MESTRADO ONCOLOGIA
Characterization of the genetic profile
of a consecutive series of papillary thyroid carcinomas
Elisabete Oliveira Teixeira
M
2
Elisabete Oliveira Teixeira
Characterization of the genetic profile of a consecutive series of
papillary thyroid carcinomas
Dissertação de Candidatura ao grau de Mestre em
Oncologia
– Especialização em Oncologia Molecular,
submetida ao Instituto de Ciências Biomédicas Abel
Salazar da Universidade do Porto.
Orientador
– Professora Doutora Ana Paula Soares Dias
Ferreira
Categoria
– Professora auxiliar.
Afiliação
– Faculdade de Medicina da Universidade do
Porto e coordenadora do grupo Cancer Signalling and
Metabolism do Instituto de Patologia e Imunologia
Molecular da Universidade do Porto/Instituto de
Investigação e Inovação em Saúde do Porto.
Co-orientador
– Professor Doutor Rui Manuel Ferreira
Henrique
Categoria
– Professor Catedrático
Afiliação
– Instituto de Ciências Biomédicas Abel
3
“Nothing in life is to be feared; it is only to be understood.”
4
Agradecimentos
Antes de tomar mais um passo nesta minha viagem, desejo expressar gratidão a todos aqueles que caminharam ao meu lado, guiando-me até esta meta com um sentimento de pura realização pessoal. Um sincero obrigada:
Aos coordenadores do Mestrado em Oncologia. Em particular, à Prof. Dra. Carmen Jerónimo e à Prof. Dra. Berta da Silva pela aceitação da minha candidatura, que me permitiu aprender e trabalhar ao lado de grandes profissionais da área da Saúde.
À minha orientadora, a Prof. Dra. Paula Soares, com quem foi um privilégio trabalhar, por me ter aceite como membro do grupo de investigação que lidera. Aprendi imensamente consigo a nível científico e cresci bastante a nível pessoal. Acrescento ainda que foi um privilégio trabalhar ao pé do Prof. Dr. Manuel Sobrinho-Simões, uma mente curiosa e uma personalidade marcante e inspiradora.
À Dra. Antónia Póvoa, e à Dra. Maria-Rosa Bella sem as quais a realização desta tese não seria possível.
A todos membros do grupo de investigação Cancer Signalling and Metabolism do i3S pelo seu companheirismo, entreajuda e amizade nesta jornada. Um agradecimento especial ao mestre Rui Batista por me ter ensinado e guiado ao longo de todo o projeto. Um agradecimento também aos mestres Ana Pestana, Cristina Sampaio e Tiago Gaspar e à Dra. Paula Boaventura por todo o apoio prestado. Quero ainda agradecer à Thalita Alves pela amizade e ajuda concedida neste projeto. Os meus dias não teriam tido uma visão tão positiva sem ti ao meu lado na bancada de trabalho.
A todos os amigos que se mantiveram ao meu lado. Um beijo especial para minha “irmã” Joana Resende, que nunca se cansa de rir e de chorar comigo.
À família, pais e irmão, por todo o apoio emocional e económico no prosseguimento da minha educação e crescimento pessoal.
Ao meu “esposo”, Carlos Moreira, a pessoa mais importante da minha vida e cuja inteligência, empenho e determinação me inspiram e impulsionam a prosseguir nesta jornada e a alcançar os meus sonhos independentemente dos inúmeros obstáculos que se atravessam no nosso caminho.
6
Index of Contents
Abbreviations ...14 Abstract ...16 Resumo ...18 Introduction……….……….201. The thyroid gland: embryogenesis, anatomy and function ...20
2. Thyroid cancer: epidemiology ...22
3. Thyroid cancer: etiology ...23
3.1 Incidental findings ...23
3.2 Radiation exposure ...24
3.3 Iodine intake ...24
3.4 Environmental pollutants ...25
3.5 Obesity ...25
4. Thyroid Cancer: Prognostic factors ...26
5. Thyroid Cancer: Neoplastic lesions; Histotypes (based on the WHO Classification, 2017)………28
5.1. Follicular thyroid adenomas: ...28
5.2. Thyroid Carcinomas: ...28
5.2.1 Papillary thyroid carcinoma:...29
a) Papillary microcarcinoma ...30
b) Follicular variant ...30
c) Non-invasive follicular thyroid neoplasm with papillary nuclear features ...30
d) Macrofollicular variant ...31
e) Tall cell variant ...31
f) Oncocytic variant ...31
g) Diffuse sclerotic variant ...31
h) Solid/Trabecular variant ...32
i) Warthin-like variant ...32
7
5.2.3 Poorly differentiated thyroid carcinoma (PDTC) ...33
5.2.4 Anaplastic thyroid carcinoma (ATC) ...33
5.2.5 Medullary thyroid carcinoma (MTC) ...33
6. Thyroid Cancer: Molecular Markers in Papillary thyroid carcinoma ...34
6.1 The MAPK signalling pathway ...35
6.1.1 BRAF mutations ...36
6.1.2 RAS mutations ...39
6.2 hTERT mutations ...40
Aims………..44
Materials and Methods ...46
1. Patient tissue samples ...46
2. Haematoxylin-eosin staining ...46
3. DNA extraction ...47
3.1. DNA extraction by the salting out method: ...47
3.2. DNA extraction by the Ultratrep Tissue DNA Kit ...48
4. DNA quantification and quality evaluation ...48
5. DNA integrity evaluation ...48
6. Molecular characterization of the tumors ...49
6.1 Multiplex polymerase chain reaction (Multiplex PCR) ...49
6.2 Polymerase chain reaction (PCR) ...49
6.3 Electrophoresis for PCR products evaluation ...50
6.4 PCR product purification ...50
6.5 Sanger sequencing ...51
6.6 Sanger Sequencing Products Purification and Precipitation ...51
7. Statistical analysis ...52
Results ...54
1. Protocol optimization ...54
1.1 DNA extraction optimization ...54
8
2. Database elaboration ...55
3. Series Description: ...55
3.1 Clinicopathologic characteristics and Clinical follow up ...55
3.2. Genetic alterations ...58
4. Effects of molecular alterations in tumor aggressiveness and patient outcome ...61
4.1 Relationship between BRAF mutation, clinicopathological features and clinical follow up ...61
4.2 Relationship between hTERT mutation, clinicopathological features and clinical follow up ...63
4.3 Relationship between hTERT and BRAF concomitant mutation with clinicopathological features and clinical follow up ...65
4.4 Relationship between RAS mutation, clinicopathological features and clinical follow up ...67
5. Clinicopathologic and clinical follow up characteristics in tumor aggressiveness, lymph node metastases, distant metastases, patient outcome and mortality. ...70
5.1 Clinicopathologic and clinical follow up characteristics in tumors with aggressive histological features...70
5.2 Clinicopathologic and clinical follow up characteristics in cases with lymph node metastases ...70
5.3 Clinicopathologic and clinical follow up characteristics in cases with distant metastases ...73
5.4 Clinicopathologic and clinical follow up characteristics in relation with patient outcome (disease recurrence, persistence and/or progression) ...75
5.5 Clinicopathologic and clinical follow up characteristics in PTC related death ...77
6. Predictive factors for lymph node metastases, distant metastases, patient outcome and death in papillary thyroid carcinoma by logistic regression analysis ...80
6.1 Clinicopathologic characteristics and molecular alteration effects on the development of lymph node metastases ...81
6.2 Clinicopathologic characteristics and molecular alterations effects on the development of distant metastases ...82
6.3 Clinicopathologic characteristics and molecular alterations effects on patient outcome ...83
9 6.4 Clinicopathologic characteristics and molecular alterations effects on PTC
related death ...84
Discussion ... 986
1. Evaluation of the clinicopathologic characteristics of the tumors ...86
2. Molecular profile of the tumors and association with clinicopathologic characteristics and patient outcome ...90
2.1 BRAF ...90
2.2 hTERT ...91
2.3 Concomitance of hTERT and BRAF/RAS mutations ...92
2.4 RAS mutations ...93
3. Molecular markers as diagnostic and prognostic tools ...95
Conclusions and future perspectives ...98
Bibliography ... 100
10
Index of Figures
Figure 1. Scheme of T3 and T4 synthesis, regulation and function ...21
Figure 2. Thyroid cancer incidence and mortality from 1992-2014 ...22
Figure 3. Distribution of thyroid cancer by age groups forming a "bell-like shape" ...23
Figure 4. The MAPK and related pathways in thyroid cancer ...36
Figure 5. Mutations in the MAPK signalling pathway result in constitutive activation ...37
Figure 6. RAS regulation between active and inactive state ...39
Figure 7. A) Schematic representation of telomeric DNA and the shelterin complex; B) Schematic representation of senescence and crisis………41
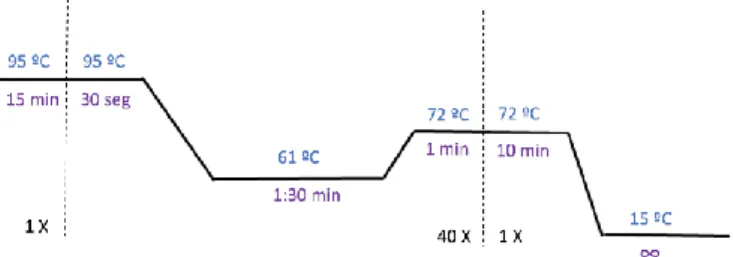
Figure 8. Thermocycler conditions applied in the multiplex PCR ...49
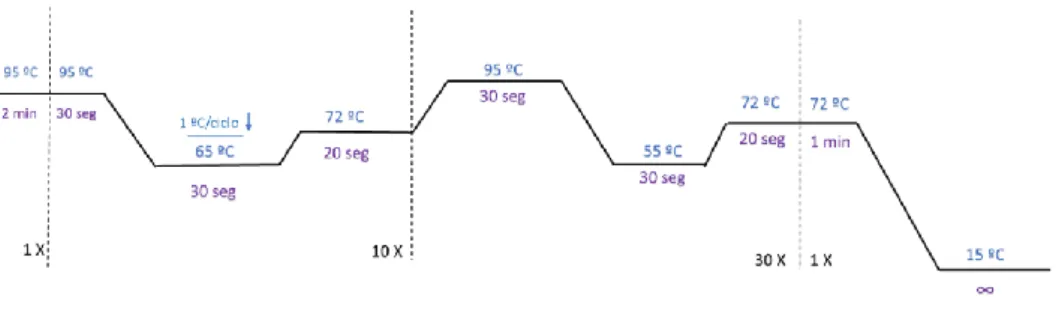
Figure 9. Thermocycler conditions applied in PCR of HRAS and KRAS genes by touchdown PCR ...50
Figure 10. Thermocycler conditions for the Sequencing reaction ...51
Figure 11. PCR Thermocycler conditions for TERT mutation validation ...52
Figure 12. PCR Thermocycler conditions for BRAF and NRAS mutations validation ...52
Figure 13. Representative electrophoresis of Quiagen multiplex PCR protocol results ....55
11
Index of Tables
Table 1 - Medium values of thyroid weight and size in adults ...20 Table 2 - Prognostic risk factors in thyroid cancer ...27 Table 3 - Primers Forward and Reverse utilized in the PCR reactions ...50 Table 4 - Number of studied lesions and distribution of the primary tumors accordingly to
the PTC variant ...55
Table 5 - Patient`s molecular status for all primary tumors and according to histologic PTC
variant ...59
Table 6 - Genetic alterations on analysed lymph node metastases ...60 Table 7 - Discordance between the molecular profiles of primary tumors and lymph node
metastases of 4 studied cases ...60
Table 8 - Univariate analysis of BRAF molecular status with clinicopathologic characteristics
and clinical follow up ...62
Table 9 - Univariate analysis of hTERT molecular status with clinicopathologic
characteristics and clinical follow up ...64
Table 10 - Univariate analysis of simultaneous hTERT and BRAF molecular alteration with
clinicopathologic characteristics and clinical follow up...66
Table 11 - Univariate analysis of RAS molecular status with clinicopathologic characteristics
and clinical follow up ...68
Table 12 - Univariate analysis for lymph node metastases with clinicopathologic
characteristics and clinical follow up ...71
Table 13 - Univariate analysis for distant metastases with clinicopathologic characteristics
and clinical follow up ...73
Table 14 - Univariate analysis for patient outcome during follow up with clinicopathologic
characteristics and clinical follow up ...76
Table 15 - Univariate analysis for death with clinicopathologic characteristics and clinical
follow up ...78
Table 16 - Clinicopathologic characteristics and molecular alterations effects on the
development of lymph node metastases ...82
Table 17 - Clinicopathologic characteristics and molecular alterations effects on patient
12
Index of Annexes
Supplementary table I – Patient`s age and gender and clinicopathologic characteristics of
all primary tumors according to histologic PTC variant. ... 108
Supplementary table II – Patient`s staging and treatment characteristics data according to histologic PTC variant of all primary tumors. ... 111
Supplementary table III – Distribution of all detected mutations for BRAF, hTERT and RAS genes according to histologic PTC variant ... 113
Supplementary tables IV, V and VI - Concomitant molecular alterations between the studied genes. ... 114
IV – hTERT and BRAF status ... 114
V – hTERT and KRAS status ... 114
VI – BRAF and RAS status ... 114
Supplementary table VII – Molecular profile of the primary tumors and the 18 tested lymph node metastases. ... 115
Supplementary tables VIII, IX and X – Univariate analysis for RAS status accordingly to clinicopathologic characteristics and clinical follow up. ... 116
VIII – Univariate analysis for NRAS ... 116
IX – Univariate analysis for HRAS ... 118
X – Univariate analysis for KRAS. ... 119
Supplementary table XI – Univariate analysis of tumors with aggressive histological features... 120
Supplementary table XII – Predictive factors of lymph node metastases ... 122
Supplementary table XIII – Predictive factors of distant metastases ... 123
Supplementary table XIV – Predictive factors of patient outcome ... 124
Supplementary table XV – Predictive factors for distant metastases using the model developed by Melo et al. (2014) ... 125
Supplementary table XVI – Predictive factors for PTC related death using the model developed by Melo et al. (2014) ... 125
Supplementary table XVII – Univariate analysis by binary logistic regression of the presence of calcification in PTC and association with TNM staging and molecular status ... 126
13
Supplementary table XVIII – Univariate analysis by binary logistic regression of the
presence of vascular invasion in PTC and association with clinicopathologic characteristics and molecular status ... 126
Supplementary figure I – Representative sanger sequencing chromatograph images of
WT BRAF and p.Val600Glu BRAF mutation. ... 127
Supplementary figure II – Representative sanger sequencing chromatograph images of
WT and Mutated -124 and -146 hTERT hotspots. ... 127
Supplementary figure III – Representative sanger sequencing chromatograph images of
NRAS codon 61 WT and p.Gln61Arg mutation. ... 128
Supplementary figure IV – Representative sanger sequencing chromatograph images of
HRAS codon 61 WT, p.Gln61Arg and p.Gln61Lys mutation. ... 128
Supplementary figure V – Representative sanger sequencing chromatograph images of
14
Abbreviations
AKAP9 - A-kinase anchoring protein 9 ALT - Alternative lengthening of
telomeres
ALK - Anaplastic lymphoma kinase ARAF - A-Raf proto-oncogene ATC - Anaplastic thyroid cancer BMI - Body mass index
BRAF - V-raf murine sarcoma viral
oncogenes homolog B1
cAMP - Cyclic adenosine
monophosphate
CCDC6 - Coiled-coil domain containing
6
CPT - Cancro papilar da tiroide CPTC - Conventional papillary thyroid
cancer
CT - Computed Tomography CTLA-4 - Cytotoxin T
lymphocyte-associated antigen-4
FFPE - Formalin-fixed,
paraffin-embedded
FNAB - Fine-needle aspiration biopsy FTA - Follicular thyroid adenoma FTC - Follicular thyroid cancer FVPTC - Follicular variant thyroid
cancer
GAPs - GTPase-activating proteins GDP - Guanosine-5'-diphosphate GEFs - Guanine nucleotide exchange
factors
Gs proteins - Guanine
nucleotide-binding proteins
GTP - Guanosine-5'-triphosphate HPF - High power fields
hTERT - Human telomerase reverse
transcriptase
LN - lymph node
MAPK - Mitogen-activated protein
kinase
MEK - Mitogen-activated protein kinase
kinase
MMPs - Metalloproteinases
MPTC - Macrofollicular papillary thyroid
carcinoma
MRI - Magnetic resonance imaging MTC - Medullary thyroid carcinoma NIFTP - Non-invasive follicular thyroid
neoplasm with papillary nuclear features
NIS – Sodium-iodine symporter NF-kB - Nuclear factor-kB
NCOA4 - Nuclear receptor coactivator
15
OPTC - Oncocytic variant of papillary
thyroid carcinoma
OR - Odds ratio OS - Overall survival
PCR - Polymerase chain reaction PET - Positron emission tomography PIK3CA - Phosphatidylinositol 3-Kinase PDTC - Poorly differentiated thyroid
cancer
POT1 - Protection of Telomere 1 PTC - Papillary thyroid cancer PTEN - Phosphatase and tensin
homolog
RAS - Rat sarcoma viral oncogenes
homolog
RAI – Radioactive iodine RAF-1 - Raf-1 proto-oncogene
RET - Rearranged during transfection RFS - Recurrence free survival RTK - Receptor tyrosine kinase SEER - Surveillance, Epidemiology,
and End Results Program
siRNA - Small interference ribonucleic
acid
SLC5A5 - Solute carrier family 5
member 5
SVPTC - Solid variant of papillary
thyroid carcinoma
T3 - Triiodothyronine T4 - Thyroxine TC - Thyroid cancer
TCPTC -Tall cell papillary thyroid
cancer
TCGA - The Cancer Genome Atlas TRF1 - Telomere Repeat Factor 1 TRF2 - Telomere Repeat Factor 2 TK - Tyrosine kinase
TSH - Thyrotropin
TREs - Thyroid response elements TRH - Thyrotropin-releasing hormone US - United States
VEGFA - Vase endothelial growth
factor A
WDTC - Well-differentiated thyroid
cancer
16
Abstract
Thyroid cancer is the most common endocrine malignancy worldwide and its incidence has been remarkably increasing over the last three decades, particularly in developed countries. There are several subtypes of thyroid cancer, yet, the great increase in incidence of thyroid cancer seems to be limited to the papillary thyroid carcinoma (PTC) subtype. Although this illness usually presents an excellent prognosis, with approximately 90% of survival rate at 10 years, some patients experience disease recurrence, persistence and progression, eventually dying from the disease. Hence, a need to understand why these patients with well-differentiated cancer experience poorer prognosis has emerged.
The current diagnostic tool for thyroid cancer is fine-needle aspiration biopsy (FNAB). Despite presenting high specificity, sensitivity is low and approximately 30% of the tumors are considered indeterminate. This requires FNAB repetition and quite frequently a diagnostic lobectomy that is usually unnecessary, since only a minority of the resected nodules are malignant. New and improved diagnostic and prognostic tools are needed to understand tumor behaviour, plan surgical approach and to predict whether these patients will respond to the standard therapy. Several proposals have been made to use molecular markers as tools for diagnosis and prognosis in patients with PTC. Recent studies of
molecular markers evaluation in FNAB and FFPE (Formalin-fixed, paraffin-embedded)
tissues have demonstrated that several genes or gene panels may be of fundamental use for prognosis determination of PTC and in the individual patient management.
Initiation and progression of thyroid cancer has been consistently associated with genetic and epigenetic events. The role of several molecular markers such as BRAF and RAS point mutations has been studied in thyroid cancer. Particularly, BRAF mutation has been proposed to be associated with worse prognosis. During treatment, some patients develop resistance to standard radioiodine (RAI) therapy. Tyrosine kinase inhibitors, such as vemurafenib, dabrafenib and sorafenib have been successfully applied in patients with RAI resistant tumors. However, the use of BRAF as an independent prognostic factor is not consensual in the scientific community and not all patients respond to these treatments. As for RAS point mutations, these have been associated either with worse or better prognosis in several studies. Therefore, controversy has rose on how these genes influence tumor behaviour. More recently, hTERT promoter mutations have also been a target of interest, being described to lead to tumor metastization and poorer prognosis.
The main aims of this study are to establish the status of BRAF, hTERT and RAS genes in a non-selected series of patients with papillary thyroid carcinoma in order to correlate the evaluated genes with tumour characteristics and patient outcome indicators.
17 We aim also to contribute to the development of a molecular panel of genes for improved patient risk stratification in PTC. To that end, clinicopathologic characteristics of a series of PTC patients were collected and the molecular profile was carefully evaluated. Univariate and multivariate analysis were performed to verify if and how mutational status contributed to the development of LN metastases, distant metastases, patient outcome and PTC related death.
We found that vascular invasion was the only predictive clinicopathologic factor for worse outcome. BRAF point mutations associated with aggressive tumor features, contrary to RAS point mutations that were related with better patient outcome on univariate analysis. Notably, we found hTERT promoter mutations to be a predictive factor for disease persistence, recurrence and progression, arising as a molecular marker of worse outcome in PTC patients. No additional tumor aggressiveness was observed when hTERT promoter mutations were concomitantly present with BRAF or RAS point mutations.
Keywords: Papillary thyroid carcinoma | Molecular markers | BRAF point mutation | RAS
18
Resumo
O cancro da tiroide é a neoplasia maligna endócrina mais comum no mundo e a sua incidência tem aumentado significativamente ao longo das últimas três décadas, particularmente em países desenvolvidos. Existem vários subtipos de cancro da tiroide, contudo, curiosamente o demarcado aumento na incidência de cancro da tiroide parece encontra-se limitado ao subtipo carcinoma papilar da tiroide (CPT). Apesar desta enfermidade usualmente apresentar um excelente prognóstico, com 90% de sobrevivência ao fim de 10 anos, alguns pacientes experienciam recorrência, persistência e progressão da doença, vários falecendo da mesma. Logo, a necessidade de compreender a razão pela qual estes pacientes com cancros bem diferenciados experienciam mau prognóstico emergiu.
A atual estratégia de diagnóstico de cancro da tiroide é a biópsia aspirativa por agulha fina. Apesar desta técnica apresentar alta especificidade, a sensibilidade da mesma é baixa e cerca de 30% dos tumores são considerados indeterminados. Isto requer repetição da biópsia aspirativa e, mais frequentemente, uma lobectomia de diagnóstico que geralmente é desnecessária, pois apenas uma minoria dos nódulos ressecados são malignos. Novas e aperfeiçoadas estratégias de diagnóstico e prognóstico são necessárias para compreender o comportamento tumoral, criar um plano cirúrgico e prever se o paciente irá responder à terapia standard. Várias propostas têm sido feitas para o uso de marcadores moleculares como estratégias de diagnóstico e prognóstico em pacientes com CPT. Estudos recentes realizados com marcadores moleculares em biópsias aspirativas e tecidos cirúrgicos fixados em formol e embebidos em parafina demostraram que vários genes ou painéis de genes podem ser uma estratégia fundamental para determinação de prognóstico em CPT e gestão individual de cada paciente.
A iniciação e progressão de cancro da tiroide têm sido consistentemente associadas a eventos genéticos e epigenéticos. O papel de vários marcadores moleculares, como mutações pontuais BRAF e RAS, tem sido estudado em cancro da tiroide. Particularmente, a mutação BRAF tem sido proposta como estando associada a pior prognóstico. Durante o tratamento, alguns pacientes desenvolvem resistência à terapia standard com iodo radioativo (RAI). Inibidores de tirosina cinase, como vemurafenib, dabrafenib e sorafenib têm tido sucesso no tratamento de pacientes com tumores resistentes à terapia com iodo. Contudo, o uso do BRAF como um fator prognóstico independente não é consensual na comunidade científica e nem todos os pacientes respondem a estes tratamentos. Quanto a mutações pontuais RAS, estas têm sido associadas tanto a pior como a melhor prognóstico em diversos estudos. Desta forma, controvérsia na forma como estes genes influenciam o comportamento tumoral surgiu. Mais recentemente, mutações no promotor
19 da hTERT têm sido alvo de interesse, sendo descritas como impulsionando a metastização tumoral e contribuindo para um pior prognóstico.
Os principais objetivos deste estudo são determinar o estado mutacional dos genes BRAF, hTERT e RAS numa série não selecionada de CPT de forma a correlacionar os genes avaliados com características tumorais e indicadores de prognóstico. Pretendemos ainda contribuir para o desenvolvimento de um painel de genes para melhoramento da estratificação de risco em CPT. Para este fim, as características clinico-patológicas de uma série de pacientes com CPT foram recolhidas e o perfil molecular cuidadosamente avaliado. Análises univariadas e multivariadas foram realizadas para verificar se, e como, o estado mutacional contribui para o desenvolvimento de metástases de LN, metástases à distância, evolução clínica do paciente e morte relacionada com a doença.
Verificou-se que a invasão vascular foi o único fator clinico-patológico preditivo para pior evolução clínica do paciente. Mutações pontuais BRAF associaram-se com características tumorais agressivas, contrariamente às mutações pontuais RAS, que se relacionaram com melhor evolução clínica do paciente em análise univariada. Notoriamente, encontramos as mutações no promotor da hTERT como um fator preditivo para persistência, recorrência e progressão da doença, emergindo como um marcador molecular para pior evolução clínica em pacientes com CPT. Não foi observada maior agressividade tumoral quando mutações no promotor da hTERT se encontravam concomitantemente presentes com mutações pontuais BRAF ou RAS.
Palavras-chave: Carcinoma papilar da tiroide | Marcadores Moleculares | Mutação
20
Introduction
1. The thyroid gland: embryogenesis, anatomy and function
The thyroid`s name arose from the Greek thyreoeidos (thyreos – shield, eidos – from), given its shape, which is also frequently referred as a “butterfly shape”. The thyroid gland is the first human endocrine organ to appear during embryogenesis, starting its formation by the 3rd week of gestation. The primary form of the organ originates from the
neural crest (a pool of multipotent cells) and the primitive pharynx. Embryogenesis begins with the proliferation of endodermal epithelial cells that form a diverticulum in the pharyngeal floor. Several morphological changes such as enlargement, bifurcation and lobulation occur during the following weeks of gestation, until a detachment of the organ from the first site takes place at the 7th week. The diverticulum descends to the final position at cervical spine
height, anterior to the larynx, and continues its development until the 11th week of pregnancy
[1, 2]. One of the most important functions of the thyroid is its role in the development of the brain in fetuses and newborns [3]. Even though thyroid organogenesis finishes in the 11th
week of pregnancy, fetuses receive hormones from their mother until the 16th week of
gestation, which are critical for their development. After that time, they are also able to produce thyroidal hormones to continue their growth [4]. Furthermore, thyroid hormones are fundamental for the continual development of the brain in adults, having a great impact on mood and neurocognition [5].
This gland is constituted by two elongated lateral lobes (with superior and inferior poles) connected by a thin isthmus. Fibrous septae divide this organ into follicles with cuboidal to low columnar epithelium. The medium values of thyroid weight and size are represented in Table 1, although it is rather important to note that these measures vary in each individual [2, 3].
Table 1 – Medium values of thyroid weight and size in adults [2]. Thyroid weight and size (medium values)
Weight 15-25 g Length of the lobes 40 mm
Width 15-20 mm Thickness 20-39 mm
Histologically, the thyroid is composed by two cellular types: follicular cells and parafollicular cells (also denominated C cells) [6].
Monolayers of follicular cells form the thyroid follicles, which are organized structures that contain colloid. These structures, and particularly follicular cells, are responsible for the
21 synthesis and secretion of the thyroid hormones T3 and T4 (triiodothyronine and thyroxine, respectively) which are regulators of several body functions [7], such as: thermogenesis, body weight, cholesterol and triglyceride metabolism and carbohydrate metabolism [8]. TRH (thyrotropin-releasing hormone) produced in the hypothalamus interacts with the pituitary gland, which liberates TSH (thyrotropin) into circulation, showing a trophic effect. The binding of TSH with its seven-transmembrane receptor in the thyroid follicular epithelium leads to a conformational change in which this receptor associates with a Gs protein. This interaction results in an intracellular increase in cAMP levels, which culminates in T3 and T4 synthesis and release into the bloodstream. In the periphery, these hormones bind to thyroid hormone receptors (TR) to form a complex that migrates into the cellular nucleus and interacts with thyroid response elements (TREs). These, lead to the initiation of transcription on target genes (Figure 1) [3, 9]. Thyroid gland follicles also contain a population of C cells, which are responsible for the synthesis and secretion of calcitonin, a hormone that controls calcium levels in the skeletal system [3].
Figure 1. Scheme of T3 and T4 synthesis, regulation and function: High levels of T3 and T4 in circulation result in a negative feedback mechanism, which inhibits TRH and TSH production by the hypothalamus and the pituitary gland [3, 8].
Illnesses with thyroid origin include hyperthyroidism, which is characterized by an excessive synthesis of thyroid hormones as seen in Graves`s disease, for instance, or hypothyroidism, which results from hormone production deficiency as seen in Hashimoto`s thyroiditis. These conditions have different manifestations and may be associated with different clinical diseases other than the ones mentioned [3]. Nodular lesions (which will be
22 better described further in this study) are also a cause of illness and are very commonly found worldwide. Most nodular lesions are proven to be benign, still, 2-15 % are malignant and may present with a poor prognosis, and so, are in need to be studied [10, 11].
2. Thyroid cancer: epidemiology
Thyroid cancer is the most common endocrine malignancy worldwide, and its incidence has been remarkably increasing over the past three decades, particularly in developed countries [12, 13]. This pathology accounts for 2,1% of all diagnoses of cancer worldwide, showing a predominance in women, with and incidence 3-folds higher than in men [14]. According to SEER (Surveillance, Epidemiology, and End Results Program), even though thyroid cancer incidence is increasing in the United States (US), mortality has remained stable (Figure 2), with a 5 year-survival rate of 98.2% from 2007 to 2013. Thus, showing in general a very good prognosis. (https://seer.cancer.gov/statfacts/html/thyro.html; consulted in March 2018) [15].
Figure 2. Thyroid cancer incidence and mortality from 1992-2014. (Adapted from SEER, https://seer.cancer.gov/statfacts/html/thyro.html; consulted in March 2018).
In 2017, EUROCARE-5 performed a study involving 87 cancer registries of 29 European countries and determined a 5 year-survival rate of 88% in women and 81% in men [16]. Also, a study performed by Kilfoy et al. from 1973 to 2002 comparing registries from 19 populations in America, Asia, Europe and Oceania demonstrated a global increase in thyroid cancer, except for Spain, Sweden and Norway, where thyroid cancer incidence actually decreased, mostly for the female gender [17].
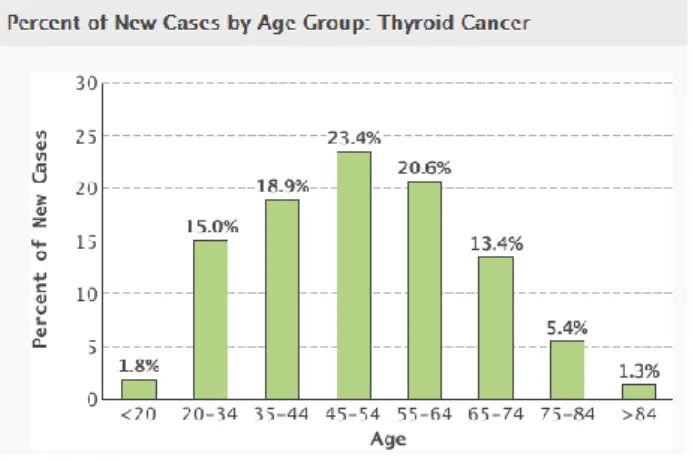
This pathology emerges in a wide range of ages, from young children to octogenarians [15]. Data from SEER from 2010 to 2014, show that age distribution at diagnosis forms a “bell-like” shape curve with highest incidence in the third, fourth and fifth decades of life, and a median age at diagnosis of 51 years of age. Notably, incidence at the second decade of life is also significantly high, showing a predominance of the incidence of
23 this cancer in younger groups (Figure 3) [18] (https://seer.cancer.gov/statfacts/html/thyro.html; consulted in March 2018).
Figure 3. Distribution of thyroid cancer by age groups forming a "bell-like shape". (Adapted from SEER, https://seer.cancer.gov/statfacts/html/thyro.html; consulted in March 2018).
In Portugal, thyroid cancer is the 3rd most frequent cancer among women [19].
According to the most recent national data from ROR-Centro (2014), the crude incidence rates were 22.6/100 000 women and 4.7/100 000 men, corresponding to 6.2 and 1.0% of all cases of cancer, respectively. This study revealed that between the years of 1989 and 2009, thyroid cancer incidence suffered an astonish increase of 8.7% in women and 8.8% in men from the northern region per year [19], and these numbers are expected to increase during the next decades. Therefore, suggesting that we are facing a need to understand thyroid cancer emergence and histologic and molecular characterization in order to prevent cancer and/or to treat it more efficiently.
3. Thyroid cancer: etiology
Clearly a higher number of thyroid tumours are being diagnosed, but whether this rise in incidence is only apparent, being due only to the development of new and improved imaging diagnostic methods, or if we are truly observing a true increase in the number of cases caused by specific carcinogens and lifestyle habits is still controversial. Yet, evidences indicate that more than just for overdiagnosis, a true incidence is also occurring [14, 15, 18].
3.1. Incidental findings
The upsurge in diagnosis has been indeed due to incidental findings. The growing use of imaging methods (ultrasound, computed tomography (CT), magnetic resonance imaging (MRI) or positron emission tomography (PET)) and fine-needle aspiration biopsy (FNAB) has led to the detection of numerous subclinical thyroid cancers. This imaging modalities have detected occult nodules in 10-68% of adults, being a large proportion of
24 these asymptomatic and non-palpable, thus clinically irrelevant [14]. Curiously, countries like Portugal [20], the US and Finland have reported high occult thyroid cancers detected upon autopsy, which creates a discussion in whether thyroid cancer must be treated, or not, and how [18, 21]. Yet, the overdiagnosis hypothesis has some shortcomings, since it does not explain why other types of cancer (breast, cervical, colorectal) with increased surveillance and large use of imaging modalities and biomarkers haven´t suffered abrupt increases in incidence like thyroid cancer, which leads to the belief that the cause must be thyroid specific [21]. It is important to note that the incidence increase in thyroid cancer seems to be limited to the papillary variant and most tumours are microcarcinomas (≤ 10 mm diameter), even though an increase was also observed in larger tumours. This way, for overdiagnosis to be the only explanation, it would be expected a more prominent decrease in the incidence of advanced stage and large thyroid carcinomas. As well, the increasing rates would be limited to small and localized tumours. Plus, all these incidental findings should result in a decline in thyroid cancer specific mortality, which was not observed since mortality rates seem to remain stable [14, 21].
3.2. Radiation exposure
Radiation exposure after Hiroshima and Nagasaki bombing during the World War II has been associated with thyroid cancer incidence among survivors, as has the Chernobyl accident in April of 1986 particularly in children [14, 22, 23]. Plus, there is evidence that exposure to low-dose radiation in children receiving treatment for other illnesses (such as hematologic malignancies) display an increased incidence in thyroid cancer. Studies show that the risk to develop thyroid cancer upon exposure to radiation is higher during childhood, decreasing during time. The papillary carcinoma subtype has shown to be the most frequent to emerge after exposure. Molecular alterations like RET/PTC rearrangements also seem to appear in radiation exposed tumours in higher frequency than in sporadic thyroid carcinomas [14, 18, 24, 25]. Yet, several studies showed that PTC with radiation induced mutations have declined over time, while PTC harbouring mutations non-induced by radiation have increased over time [14].
3.3. Iodine intake
Iodine is a required component for the proper synthesis of thyroid hormones. Iodine molecules are incorporated in tyrosine residues of thyroglobulin that then by oxidative reactions lead to the synthesis of T4 and T3 [26]. For adults, the recommended dietary allowance of iodine is of 150 mg/day. Yet overconsumption of iodine has been reported in several countries and associated with thyroid illness (Data from National Instituts of Health
25 Iodine intake has been hypothesized to be related to thyroid carcinogenesis. In patients with Hashimoto`s thyroiditis, for instance. This autoimmune disease is caused by a body response against thyroglobulin and thyroid peroxidase antigens, which results in inflammation, thyroid destruction and hypothyroidism. It is hypothesised that higher amounts of iodine intake can be incorporated in thyroglobulin and potentiate its antigenicity, leading to the production of proinflammatory cytokines and oxidative stress that might result in the development of cancer [3, 26, 27]. Likewise, favouring iodine intake in the diet, such as salt iodization, seems to have provoked a shift from the follicular carcinoma (which is favoured by iodine deficiency) to the papillary carcinoma [28]. This way, levels of iodine intake might, not only potentiate cancer development, but also influence cancer morphology [29, 30]. Animal studies, like the one performed by Yamashita et. al in 1990, found only the PTC variant of cancer in animal fed with an iodine-enriched diet [28, 31]. Yet, more studies are needed to make a true association [21, 32]. Curiously, in 2016, a study lead by Vuong
et al. in an iodine rich country (Japan) and an iodine deficient country (Vietnam), found no
genetic differences between these thyroid cancers, suggesting that iodine intake/deprivation might not affect thyroid cancer at a molecular level, when evaluating its influence in the emergence of BRAF and RAS point mutations and RET/PTC translocations [33].
3.4. Environmental pollutants
Environmental pollutants resulting from the industrialization have also been pointed has possible risk factors. The influence of several chemical compounds in the normal regulation of hypothalamic–pituitary–thyroid axis and in the detoxification system is still unclear. Some of these, such as pesticides and preservatives, may lead to a susceptibility to cancer development, either by resulting in deregulation of hypothalamic–pituitary–thyroid axis, in carcinogens by biochemical processing or increasing the effect of toxic agents [21, 32]. Plus, according to Malandrino et al. (2013), natural environmental factors may also be implicated in PTC development. Data from different volcanic regions show a higher propensity for habitants to develop thyroid cancer than habitants from a non-volcanic region. A risk which they attribute to the highly concentrated drinking water components, like heavy metals in areas such as Hawaii and Iceland [34].
3.5. Obesity
Recently, obesity has also been proposed to be associated with an increased risk of thyroid cancer development. In 2013, Kim et al. showed a direct influence of obesity in thyroid cancer emergence in ThrbPV/PVPte mice (which harbour a mutated thyroid hormone receptor-β and haplodeficiency of the PTEN gene, spontaneously developing thyroid cancer). They reported that obesity led to higher tumour aggressiveness and
26 anaplastic transformation [35]. In 2015, a metanalysis study lead by Schmid et al. showed a correlation between BMI (Body mass index) and thyroid cancer, revealing that overweight and obese patients presented a greater risk of thyroid cancer development. This study also found a predisposition of this patients to develop papillary, follicular and anaplastic carcinomas, while an inverse correlation was found with medullary thyroid cancer [14, 36].
Nevertheless, radiation exposure during childhood and adolescence is the only well established and documented risk factor for triggering thyroid carcinogenesis, so far. Other possible etiologic factors, as the ones previously mentioned in this section are not fully understood and are in need of further investigation.
4. Thyroid Cancer: Prognostic factors
There are several factors influencing thyroid cancer prognosis, those of which are related to the patient itself, the tumor and/or the course of treatment [15] (Table 2).
The patient`s age is an important prognostic factor. Previously, it was considered that patients older than 20 years old and younger than 45 years of age were the group that usually presented increased survival rates and lower recurrence rates [15, 18, 37, 38]. In 2016, the AJCC/TNM staging system for PTC has been updated to its 8th edition which was
then implemented in January 2018. One of the major alterations applied in the staging system was the raising of the age cut-off from 45 to 55 years of age. To validate this alteration, Kim et al. (2018) has performed a study with 505 PTC cases from the TCGA (The Cancer Genome Atlas) database. This study aimed to compare OS (overall survival) and RFS (recurrence-free survival) between the different age cut-off values (45 and 55 years). Their results validated the cut-off change that has been implemented, by showing stronger statistical differences on OS and RFS when adjusting patients age to the 55 years cut-off [38].
As previously mentioned, females have a 3-fold higher rate of thyroid cancer incidence than men, and this trend has remained stable over time [17], however some studies show a worse prognosis for males affected by thyroid cancer [39, 40].
Tumor related factors, such as histology, size (larger tumors show higher propensity to invade local tissues or to metastasize to distant organs than smaller tumors, which may result in survival decrease), invasiveness and molecular profile, will be discussed in detail in the following sections [15].
27 Table 2 - Prognostic risk factors in thyroid cancer [15]. Several prognostic factors have been related with thyroid cancer. Those of which are related to the patient itself, the tumor and/or the course of treatment. Studies are still being conducted in order to understand how tumor molecular status influences prognosis.
Standard thyroid cancer treatment is composed of surveillance and surgery (when indicated), which may be followed by RAI treatment when the tumor is iodine avid, which is verified in most tumors. Yet, some thyroid cancers either do not respond to RAI treatment or become resistant throughout the course of therapy [14]. These tumors tend to progress into higher stages of cancer, develop distant metastases and therefore resulting in low quality of life and decreased survival [37]. Studies have shown that tumor histology and genetic profiles, which will be better discussed during the next sections, are determinant to patient outcome and related to the avidity of the tumor to respond to therapy. Thus, being the genetic characterization of sundry types of tumors a main goal of many researchers [12, 41-44].
28
5. Thyroid Cancer: Neoplastic lesions; Histotypes (based on the WHO Classification, 2017 [6])
Clinically, thyroid cancer is a major concern on patients diagnosed with thyroid nodules. Fortunately, most nodules are localized, homogeneous and non-neoplastic, and a few are benign neoplasms. Actually, the ratio adenoma:carcinoma is accounted to be 10:1 [3]. Still, a small but significative percentage of thyroid cancer is highly aggressive and fatal, and given the high increase of incidence of this disease in the last decades, there is a need to continue the search for new and improved therapies and diagnosis methods. Before approaching the focus of this study, PTC, a brief presentation of other thyroid lesions, such as adenomas, and other forms of thyroid cancer will be discussed.
5.1. Follicular thyroid adenomas (FTA):
Follicular adenomas are well defined benign lesions, encapsulated, that can compress the adjacent thyroid parenchyma. These lesions have a clonal origin, deriving from follicular cells, and are present in 3-5% of adults (as estimated from autopsy series), affecting all age groups but being more commonly detected during the 5th and 6th decades
of life [6]. Most of these benign lesions arise sporadically and radiation exposure is known to be an important risk factor, once exposure during childhood increases the risk of FTA by 15 times [6]. Clinically, these lesions present as painless, solid, homogenous round or oval solitary masses. Within larger lesions, calcification, oedema, fibrosis and haemorrhage may be found [6]. Tumor cells assume a cuboidal or polygonal shape, with round and basal nuclei. Capsule integrity defines the nodule diagnosis as benign and it may present to be thin or thick. Little variation in the morphology of cells is observed in benign lesions and mitotic figures are expected to be rare. Yet, more than one pattern of growth may be seen, such as solid, trabecular or macrofollicular, for instance. Contrary to carcinomas, follicular adenomas do not recur or metastasize [3, 6, 43-47]. This way, standard care consists in conservative monitoring and thyroidectomy if the lesion becomes symptomatic [6, 43, 48].
5.2. Thyroid Carcinomas (TC):
Distinct genetic alterations and morphologic characteristics are related to each variant of thyroid cancer. This illness may arise from one of the two types of cells that compose the thyroid parenchyma: thyroid follicular cells and C cells (described in the first section). The most common subtypes rising from thyroid follicular cells are PTC and FTC (Follicular thyroid carcinoma) which are characterized as WDTC (well-differentiated thyroid cancer). PDTC (Poorly differentiated thyroid carcinoma) and ATC (Anaplastic thyroid carcinoma), are the more aggressive forms of carcinoma derived from follicular cells. MTC (Medullary thyroid carcinoma) arises from C cells transformation.
29
5.2.1 Papillary thyroid carcinoma (PTC):
Papillary carcinomas are the most frequent form of thyroid cancer around the world, accounting for nearly 85% of all thyroid carcinomas, and the main interest in this study given its high frequency and the continuously increasing incidence.
PTC is a malignant epithelial tumor of follicular differentiation that may arise from either lobe of the thyroid as well from the isthmus [6]. These tumors tend to be indolent and show excellent prognosis with survival rates above 90% at 10 years. Still, an approximate 30% risk of relapse or persistent disease is present [49]. The age spectrum of patients affected by this disease is wide, ranging more frequently from the ages of 25 to 50 years, being females affected more frequently than males (3:1), even though this tendency tends to decrease with increasing age [3, 6, 48, 50]. Morphologically, papillary carcinomas can be solitary lesions as well as multifocal. Encapsulation may exist, but usually lesions infiltrate the capsule and the surrounding parenchyma, leading to multifocality and LN metastases in 30 to 80% of the cases [51, 52]. Hoarseness and dysphagia are present in about 20% of the cases, indicating involvement of the laryngeal nerve [6, 48]. Yet, venous dissemination and distant metastases are unusual, accounting only to 5 to 7% of the cases. These lesions may appear anywhere in the gland, being normally white, firm, with poorly defined margins. They often contain calcification, and many are even cystic which brings difficulty in performing a diagnosis [3, 6, 50]. Notably, the diagnosis of conventional PTC (CPTC) is made based on the presence of well-formed papillae and the nuclear features of the neoplastic cells. Normally, the nuclei size and shape changes and presents disperse chromatin, being often designated as Orphan Annie eye nuclei given their almost empty appearance [6]. Products of dystrophic calcification (psammoma bodies) are also commonly found in PTC. When detected by FNAB these products are a strong pointer that we are facing a PTC, once they are not detected on FTC or MTC [3, 50]. Squamous metaplasia is also found in PTC, in up to 40% of the cases [6]. Fibrosis is common, particularly in advanced stages. PTC standard treatment usually consists of thyroidectomy, RAI therapy and novel drugs for resistant disease [43].
Papillary carcinomas can be divided into several subtypes or variants, several of which will now be described. Each variant presents specific growth patterns, cellular types and stromal changes. Plus, genetic variation is present [6]. The most common variants include papillary microcarcinoma, conventional PTC, follicular variant of PTC and tall cell variant. Yet, several uncommon variants have been described during the last few years, including oncocytic, diffuse sclerosing and solid variants [53]. It is important to account that the criteria used to classify PTC histotypes is not rigorously established, sometimes creating discordance in subtype classifications [53].
30
a) Papillary microcarcinoma
These tumors present a size smaller than 10 mm and show a good prognosis, given that more than 90% of patients are free of disease during follow-up. Given their small size, microcarcinomas are easily missed on gross examination. Incidence of these tumors upon autopsy is 5.6-35.6%, and they show to have an irregular, scar-like appearance. Microscopically, they are characterized by the typical nuclear alterations of PTC, psammoma bodies, fibrosis and sometimes well-formed papillae. Yet, despite small size and good prognosis, a minority may present aggressive behaviour [6].
b) Follicular variant
The Follicular variant of papillary thyroid carcinoma (FVPTC) comprises about 30% [54] of all PTCs, yet, the incidence of this variant continues changing. Over the last decades, the histological categorization of thyroid cancer has evolved. In 1988, the WHO recognized nuclear features to be more significant to diagnosis of thyroid cancer than the architectural organization of the tissue, which led to the recognition of follicular variants of papillary thyroid carcinoma. These were previously believed to be a branch of follicular adenomas or carcinomas [50]. The diagnosis of FVPTC is difficult and it took years before this variant was recognized as a distinct subtype of PTC. Histologically FVPTC shows the same nuclear features as PTC, but an exclusive or almost exclusive follicular growth pattern with follicles of variables sizes (with less than 5% of well-formed papillae) [6]. The colloid is usually hyper-eosinophilic or darker than in healthy follicles and multinucleated giant cells may be present [53]. Plus, this variant can too be divided into two subtypes: encapsulated with invasion and infiltrative [6] (which also represent different tumor behaviours). Encapsulated FVPTC shows a similar behaviour to follicular adenoma or carcinoma, rarely metastasizing to LN, and with high rates of RAS point mutations in detriment of BRAF point mutations, which are absent. On the other hand, infiltrative FVPTC presents higher rates of LN metastases, behaving more likely to classic PTC and showing high rates of BRAF point mutations and low rates of RAS point mutations, which implicates a more aggressive treatment [54-57].
c) Non-invasive follicular thyroid neoplasm with papillary nuclear features (NIFTP)
NIFTP is a “non-invasive lesion with a follicular growth pattern that presents nuclear characteristics of PTC” [6]. These tumors can be detected in any part of the thyroid, usually presenting as mobile nodules, painless and asymptomatic, and presenting a very low malignant potential. NIFTPs were previously classified either as non-invasive encapsulated FVPTC or as well-differentiated tumor of uncertain malignant potential. An algorithm was developed to better diagnose these entities. It was established that for a tumor to be diagnosed as NIFTP it should be encapsulated or at least well-circumscribed from the adjacent tissue, it should present follicular growth of pattern, nuclear features of PTC and
31 no signs of invasion. These are distinguished from CPTC by the lack of papillary structures and from FVPTC by the lack of invasion [6, 58].
d) Macrofollicular variant
The Macrofollicular variant of PTC is a rare variation of FVPTC that shows complete absence of papillae [59]. Diagnosis is made when more than 50% of each section presents follicles of diameter superior to 0.25 mm [60]. These lesions are usually encapsulated and indolent, being sometimes mistaken with benign nodules [59, 61].
e) Tall cell variant
The Tall cell variant (TCPTC) corresponds to 10% of the diagnosed PTCs. These tumors are composed by tall columnar cells (2-3 times as tall as they are wide) and abundant eosinophilic cytoplasm [6, 53]. These tend to be large tumors with more than 60 mm in size. A PTC is characterized as Tall cell variant when tall cells account for 30% or more of the carcinoma cells. Usually, this variant occurs in elderly patients, tending to be aggressive [6] and presenting a high mitotic rate. Vascular invasion and dissemination are commonly found. Invasion of the trachea may be detected, and it is frequently the cause of complications and mortality. Distant metastatic lesions are more regular than in conventional PTC, resulting in a lower survival rate (75% at 10 years follow up) [3, 6, 50, 53]. Notably, dedifferentiation of the Tall cell variant to anaplastic carcinoma has been described [62].
f) Oncocytic variant
The Oncocytic variant PTC (OPTC) is an extremely rare variant with papillary features. It is characterized by a subset of papillary tumours often encapsulated but invasive and with an oncocytic cell cytology [6, 53].
g) Diffuse sclerotic variant
The Diffuse sclerotic variant is an uncommon variant that appears in younger patients, more commonly in women between the 2nd and 3rd decades of life [6]. It appears
many times as bilateral goiter once usually both lobes are involved [53]. It is typically accompanied by diffuse enlargement of the thyroid gland, chronic lymphocytic thyroiditis and elevated serum antibodies that resemble Hashimoto thyroiditis. Dense sclerosis and high numbers of psammoma bodies are detected. Tumor nests are solid and metaplasia is usually present [6]. Capsule rupture and local and distant metastases are often encountered, showing a decreased disease free-survival [3, 50, 53].
32
h) Solid/Trabecular variant
The Solid variant of papillary carcinoma is diagnosed when solid, trabecular or nested growth represents all or at least half of the tumor mass. It is more common in paediatric tumors, being very frequent in patients with history of exposure to ionizing radiation [6]. This variant is usually seen in children after the Chernobyl nuclear accident [50], but it also represents 1-3% of all PTCs in adults, showing higher mortality rates than conventional PTC by being associated with lung metastases [6]. Vascular invasion and extrathyroidal extension are present in approximately 1:3 of the cases [50]. Notably, this variant shows the same growth pattern as PDTC. Yet, these should not be mistaken, once Solid variant PTC maintains the nuclear features of CPTC [6].
i) Warthin-like variant
The Warthin-like tumors are usually not encapsulated but circumscribed. Papillae cells tend to be eosinophilic and large. At the centre of the papillae, plentiful lymphocytic infiltrate is found, resembling Hashimoto´s thyroiditis, which causes sometimes the tumor to be overlooked. Some tumors are cystic at the centre of the lesion [6]. This tumor pattern is maintained at LN metastases. The diagnosis is usually made accordingly to the nuclear features of PTC [53]. Prognosis is similar to that of a conventional PTC of the same size and stage [6].
5.2.2 Follicular thyroid carcinoma (FTC)
Follicular carcinomas are malignant epithelial tumors showing follicular cell differentiation and lacking the diagnostic nuclear features of PTC. Usually, these lesions appear as painless neck masses of multiple sizes and several times, the first symptom results from metastases (bone, lung) [6]. FTC varies in appearance, from non-encapsulated lesions to encapsulated lesions similar to follicular adenomas [6, 48, 57]. Whenever a break (invasion) in the capsule is observed microscopically, the nodule is characterized as a follicular carcinoma. When encapsulated, FTC may be hard to distinguish from follicular adenoma, only that the capsule on FTC tends to be thicker and more irregular [6]. FTC represents 10-15% of all thyroid cancers [43], being more frequent in women and showing a peak of incidence between 40-60 years of age [3]. These tumors seem to be more prevalent in areas with iodine deficiency [28]. FTC is found to be a solitary nodule, which can be well delimitated by a capsule or quite infiltrative, which are more aggressive forms with propensity for metastases through the blood stream and poor prognosis [6, 43]. When lymphatic involvement is present, the diagnosis of FVPTC should be appointed [6]. The presence of fibrosis and calcification may be found in these lesions. FTC treatment usually consists in thyroidectomy and RAI. Novel therapies are applied when resistance to therapy emerges [43].
33
5.2.3 Poorly differentiated thyroid carcinoma (PDTC)
PDTC accounts for 5-10% of all thyroid cancers [43]. It is characterized as a malignant neoplasm that shows little evidence of follicular cell differentiation, with an intermediate morphology between well-differentiated and anaplastic carcinomas [6]. Different diagnostic criteria have been employed, which resulted in discrepancies among clinicians. In 2006, a conference was held in Turin, Italy, to develop a uniform algorithm diagnostic approach for PDTC. It was established that PDTC should show a solid, trabecular or insular pattern of growth, without nuclear features of PTC and it should present at least one of the following characteristics: convoluted nuclei, mitotic activity of 3x10 HPF or higher and/or tumor necrosis [63]. The mean age of diagnosis is 55 to 63 years of age, being rare on young patients. Studies have shown that iodine deficiency may be a risk factor for triggering PDTC. This type of thyroid cancer may appear de novo or by dedifferentiation of well differentiated lesions, as a large solitary mass (medium size of 50 mm). PDTC is a highly invasive form, showing extrathyroidal extension in 60-70% of the cases, vascular invasion in 60-90%, regional LN metastases in 15-65% and distant metastases in 40-70% of the cases [6]. Macroscopically, these lesions appear as solid, brown to grey masses with signs of necrosis and may be partially encapsulated. Moreover, they present high grade microscopic features and overall poor prognosis. Colloid formation is minimal or absent. Marked pleomorphic and anaplastic cells are present, being small and uniform [6].
5.2.4 Anaplastic thyroid carcinoma (ATC)
ATC accounts for 2-3% of all thyroid cancers. These cancers may arise de novo or, more frequently from loss of differentiation from WDTC [43]. ATC is described as the most aggressive thyroid malignancy composed of undifferentiated follicular thyroid cells. ATC mortality rate is high, reaching more than 90% of the cases at 1 year, being that 30-40% of the patients already show distant metastases at presentation. Lesions are characterized as bulky and infiltrative with a tan colour and flesh-like features. Haemorrhage and necrosis are very commonly found. Cells show a high mitotic rate and infiltrative pattern of growth. Multinucleate giant cells and inflammatory infiltrate are also common in this variant [6].
The standard care for both forms includes surgery, chemotherapy, radiotherapy and the application of novel therapies like tyrosine kinase inhibitors. For ATC, palliative care is also required, due to its rapid and highly lethal behaviour [3, 42, 43].
5.2.5 Medullary thyroid carcinoma (MTC)
Parafollicular cells of the thyroid are calcitonin producers that under specific genetic alterations may give rise to MTC. MTC is a rare neuroendocrine neoplasm that accounts for approximately 2-3% of thyroid cancers. About 70% of MTCs arise sporadically, mostly
34 during the 5th and 6th decades of life, and are constituted by a solitary nodule. Cervical node
metastases are detected in 70% of the cases and distant metastases are found in 10% of the patients at presentation [6]. Microscopically, MTCs are composed by polygonal, round, plasmocytoid or spindle-shaped cells with eosinophilic to amphophilic cytoplasm. The nuclei are round with crumpled chromatin and small nucleoli [6]. Several anaplastic cells and amyloid deposits resultant from altered calcitonin metabolism may be found. [3, 43, 64]. Surgery, chemotherapy, radiotherapy and directed therapies such as vandetanib are part of the standard care [43]. Given that this cancer arises from different precursor cells and mechanisms than the one in study, it won´t be further discussed in this thesis.
6. Thyroid Cancer: Molecular Markers in Papillary thyroid carcinoma
During the last two decades, knowledge of genetic alterations present in thyroid cancer was swiftly acquainted. Novel insights on thyroid cancer mechanisms permitted an improved diagnosis of the illness. Plus, and quite importantly, the study of prognostic/molecular markers led to a more personalized and effective treatment of the patients. Ultrasound and FNAB are the most accurate and frequent methods of diagnosis of thyroid cancer in use presently. Still, in approximately 1/4 of the cases the physicians cannot reach a conclusive diagnosis or predict how some tumors will behave or respond to therapy. Additionally, the vast majority of thyroid nodules removed by surgery are benign, therefore, novel diagnostic and prognostic tools are required to better treat the cancer and also to avoid unnecessary treatments and surgeries [12]. Given the scope of the study, the molecular characterization of this thyroid cancer variant will be emphasized in this section.
Thyroid cancer initiation and progression have been related to the progressive accumulation of several genetic and epigenetic events that lead to the constitute activation of cellular signalling pathways, such as MAPK, PI3K-AKT, NF-kB and WNT-β-catenin signalling pathways. The genes affected in these pathways either code for cellular membrane receptors or intracellular signal transducers. Point mutations, gene amplification, chromosomal rearrangements and aberrant gene methylation seem to be the mechanisms behind these pathogenic molecular alterations [6, 12, 13, 43]. In 2014, TCGA published the results of a 496 PTC series, characterizing this subtype of cancer in a molecular fashion. Their results largely reduced the proportion of cases without an established oncogenic driver, allowing PTC to be divided into different subgroups according to their genetic print [13, 65]. Thus, demonstrating how the knowledge of PTC molecular characteristics is fundamental for risk stratification and prognosis.
35
6.1 The MAPK signalling pathway
The Mitogen-activated protein kinase (MAPK) pathway involves interconnected cascades of proteins that have a fundamental role in cellular maintenance, proliferation, senescence and survival. These mechanisms are highly conserved in all eukaryotes [66]. The best described cascade of this pathway is the ERK pathway, also known as the RAS-RAF-MEK-ERK pathway (Figure 4). The MAPK pathway acts through signal transducers between the extracellular and intracellular environment of the cell. Hormones, cytokines and growth factors interact with cellular receptors, leading to conformational changes that result in RAS activation. RAS proteins then recruit RAF proteins that migrate to the cellular membrane, being activated. RAF activates MEK proteins, which then interact with ERK, that migrates into the nucleus of the cell and regulates several cellular processes [12, 43, 66-68]. Studies revealed that about 30% of all cancers are mutated for proteins in this signalling pathway. So, the role of this pathway in cell survival and proliferation has been well studied during the last decades, as well as the importance of this cascade in thyroid tumorigenesis, particularly in PTC. Zheming et. al. (2017), characterized a PTC series by next generation sequencing, revealing that about 70% of the PTC cases possessed genetic alterations that resulted in the constitutive activation of the MAPK pathway [13, 65].
In PTC, activating point mutations (such as in BRAF and RAS) are commonly detected (75% of the cases). Gene fusions (15% of the cases), like RET/PTC translocations and the recently described ALK mutations are also drivers of tumorigenesis. Copy number variations account for 7% of the cases [6]. Mutations in the MAPK signalling pathway are usually mutually exclusive. Curiously, the rate of chromosomal rearrangements found on PTC, which are related to radiation exposure (ex: RET/PTC translocation) has decreased during the last years. Yet, a remarking upsurge in point mutations has been noted [12]. The RET/PTC translocation is the most common chromosomal rearrangement found on PTC, being present in 10-20% of the sporadic cases. The RET proto-oncogene codes for a cellular membrane receptor tyrosine kinase (RTK). RET chimeric genes retain RET TK domain active binding to active promoter regions of other genes, resulting in the expression of an active RET TK domain in the cytoplasm (independent of external signalling). There are over 10 described RET/PTC translocations known to be pathogenic in thyroid cancer, being the isoforms RET/PTC1 and RET/PTC3 the most frequent, where RET binds to CCDC6 and NCOA4, respectively. Even though these alterations are found in FVPTC and mostly in CPTC [6, 12, 43, 66], its presence was also described in cases of Hashimoto thyroiditis and in FTA [43, 69].
36 Figure 4. The MAPK and related pathways in thyroid cancer. The classic MAPK signalling pathway is represented inside the red dotted box. (Adapted from Xing, Nature Reviews, 2013 [43], after permission request). When the ligand (ex. growth factor) binds to the RTK, the receptor forms a dimer leading to the activation of the RAS protein. The activated RAS leads to the activation of the BRAF protein that interacts with MEK. Then ERK is activated by phosphorylation by MEK, being able to enter the nucleus of the cell and to regulated gene expression and synthesis of several proteins (MET, VEGFA, NF-kB, MMPs) [7, 33, 49, 50].
6.1.1 BRAF mutations
RAF are highly conserved serine-threonine kinase proteins which emerge in 3 differently regulated isoforms (ARAF, RAF-1 and BRAF). BRAF (v-raf murine sarcoma viral oncogenes homolog B1) isoform has the highest basal activity and needs less phosphorylation to become active, being the most potent activator of the MAPK pathway [66]. BRAF is a protooncogene located at 7q34 that is very commonly found actively mutated in several cancers, either by point mutations, chromosomal rearrangements, such as the AKAP9/BRAF translocation, or in frame deletions or insertions. Thus, leading to loss of control of the cellular metabolism and potentiating the emergence of malignancy [12].
Point mutations are the most common mechanism of constitutive activation of BRAF, being that the BRAF V600E point mutation (p.Val600Glu) in exon 15 is the most frequently
![Table 1 – Medium values of thyroid weight and size in adults [2].](https://thumb-eu.123doks.com/thumbv2/123dok_br/15147459.1012505/21.892.286.634.851.995/table-medium-values-thyroid-weight-size-adults.webp)
![Figure 1. Scheme of T3 and T4 synthesis, regulation and function: High levels of T3 and T4 in circulation result in a negative feedback mechanism, which inhibits TRH and TSH production by the hypothalamus and the pituitary gland [3, 8]](https://thumb-eu.123doks.com/thumbv2/123dok_br/15147459.1012505/22.892.137.775.520.857/synthesis-regulation-function-circulation-mechanism-production-hypothalamus-pituitary.webp)