant w as enough t o
collect and r ecor d t he dat a.
Th e c o l l e c t e d d a t a w e r e i n s e r t e d i n a
d at ab ase, u si n g t h e St at i st i cal Pr o g r am f o r So ci al
Scien ces ( SPSS- PC) f or Win d ow s, v er sion 1 0 . 0 , f or
st at ist ical calculat ions and analy ses.
RESULTS
Of all t he par t icipant s ( n= 80) , 58 w er e w om en
( 72.5% ) and 22 m en ( 27.5% ) . Aver age age w as 83.56
( ± 3 . 4 7 , xm in= 8 0, xm ax= 9 5 ) and 8 3 . 0 0 y ear s ( ± 2 . 9 1 ,
xm in= 8 0, xm ax= 9 0 ) , r espect iv ely.
I n t e r m s o f e d u c a t i o n , 6 0 ( 7 5 % ) w e r e
illit er at e or had not concluded elem ent ar y educat ion;
1 0 ( 1 2 . 5 % ) had com plet e elem ent ar y or incom plet e
pr im ar y edu cat ion ; 2 ( 2 . 5 % ) h ad com plet e pr im ar y
or in com p let e secon d ar y ed u cat ion ; 5 ( 6 . 3 % ) h ad
com plet e secondar y or incom plet e higher educat ion;
and 3 ( 3.8% ) had com plet e higher educat ion.
Dat a con cer n in g av er ag e f am ily in com e in
Br azilian Reais, obt ained t hr ough t he Br azil Cr it er ion
socioeconom ic quest ionnaire( 12), r evealed t hat 8 ( 10% )
par t icipan t s r eceiv ed R$ 2 8 0 4 ; 1 0 ( 1 2 . 5 % ) r eceiv ed
R$ 1 6 6 9 ; 2 4 ( 2 3 % ) r eceiv ed R$ 9 2 7 ; 3 7 ( 4 6 . 2 5 % )
r eceiv ed R$ 424; and 1 ( 1.25% ) r eceiv ed R$ 207.
Reg ar d i n g f am i l y co m p o si t i o n , w e v er i f i ed
t h at 7 ( 8 . 8 % ) w er e sin gle an d w it h ou t ch ildr en , 3 3
( 4 1 . 3 % ) w er e m ar r ied w it h ch ildr en , an d 4 0 ( 5 0 % )
w er e w idow ed. No subj ect s r epor t ed being separ at ed
or div or ced. As t o t he r elat ion bet w een t he v ar iables
g en d er an d m ar it al st at u s, 1 5 m en an d 1 8 w om en
h ad a com p an ion ; w id ow s w er e t h e m aj or it y, at a
r at io of 33: 7, and single subj ect s w er e all w om en.
I n t erm s of t heir part icipat ion in act ivit ies t hey
considered enhancing t o t heir healt h or qualit y of life,
41 oct ogenar ians ( 48.8% ) r epor t ed having no access;
29 ( 36.6% ) r epor t ed r eligion as a sour ce of happiness,
p l easu r e, or com f or t ; 3 ( 3 . 8 % ) p r act i ced p h y si cal
t her apy ; 2 ( 2. 5% ) follow ed psy chological t r eat m ent ;
2 ( 2 . 5 % ) did cr aft w or k ; 1 ( 1 . 2 5 % ) w as an elder ly
clu b m em b er ; 1 ( 1 . 2 5 % ) t ook p ar t in a u n iv er sit y
p r o g r a m f o r e l d e r l y ; a n d 1 ( 1 . 2 5 % ) f o l l o w e d
As t o spor t s act iv it ies, on ly w om en ( 1 . 3 % )
r epor t ed being a healt h club m em ber, 21 ( 26.3% ) w ent
w alking at least once a w eek, and m ost ( n= 58; 72.5% )
did not do any physical act ivit y at all.
I n term s of the total scores obtained on the
QOL-AD(10), on a scale from 13 to 52 possible points, the lowest
score was 19 and the highest was 48 (Figure 1).
Figur e 1 - Dist r ibut ion of scor es obt ained by QOL- AD
The evaluation frequencies participants reported
about their quality of life dim ensions are shown in Table 1.
Table 1 - Oct ogenar ians’ self- per cept ion about qualit y
of life dim ensions
When oct ogenarians’ inform at ion regarding t he
socioeconom ic st at us is cr ossed w it h educat ion lev el
an d t ot al QOL- AD( 1 0 ) scor e, t h er e is n o st at ist ically
sign if ican t cor r elat ion r egar din g edu cat ion lev el an d
qualit y of life. However, it can be st at ed t hat t here is a
t en den cy t ow ar ds h igh er scor es am on g people w it h
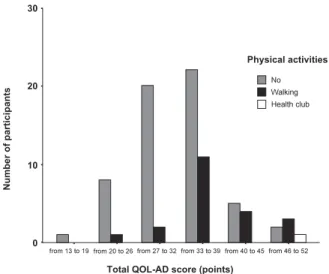
h igh er edu cat ion lev els ( Figu r e 2 ) . Par t icipan t s w h o
were used t o walking were m ore fulfilled ( m = 38.2381,
s d = 5 . 2 7 ) c o m p a r e d t o s e d e n t a r y p a r t i c i p a n t s
( m = 3 2 . 9 1 3 8 , sd = 6 . 2 8 3 6 ) , t ( 7 7 ) = 3 . 4 6 3 , p < 0 . 0 0 1
( Figure 3) . I t appears t hat t he average m ont hly incom e
is not affect ed by subj ect s’ qualit y of life. ( Figure 4) .
from 13 to 19 from 20 to 26 from 27 to 32 from 33 to 39 from 40 to 45 from 46 to 52
Total QOL-AD score (points) 0
10 20 30
Illiterate/incompl. elementary ed. Compl. elementary/incompl. primary ed. Compl. primary/incompl. secondary ed. Compl. secondary/incompl. superior ed. Compl. superior ed.
Education level
Number
of
participants
Figure 2 - Distribution of octogenarians per education level
and total quality of life score obtained through the QOL-AD
from 13 to 19 from 20 to 26 from 27 to 32 from 33 to 39 from 40 to 45 from 46 to 52
Total QOL-AD score (points) 0 10 20 30 No Walking Health club Physical activities Number of participants
Figur e 3 - Dist r ibut ion of oct ogenar ians per phy sical
act iv it y p er f or m an ce an d t ot al q u alit y of lif e scor e
obt ained t hr ough t he QOL- AD
from 13 to 19 from 20 to 26 from 27 to 32 from 33 to 39 from 40 to 45 from 46 to 52
Total QOL-AD score (points)
&" $$' ' %
Monthly income (R$)
" " % 0 2 4 6 8 10 12 14 16 s n o i s n e m i D n o i t p e c r e p -f l e S l a t o T d o o
G Regular Good Excellent
n % n % n % n % n %
h t l a e H l a c i s y h
P 11 13.8 34 42.5 30 37.5 5 6.3 80 100 s s e n r e g a
E 17 21.3 22 27.5 30 37.5 11 13.8 80 100 d
o o
M 7 8.8 15 18.8 45 56.3 13 16.3 80 100 g n i s u o
H - - 7 8.8 68 85 5 6.3 80 100 y
r o m e
M 16 20 16 20 28 35 20 25 80 100 y
l i m a
F - - 1 1.3 64 80 15 18.8 80 100 ) p i h s n o i t a l e r ( e g a i r r a
M - - 3 3.8 52 65 25 31.3 80 100 s d n e i r
F 5 6.3 7 8.8 47 58.8 21 26.3 80 100 u o y ll a r e v o e h
T 2 2.5 24 30 43 53.8 11 13.8 80 100 h s il p m o c c a o t y t il i b A s k s a
t 24 30 13 16.3 30 37.5 13 16.3 80 100 m r o f r e p o t y t il i b A s e i t i v i t c a l a c i s y h
p 23 28.8 20 25 27 33.8 10 12.5 80 100 y
e n o
M 22 27.5 50 62.5 8 10 - - 80 100 l a r e n e g n i e f i
L 8 10 40 50 29 36.3 3 3.8 80 100
l a t o
T 13512.9725224.2250148.1915214.621040
Figur e 4 - Dist r ibut ion of oct ogenar ians per av er age
m ont hly incom e and t ot al qualit y of life scor e obt ained
DI SCUSSI ON
Our r esear ch is in agr eem ent w it h num er ous
st udies t hat point at t he pr evalence of fem ales in t he
elder ly popu lat ion . Th is in for m at ion is im por t an t for
planning and im plem ent ing int er vent ion pr ogr am s and
pr ev en t iv e h ealt h act ion s.
I n t er m s of educat ion, it is w or t h obser v ing
t hat high illit eracy rat es are due t o difficult access t o
school. Men had higher educat ion levels com par ed t o
w o m en , an d al l p ar t i ci p an t s w i t h co m p l et e h i g h er
educat ion w er e m en. That w as expect ed since, in t he
past , cult ur e did not value w om en’s school educat ion.
I n fact , w om en w er e oft en r aised t o be good w iv es,
m ot her s and housew ives. Today, it is bet t er under st ood
w h y m an y p u b lic in cen t iv es an d n on - g ov er n m en t al
act ion s f ocu s on lit er acy an d con t in u ou s ed u cat ion
pr ogr am s for adult s and elder ly.
Regarding socioeconom ic st at us, according t o
pr e- ex ist ing dat a about t he Sao Paulo populat ion( 12),
w e e x p e c t e d t o f i n d a g r e a t e r c o n c e n t r a t i o n o f
individuals wit h an average fam ily incom e of R$927.00;
how ever, t he m aj orit y of t he sam ple ( n= 37, 46.25% )
r ecei v ed a n i n co m e l o w er t h a n a p p r o x i m a t el y R$
424.00. This dat a is im port ant , since inferior incom es
could lim it people’s access t o nut rit ional and social care,
e sp e ci a l l y f o r h e a l t h a n d e d u ca t i o n , si g n i f i ca n t l y
com pr om ising people’s qualit y of life.
The subj ect ivit y of t he qualit y of life const r uct
w as confir m ed in our st udy, ev idencing t hat w elfar e
is influenced by m ult iple fact ors, w hich are not lim it ed
by t im e, as w ell as socioeconom ic, cult ural and healt h
con d it ion s.
CONCLUSI ONS
The st udy populat ion’s pr ofile m ainly consist s
of fem ale w idow s, illit erat e or w it h incom plet e prim ary
educat ion, fr om classes “ C” or “ D”. I n addit ion, t hey
do not pract ice any kind of physical act ivit y, com plain
abou t t h e lack of leisu r e oppor t u n it ies for t h eir age
gr oups, and t heir gr eat est encour agem ent for qualit y
of life is r eligion. They lack access t o healt h ser v ices
l i k e o c c u p a t i o n a l t h e r a p y, p h y s i c a l t h e r a p y a n d
psy ch ological t r eat m en t s.
Old age is a m om ent in t he life cycle in w hich
biopsychosocial int er act ions ar e ver y nar r ow( 14,15) and
m ost of t h e st u dy su bj ect s w er e f u lf illed w it h t h eir
fam ily, m ar r iage, close r elat ion sh ips an d t h eir place
of r esiden ce. Nev er t h eless, it is im por t an t t o st r ess
t hat none of t hem w er e st ay ing in shelt er s, nur sing
hom es, hospit als or inst it ut ions. This m ay have caused
a posit iv e bias in t he ev aluat ion of t hese v ar iables.
The aver age m ont hly incom e w as t he highest
poin t of t h e oct ogen ar ian s’ dissat isfact ion . How ev er,
w e d i d n o t f i n d a n y r e l a t i o n s h i p b e t w e e n t h e
i n d i v i d u a l s ’ s e l f - p e r c e p t i o n a n d t h e i r r e a l
socioeconom ic level; t hat is, m any of t hose w it h higher
in com e r epor t ed bein g j u st as dissat isf ied as t h ose
w it h low er in com es. Th e m ost f r eq u en t com p lain t s
regarded healt h, readiness and lack of leisure opt ions
for t he elder ly.
I t a p p e a r s t h a t t h e r e s e a r c h e r s ’
socioeconom ic lev el did not hav e any posit iv e effect
on t he per cept ion of ov er all qualit y of life. How ever,
t h e o b t a i n e d d a t a su g g e st a t e n d e n cy o f h i g h e r
e d u c a t i o n a l l e v e l s a n d i n v o l v e m e n t i n p h y s i c a l
act iv it ies, r esu lt in g in h ig h er QOL- AD scor es. Th is
dir ect s us t o t he concer n t hat public policies should
encour age t he or ganizat ion of phy sically appr opr iat e
and safe ar eas for w alking or doing adapt ed exer cises.
Mor eov er, ed u cat ion an d lear n in g r esou r ces sh ou ld
be per m anent ly pr om ot ed w it h a v iew t o m inim izing
t he cult ural dist ance bet w een generat ions, w hich could
cause loneliness and social isolat ion. I n addit ion, j ust
as im port ant as t he availabilit y is t he diffusion of t hese
r esour ces in t he com m unit y, so t hat people hav e t he
r ight t o choose bet w een par t icipat ing or not in w hat is
o f f e r e d i n t h e i r a r e a , i n t e r m s o f r e so u r ce s a n d
act iv it ies.
We r ecognize t hat t his st udy does not per m it
u s t o m a k e g e n e r a l i z a t i o n s d u e t o s o m e
m et hodological lim it at ions; for exam ple, it is a specific
experience, in one cit y, w it h a relat ively sm all num ber
of par t icipant s ( n= 80) . I t w ould also be int er est ing t o
com par e t he sam ple w it h a gr oup of elder ly y ounger
t han 80, since it w ould per m it a bet t er assessm ent on
t he im pact of age on people’s qualit y of life. How ever,
t he im por t ance of st udy ing populat ions aged ov er 80
y ear s can be ar gu ed, du e t o t h e scar cit y of st u dies
on t h ese su bj ect s an d t h e acceler at ed dem ogr aph ic
incr em ent of elder ly ar ound t he w or ld.
Despit e t hese lim it at ions, and based on t he
obt ained r esult s, it can be affir m ed t hat people w it h
a d v a n c e d a g e h a v e l i v e d i n a d v e r s e c o n d i t i o n s
r egar ding t heir access t o em pow er m ent oppor t unit ies
and r esour ces. I t should be em phasized t hat
aging-elat ed issues should consider t he ent ir e div er sit y t he
FI NAL CONSI DERATI ONS
Wit h healt h advancem ent s, t he t endency t hat
people w ill liv e longer is incont est able. Ther efor e, it
should be seen t o t hat t his t r ack be pur sued in t he
m ost sat isfact or y w ay possible, by m eans of planning
p r o ce sse s t h a t o p t i m i ze a cce ss t o r e so u r ce s a n d
o p p o r t u n i t i es o f m ai n t ai n i n g an d i m p r o v i n g so ci al
par t icipat ion , w elfar e, in depen dence an d dign it y.
I t i s i n d i s p e n s a b l e t h a t i n f o r m a t i o n b e
collect ed am ong t he elder ly populat ion, inv est igat ing
econ om ic, cu lt u r al an d em ot ion al asp ect s, so t h at
gov er nm ent al st r at egies fav or t he im plem ent at ion of
p r og r am s t h at p r om ot e t h e im p r ov em en t of eld er s’
qualit y of liv e, based not only on t heir const it ut ional
right s, but also an t heir real needs. By ident ifying t he
t arget populat ion’s profile, as w ell as t heir specificit ies,
it is possible t o m ak e per sonalized int er v ent ions t hat
cont ribut e t o im prove qualit y of life and r educe public
ex pen ses on h ealt h car e.
Th e pr of ession als in v olv ed, especially t h ose
i n h e a l t h a n d so ci a l se r v i ce s, r e q u i r e co n t i n u o u s
t r aining and em pow er m ent so t hey can offer ser vices
co m p a t i b l e w i t h t h e n e w d e m o g r a p h i c d e m a n d s.
Modu les abou t h ealt h y agin g, as w ell as in st r u ct ion
c o n c e r n i n g s e l f - c a r e , h e a l t h m a i n t e n a n c e a n d
en h an cem en t sh ou l d b e i n cor p or at ed i n t o t r ai n i n g
cour ses, as t he basis for t he consensual const r uct ion
o f n e w a p p r o a c h e s t h a t r e s p e c t g e n e r a t i o n
differ en ces, w it h ou t discr im in at ion .
Si n ce t h e f a m i l y e n v i r o n m e n t ca n b e t h e
sou r ce of su p p or t f or d ealin g w it h ad v er sit ies, t h e
e n c o u r a g e m e n t a n d s t r e n g t h f o r p a r t n e r s h i p s
b et w een f a m i l y a n d p r o f essi o n a l ca r eg i v er s co u l d
m in im ize t h e d if f icu lt ies b ot h ex p er ien ce. Th r ou g h
m u t u a l ef f o r t , w e ca n t h i n k o f a l l t h e p r ev en t i v e
m easu r es an d in t er v en t ion s t h at w ou ld en su r e t h at
a g i n g i s s e e n a s a c o n q u e s t , b y m e a n s o f t h e
r esi g n i f i cat i o n o f n eg at i v e v al u es an d st er eo t y p es
associat ed w it h old age.
REFERENCES
1 . Wor d Healt h Or g an izat ion . En v elh ecim en t o at iv o: u m a polít ica de saúde. Br asília ( DF) : Or ganização Pan- Am er icana da Saú de; 2 0 0 5 .
2 . Ro d r i g u e s D . D e z i d é i a s ( m a l ) f e i t a s so b r e e d u ca çã o inclusiva. I n: Rodr igues D, or ganizador. I nclusão e educação: d oze olh ar es sob r e a ed u cação in clu siv a. São Pau lo ( SP) : Su m m u s; 2 0 0 6 . p . 2 9 9 - 3 1 8 .
3 . Jan n u zzi GM. A Ed u cação d o d ef i ci en t e n o Br asi l : d o s pr im ór dios ao início do século XXI . São Paulo ( SP) : Aut or es Asso ci a d o s; 2 0 0 4 .
4 . Pi r e s J. A q u e s t ã o é t i c a f r e n t e à s d i f e r e n ç a s : u m a p e r s p e c t i v a d a p e s s o a c o m o v a l o r. I n : M a r t i n s LA R, or g an izad or. I n clu são: com p ar t ilh an d o sab er es. Pet r óp olis ( RJ) : Vozes; 2 0 0 5 . p. 7 8 - 9 4 .
5 . Alm eid a N Filh o. Th e con cep t of h ealt h : b lin d - sp ot f or epidem iology. Rev Bras Epidem iol 2000 dezem bro; 3( 1- 3) : 4- 20. 6. Ram os LR. Fatores determ inantes do envelhecim ento saudável em idosos resident es em cent ro urbano: Proj et o Epidoso, São Paulo. Cad Saúde Pública 2003 j unho; 19( 3) : 793- 7. 7 . M a r t u r a n o EM . Fa t o r e s d e r i s c o e p r o t e ç ã o n o d e s e n v o l v i m e n t o s ó c i o e m o c i o n a l d e c r i a n ç a s c o m dificuldades de apr endizagem . I n: Mendes EG, Alm eida MA, Willian s LCA, or gan izador as. Tem as em Edu cação Especial: av an ço s r ecen t es. São Car l o s ( SP) : ED UFSCar ; 2 0 0 4 . p . 1 5 9 - 6 5 .
8. Br onfenbr enner U. A ecologia do desenvolvim ent o hum ano: exper im ent os nat ur ais e planej ados. Por t o Alegr e ( RS) : Ar t es Mé d i ca s; 1 9 9 6 .
9. Paschoal SMP. Qualidade de v ida do idoso: const r ução de um inst r um ent o de av aliação at r av és do m ét odo do im pact o clínico. [ Tese de Dout or ado] . São Paulo ( SP) : Faculdade de Me d i ci n a / USP; 2 0 0 4 .
10. Nov elli MMPC. Validação da escala de qualidade de v ida ( QdV- DA) par a pacien t es com doen ça de Alzh eim er e seu s r espect ivos cuidador es fam iliar es. [ Tese de Dout or ado] . São Pau lo ( SP) : Facu ldade de Medicin a/ USP; 2 0 0 6 .
1 1 . I BGE ( BR) . Est at íst icas d a Saú d e: Assist ên cia Méd ica Sanit ár ia. Depar t am ent o de População e I ndicador es Sociais. Rio de Janeir o ( RJ) : I BGE; 1999.
12. Associação Nacional de Em presas de Pesquisa [ hom epage n a i n t e r n e t ] . B e l o H o r i z o n t e : A s s o c i a ç ã o N a c i o n a l d e Em p r esas d e Pesq u i sa; [ Acesso em 2 0 0 5 d ezem b r o 1 3 ] . Cr i t é r i o d e Cl a s s i f i c a ç ã o Ec o n ô m i c a B r a s i l ; [ 3 t e l a s ] . Disponível em : ht t p: / / www.anep.org.br/ codigosguias/ CCEB.pdf 1 3 . Lop es MA, Bot t in o CMC. Pr ev alên cia d e d em ên cia em d i v e r s a s r e g i õ e s d o m u n d o : A n á l i s e d o s e s t u d o s epidem iológicos de 1 9 9 4 a 2 0 0 0 . Ar q Neu r o- Psiqu iat r 2 0 0 2 m ar ço; 6 0 ( 1 ) : 6 1 - 9 .
14. Dessen MA, Silva NLP. A fam ília e os program as de intervenção: t endências at uais. I n: Mendes EG, Alm eida MA, Willians LCA, organizadoras. Tem as em Educação Especial: avanços recent es. São Carlos ( SP) : EDUFSCar; 2004. p. 179- 87.
1 5 . Ma i a LC, D u r a n t e AMG, Ra m o s LR. Pr e v a l ê n c i a d e t r anst or nos m ent ais em ár ea ur bana no nor t e de Minas Ger ais. Rev Saú de Pú blica 2 0 0 4 ou t u br o; 3 8 ( 5 ) : 6 5 0 - 6 .