Revista
Portuguesa
de
Cardiologia
Portuguese
Journal
of
Cardiology
www.revportcardiol.org
ORIGINAL
ARTICLE
The
role
of
propranolol
in
the
treatment
of
infantile
hemangioma
Sérgio
Laranjo
∗,
Glória
Costa,
Filipa
Paramés,
Isabel
Freitas,
José
Diogo
Martins,
Conceic
¸ão
Trigo,
Fátima
F.
Pinto
Servic¸odeCardiologiaPediátrica,HospitaldeSantaMarta,CentroHospitalarLisboaCentral,EPE,Lisboa,Portugal
Received15April2013;accepted19October2013 Availableonline4June2014
KEYWORDS Infantile hemangioma; Propranolol
Abstract
Introduction:Infantilehemangioma(IH)isoneofthemostcommonchildhoodtumors.There arevariousmedicalorsurgicaltherapeuticoptions,allwithsuboptimalresults.Recently,the successful useofpropranololfor involutionofIH wasdescribed.We reporttheresultsofa single-centerexperiencewiththistherapeuticoption.
Objective: Toprospectivelyassesstheefficacyandsafetyofpropranololinchildrenwith infan-tilehemangioma.
Methods:WeperformedaprospectiveanalysisofclinicaldataofallpatientswithIHreferred to apediatriccardiologycenterfor baseline cardiovascularassessmentprior topropranolol therapy.Propranololwasgivenatastartingdoseof1mg/kg/dayandtitratedtoatargetdose of2---3mg/kg/dayaccordingtoclinicalresponse.Efficacywasassessedthrougha photograph-basedseverityscoringscale.Safetywasassessedbycollectingdataregardingsignificantside effects.
Results:Starting in2010, 30 patients (15 female) were referred for propranololtreatment ofIH,atamedianageofsixmonths (1---63months).Themeantargetpropranololdosewas 2.8mg/kg/day,withameandurationoftherapyof12months.Allpatientsexperienced signif-icantreductionofIHsizeandvolume.Therewerenosideeffects.
Conclusions: Inourexperiencepropranololappearstobeausefulandsafetreatmentoptionfor severeorcomplicatedIH,achievingarapidandsignificantreductionintheirsize.Noadverse effects were observed, although until larger clinical trials are completed, potential adverseeventsshouldbeborneinmindandconsultationwithlocalspecialistsisrecommended priortoinitiatingtreatment.
© 2013 SociedadePortuguesa de Cardiologia. Published by Elsevier España, S.L. All rights reserved.
∗Correspondingauthor.
E-mailaddress:[email protected](S.Laranjo).
http://dx.doi.org/10.1016/j.repc.2013.10.018
PALAVRAS-CHAVE Hemangiomainfantil; Propranolol
Opapeldopropranololnotratamentodoshemangiomasemidadepediátrica
Resumo
Introduc¸ão:Oshemangiomassãoalesãotumoralcutâneamaisfrequenteemidadepediátrica. Atéao momentotodasasopc¸ões terapêuticas(tantomédicascomo cirúrgicas)têm resulta-dossub-ótimos.Recentemente,foidescritaautilizac¸ãodepropranololparatratamentodos hemangiomas.Relatamososresultadosdanossaexperiênciacomestaopc¸ãoterapêutica.
Objetivo:Avaliac¸ãoprospetivadaeficáciaeseguranc¸adepropranololemcrianc¸ascom heman-giomainfantil.
Métodos: Avaliac¸ão prospetiva de todos os doentes com hemangioma referenciados para avaliac¸ão cardiovascularprévia ao iníciode terapêuticacompropranolol. Opropranololfoi administradonumadoseinicialde1mg/kg/diaetituladaparaumadosealvode2---3mg/kg/dia, deacordocomarespostaclínica.Aeficáciafoiavaliadaatravésdeumaescala fotográfica. Aseguranc¸afoiavaliadaatravésdarecolhadedadossobreosefeitossecundáriossignificativos.
Resultados: Desde2010,30crianc¸as(15dosexofeminino)comhemangiomasforam referenci-adosparaavaliac¸ãocardiovascularpréviaaoiníciodeterapêuticabeta-bloqueante,comuma idademédiade6meses(1-63meses).A dosealvo médiaatingidafoi de2,8mg/kg/dia, comumadurac¸ãomédiadetratamentode12 meses.Emtodososdoentesseverificouuma reduc¸ãosignificativadasdimensõesevolumedoshemangiomas.Nãoforamobservadosefeitos colaterais.
Conclusões:Nanossaexperiência,opropranololéumaopc¸ãoeficazeseguraparaotratamento dehemangiomasextensosoucomplicados,obtendo-seumareduc¸ãorápidaesignificativadas suasdimensões.Nãoforamobservados efeitosadversoscontudo,recomenda-se aavaliac¸ão cardiovascularsistemática,préviaaoiníciodeterapêuticacompropranolol.
© 2013 SociedadePortuguesa de Cardiologia. Publicado por Elsevier España, S.L.Todos os direitosreservados.
Introduction
Infantile hemangiomasare the most common benign vas-culartumorsininfancy,affecting5---10%ofthepopulation. Femalesareaffectedmoreoften thanmales,witha ratio of3:1.1Typicallytheypresentshortlyafterbirth,undergo
a period of rapid proliferation, and then slowly involute overmanyyears.2,3Althoughmostaresmallcutaneous
vas-cular malformationsof the face,4 theycan alsobe large,
disfiguringlesionswithseriouscomplications.Infants with largehemangiomas,especiallythosewithasegmental dis-tribution or hemangiomatosis, are at particular risk for extracutaneous complications. They may also be associ-atedwithothercongenitalmalformations,suchasPHACE,5
PELVIS4orSACRALsyndrome.6,7
In mostcases only parentaleducationand reassurance arerequired.Although85---90%ofallinfantilehemangiomas eventuallyundergospontaneousinvolution,aminoritycan stillcausedisfigurementandseriouscomplications, depend-ing on their location (obstruction of airways and vision), size, and speed of regression, which can be associated with painful ulcerations and hemorrhage or even high-outputheartfailure.4,8,9Hemangiomaswiththepotentialto
threatenachild’slifeorvitalfunctionsandthosethat ulcer-ateorcausesubstantialdisfigurementwarranttreatment,10
which may be medical or surgical, or a combination of both.11
Atpresentthereisnogoldstandardmedicaltreatment. Unfortunately,currenttherapeuticapproacheshavelimited
success and significant adverse effects that limit their use.12---16 Since Léauté-Labrèze’s accidental observation17
of the anti-proliferative effect of propranolol on infan-tile hemangiomas, propranolol has become increasingly popular18,19 asasuccessfultherapeuticoption,withfewer
sideeffectsthanothertreatments.
Wepresentasingle-centerstudydescribingtheefficacy andsafetyofpropranololinchildrenwithinfantile heman-giomas.
Methods
Inclusionandexclusioncriteria
Allpatientswerereferredbytheirpediatricdermatologist or pediatric surgeontoapediatric cardiology department forbaselinecardiovascularassessmentpriortopropranolol therapy,andcardiovascularassessmentduringtherapy.
Patients with infantile hemangiomas were considered for propranolol treatment if they met the following cri-teria: eyelid involvement withrisk of ocular occlusionor compression;airwayobstruction;orlargehemangiomawith significant disfigurement orulceration. Patientspreviously treated with other therapeutic modalities were also con-sidered candidatesfor inclusion iftheprevious treatment had failed. Exclusioncriteria included cardiac anomalies, centralnervoussystemvascularanomaliesasinPHACE syn-drome,hypoglycemia,asthmaorbronchospasm.Whilethe
study focused on infants, patients over one year of age wereenrollediftheirhemangiomasshowedsignsof contin-uedproliferationorhadshownnosignsofresolutionsince infancy.
Treatmentprotocol
All patients underwent full cardiac examination before treatment,whichincludedclinicalexamination,heartrate andbloodpressuremeasurements,electrocardiogram,and echocardiogram.Abaselinefingerstickblood glucoselevel wasobtained.Furthermonitoringduringthestudyincluded a weekly re-evaluationwhile thedose wasbeing titrated toits maximum target dose, at weeks1---4. Parents were instructed to look for signs of lethargy, poor feeding or wheezing. After the first month, monthly follow-up visits werescheduled until theend of the treatment for sever-ity scoring of the hemangiomas, physical assessment and monitoringforadverseeffects.
Dosageandduration
Propranololwasgivenatastartingdoseof1mg/kg/day,in twoorthreedivideddoses,andtitratedtoatargetdoseof 2---3mg/kgperdayaccordingtoclinicalresponse.
Severityscoringsystem
Aphotograph-basedseverityscoringscalewasused.Frontal and lateral pictures of every patient were taken before treatmentandateveryfollow-upvisit.
Results
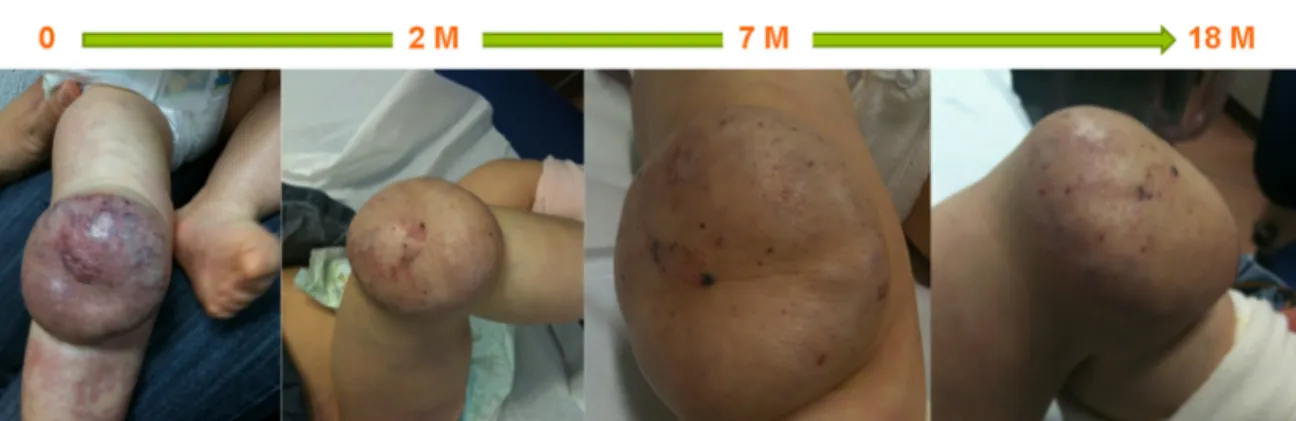
Startingin2010thirtypatientswereincludedinthisstudy, of whom 15 (50%) were female; none were born prema-turely.Superficialhemangiomawasthepredominanttype, observed in 25 (83%) patients, whereas in three (10%) the hemangiomas had a segmental distribution (Table 1). The mostfrequent locationwasfacial-cervical(70%). Pro-pranolol was started at a median age of six months (1---63months);theoldestpatientwasfiveyearsold.Themean target propranolol dose was 2.8 mg/kg/day (range 2.5---3.2 mg/kg/day). The mean duration of therapy was 12 months.Allpatientsexperiencedimmediatecolorchanges and effects on the rate of hemangioma growth; in all patients a reduction of its size and volume was seen (Figures1---3).Noadverseeffectswereidentifiedorreported by the patients or their parents. Propranolol was discon-tinuedin fivepatientswhentheresiduallesionsceasedto respondtotherapy;onehadaslightrelapsebutitwasnot necessarytore-startpropranolol.
In this groupof patients propranolol therapy had simi-lareffectivenessregardlessofageatinitiationoftreatment (beforeoraftersixmonthsofage).Itwasequallyeffective in hemangiomas considered to be beyond the prolifera-tivephase.Also,segmentalandnonsegmental,superficial, mixed, and deepinfantile hemangiomas showeda similar responsetopropranolol(Figures1---3).
Table1 Summaryofpatientcharacteristics. n=30 Female:maleratio 1:1 Typeofhemangioma Superficial 25 Deep 5 Distributionofhemangioma Head 8 Periocular/eyelidinvolvement 9 Peribuccualinvolvement 4 Thoracicinvolvement 5 Limbinvolvement 4
Baselineassessment(bloodpressure,fastingblood glucose,heartrate)
Normal All Electrocardiogrampre-treatment Normal All Echocardiogrampre-treatment Normal 24 Abnormal 6
Discussion
Inourexperiencepropranololappearstobeauseful treat-ment for severe or complicated infantile hemangiomas, achieving a rapid and significant reduction in size. This reductionwasmainlyachievedduringthefirst20weeksof treatment,andfurthertreatmentinduced alessdramatic therapeutic effect. In this series of patients propranolol wasequallyeffectiveinbothsegmentalandnonsegmental infantilehemangiomasandinthosebeyondtheproliferative phase.
Infantile hemangiomas have a predictable natural history.4,20Themajorityarenotpresentatbirth.Ahallmark
ofinfantilehemangiomaisitsdramaticgrowthafterbirth, bydiffuseproliferationofimmature endothelialcells, fol-lowedbyspontaneousregression.Themajorityofchildren with infantile hemangiomas require no treatment as the lesionsregressovertimeandproducenolong-termscarring; regressionis completein50%offive-year-oldpatientsand 90%ofnine-year-olds.16Inapproximately10%ofcasesthere
canbeseriousor life-threatening hemangiomas,requiring treatment.10
Current treatment options for complicated heman-giomas include various medical or surgical modalities. Until recently, the mainstay of treatment for infantile hemangiomaswascorticosteroidsin variousforms, includ-ingtopical, intralesional,and oral formulations,the most commonbeingoralprednisolone.12 Onlyin complicatedor
refractoryhemangiomacaseshaveothertreatment modal-ities been considered, such as chemotherapeutic agents (vincristine, interferon-alpha), laser therapy, surgery or a combination of these, and, most recently, propranolol. Each treatment option has limited therapeutic benefit, withits own side effects and risks. However,in the past three years there have been more than 120 reports of theefficacy of oral beta-blockers, usually propranolol, as
Figure1 Afour-month-oldgirlwhopresentedwithalargehemangiomaontheleftuppereyelid,showingcompleteinvolutionof thelesionsafterfivemonthsoforalpropranolol.M:months.
Figure2 Atwo-month-oldboywhopresentedwithhemangiomaontheleftthigh,showingcompleteinvolutionofthelesionon
thighandscrotumaftereightmonthsoftherapy.M:months.
ahighly effective therapeuticoption for infantile heman-gioma and its complications.18,21---23 Furthermore, it has
beendemonstratedthatpropranolol therapyissuperiorto oral corticosteroid treatment, the former standard ther-apy for infantile hemangioma, and should be considered the first-line agent given its safety and efficacy.24
Possi-bleexplanationsfor the therapeuticeffectof propranolol onhemangiomasincludevasoconstrictionbydecreasingthe releaseof nitric oxide, which is immediately visible asa
change incolor,associatedwithpalpabletissuesoftening. Othersuggestionsaredown-regulationofproangiogenic sig-nalssuchasVEGF,bFGF, MMP-9andHBMEC,andinduction ofapoptosisinproliferatingcapillaryendothelialcells.25,26
A large international randomized clinical trial is under-way,butmanyarealreadyadvocatingitsuseasafirst-line treatment for infantile hemangiomas, in terms of both safety and efficacy.21,27 Its effects were first discovered
by chanceby Léauté-Labrèzeetal.in2008.17 Subsequent
Figure3 Aten-month-oldboywithhemangiomaontherightpatellaandupperrightleg,showingafairresponseafter18months
Infan
til e he
mang
ioma
The
prop
rano
lol
algo
rithm
Infantile hemangioma- risk of ulceration - risk of organ dysfunction - risk of disfiguration Exclude - PHACE syndrome - diffuse hemangiomatosis - PELVIS syndrome Cardiovascular assessment - Physical examination - Heart rate, blood pressure - Blood glucose - Electrocardiogram - Echocardiogram Contraindications - Bradycardia - Bronchospasm - Hypotension - Hypoglycemia Dosage
- Start with 1 mg/kg/day
- Titrate up to 3 mg/kg/day weekly
Adverse reactions - Bradycardia - Bronchospasm - Hypotension - Hypoglycemia Follow-up
- Clinical assessment every three months - Photograph lesions at each assessment - If complete regression or plateau:
start progressive weaning – reduce dosage by 1 mg/kg/day weekly - If rebound:
return to previous dosage - If adverse reactions or no regression:
stop proranolol
Figure4 Flowchartshowingproposedwork-upandtreatmentprotocol.
reportshaveemphasizedpropranolol’srolenotonlyin halt-inghemangiomagrowthbutalsoindiminishingtheirsize.21
Most groups have used a maximum target dose of 1---3 mg/kg/day.9,11,17,18,21,22,28---37 However, there are no
estab-lishedconsistentprotocols,particularlyregardingthetiming oftreatmenttaperinganddiscontinuation.9,11,17---19,21,22,28---37
Thereisalsonoconsensusregardingtherelapserateafter discontinuation,withsomestudiesshowingnorelapses,30---32
while others reportminor recurrences.17,18,36 In our short
series only one of the patients in whom propranolol was tapered showeda slight,non-significant, relapse,withno needtore-starttreatment.
Until recently,themostcommonapproachforpatients withinfantilehemangiomasinthepost-proliferativephase was ‘‘active non-intervention’’.38 In our series,
propra-nolol improved esthetics in all patients, giving scope for more conservative surgical intervention in the future if
necessary.Thesefindingsareconsistentwiththosereported by Zvulunov et al.,39 Schupp et al.36 and Celik et al.,21
whoreportedtheresultsofpropranololtherapyfor heman-giomasbeyondtheproliferativephase,andimplythatoral propranolol therapy may be warranted in children with lateresidual infantilehemangiomas, prior toany surgical intervention.21Still,themostimpressiveresponsesoccurred
inthe youngest patients, afindingthat is consistent with thenaturalhistoryofhemangioma,inwhich80%ofitssize isreachedbysixmonthsofage,andjustifiesreferringsuch casesearlierforoptimaltherapeuticresponse.
The appropriate monitoring protocol for assessment of adverse effects in infants with infantile hemangiomas, before and during propranolol treatment, has not been established.18,19Thepotentialsideeffectsofbeta-blockers,
which are well known and include bradycardia, hypoten-sion,andhypoglycemia,11,18,33,40---44must beborneinmind.
Propranolol is also contraindicated in patients with asthma, and it is not recommended during episodes of bronchiolitis.18,45 Notwithstanding, propranolol appears to
be a safe drug when correctly administered. No adverse effectswere observed in ourseries; none of ourpatients had symptoms of hypoglycemia or hypotension. However, untillargerclinicaltrialsarecompleted,potentialadverse eventsshouldbeborneinmindandconsultationwithlocal specialistssuchaspediatric cardiologists isrecommended priortoinitiatingtreatment.PatientswithPHACEsyndrome andseverecerebrovasculardiseaseare,atleastintheory,at riskforbrainischemiaevenwiththerelativelymild hypoten-sioninducedbybeta-blockers.19Therisksandbenefitsinthis
subsetofpatientsmustbeweighedcarefully.Figure4 sum-marizesourtreatmentalgorithmbasedonourexperience.
Inconclusion,abetterunderstandingofthemechanisms ofpropranolol-inducedregressionofinfantilehemangiomas will provide opportunities to design even more success-ful therapies. Meanwhile, propranolol appears to be a uniquely effective and safe therapy for infantile heman-giomas,includinginthepost-proliferativephase,andshould beconsideredthefirst-linetherapyinthissetting.
Ethical
disclosures
Protection of human and animal subjects.The authors declarethat the proceduresfollowed were in accordance withtheregulationsoftherelevantclinicalresearchethics committeeandwiththoseoftheCodeofEthicsoftheWorld MedicalAssociation(DeclarationofHelsinki).
Confidentialityofdata.Theauthorsdeclarethattheyhave followedtheprotocolsoftheirworkcenteronthe publica-tionofpatientdata.
Right to privacy and informed consent.The authors declarethatnopatientdataappearinthisarticle.
Conflicts
of
interest
Theauthorshavenoconflictsofinteresttodeclare.
References
1.KilclineC,FriedenIJ.Infantilehemangiomas:howcommonare they? Asystematic reviewofthe medicalliterature. Pediatr Dermatol.2008;25(2):168---73.
2.DroletBA,SwansonEA,FriedenIJ,etal.Infantilehemangiomas: anemerginghealthissuelinkedtoanincreasedrateoflowbirth weightinfants.JPediatr.2008;153(5):712---5,715.e1.
3.ChangLC,HaggstromAN,DroletBA,etal.Growth character-isticsofinfantilehemangiomas:implicationsformanagement. Pediatrics.2008;122(2):360---7.
4.Léauté-LabrèzeC,PreyS,EzzedineK.Infantilehaemangioma: Part I. Pathophysiology, epidemiology, clinical features, life cycleandassociatedstructuralabnormalities.JEurAcad Der-matolVenereol.2011;25(11):1245---53.
5.MetryDW,HaggstromAN,DroletBA,etal.Aprospectivestudy ofPHACEsyndromeininfantilehemangiomas:demographic fea-tures,clinicalfindings,andcomplications.AmJMedGenetA. 2006;140(9):975---86.
6.StockmanA,BoraleviF,TaïebA,etal.SACRALsyndrome:spinal dysraphism,anogenital,cutaneous,renalandurologic anoma-lies,associatedwithanangiomaoflumbosacrallocalization. Dermatology.2007;214(1):40---5.
7.Pandey A, Gangopadhyay AN, Upadhyay VD. Evaluation and management of infantile hemangioma: an overview. Ostomy WoundManage.2008;54(5):16---8,20,22---6,28---9.
8.Chamlin SL, Haggstrom AN, Drolet BA, et al. Multicen-ter prospective study of ulcerated hemangiomas. J Pediatr. 2007;151(6):684---9,689.e1.
9.Léauté-LabrèzeC,PreyS,EzzedineK.Infantilehaemangioma: PartII.Risks,complicationsandtreatment.JEurAcadDermatol Venereol.2011;25(11):1254---60.
10.SchwartzRA,SidorMI,MusumeciML,etal.Infantile haeman-giomas: a challenge in paediatric dermatology. J Eur Acad DermatolVenereol.2010;24(6):631---8.
11.Buckmiller LM, Munson PD, Dyamenahalli U, et al. Pro-pranolol for infantile hemangiomas: early experience at a tertiaryvascularanomaliescenter.Laryngoscope.2010;120(4): 676---81.
12.BennettML,FleischerAB,ChamlinSL,etal.Oralcorticosteroid useiseffectiveforcutaneoushemangiomas:anevidence-based evaluation.ArchDermatol.2001;137(9):1208---13.
13.AkhavanA,ZippinJH.Currenttreatmentsforinfantile heman-giomas.JDrugsDermatol.2010;9(2):176---80.
14.EzekowitzRA,MullikenJB,FolkmanJ.Interferonalfa-2a ther-apyforlife-threateninghemangiomasofinfancy.NEnglJMed. 1992;326(22):1456---63.
15.MichaudAP,BaumanNM,BurkeDK,etal.Spasticdiplegiaand othermotordisturbancesininfantsreceivinginterferon-alpha. Laryngoscope.2004;114(7):1231---6.
16.ZimmermannAP,WiegandS,WernerJA,etal.Propranolol ther-apyforinfantilehaemangiomas:reviewoftheliterature.IntJ PediatrOtorhinolaryngol.2010;74(4):338---42.
17.Léauté-LabrèzeC,DumasdelaRoqueE,HubicheT,etal. Pro-pranolol for severe hemangiomasof infancy. N Engl J Med. 2008;358(24):2649---51.
18.Sans V, de la Roque ED, Berge J, et al. Propranolol for severe infantile hemangiomas: follow-up report. Pediatrics. 2009;124(3):pe423---31.
19.Lawley LP, Siegfried E, Todd JL. Propranolol treatment for hemangiomaof infancy: risksand recommendations.Pediatr Dermatol.2009;26(5):610---4.
20.JinninM,IshiharaT,BoyeE,etal.Recentprogressinstudiesof infantilehemangioma.JDermatol.2010;37(4):283---98.
21.CelikA,TiryakiS,MusayevA,etal.Propranololasthefirst-line therapyforinfantilehemangiomas:preliminaryresultsoftwo centers.JDrugsDermatol.2012;11(7):808---11.
22.NeriI,BalestriR,PatriziA.Hemangiomas:newinsightand medi-caltreatment.DermatolTher.2012;25(4):322---34.
23.PhillipsCB,PachaO,Biliciler-DenktaG,etal.Areviewofbeta antagonisttreatmentforinfantilehemangioma.JDrugs Derma-tol.2012;11(7):826---9.
24.PriceCJ, Lattouf C,Baum B, et al. Propranolol vs corticos-teroidsforinfantilehemangiomas:amulticenterretrospective analysis.ArchDermatol.2011;147(12):1371---6.
25.Leaute-Labze C, Taieb A. Efficacy of beta-blockers in infantilecapillaryhaemangiomas:thephysiopathological signif-icanceandtherapeuticconsequences.AnnDermatolVenereol. 2008;135(12):860---2.
26.Leaute-LabrezeC,DumasdelaRoqueE,HubicheT,etal. Pro-pranolol for severe hemangiomasof infancy. N Engl J Med. 2008;358(24):2649---51.
27.Holmes WJ, Mishra A, Gorst C, et al. Propranolol as first-linetreatmentforinfantilehemangiomas.PlastReconstrSurg. 2010;125(1):420---1.
28.DenoyelleF,LeboulangerN,EnjolrasO,etal.Roleof propra-nololin thetherapeuticstrategyofinfantile laryngotracheal
hemangioma. Int J Pediatr Otorhinolaryngol. 2009;73(8): 1168---72.
29.RosbeKW,SuhKY,MeyerAK,etal.Propranololinthe manage-mentofairwayinfantilehemangiomas.ArchOtolaryngolHead NeckSurg.2010;136(7):658---65.
30.MarscianiA, PericoliR,AlaggioR, etal.Massive responseof severe infantile hepatic hemangioma to propanolol. Pediatr BloodCancer.2010;54(1):p176.
31.Li YC, McCahon E, Rowe NA, et al. Successfultreatment of infantile haemangiomas of the orbit with propranolol. Clin ExperimentOphthalmol.2010;38(6):554---9.
32.ManunzaF, SyedS, LagudaB, et al.Propranolol for compli-catedinfantilehaemangiomas:acaseseriesof30infants.Br JDermatol.2010;162(2):466---8.
33.HaiderKM,PlagerDA,NeelyDE,etal.Outpatienttreatment of periocular infantile hemangiomas with oral propranolol. JAAPOS.2010;14(3):251---6.
34.MaturoS,HartnickC.Initialexperienceusingpropranololasthe soletreatmentforinfantileairwayhemangiomas.IntJPediatr Otorhinolaryngol.2010;74(3):323---5.
35.NaouriM,SchillT,MaruaniA, et al.Successfultreatmentof ulceratedhaemangiomawithpropranolol.JEurAcadDermatol Venereol.2010;24(9):1109---12.
36.SchuppCJ, KleberJB, GüntherP,et al. Propranololtherapy in 55 infants with infantile hemangioma: dosage, duration, adverseeffects,andoutcome.PediatrDermatol.2011;28(6): 640---4.
37.Starkey E, Shahidullah H. Propranolol for infantile haeman-giomas:areview.ArchDisChild.2011;96(9):890---3.
38.Maguiness SM, Frieden IJ. Current management of infantile hemangiomas.SeminCutanMedSurg.2010;29(2):106---14.
39.Zvulunov A, McCuaig C, Frieden IJ, et al. Oral propranolol therapy for infantile hemangiomas beyond the proliferation phase: a multicenter retrospective study. Pediatr Dermatol. 2011;28(2):94---8.
40.Kallen RJ,Mohler JH, LinHL. Hypoglycemia:a complication of treatment of hypertension with propranolol. Clin Pediatr (Phila).1980;19(8):567---8.
41.Belson MG, Sullivan K, Geller RJ. Beta-adrenergic antag-onist exposures in children. Vet Hum Toxicol. 2001;43(6): 361---5.
42.BreurJM,deGraafM,BreugemCC,etal.Hypoglycemiaasa resultofpropranololduringtreatmentofinfantilehemangioma: acasereport.PediatrDermatol.2011;28(2):169---71.
43.de GraafM,BreurJM,RaphaëlMF,et al.Adverse effectsof propranolol when usedin thetreatment ofhemangiomas: a case series of28 infants. J Am Acad Dermatol. 2011;65(2): 320---7.
44.Holland KE, Frieden IJ, Frommelt PC, et al. Hypoglycemia in childrentakingpropranolol for thetreatmentof infantile hemangioma.ArchDermatol.2010;146(7):775---8.
45.FraleyDS,BrunsFJ,SegelDP,etal.Propranolol-related bron-chospasminpatientswithouthistoryofasthma.SouthMedJ. 1980;73(2):238---40.