BrazJOtorhinolaryngol.2016;82(3):353---364
www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
REVIEW
ARTICLE
Intratympanic
corticosteroid
for
sudden
hearing
loss:
does
it
really
work?
夽
,
夽夽
Monique
Antunes
de
Souza
Chelminski
Barreto
a,b,c,d,
Aleluia
Lima
Losno
Ledesma
d,
Carlos
Augusto
Costa
Pires
de
Oliveira
d,
Fayez
Bahmad
Jr
e,∗aPostgraduateSpeechandHearing,UniversidadeFederaldeSantaMaria(UFSM),SantaMaria,RS,Brazil bEducationalPsychology,UniversidadeFederaldoRiodeJaneiro(UFRJ),RiodeJaneiro,RJ,Brazil cAudiologyandNeurotology,UniversidadeFederaldePernambuco(UFPE),Recife,PE,Brazil
dUniversidadedeBrasília(UnB),Brasília,DF,Brazil
eOtologyandNeurotology,HarvardMedicalSchool,Boston,USA
Received15April2015;accepted23June2015 Availableonline6November2015
KEYWORDS
Suddenhearingloss; Suddendeafness; Corticosteroids
Abstract
Introduction:Suddendeafnessischaracterizedbyanabrupthearinglossofatleast30dBin three sequentialfrequencies in thestandardpure toneaudiogram overthree daysor less. Treatment isbased onits etiology,and oralcorticosteroids arewidelyused. Intratympanic corticosteroidsareincludedasprimaryorsecondarytreatmentwhenthereisnoimprovement withtheuseoforalcorticosteroids.
Objective: Todeterminetheeffectiveness oftherapywithintratympanicsteroidsinsudden deafness.
Methods:Asystematicreviewwasperformedofpublicationsonthetopicinthedatabasesof PubMed/MEDLINE,withthekeywords:suddendeafness,suddenhearingloss,and corticoste-roids.
Results:Thirty scientificstudieswereanalyzed.Astotheobjectivesofthestudyanalyzed, 76.7%soughttoevaluatetheuseofintratympanictherapysalvageafterfailuretoconventional treatment,andintratympanictherapywasusedastheprimarytreatment23.3%ofthestudies.
夽 Pleasecitethisarticleas:BarretoMASC,LedesmaALL,deOliveiraCACP,BahmadJrF.Intratympaniccorticosteroidforsuddenhearing
loss:doesitreallywork?BrazJOtorhinolaryngol.2016;82:353---64.
夽夽Institution:UniversidadedeBrasília(UnB),Brasília,DF,Brazil.
∗Correspondingauthor.
E-mail:[email protected](F.BahmadJr). http://dx.doi.org/10.1016/j.bjorl.2015.06.007
Conclusion:Intratympaniccorticosteroidtherapyisprescribedprimarilywhenthereisfailure ofconventionaltherapy andwhenitis limitedtousesystemic corticosteroids,such asthe diabeticpatient.
© 2015Associac¸˜ao Brasileira de Otorrinolaringologiae CirurgiaC´ervico-Facial. Publishedby ElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE
Perdasúbitada audic¸ão; Surdezsúbita; Corticosteroides
Corticosteroideintratimpânicoparaperdasúbitadaaudic¸ão:issorealmente funciona?
Resumo
Introduc¸ão:Asurdezsúbitaécaracterizadaporumaperdaabruptadaaudic¸ãodepelomenos 30dBemtrêsfrequênciassequenciadasnoaudiogramatonalderotinaaolongodetrêsdias,ou menos.Otratamentoéfundamentadoemsuaetiologiaecorticosteroidesoraissãoamplamente utilizados.Aterapiacomcorticosteroideintratimpânicofoiincluídacomotratamentoprimário ousecundárionoscasosemquenãohouvemelhoracomousodecorticosteroidesorais. Objetivo:Determinaraeficáciadaterapiaintratimpânicacomesteroidesemcasosdesurdez súbita.
Método: Foirealizada uma revisão sistemáticadaspublicac¸õessobre otópicono bancode dadosPubmed/Medline,comaspalavras-chave:surdezsúbita,perdasúbitadaaudic¸ãoe cor-ticosteroides.
Resultados: Foramanalisados30 estudoscientíficos.Com relac¸ãoaosobjetivos dosestudos analisados,76,7%procuravamavaliarousodaterapiaintratimpânicaemseguidaaoinsucesso com otratamento convencional; aterapia intratimpânica foi empregada como tratamento primárioem23,3%dosestudos.
Conclusão:Aterapiacomcorticosteroideintratimpânicoéprescritaprimariamentenoscasos deinsucessocomaterapiaconvencionalequandohálimitac¸ãoparaousodecorticosteroides sistêmicos,comoocorrecomopacientediabético.
©2015Associac¸˜aoBrasileira deOtorrinolaringologiaeCirurgiaC´ervico-Facial.Publicadopor ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Suddenhearingloss(SHL)wasfirstdescribedbydeKleynin 1944anddefinedasahearinglossofatleast30dBinthree sequentialfrequenciesinthestandardpuretoneaudiogram over three days or less.1 It may be characterized as an impairmentoftheinnerearand/orcentralauditory path-ways,withvariableintensity and frequency,ranging from mildfeelingofearbeingcloggedtototallossofhearing.2,3 Althoughitisthoughttooriginatemainlyfromviral, vas-cular,or immunologiccauses, theetiopathogenesis ofthe diseaseisstillunknown,sothe diseaseisusuallyreferred toasidiopathicsuddenhearingloss(ISHL).Ithasareported incidenceof5---20per100,000patientsperyear,withamean of50---60yearsandnopredominanceofsex.Inmostcases, thereisunilateral hearingloss,withbilateralinvolvement reportedinlessthan5%.1
Recoveryrateinuntreatedpatientsrangesfrom25%to 50%,mostlyresolvingwithintwoweeksof onsetof symp-toms.Although themethods oftreatment of SHLpatients varyamongdifferentcenters,systemicsteroid(SS)therapy isthemostcommonlyusedmodalityfortreatmentofsudden hearingloss.2
Thetreatmentofsuddenhearinglossisbasedonits etiol-ogy.Inidiopathiccases,oralcorticosteroidsarewidelyused;
intratympanic steroids have been trialed in patients with sudden hearingloss, becausetheyprovide a high concen-tration in the labyrinth in animal models,1 although their resultsareconflicting.
Thereareseveraladvantagesofintratympanictreatment (Table 1): (1) the procedure is well tolerated and rela-tivelyeasytoperformasanoutpatientprocedureperformed under local anesthesia (topical); (2) general anesthesia canbeavoided;(3)mostpatientsunderstand theconcept of intratympanic therapy and easily accept the proposed therapy.4
Intratympanic steroid has become an attractive alter-native, especiallyin caseswhensystemictherapyfails,or to avoid the side effects of the systemicuse of steroids. However,thestandardization of numberandfrequency of intratympanictreatmentsanddrugdeliverymethodsremain tobedetermined.5---7
Intratympaniccorticosteroidforsuddenhearingloss 355
Table1 Advantagesofintratympanictreatment.
Advantages
Outpatientprocedure Easilyadministered
Itcanbegivensoonafterdiagnosis Relativelypainless
Possibleuseinpatientsinwhichcorticosteroidsare contraindicated(e.g.:immunesuppression,HIV, tuberculosis,diabetes)
Highdrugconcentrationwhenadministereddirectly ontheaffectedear
Disadvantages/complications Invasiveprocedure
Tympanicmembraneperforation Pain
Otitismedia
Vertigo(generallytemporary) Hearingloss
Theaimofthisstudywastopresenttheeffectivenessof intratympaniccorticosteroidtherapyinsuddenhearingloss.
Methods
This was a systematic review that followed the precepts of the Cochrane Handbook as to the formulation of the question,location,selection,andcriticalevaluationofthe articles.Theresearchwasbaseduponthequestion‘‘should intratympaniccorticosteroidtherapy beindicatedfor sud-dendeafness?’’with‘suddendeafness’and‘suddenhearing loss’associatedbytheBooleanANDoperatorto ‘corticoste-roids’.Alldescriptorsarecontainedinthevocabularyand PubMed/MEDLINE usingasstrategy thedescriptor Medical SubjectHeadingTerms(MeSH).
ThetypeofstudyandEnglishlanguagewereconsidered asinclusion criteria.Thus,articleswritteninanother lan-guage, case studies, and lettersto theeditor andreview articleswereexcluded.
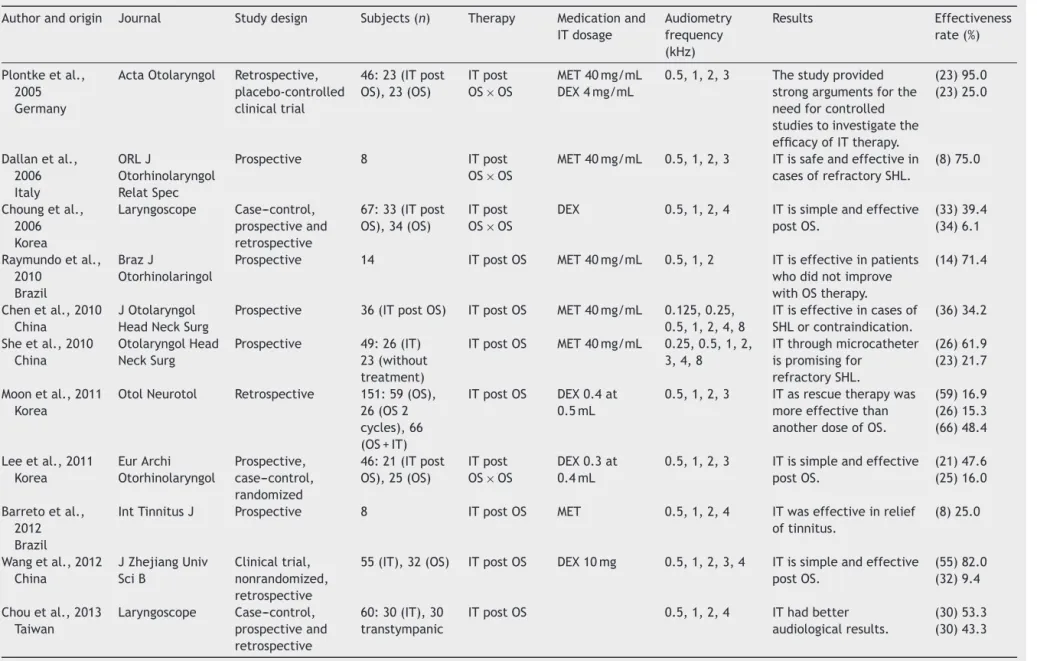
Abstracts from 149 articles were assessed by two reviewers, who pre-selectedfor analysisthose correlated descriptorsfocusingontheapplicationofintratympanic cor-ticosteroidinisolation,asrescuetherapy,orincombination. A total of 30 items had tabular data containing the following information: author,origin and year of publica-tion,journal,samplesize(n),studydesign,descriptionof intratympanic corticosteroids andcorticosteroid, frequen-ciesanalyzedinpuretoneaudiometry,andresultsofstudies (Tables2---5).
Results
Regardingthedesignofthestudies,63.3%wereprospective, 30%and6.7%retrospectiveprospectiveandretrospective. Onlythreestudies(10%)werecontrolledandrandomized. Three other studies (10%) were randomizedand only two (5%)werecontrolled.
Astotheobjectivesofthestudiesanalyzed,76.7%sought toevaluatetheuseofintratympanictherapysalvageafter failureofconventionaltreatment.Treatmenttherapywith
systemicsteroids wasconsidered asconventional therapy; 52.2% of the studies used oral administration and 47.8%, intravenousadministration.Intratympanictherapywasused astheprimarytreatment23.3%ofthestudies.
Itis noteworthythat100%of thestudiesusedauditory evaluationbypuretoneaudiometryasamethodof check-ingtheeffectivenessofthetherapychosen,mainlyusingas improvementcriteria20dBincrease inthemean frequen-ciesof0.5,1,2,and4kHz.Ofthese,somestudiesincluded evaluationthroughspeechaudiometryandimpedance.
Analyzingthe articlespublishedonsudden hearingloss anduse of intratympanic corticosteroidtherapy, thedata showedthatthisis apromising treatmentmodality, espe-ciallyforcaseswheretherewasafailureintheconventional treatment,aswellasinthosewheresystemiccorticosteroid therapyiscontraindicated.
It can be seen that in most of the analyzed studies, theauthorsmadethreeintratympaniccorticosteroid appli-cations, usually every other day. However, dosages were different,rangingfromonetofiveapplications.
Puretoneaudiometrywastheaudiologicaltestusedin allthestudiesanalyzed.However,becauseofthepossibility ofsudden deafness is multifactorial andaffects theinner earand/or auditorypathways,theauthorssuggest testing electrophysiologicalobjectivesaccompanyingapatient.
The study by Rauch et al. in 2011 comparedthe non-inferiority in the two therapeutic approaches for sudden deafness(intratympanic and oral), and250 subjectswere followedforaperiodofsix months.They foundthat non-inferioritywas defined as a difference of less than 10dB inhearingimprovementbetweentreatments.Inthegroup treated with oral prednisolone (n=121), the pure tone average (PTA) improved 30.7dB compared to the group receiving intratympanic corticosteroid therapy (n=129), whopresentedimprovementof28.7dB.4Similarlytothese authors,Dallanetal.,8 inItaly, alsofollowedpatients for sixmonths.However,theirstudyexaminedtheefficacyof intratympanic corticosteroid therapy after failure of oral therapy.
Other researchersfollowed-upfor uptothreemonths, andmostofthetime,duringonlyonemonthafterstarting treatmentwithintratympaniccorticosteroid.
Thefollowingstudiesarepresentedaccordingtothetype oftherapyused.
Salvagetherapyafterfailureoforalsteroids
Plontkeetal.evaluated23patientswithunilateralsevere and profound SHL refractory to initial systemic therapy andcomparedthem withacontrol group(n=23)whodid not receive salvage treatment. The PTA threshold after intratympanicsalvagetreatmentshowedastatistically sig-nificantimprovementof15dB(7---24dB).Thelocaltherapy group showed a significantly better improvement (mean 19dB,6---32dB)thanthehistoricalcontrolgroup(mean5dB, 2---11dB).9
Barreto
MASC
et
al.
Table2 Studiesemphasizingsalvagetherapyfailureoforalsteroids.
Authorandorigin Journal Studydesign Subjects(n) Therapy Medicationand ITdosage
Audiometry frequency (kHz)
Results Effectiveness rate(%)
Plontkeetal., 2005 Germany
ActaOtolaryngol Retrospective, placebo-controlled clinicaltrial
46:23(ITpost OS),23(OS)
ITpost OS×OS
MET40mg/mL DEX4mg/mL
0.5,1,2,3 Thestudyprovided strongargumentsforthe needforcontrolled studiestoinvestigatethe efficacyofITtherapy.
(23)95.0 (23)25.0
Dallanetal., 2006 Italy
ORLJ
Otorhinolaryngol RelatSpec
Prospective 8 ITpost OS×OS
MET40mg/mL 0.5,1,2,3 ITissafeandeffectivein casesofrefractorySHL.
(8)75.0
Choungetal., 2006 Korea
Laryngoscope Case---control, prospectiveand retrospective
67:33(ITpost OS),34(OS)
ITpost OS×OS
DEX 0.5,1,2,4 ITissimpleandeffective postOS.
(33)39.4 (34)6.1
Raymundoetal., 2010
Brazil
BrazJ
Otorhinolaringol
Prospective 14 ITpostOS MET40mg/mL 0.5,1,2 ITiseffectiveinpatients whodidnotimprove withOStherapy.
(14)71.4
Chenetal.,2010 China
JOtolaryngol HeadNeckSurg
Prospective 36(ITpostOS) ITpostOS MET40mg/mL 0.125,0.25, 0.5,1,2,4,8
ITiseffectiveincasesof SHLorcontraindication.
(36)34.2
Sheetal.,2010 China
OtolaryngolHead NeckSurg
Prospective 49:26(IT) 23(without treatment)
ITpostOS MET40mg/mL 0.25,0.5,1,2, 3,4,8
ITthroughmicrocatheter ispromisingfor
refractorySHL.
(26)61.9 (23)21.7
Moonetal.,2011 Korea
OtolNeurotol Retrospective 151:59(OS), 26(OS2 cycles),66 (OS+IT)
ITpostOS DEX0.4at 0.5mL
0.5,1,2,3 ITasrescuetherapywas moreeffectivethan anotherdoseofOS.
(59)16.9 (26)15.3 (66)48.4
Leeetal.,2011 Korea
EurArchi Otorhinolaryngol
Prospective, case---control, randomized
46:21(ITpost OS),25(OS)
ITpost OS×OS
DEX0.3at 0.4mL
0.5,1,2,3 ITissimpleandeffective postOS.
(21)47.6 (25)16.0
Barretoetal., 2012 Brazil
IntTinnitusJ Prospective 8 ITpostOS MET 0.5,1,2,4 ITwaseffectiveinrelief oftinnitus.
(8)25.0
Wangetal.,2012 China
JZhejiangUniv SciB
Clinicaltrial, nonrandomized, retrospective
55(IT),32(OS) ITpostOS DEX10mg 0.5,1,2,3,4 ITissimpleandeffective postOS.
(55)82.0 (32)9.4
Chouetal.,2013 Taiwan
Laryngoscope Case---control, prospectiveand retrospective
60:30(IT),30 transtympanic
ITpostOS 0.5,1,2,4 IThadbetter audiologicalresults.
(30)53.3 (30)43.3
Intratympanic
corticosteroid
for
sudden
hearing
loss
357
Table3 Studiesemphasizingsalvagetherapyafterfailureofintravenoussteroids.
Authorandorigin Journal Studydesign Subjects(n) Therapy Medicationand ITdosage
Audiometry frequency(kHz)
Results Effectiveness rate(%)
Kakehataetal., 2006
Japan
OtolNeurotol Prospective Diabetics
31:10(IT),21(IV)
IT×IV DEX4mg/mL 0.25,0.5,1,2,4 ITisaseffectiveas IV.
(10)100.0 (21)67.0
Xenellisetal., 2006 Greece
OtolaryngolHead NeckSurg
Prospective 37:19(ITpostIV), 18(IV)
ITpostIV MET40mg/mL 0.5,1,2,4 ITpostfailureIVis safeandeffective incasesof refractorySHL.
(19)47.0 (18)0.0
PlazaandHerráiz, 2007
Spain
OtolaryngolHead NeckSurg
Prospective, non-randomized
18:9(ITpostIV), 9(OSpostIV)
ITpostIV MET20mg/mL 0.5,1,2,3 ITissafeand effectiveincasesof refractorySHL.
(9)55 (9)0.0
Plontkeetal., 2009 Germany
Laryngoscope Randomized, double-blind, placebo-controlled, multicenter
23 ITpostIV DEX 0.5,1,2,4 IThadbetter results.
(23)24.4
Dallanetal.,2010 Italy
OtolNeurotol Retrospective 27 ITpostIV MET40mg/mL 0.5,1,2,3 ITiseffectivein casesofrefractory SHL.
(27)55
Lietal.,2011 China
Audiol& Neurotol
Prospective 65:24ITpostIV, 21topicpostIV, 20IV
ITpostIV MET40mg/mL 0.5,1,2,4 ITisefficientrescue (24)37 (21)0.0 (20)0.0
Barreto
MASC
et
al.
Table4 Studiesemphasizingprimarytherapy.
Authorandorigin Journal Studydesign Subjects(n) Therapy Medicationand ITdosage
Audiometry frequency(kHz)
Results Effectiveness rate(%)
Banerjeeand Parmers,2005 Canada
OtolNeurotol Retrospective 26 IT MET40mg/mL 0.5,1,2 ITissafeand effective,no significantadverse effects.
(26)75.4
Filipoetal.,2010 Italy
Acta Otolaryngol
Prospective 34 IT P62.5mg/mL 0.5,1,2 ITwaseffective. (34)79.3
Rauchetal.,2011 USA
JAMA Clinicaltrial, prospective, randomized, multicenter
250:129(IT) IT×OS MET40mg/mL 0.5,1,2,4 ITcanbeused whenthereis contraindication toOS.
(129)86.8 (121)87.6
Kakehataetal., 2011
Japan
Audiol& Neurotol
Retrospective 76:19IT,24IT postOS,33OS
IT×OS×IT postOS
DEX4mg/mL 0.25,0.5,1,2,4 Short-termIThas highresponserate andhealing,and canbeusedasa firstorsecond choice.
(19)95.0 (24)63.0 (33)84.0
Zhangetal.,2012 China
Acta Oto-Laryngologica
Prospective 74:35IT,39IT postOS
IT DEX0.5at 0.7mL
0.25,0.5,1,2,4 ITiseffectiveas firstchoiceandas rescuetherapy, andthe
Eustachiantubeis anoninvasiveway toprovidesafe medication administration.
(35)80.0 (39)64.1
Filipoetal.,2013 Italy
Laryngoscope Prospective, randomized, triple-blind
50:25(IT),25 (without treatment)
IT MET40mg/mL 0.25,0.5,1,2,3, 4,8
ITwaseffective. (25)76.0 (25)20.0
Intratympanic
corticosteroid
for
sudden
hearing
loss
359
Table5 Studiesemphasizingcombinationtherapy.
Authorandorigin Journal Studydesign Subjects(n) Therapy Medicationand ITdosage
Audiometry frequency(kHz)
Results Effectiveness rate(%)
Lautermann etal.,2005 Germany
EurArch Otorhinolaryn-gol
Prospective, nonrandomized
27:14(IV),13 (IT+IV)
IV×IT+IV MET32mg/mL 0.5,0.75,1,2, 3,4
ITdidnotincrease thehearinggain.
(14)51.8 (13)48.4
Gouverisetal., 2011 Germany
OtolNeurotol Retrospective 170:94HL moderate(IV) 76HLsevere (IV+IT)
IV×IV+IT DEX0.4mL, 8mg/mL
0.5,1,2,4,8 Therewasno differencebetween thegroups.
(94)70.0 (76)73.0
Arslanetal., 2011 Turkey
OtolNeurotol Prospective 128:73 (IV+OS),84 (ITpostOS)
ITpost OS×IV+OS
MET0.5mL 125mg/mL
0.5,1,2,4 ITasrescuetherapy increasedthe likelihoodofhearing recovery.
(73)40.0 (84)70.0
Baeetal.,2013 Korea
Acta Oto-Laryngologica
Retrospective 735:94(IT), 444(OS),197 (OS+IT)
IT×OS×IT+OS DEX0.5at 0.6mL
0.5,1,2,3 ITwasaseffectiveas OSandOS+ITshould indicatewhenthere isacontraindication toOS.
94(64.9) 444(68.7) 197(59.3)
Koltsidopoulos etal.,2013 Greece
OtolNeurotol Prospective, clinicaltrial, quasi-randomized, controlled
92 46
(IT+OS)×46 (IV+OS)
IT+OS×IV+OS DEX0.4at 0.6mL
0.5,1,2,4 IT+OSweremore effectiveinpatients withmoderateto severeHL.
(46)75.0 (46)41.1
Baysaletal., 2013 Turkey
JCraniofac Surg
Retrospective 69:30(OS), 39(OS+IT)
OS+IT X OS
DEX0.5mL 0.5,1,2,4 Therewasno differencebetween thegroups.
30(74.3) 39(77.4)
Gundoganetal., 2013
Turkey
Otolaringol HeadNeckSurg
Clinicaltrial, prospective, randomized
73:37 (IT+OS),36 (OS)
OS+IT×OS MET0.4mL 0.5,1,2,3 Combinationtherapy achievedbetter hearingthresholdand auditory
discrimination,and shouldbeconsidered asinitialtreatment.
(37)89.0 (36)61.1
whounderwentIT-DEX,andintwo(6.1%)of34patientsin thecontrolgroup.10
In2006,Dallanetal.soughttounderstandthereal effi-cacyoftranstympanicsteroidtherapyforSHLinpatientsin whomtraditionaltherapieshadfailed.Asolutionof methyl-prednisolone(MP)andsodiumbicarbonatewasadministered viatranstympanicinjectiontoeightpatients.Hearinglevel was evaluated before therapy and at days one, seven, and30. Hearing improvementwasobtained in 75%of the patients.8
In2010,Raymundoetal.evaluated14patientstreated withthreeintratympanicinjectionsofmethylprednisolone (IT-MP) after failing treatment with systemic steroids. Pre-treatmentandpost-treatmentaudiometricevaluations includingPTAatfrequenciesof0.5,1,and2kHz,andspeech receptionthresholds(SRT)wereanalyzed.Tenof14patients presentedwithhearingrecovery>20dBinPTAor20percent inSRT.5
In2010,Chenetal.evaluatedtheeffectivenessofIT-MP in36patients whofailedroutineoralsteroid therapyand twopatients witha contraindication tosystemic steroid, with a maximum of four injections. Hearing level, dizzi-ness,andtinnituswereevaluatedbeforethefirstprocedure and20daysafterthelastinjection.Thirteenof38patients (34.2%)showedanimprovementinhearinglevels.The aver-ageimprovement20daysaftertreatmentwas54dBinthe hearingthresholdsof0.125---8kHz.11
In 2010, She et al. investigated 26 patients in the studygroup(SG)whoreceivedmethylprednisolone(MP)for tendaysandtheconventionaltreatment, and23patients whoreceivedasecondconventionaltreatment(nosteroid) servedasthecomparisongroup(CG).ThePTAimprovement was20.2±15.6dBintheSG,and9.2±13.7dBintheCG.In theSG,hearingimprovementatlowfrequencieswasbetter thanthatathighfrequencies.Thedatasuggestedthatthe treatmentmaybemoreeffectivewhenadministeredatthe earlierstagesofSHLwhentheconventionaltreatmenthas failed.12
In 2011, Moon et al. investigatedthe therapeutic effi-cacyofIT-DEXasa salvagetreatmentin151 patientswho weretotallyunresponsivetwoweeksaftertreatment initi-ation.The 151refractorypatientsweredividedintothree groups:thosereceivingnofurthertreatment(controlgroup,
n=59), those receiving one more ten day cycle of oral steroids (systemic reapplication group, n=26), and those receivingIT-DEXtherapy(IT-DEXgroup,n=66).Overall hear-ingimprovementwasobservedintenof59patientsinthe controlgroup, in fourof 26 in the systemicreapplication group,andin32of66intheIT-DEXgroup.Analyzingby fre-quency,hearingofthelow andmidfrequencies wasmore significantlyimproved thanhigh frequencies in theIT-DEX group.13
In 2011, Lee et al. analyzed patients who were ran-domlyclassifiedintotwogroups: theIT-DEXgroup(n=21) receivedfoursequentialIT-DEXwithintwoweeksafter sys-temicsteroids,andthecontrolgroup(n=25)tookanymore medications.Hearing improvementwasdefinedasa10dB ormoredecreasein thePTAof thefourfrequencies(0.5, 1,2,and3kHz).Hearingimprovementwasobservedinten (47.6%)of21IT-DEXpatientsandinfour(16.0%)of25control patients.TheimprovementofthemeanPTAwas11.4dBin theIT-DEXgroupand1.7dBinthecontrolgroup.TheIT-DEX
group showedsignificanthearing improvementat low fre-quency(0.5Hz)comparedtothecontrolgroup.Thepatients with≥70dBinPTAbeforeIT-DEXshowedsignificanthearing improvement comparedto theother patients withbetter PTAs.6
In 2012, Barreto et al. analyzed the effectiveness of oralandintratympanicsteroidsfortinnituscontrolineight patients with SHL and severe disabling tinnitus. Hearing evaluationandapplicationoftheTinnitusHandicap Inven-toryandvisualanaloguescalewereperformedbeforeand aftertreatmentofsuddendeafnesswithoraland intratym-panic steroids. Two patients showed improvement in the hearing, but seven showed large improvements in their tinnitus, which was demonstrated by an improvement in the valuesof thedegrees of severityof tinnitus.Patients with SHL and severe disabling tinnitus who underwent intratympanicandoralcorticosteroidsshowed,inthisstudy, significantreductionand/orremissionoftinnitus.14
In2012,Wangetal.observedandcomparedtheefficacy ofIT-DEXforthetreatment55patientswithrefractorySHL. For21patients(theperfusiongroup),DEX(2.5mg/0.5mL) was perfused transtympanically through a round window catheter,usinganinfusionpumpforonehourtwiceadayfor sevendays,givingatotalamountof35.0mg.For23patients (the injection group), DEX (2.5mg/time) wasinjected by tympanicmembrane puncture atintervals of twodayson atotaloffouroccasions,givingatotalamountof10.0mg. For11patients (thedripgroup),DEX (2.5mg/0.5mL)was drippedviaaventilationtubeplacedbymyringotomy,once onthefirstdayandtwiceadayfortheremainingsixdays, givingatotalamountof 32.5mg.Thirty-twopatientswith refractorySHLwhorefusedtoundertakefurthertreatments were defined as the control group. Hearing results were evaluatedbasedonPTAinfourfrequencies(0.5,1,2,and 4kHz). The improvements in meanPTA for the perfusion, injection,anddripgroupswere9.0,8.6,and1.7dB, respec-tively.Hearingimprovementwassignificantlygreaterinthe perfusion and injection groups than in the control group (1.4dB). In the perfusion group, eight out of 21 patients (38.1%)hadaPTAimprovementof15---56dB(mean29.8dB); intheinjectiongroup,eightoutof23patients(34.8%)had aPTAimprovementof16---54dB(mean24.9dB);inthedrip group,oneof11patients(9.1%)hadaPTAimprovementof 26.0dB;inthecontrolgroup,threeoutof32patients(9.4%) hadaPTAimprovementof15---36dB(mean14.9dB).15
In2013,Chouetal.investigatedwhethernear-continual transtympanic steroid perfusion is more effective than intermittent intratympanic steroid injection as a salvage therapy forSHL in60patients. The pre-salvagepure tone threshold was65.4±13.5dB in the transtympanic steroid perfusion group. After the therapy,the hearing threshold wasimprovedbyanaverageof15.0±9.7dB,and53.3%of subjects hadimproved by 10dB or more. The speech dis-crimination score(SDS) wasimprovedfrom 12.6±7.0%to 54.4±6.4%. In the intratympanic steroid injection group, the pre-salvage pure tone threshold was 68.8±16.0dB. Afterthe therapy,thehearing thresholdwasimproved by an average of 10.7±9.8dB, and 43.3% of subjects had improvedby10dBormore.Thespeechdiscriminationscore wasimprovedfrom13.3±6.0%to46.4±12%.16
Intratympaniccorticosteroidforsuddenhearingloss 361
refractorySHL,especiallythosewhohavecontraindications tosystemicsteroidadministration.
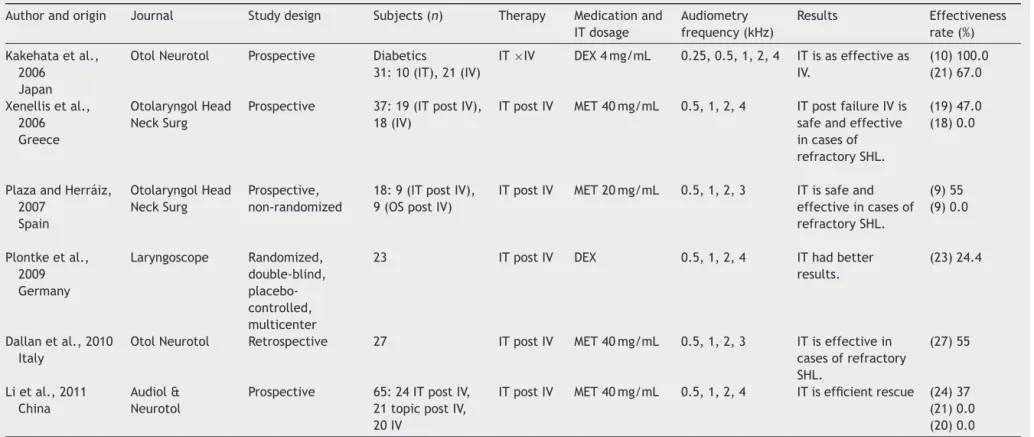
Salvagetherapyafterfailureofintravenous steroids
In2006,Xenellisetal.analyzed37patientswithSHLwho, attheendoftendaysoftherapywithintravenoussteroids asa firstline treatment, had fourfrequency PTA (0.5, 1, 2,and4kHz)andwererandomizedintotwogroups: treat-mentandcontrol.Nineteenpatientsofthetreatmentgroup received approximately0.5mL sterile aqueous suspension of MP in a concentration of 80mg/2mL by direct injec-tion. The procedure was carried out four times, and an audiogramwasperformedbeforeeachinjectionand approx-imately 1.5 months afterthe last session. Withregard to the19patientswhoreceivedintratympanictreatment(IT), in nine patients, the PTA threshold improved more than 10dB, in ten patients there was no change greater than 10dB, and no patients deteriorated more than 10dB. In thecontrolgroup,noneofthepatientsshowedanychange greaterthan10dB.Thedifferencewasstatistically signifi-cant.Thetreatmentgroupshowedanimprovementinmean PTAof14.9dB,whereasthecontrolgroupshoweda deteri-orationof0.8dB,andthisdifferencealsowasstatistically significant.17
In2006,Kakehataetal.evaluatedtheefficacyofIT-DEX treatmentonSHLpatientswithdiabetesbycomparingthe results withintravenousadministration ofdexamethasone (IV-DEX)treatment.IntheIT-DEXgroup(n=10,4mg/mLfor eightdays)theaveragehearinglevelbeforethetreatment was 79dB. Overall, all ten patients showed improvement ofmorethan10dBinthePTA,withameanimprovementof 41dB.Sevenpatients(70%)demonstratedsuccessfulresults, andfourrecoveredcompletely.IntheIV-DEXgroup(n=21, 8mg/dfortendays),14(67%)showedimprovementofmore than 10dB, with a mean improvement of 25dB. Thirty-threepatients(62%)demonstratedsuccessfulresults.IT-DEX treatmentisatleastaseffectiveasIV-DEXtreatmentforSHL patientswithdiabetes.18
In 2007, Plaza and Herráiz described their experience with 50 patients presenting with idiopathic SHL, treated intravenously over five days. After this period, patients with treatment failure (18 cases) were offered intratym-panicsteroidtreatment.Ninepatientsrefused,whereasthe otherninepatientsreceivedthreeweeklyinjectionsofMP. Recoveryofhearingwasreportedasimprovementofmore than15dBinPTA.Intratympanicsteroidtreatmentimproved hearinglossinfivepatients(55%).19
In 2009, Plontke et al.studied thesafety andefficacy of continuous IT-DEX in patients with SHL and insuf-ficient recovery (mean four PTA=97dB) after systemic high-dose glucocorticoid therapy, who received either IT-DEX(4mg/mL)orplacebo(NaCl0.9%)continuouslyapplied for14days.Intention-to-treatanalysisfortheprimary out-comecriterion(fourPTA:0.5,1,2,3kHz)duringtheplacebo controlledstudyperiod(14days)showedanaveragehearing improvementinthetreatmentgroupof13.9dBandinthe placebogroupof5.4dB.Ofthesecondaryoutcome param-eters,thelargestbenefitoflocalsalvagetherapywasfound formaximum speechdiscrimination,withan improvement
of24.4% inthetreatment and4.5% inthe placebogroup. Afterathree-monthfollow-upperiod,hearingimprovement inthetwogroupswasverysimilar.20
In 2010, Dallan et al. analyzed 27 patients unrespon-sivetotraditionalsystemictherapywhoweretreatedwith intratympanicsteroids.ThemeanPTAbeforeintratympanic treatmentwas79.9±21.4dB;atday30,afterlocalsteroid administration, the mean PTA was 60.6±24.9dB. Fifteen (55%)of27patientspresenteda‘‘useful’’improvementin thehearingstatus,toconfirmtheusefulness(atleast50%of patients)oflocalsteroidsadministrationincasesof refrac-torySHL.21
In2011,Lietal.followed65patientswithSHLwhodid notrespondtoIVtreatmentwithprednisolone,randomized intothreegroups:treatmentwithITsteroid,treatmentwith steroidineardrops,andacontrolgroup.The 24patients intheITgroupreceivedIT-MET, andthe21patientsinthe eardrop group received IT-METthat was directly dropped ontothetympanicmembranethroughtheearcanal.Inthe ITtreatmentgroup,audiogramresultsshowedthatthePTA forspeechfrequencies(0.5,1,2,and4kHz)was52.9dBat theendof systemictreatment, and64.8dBat theend of ITtreatment.TheimprovementintheITgroupwas signif-icantlybetterthanthatintheothertwogroups, with37% oftheITpatientsdemonstratingsignificantimprovementin theirhearing.22
ITsteroidadministrationafterfailedintravenoussteroids isasafeandeffectivetreatmentinsuddenhearingloss.
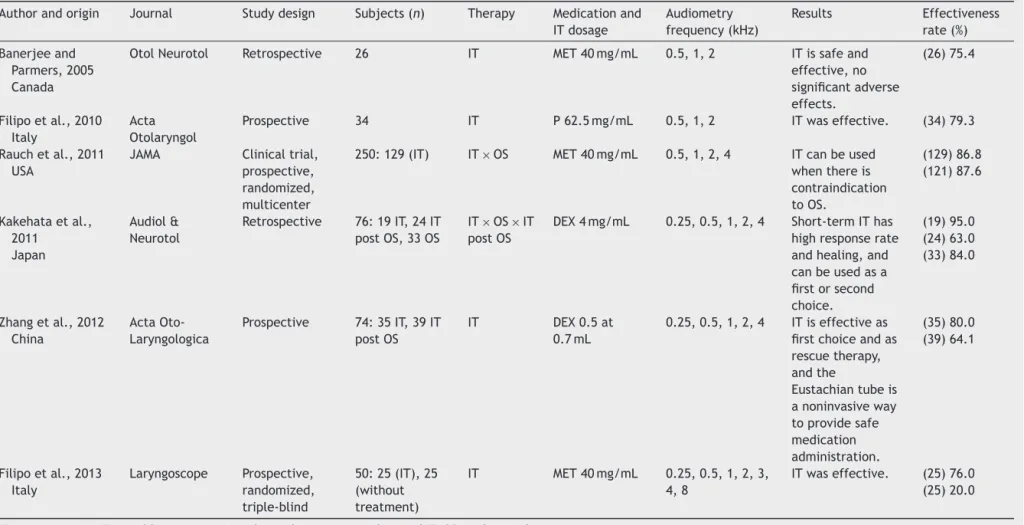
Primarytherapy
In2005,BanerjeeandParnersdeterminedwhether instilla-tionof intratympanicsteroids (methylprednisoloneand/or dexamethasone)iseffectiveinthetreatment ofSHL. Pre-treatment and post-treatment of 26 patients’ PTA and SDS were compared. Overall, there was a 27.2±5.7dB improvementinthepuretonethresholdsanda25.4%±6.2% improvementinSDS.23
In 2010, Filipo et al. evaluated the overall success rate, morbidity, and prognostic factors of a protocol of intratympanic steroid administration as a means of pri-mary therapy for SHL. 34 patients were treated once a day for three consecutive days with a single intratym-panic injection of prednisone diluted in saline solution. Amongthem,16patients(47%)reportedcompleterecovery, withaPTAthatreturnedwithin25dB;11patients(32.3%) showed improvement in hearing of more than 30dB, and fourpatientspresentedimprovementinPTAbetween10and 30dB.24
treatmentmethods.Thesefindingscouldbeobtainedafter analyzingtheaudiologicalresultsbypuretoneaudiometry, analyzingmeansinthefrequencies0.5Hz,1,2,and4kHz.4 In2011,Kakehataetal.evaluatedtheefficacyofdaily short-termIT-DEX treatment alonein 76 SHL patients for initialand/orsalvagetreatment.Theaveragehearinglevel wasdetermined by five frequencies (0.25, 0.5, 1, 2, and 4kHz).19outof76patientsfitthecriteriaforinitial treat-mentinthestudy(groupI),while24patients,whohadfailed systemictherapy,receivedsalvagetreatment(groupS).In groupI,18 of the19 patients(95%) showedimprovement of more than 10dB in the PTA, with a mean improve-mentof40dB.20patients(63%)recoveredcompletelyand 16patients(84%)demonstratedsuccessfulresults,withan improvementofmorethan30dB.IngroupS, 14ofthe24 patients(58%)showedimprovementof16dBandtwo(8%)of thesevenpatients(29%)withsuccessfulresultsrecovered completely. Daily short-term IT-DEX administration using LAM for SHL patients without concurrent therapy showed a high response rate and high cure rate, and proved to beanalternativetherapeuticoptiontohigh-dosesystemic steroidsasafirst-and/orsecond-linetreatment.7
In 2012, Zhang et al. investigated the effectiveness and safety of noninvasive IT-DEX perfusion through the Eustachiantube in 74 patients withSHL. 35 patientsmet the criteria for initial treatment in the study (Group I), while39patients,whohadfailedsystemictherapy,received salvagetreatment(GroupS). IT-DEXperfusionthroughthe Eustachiantubewasappliedfourtimesattwo-dayintervals. Puretone test andtympanometrywere performed before startingtreatment,and24handoneweekafterwards.With regardtothe74patientswhoreceivedIT,80.0%(28of35)of thepatientsinGroupIand64.1%(25of39)patientsinGroup Shadimprovementintheirhearingability.Noninvasive IT-DEXperfusionthroughthe Eustachiantube isan effective andsafetherapyincasesofSHL.25
In 2013, Filipo etal. investigated50 patients affected bymoderateSHL,involving allfrequenciesfrom250Hz to 8kHz(aflataudiogram).Patientswererandomizedintotwo groupsof 25 each.The firstgroup (intratympanicsteroid) underwent a daily intratympanic administration of pred-nisolone for three consecutive days. The second group (control)receivedadailyintratympanicinjectionofasaline solutionforthreeconsecutivedays.Audiometrictestswere performedatdaysevenafterthebeginningoftherapy(T1), and then 10 and 30 days after T1. The patients in both groupswhodidnot showacomplete recovery atT1were treated with oral prednisone at a tapering dose. In the intratympanicsteroidgroup,19outof25patientspresented complete recovery at T1 (76%), whereas in the control group,the number of patients whorecovered completely at T1 was five out of 25 (20%). The PTA recorded at T1 demonstratedastatisticallysignificantimprovementinthe hearingthresholdofthefirstgroupcomparedtothecontrol group.ThemeanPTArecordedafterthefirst-linetreatment (T1)demonstrated a significant therapeutic action of the short-durationintratympanic steroidtherapy onmoderate SHL,withaflataudiogramshape,comparedtothenatural courseof thediseaseandtheplacebo effectatthat time point.26
ITissafe,effective,withoutsignificantadverseeffects, andcanbeusedasafirstorsecondchoice.
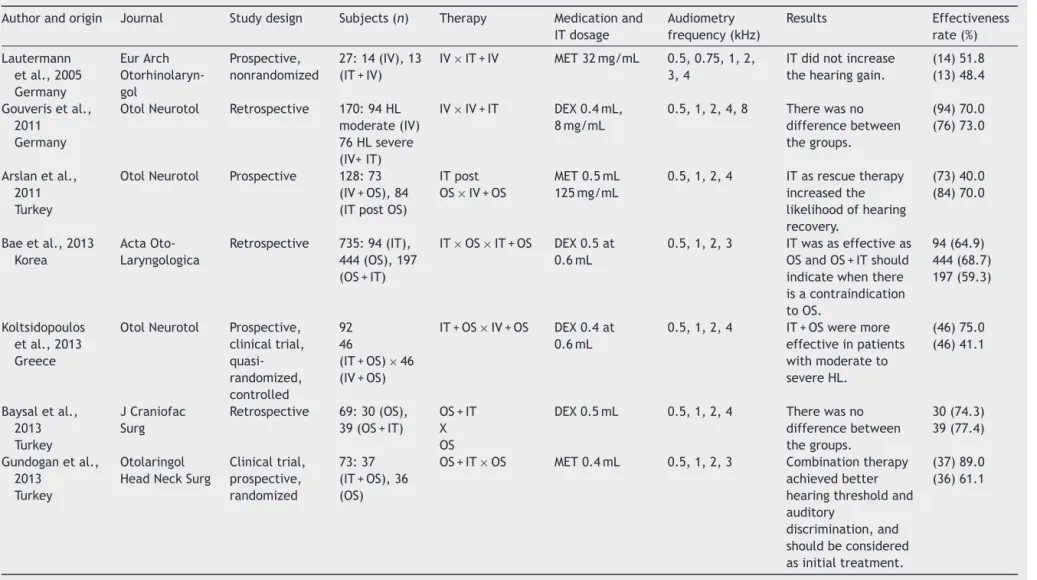
Combinationtherapy
In2005, Lautermannetal.analyzed 27patientswith pro-foundSHL.Fourteenweretreatedwitharheologicinfusion therapy consisting of systemicprednisolone, and 13 were treatedadditionallywithmethylprednisolone transtympan-ically throughaventilation tube. Inthe firstgroup,three patientshadgoodrecoveryofhearing.Anotherfivepatients hadapartialrecovery.Theaveragehearinggainfrom0.5, 0.75,1,2,3,and4kHzwas15dB.Inthegroupofpatients who were treated additionally with local corticoids, two reportedagoodrecovery ofhearingandanothertwoonly hadapartialrecovery.Theadditionaltranstympanic appli-cationofcorticoidsdidnotresultinasignificantlyimproved recovery ofhearingin comparisontothepatients treated withthestandardtherapyalone.
In 2011, Gouveris et al. evaluated the differences in effectiveness between SHL patients treated with intravenous therapy alone and patients treated with a combination of intravenous and intratympanic therapy. Ninety-fourpatientswithmoderateSHLweretreatedwith an intravenous steroid and vasoactive regimen, and 76 patientswithsevere SHLweretreatedwithacombination regimen of intravenous andintratympanic therapy. In the lattergroup,aseriesofthreeIT-DEXwereappliedeverytwo days.PTAat0.5,1,2,4,and8kHzwerecomparedbetween groups.ThecombinationtherapyinsevereSHLdidnotshow anystatisticallysignificantdifferenceineffectiveness com-paredtointravenoustherapyinmoderateSHL.Inpatients withsevereSHL,startingintratympanicsteroidtherapyas an adjunct early in the course of intravenoussteroid and vasoactive therapy improved hearing to a level which is obtainedinpatientswithlesssevere(moderate)SHLtreated withintravenoustherapyalone.27
In2011,Arslanetal.comparedhearingresultsinSHLin 158patientstreatedwithsystemicsteroidsalone,or com-binedintratympanicandsteroids.Seventy-threepatientsin the systemictherapy groupreceivedconsecutive adminis-trationof100mgintravenousmethylprednisoloneinthefirst day,then80mg/dayoralprednisoloneinthreedivideddoses forthenexttwodays,andcontinuedwithoral administra-tion of steroids by tapering the dose 20mg in every two days.Eighty-fivepatientsinthecombinedtreatmentgroup receivedintratympanicinjectionofmethylprednisolone(an approximatedoseof 0.5mLat125mg/mL).Atotaloffive injectionsonalternatedayswereperformed.Themeanand medianPTAgains ofsystemiccorticosteroidtherapy (SCT) group were 7.5 and 5dB at fifth day, 12.1 and 7.5dB at tenthday,and13.0and8.8dBat 15thday. Themeanand medianPTAgainsforcombinedtreatment(CT)groupwere 12.5 and 7.5dB, 17.8 and 13.8dB, and 21.8 and 20.0dB, respectively.BoththemeanandthemedianPTAgainswere significantlydifferentbetweentheSCTandCTgroups,and addingintratympanicmethylprednisolonetosystemic ther-apyincreasedtheprobabilityofhearingrecoveryinpatients withSHL.28
Intratympaniccorticosteroidforsuddenhearingloss 363
groupand87.49dBintheITsteroidgroup.Thedifferencein theinitialPTAresultswassignificantbetweentheSSgroup andITsteroidgroup.ThepuretonegainintheSSgroupwas 20.97dB,andthatofthegrouptreatedwithbothsystemic andITsteroidswas19.36dB.InSHL,theadministrationof ITsteroids inconjunctionwithSStherapyappearstohave thesameeffectontherestorationofhearingastheeffect obtainedusingSStherapyalone.29
In 2013, Gundogan et al. compared the efficacy of SS alone and combined with IT-MET in the treatment of 73 patients. The patients were randomly divided into two groups according to treatment: group A (n=37) received combination therapy (intratympanic methylprednisolone andoralsteroid)andgroupB(n=36)receivedoral steroid alone.Group Ademonstrated significanthearing improve-mentandSDScomparedwiththeuseofSSalone.Inhearing outcomesinpatientswithseverehearingloss,combination therapy showed statistically significant hearing improve-ment compared withoral steroidalone, and combination therapycanbeconsideredasaninitialtreatment,especially forpatientswithseverehearingloss.30
In2013,Koltsidopoulosetal.investigatedthe therapeu-ticefficacyofIT-DEXcombinedwithsystemicprednisolone in92patientsallocatedintotwogroups.Thecontrolgroup wastreatedwithsystemicprednisolonealoneandpatients inthecombinedtreatmentgroupreceivedthreeadditional IT-DEXinjectionswithinfivedays.Themainoutcome meas-ures used were the differences between pre-treatment andpost-treatmentPTAandSDS.Successfultreatmentwas defined as a greater than 10dB improvement in PTA and 15%inSDS.Audiometricevaluationwasperformedregularly every other day during admission, and subsequently once a month after the discharge. The final assessment of the patientsinbothgroups wasperformedthreemonthsafter thecompletionoftreatment.31
In2013,Baeetal.comparedthetherapeuticefficacyof intratympanicsteroidtherapy(IT-S)andcombinedtherapy withSStherapyandIT-Sin735patients.Thepatientswere dividedintothreegroups: 94intheIT-Sgroup,444in the SStherapy group,and197 inthecombinedtherapy group (SSplusIT-S).Hearingwasevaluatedby PTAbeforeinitial treatmentandatfourweeksfollowingthefinaltreatment.A decreaseofmorethan10dBinaverageairconduction hear-ingthresholdat0.5,1,2,and3kHzwasdefinedasimproved hearing.Nodifferenceinthelevelofhearinggainorratioof hearingimprovementwasobservedamongthethreegroups. IT-S was as effective as SS therapy or combined therapy and could be considered a first-line therapeutic modality forSHL.Duetoitsknownsafetyandefficacy,IT-Sshouldbe particularlysuitableforpatientswithSHLwhohavechronic diseasessuchasdiabetesmellitus,hypertension,orchronic renalfailure.32
Somestudieshaveshownbenefitsincombinedtherapy, especiallyforpatientswithmoderatetoseverehearingloss, whileothersfoundnodifference.
Conclusion
Intratympaniccorticosteroidtherapyisprescribedprimarily whenthereisfailureofconventionaltherapyorwhenuseof systemiccorticosteroidsislimited,suchindiabeticpatients.
Based on these results, there is still need for more prospectivestudieswithcontrolgroupsandstandardization oftreatmentforcomparisonofthedataobtainedand appli-cability of the proposed therapy, as well as audiological follow-upthroughacousticandelectrophysiological meth-ods.
Intratympanic corticosteroidtherapy is indicated espe-ciallywhenthereisfailureofconventionaltherapyandwhen theuseofsystemiccorticosteroidsshouldbeavoided.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.BenjaminES,CharlotteA, DorianOH,LuxonLM.Sudden sen-sorineuralhearingloss.Lancet.2010;375:1203---11.
2.Maia RA, Cahali S. Surdez súbita. Braz J Otorhinolaryngol. 2004;70:238---48.
3.PenidoNO,RamosHVL,BarrosFA,CruzOLM,ToledoRN. Clin-icalandetiologicalfactorsandevolutionofhearinginsudden deafness.BrazJOtorhinolaryngol.2005;71:633---8.
4.RauchSD,HalpinCF,AntoniellePJ,BabuS,CareyJP,GantzBJ, etal.Oralvsintratympaniccorticosteroidtherapyforidiopathic suddensensorineuralhearingloss.JAMA.2011;305:2071---9. 5.RaymundoIT,BahmadF Jr,BarrosFilho J,PinheiroTG, Maia
NA,OliveiraCA.Intratympanicmethylprednisoloneasrescue therapyinsuddensensorineuralhearingloss.BrazJ Otorhino-laryngol.2010;76:499---509.
6.Lee JB, Choi SJ, Park K, Park HY, Choo OS, Choung YH. Theefficiencyofintratympanicdexamethasoneinjectionasa sequentialtreatmentafterinitialsystemicsteroidtherapyfor suddensensorineuralhearingloss.EurArchOtorhinolaryngol. 2011;268:833---9.
7.Kakehata S, Sasaki A, Futai K, Kitani R, Shinkawa H. Daily short-term intratympanicdexamethasonetreatmentaloneas aninitialorsalvagetreatmentforidiopathicsudden sensorineu-ralhearingloss.AudiolNeurootol.2011;16:191---7.
8.DallanI,BruschiniL,NacciA,BruschiniP,TrainoC,RogniniF, et al.Transtympanicsteroids asasalvage therapyinsudden hearingloss:preliminaryresults.ORLJOtorhinolaryngolRelat Spec.2006;68:247---52.
9.PlontkeS,LöwenheimH,PreyerS,LeinsP,DietzK,Koitschev A, etal.Outcomesresearchanalysisofcontinuous intratym-panicglucocorticoiddeliveryinpatientswithacutesevereto profoundhearingloss:basisforplanningrandomizedcontrolled trials.ActaOtolaryngol.2005;125:830---9.
10.ChoungYH,ParkK,ShinYR,ChoMJ.Intratympanic dexametha-soneinjectionforrefractorysuddensensorineuralhearingloss. Laryngoscope.2006;116:747---52.
11.ChenY,WenL,HuP,QiuJ,LuL,QiaoL.Endoscopic intratym-panicmethylprednisoloneinjectionfortreatmentofrefractory suddensensorineuralhearinglossandonecaseinpregnancy.J OtolaryngolHeadNeckSurg.2010;39:640---5.
12.She W, Dai Y, Du X, Yu C, Chen F, Wang J, et al. Hearing evaluationofintratympanicmethylprednisoloneperfusionfor refractorysuddensensorineuralhearingloss.OtolaryngolHead NeckSurg.2010;142:266---71.
15.Wang CT, Chou HW, FangKM, LaiMS, ChengPW. Treatment outcome of additional dextran to corticosteroid therapy on sudden deafness: propensity score-matched cohort analysis. OtolaryngolHeadNeckSurg.2012;147:1125---30.
16.Chou YF, Chen PR, Kuo IJ, Yu SH, Wen YH, Wu HP. Com-parison of intermittent intratympanic steroid injection and near-continual transtympanic steroid perfusion as salvage treatments for sudden sensorineural hearing loss. Laryngo-scope.2013;123:2264---9.
17.Xenellis J, Papadimitriou N, Nikolopoulos T, Maragoudakis P, SegasJ,TzagaroulakisA,etal.Intratympanicsteroidtreatment inidiopathicsuddensensorineuralhearingloss:acontrolstudy. OtolaryngolHeadNeckSurg.2006;134:940---5.
18.KakehataS,SasakiA,OjiK,FutaiK,OtaS,MakinaeK,etal. Comparisonofintratympanicand intravenousdexamethasone treatmentonsuddensensorineuralhearinglosswithdiabetes. OtolNeurotol.2006;27:604---8.
19.Plaza G, Herráiz C. Intratympanic steroids for treatment of sudden hearing loss after failure of intravenous therapy. OtolaryngolHeadNeckSurg.2007;137:74---8.
20.PlontkeSK,LöwenheimH,MertensJ,EngelC,MeisnerC, Weid-nerA,etal.Randomized,doubleblind,placebocontrolledtrial onthesafetyandefficacyofcontinuousintratympanic dexa-methasonedeliveredviaaroundwindowcatheterforsevere toprofoundsuddenidiopathicsensorineuralhearinglossafter failureofsystemictherapy.Laryngoscope.2009;119:359---69. 21.DallanI,DeVitoA,FattoriB,CasaniAP,PanicucciE,Berrettini
S,etal.Intratympanicmethylprednisoloneinrefractory sud-denhearingloss:a27-patientcaseserieswithunivariateand multivariateanalysis.OtolNeurotol.2010;31:25---30.
22.Li P,Zeng XL,Ye J,YangQT, Zhang GH, Li Y.Intratympanic methylprednisolone improves hearing function in refractory suddensensorineuralhearingloss:acontrolstudy.Audiol Neu-rootol.2011;16:198---202.
23.BanerjeeA,ParnesLS.Intratympaniccorticosteroidsfor sud-den idiopathic sensorineural hearing loss. Otol Neurotol. 2005;26:878---81.
24.FilipoR,CovelliE,BalsamoG,AttanasioG.Intratympanic pred-nisolonetherapyforsuddensensorineuralhearingloss:anew protocol.ActaOtolaryngol.2010;130:1209---13.
25.Zhang Q, Song H, Peng H, Yang X, Zhou J, Huang W. Noninvasiveintratympanicdexamethasonetreatmentfor sud-den sensorineural hearing loss. Acta Otolaryngol. 2012;132: 583---9.
26.FilipoR,AttanasioG,RussoFY,ViccaroM,ManciniP,CovelliE. Intratympanicsteroidtherapyinmoderatesuddenhearingloss: arandomized,triple-blind,placebo-controlledtrial. Laryngo-scope.2013;123:774---8.
27.GouverisH, Schuler-SchmidtW,Mewes T, MannW. Intratym-panic dexamethasone/hyaluronic acid mix as an adjunct to intravenoussteroidandvasoactivetreatmentinpatientswith severeidiopathicsuddensensorineuralhearingloss.Otol Neu-rotol.2011;32:756---60.
28.ArslanN,O˘guz H,Demirci M,S¸afakMA, ˙Islam A,Kaytez SK, et al. Combined intratympanic and systemic use of steroids foridiopathicsuddensensorineuralhearingloss.OtolNeurotol. 2011;32:393---7.
29.BaysalE,Tunc¸O,BaglamT,DurucuC,OzA,KaratasZA,etal. Systemicsteroidversuscombinedsystemicandintratympanic steroidtreatmentforsuddensensorineuralhearingloss.J Cran-iofacSurg.2013;24:432---4.
30.GundoganO,PinarE,ImreA,OzturkcanS,CokmezO,Yigiter AC. Therapeutic efficacy of the combination of intratym-panic methylprednisolone and oral steroid for idiopathic sudden deafness. Otolaryngol Head Neck Surg. 2013;149: 753---8.
31.Koltsidopoulos P, Bibas A, Sismanis A, Tzonou A, Seggas I. Intratympanicand systemicsteroids forsudden hearingloss. OtolNeurotol.2013;34:771---6.