SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Technical
Note
Reconstruction
of
anterior
cruciate
ligament
and
anterolateral
ligament
using
interlinked
hamstrings
–
technical
note
夽
Marcio
de
Castro
Ferreira
a,b,∗,
Flavio
Ferreira
Zidan
b,
Francini
Belluci
Miduati
b,
Caio
Cesar
Fortuna
a,b,
Bruno
Moreira
Mizutani
b,
Rene
Jorge
Abdalla
a,caHospitaldoCorac¸ão,DepartamentodeOrtopediaeTraumatologia,SãoPaulo,SP,Brazil
bHospitalRenascenc¸a,DepartamentodeCirurgiadeJoelho,Osasco,SP,Brazil
cUniversidadeFederaldeSãoPaulo,EscolaPaulistadeMedicina,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received19August2015 Accepted25August2015 Availableonline4July2016
Keywords:
Anteriorcruciateligament reconstruction
Anterolateralligament Orthopedicprocedures
a
b
s
t
r
a
c
t
Recentanatomicalandbiomechanicalstudiesontheanterolateralligament(ALL)ofthe kneehaveshownthatthisstructurehasanimportantfunctioninrelationtojointstability, especiallywhenassociatedwithanteriorcruciateligament(ACL)injury.However,the crite-riaforitsreconstructionhavenotyetbeenfullyestablishedandthesurgicaltechniques thathavebeendescribedpresentvariationsregardinganatomicalpointsandfixation mate-rials.ThisstudypresentsareproducibletechniqueforALLandACLreconstructionusing hamstringtendons,inwhichthreeinterferencescrewsareusedforfixation.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Reconstruc¸ão
dos
ligamentos
cruzado
anterior
e
anterolateral
com
flexores
enlac¸ados
–
Nota
técnica
Palavras-chave:
Reconstruc¸ãodoligamentocruzado anterior
Ligamentoanterolateral Procedimentosortopédicos
r
e
s
u
m
o
Osrecentes estudosanatômicos e biomecânicossobre oligamento anterolateral(LAL) dojoelhoevidenciamqueessaestruturaapresenta func¸ãorelevanteparaaestabilidade articularprincipalmentequandoassociadaàlesãodoligamentocruzadoanterior(LCA). Noentanto,os critérios parasua reconstruc¸ão aindanão estãototalmente estabeleci-dos,assimcomo astécnicascirúrgicasdescritas apresentamvariac¸õessobreospontos
夽
StudyconductedattheHospitalRenascenc¸a,DepartamentodeCirurgiadeJoelho,Osasco,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](M.C.Ferreira).
http://dx.doi.org/10.1016/j.rboe.2015.08.021
anatômicosemateriaisdefixac¸ão.Oestudoapresentaumatécnicareprodutívelparaa reconstruc¸ãodoLALeLCAcomostendõesflexoresqueusatrêsparafusosdeinterferência paraasfixac¸ões.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Thetreatmentofanteriorkneeinstabilitythrough reconstruc-tion of the anterior cruciate ligament (ACL) presents good clinicalresults. However,the failurerate forthis operation isestimatedtorangefrom1.8%to14%.1,2Thepersistenceof anterolateralinstabilityassessedbythepivot-shifttest post-operativelyisdescribedasoneofthosefactors.2,3
After the anatomical “rediscovery” and biomechanical studies of the anterolateral ligament (ALL) demostrated that this structure is important in anterolateral knee sta-bility, it was observed that insufficiency of this ligament may contribute to the functional failure of isolated ACL reconstructions.4
Thisstudy aimedtopresentareproducibletechniqueof anatomicalACLandALLreconstructionwiththehamstring tendons,usingthreeinterferencescrews.
Surgical
technique
Fifteenadultpatients(19–38years),12menandthreewomen, underwent ACL and ALL reconstruction by the technique describedbelow,withameanfollow-upof10months(6–15 months).Allpatientsreturned,withoutcomplaints,to activi-tiesofdailylivingand/ortosportsandrecreationalactivities thattheypracticedpriortoinjury.
Indication
Afterspinalanesthesia,aclinicalexaminationwasperformed toestimateALLsufficiency.
Theanteriorasymmetryofthelateralplateauwith inter-nalrotationofthetibiainflexionof30–60◦5 relativetothe
contralateralknee,andincreasedpositivityofthepivot-shift maneuvercanbeaclinicalsignoffailureoftheALL.4
Thestudyusedtheclassificationforthepivot-shift maneu-ver determined by the International Knee Documentation Committee6(IKDC)2000,whichdescribesfourgrades:0– nor-mal,1–glide,2–clunk,3–grossshift.
ThecriteriausedforALLreconstructionassociatedwith ACLinjurieswere:
1. InjuryintheALLsubstanceidentifiedatamagnetic reso-nanceimaging(MRI),termedSegond-likeinjury;
2. Segondfracture7;
3. Pivot-shiftclassifiedasgradeII/III;
4. ACL reconstruction reviewin which patients had resid-ualpivot-shiftduringthepostoperativeperiodandevolved withgraftinjury;
5. Asymmetrical anterior lateral plateau visible with knee internalrotationinflexionbetween30◦and60◦.
6. Lateralfemoralnotchsign.8
Graftpreparationandsurgicaltechnique
Theexcisionofthesemitendinosustendon(ST)andgracilis tendon(GR)ismadethrougha4-cmanteromedialincisionin
thetibiaoverthepesanserinus.
During the arthroscopic procedure forthe anteromedial and anterolateral portals, the joint is assessed and the intercondyle is cleaned, whiletendons are handled at the instrumentationtable.AllgraftsarepreparedwithEthibondR n◦2(Ethicon,Somerville,NJ).
TheGRusedtorebuildtheALLispreparedtoformadouble graft.EachendissuturedwithKrackowstitches.
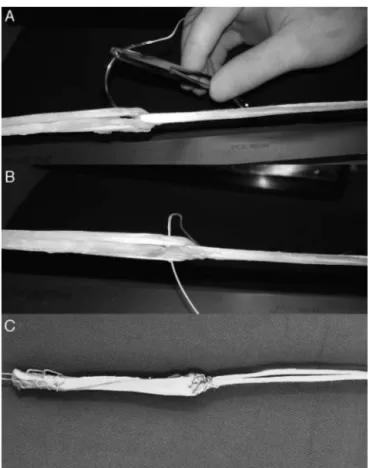
One end ofthe GR is passed as a “handle” during the preparationofthetripleSTgraft,whichwillbeusedforACL reconstruction, so that the double GR graft has the same sizeinits twoparts and thetriple STgraft hasaKrackow sutureinoneendandtheotherendisanchoredinthe GR (Fig.1A–C).
After preparation and measurement of graft diameters (usually8mmforthetripleSTgraftand5mmforthedouble GR),thefemoralandtibialtunnelsareprepared.
Thefemoraltunnel,commontotheACLandALL,ismade usingtheoutside-intechnique.AtibialACLguideisplacedso thatitsjointpositionoverlapsthefootprintoftheanatomical insertionoftheACLintheintercondylarwall.A65◦opening
isappliedtominimizethe“killerturn”ofthegraft.
AftertheACLguideispositionedandthesitewherethe guide wirewill beintroducedis assessed,the guidewireis removed,and a4-cmlongitudinal incisionin theskin and iliotibialtractisperformedonthelateralsideoftheknee.
The lateral epicondyle is identified by palpation; the guidewire is introduced 8mm (about one digital tip) posterosuperiorly9,10inthelateralfemoralcortextomarkthe entrysite.
The ACL guide is then reattached and coupled to the guidewire,followedbythedrillingofthepathfortheACL foot-print.Sequentially,onedrillofthesamediameterasthegraft isusedtomakethetunnel,whichisgenerally35-mmlong.
Fig.1–(A)Tensionedtriplesemitendinosusgraftand doublegracilisgraft;intertwined,readyforsuturing.(B) Triplesemitendinosusgraft(LCA)anddoublegracilisgraft (LAL),startedsuturing.(C)Finishedgrafts.
AftercreatingthetunnelsfortheACL,asutureispassed withtheguidewirethroughfouroutside-inholesthroughthe femoraltunneland withdrawnwithagraspertoolthrough thetibialtunnel,soastopassoverthejointandallowforthe passageofthegraft.
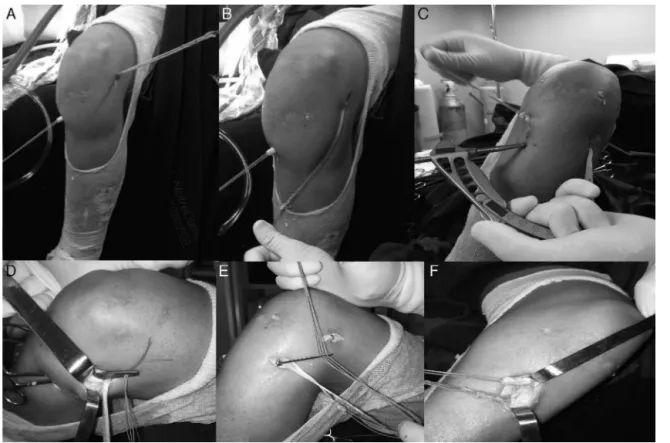
SuturesattheloosenedgeoftheSTgraft(ACL)arelooped inthetransacetabularwireandthegraft ispassed outside-infromthefemurtothetibia,remaininginitsfinalposition (Fig.2AandB).Aninterferencescrewofthesamediameteras thedrilledtunnel,with30–35mmlength,isusedforfemoral fixation.
ForthereconstructionandattachmentoftheALLinthe tibia,theACLguideispositionedat65◦,sothattheguidewire
canbeinserted2cmdistaltothetibialtunnelthroughthe sameincision madeforACLgraft removal.Itexitshalfway betweenGerdy’stubercleandtheheadofthefibula,9–13mm distaltothesurfaceofthelateraltibialplateau,theanatomical ALLpoint.9
A 3-cmanterolateral skin and iliotibial tract incision is made(Fig.2C)andthetunnelisdrilledwitha6-mmbit.
Alongforcepsisintroduced throughtheALLtibial inci-siondeepintotheiliotibialtractuntilitsoutputinthefemoral ACLtunnelincision,wheretheGRgraftispulledandpassed throughthetibialALLtunnel(Fig.2D–F).
Thekneeisthenplacedat30◦flexionforACLfixationand
at45–60◦ forALLfixation5withinterferencescrewsthatare
2mmlargerthanthedrilledtunnels,boththroughthesame anteromedialincision.Thesuturegraftscanbetiedto rein-forcethefixation.
Postoperative rehabilitationfollowsthe protocol forACL reconstructionwithhamstrings.
Discussion
The“rediscovery”oftheALLanditsroleinanterolateralknee stabilityiscurrentlypresentedasoneofthetrendsinknee ligamentreconstructions.11
ThefactsthattheALLisnotastructureroutinelydescribed inMRIreportsandthatthereconstructioncriteriaarenotfully establishedcontributetothemissdiagnosisand undertreat-mentofthisinjury.
Helito etal.12 showedthat theALLisfully visualizedin 71.7%oftheMRIs.Inturn,Tanejaetal.13haveidentifiedthe fullALLviewin11%.
Spenceretal.4showedthattheanterolateralknee insta-bility is accentuated when the ACL and the ALL are torn, emphasizingthepivot-shiftmaneuver.
Sonnery-Cottetetal.11recommendALLreconstructionin Segondfractures,chronicACLinjuries, gradeIIIpivot-shift,
high-levelathletesorthosewhopracticesportsthatrequire rotationoftheknee,andinthepresenceoflateralfemoral notch sign.8 However, the presentauthors donot consider chronicityand thepatient’sactivitiesascriteriafor empiri-calALLreconstructionifthephysicalexaminationshowsno evidenceofitsfailure.
RegardingthedescribedtechniquesforACLandALL recon-struction,Helitoetal.14usedaquadruplegraft(tripleSTand oneGR)forACLandoneGRforALL;tibialfixationwas con-ducted withanchors.Sonnery-Cottet etal.11 usedtriple ST graftforACLanddoubleGRgraftforALL,withtwotibialholes torebuildtheALL.
Inthepresenttechnique,themethodusedforgraft prepa-rationcreatesasuspensioneffectsimilartotheEndobutton, added to the suture to reinforce this union, which also includesaninterferencescrew.ThisallowstheendoftheST grafttoremainclosetothearticularfemoralpoint,andthereis noneedtooccupytheentiretunnel,whichwillbecompleted bytheGRgraft,thusfacilitatingtheprocedureincaseofshort grafts.
StudieshaveshowndifferencesintheALLfemoral anatom-icalpoint.Caterineetal.10andKennedyetal.9demonstrated thatitsoriginisonaverage3mmposteriorandproximalto the lateral epicondyle; this point was used in the present technique.Inturn,Helitoetal.15 andClaesetal.16 demon-strated that the origin ofthe ALLis anteriorto the lateral epicondyle.
Theoptionadoptedinthepresenttechniquewastomake thetunnelposterosuperiortothelateralepicondyle,inorder toreducetheintraarticular“killerturn”ofthegraft;thispoint approachestheisometricsdescribedbyKurosawaetal.17for lateraltenodesisoftheiliotibialtract.
Fig.2–(A)ACLgraftpositionedinthefemoralandtibialtunnelsandALLgraftfixedinthefemoralpoint;(B)doubleGRgraft lengthtorebuildtheALLonthepathitmustfollow;(C)positioningoftheACLguideat65◦andexitpointhalfwaybetween
Gerdy’stubercleandthefibularhead,13mmfromthesurfaceofthelateraltibialplateau;(D)clamppasseddeepintothe iliotibialtracttodrivetheALLgraftintothetibialtunnel;(E)passageoftheALLgraftthroughthetibialtunnel;(F)ACLand ALLgraftsreadytobefixedwithinterferencescrewthroughthesameincision.
Conclusion
ACLand ALL reconstructionusing the techniquedescribed fortheanterolateralinstabilityofthekneewassatisfactory inthesepatients;itusesmaterials,guides,andincisionsthat arefamiliartoanysurgeon,whichfacilitatesitsreproduction.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. MariscalcoMW,FlaniganDC,MitchellJ,PedrozaAD,Jones MH,AndrishJT,etal.Theinfluenceofhamstringautograft sizeonpatient-reportedoutcomesandriskofrevisionafter anteriorcruciateligamentreconstruction:aMulticenter OrthopaedicOutcomesNetwork(MOON)CohortStudy. Arthroscopy.2013;29(12):1948–53.
2. ProdromosCC,JoyceBT,ShiK,KellerBL.Ameta-analysisof stabilityafteranteriorcruciateligamentreconstructionasa functionofhamstringversuspatellartendongraftand fixationtype.Arthroscopy.2005;21(10):1202.
3. MohtadiNG,ChanDS,DaintyKN,WhelanDB.Patellartendon versushamstringtendonautograftforanteriorcruciate
ligamentruptureinadults.CochraneDatabaseSystRev. 2011;(9):CD005960.
4.SpencerL,BurkhartTA,TranMN,RezansoffAJ,DeoS, CaterineS,etal.Biomechanicalanalysisofsimulatedclinical testingandreconstructionoftheanterolateralligamentof theknee.AmJSportsMed.2015;43(9):2189–97.
5.ParsonsEM,GeeAO,SpiekermanC,CavanaghPR.The biomechanicalfunctionoftheanterolateralligamentofthe knee.AmJSportsMed.2015;43(3):669–74.
6.IrrgangJJ,HoH,HarnerCD,FuFH.UseoftheInternational KneeDocumentationCommitteeguidelinestoassess outcomefollowinganteriorcruciateligamentreconstruction. KneeSurgSportsTraumatolArthrosc.1998;6(2):107–14.
7.ClaesS,LuyckxT,VereeckeE,BellemansJ.TheSegond fracture:abonyinjuryoftheanterolateralligamentofthe knee.Arthroscopy.2014;30(11):1475–82.
8.HerbstE,HoserC,TecklenburgK,FilipovicM,DallapozzaC, HerbortM,etal.ThelateralfemoralnotchsignfollowingACL injury:frequency,morphology,andrelationtomeniscal injuryandsportsactivity.KneeSurgSportsTraumatol Arthrosc.2015;23(8):2250–8.
9.KennedyMI,ClaesS,FusoFA,WilliamsBT,GoldsmithMT, TurnbullTL,etal.Theanterolateralligament:ananatomic, radiographic,andbiomechanicalanalysis.AmJSportsMed. 2015;43(7):1606–15.
10.CaterineS,LitchfieldR,JohnsonM,ChronikB,GetgoodA.A cadavericstudyoftheanterolateralligament:re-introducing thelateralcapsularligament.KneeSurgSportsTraumatol Arthrosc.2015;23(11):3186–95.
ligamentandanterolateralligamentreconstruction techniquewithaminimum2-yearfollow-up.AmJSports Med.2015;43(7):1598–605.
12.HelitoCP,HelitoPV,CostaHP,Bordalo-RodriguesM,PecoraJR, CamanhoGL,etal.MRIevaluationoftheanterolateral ligamentoftheknee:assessmentinroutine1.5-Tscans. SkeletalRadiol.2014;43(10):1421–7.
13.TanejaAK,MirandaFC,BragaCA,GillCM,HartmannLG, SantosDC,etal.MRIfeaturesoftheanterolateralligamentof theknee.SkeletalRadiol.2015;44(3):411.
14.HelitoCP,BonadioMB,GobbiRG,daMotaE,AlbuquerqueRF, PécoraJR,etal.Combinedintra-andextra-articular reconstructionoftheanteriorcruciateligament:the
reconstructionofthekneeanterolateralligament.Arthrosc Tech.2015;4(3):e239–44.
15.HelitoCP,DemangeMK,BonadioMB,TiricoLE,GobbiRG, PecoraJR,etal.Radiographiclandmarksforlocatingthe femoraloriginandtibialinsertionofthekneeanterolateral ligament.AmJSportsMed.2014;42(10):2356–62.
16.ClaesS,VereeckeE,MaesM,VictorJ,VerdonkP,BellemansJ. Anatomyoftheanterolateralligamentoftheknee.JAnat. 2013;223(4):321–8.