w w w . r b o . o r g . b r
Original
Article
Preoperative
planning
of
primary
total
hip
arthroplasty
using
conventional
radiographs
夽
,
夽夽
Edson
Hidenori
Miashiro
a,∗,
Edson
Noboru
Fujiki
b,
Eduardo
Nagashigue
Yamaguchi
b,
Takeshi
Chikude
b,
Luiz
Henrique
Silveira
Rodrigues
b,
Gustavo
Martins
Fontes
b,
Fausto
Boccatto
Rosa
baUniversidadeEstadualdeLondrina,Londrina,PR,Brazil
bOrthopedicsClinic,HospitalEstadualMárioCovas,FaculdadedeMedicinadoABC(FMABC),SantoAndré,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received11October2012
Accepted5December2012
Availableonline2April2014
Keywords:
Hiparthroplasty
Planning
Hipradiography
a
b
s
t
r
a
c
t
Objective:theobjectiveofthisstudywastopresentananalogmethodforpreoperative
plan-ningofprimarytotalhiparthroplastyproceduresbasedonmeasuringthecomponentsby
overlayingthetransparenciesoftheprosthesisonthepreoperativeradiographsand
check-ingtheaccuracy,bothforpredictingthesizeoftheacetabularandfemoralcomponents
usedandforrestoringtheoffsetandcorrectingthedysmetria.
Methods:betweenMarch2005andJuly2009,56primarytotalhiparthroplastyprocedures
performedon56patientsattheMarioCovasStateHospitalinSantoAndréwereanalyzed.
Themeasurementsonthefemoralandacetabularcomponentsobtainedthroughplanning
werecomparedwiththosethatwereusedinthesurgery.Theoffsetsmeasuredthrough
thepreoperativeplanningwerecomparedwiththosemeasuredonthepostoperative
radio-graphs.Dysmetriawasevaluatedbeforeandaftertheoperation.
Results:accuracyof78.6%(p<0.001)inpredictingthesizeoftheacetabularcomponentand
82.2%(p<0.001)inpredictingthefemoralnailwasobserved.Theoffsetsmeasuredthrough
preoperativeplanningwerestatisticallysimilartotheoffsetsmeasuredonthepostoperative
radiographs.Aftertheoperation,weobservedabsoluteequalizationin48.2%ofthecases.
In87.5%,thedysmetriawaslessthanorequalto1cmandin69.6%,itwaslessthanorequal
to0.5cm.
Conclusions:theaccuracywas78.6%and82.2%,respectively,fortheacetabularandfemoral
components.Theoffsetsthatwereplannedpreoperativelywerestatisticallysimilartothose
measuredonpostoperativeradiographs.Wefoundabsoluteequalizationin48.2%ofthe
cases.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora
Ltda.Allrightsreserved.
夽
Pleasecitethisarticleas:MiashiroEH,FujikibEN,YamaguchibEN,ChikudebT,RodriguesbLHS,FontesbGM,etal.Planejamento
pré-operatóriodeartroplastiastotaisprimáriasdequadrilcomousoderadiografiasconvencionais.RevBrasOrtop.2014;49:140–148.
夽夽
WorkperformedatHospitalEstadualMárioCovas,FaculdadedeMedicinadoABC(FMABC),SantoAndré,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](E.H.Miashiro).
2255-4971/$–seefrontmatter©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditoraLtda.Allrightsreserved.
Planejamento
pré-operatório
de
artroplastias
totais
primárias
de
quadril
com
o
uso
de
radiografias
convencionais
Palavras-chave:
Artroplastiadequadril
Planejamento Quadril/radiografia
r
e
s
u
m
o
Objetivos:apresentarummétodoanalógicodeplanejamentopré-operatóriodeartroplastias
totaisprimáriasdequadrilbaseadonamedidadoscomponentespelasobreposic¸ãodas
transparênciasdaprótesesobrearadiografiapré-operatória.Everificaraacurácia,tantona
previsãodotamanhodocomponenteacetabularedocomponentefemoralusadocomona
restaurac¸ãodooffsetenacorrec¸ãodasdismetrias.
Métodos: entremarc¸ode2005e julhode 2009foramanalisadas56artroplastias totais
primáriasdequadrilfeitasem56pacientesnoHospitalEstadualMárioCovas.As
medi-dasdoscomponentesfemoraiseacetabularesobtidasnoplanejamentoforamcomparadas
comasqueforamusadasnacirurgia.Osoffsetmedidosnoplanejamentopré-operatório
foramcomparadoscomosmedidosnaradiografiapós-operatória.Adismetriafoiavaliada
nosmomentospréepós-operatórios.
Resultados: foi observadaumaacurácia de78,6%(p<0,001)naprevisão dotamanhodo
componenteacetabularede82,2%(p<0,001)naprevisãodahastefemoral.Osoffsetmedidos
noplanejamentopré-operatórioforamestatisticamentesemelhantesaosoffsetmedidosna
radiografiapós-operatória.Nopós-operatórioobservamosaequalizac¸ãoabsolutaem48,2%
doscasos.Em87,5%adismetriafoiigualaoumenordoque1cmeem69,6%foiigualaou
menordoque0,5cm.
Conclusões: aacuráciafoide78,6%e82,2%,respectivamente,paraoscomponentes
acetab-ularesefemorais.Osoffsetplanejadospré-operatórioforamestaticamentesemelhantes
aosmedidosnaradiografiapós-operatória.Verificamosequalizac¸ãoabsolutaem48,2%dos
casos.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier
EditoraLtda.Todososdireitosreservados.
Introduction
Preoperative planning for hip arthroplasty procedures was
initially poorly understood and used, since the designs
and sizes of the prostheses were very limited.1,2 Today,
the variety of designs and the number of sizes of the
components have increased considerably, and total hip
arthroplasty has been transformed into a more complex
procedure.2
Preoperativeplanningmakesitpossibletoappropriately
choosethesizesofthecomponents,equalizethelimbsand
reducethedurationoftheoperation.2
Charnley1 demonstrated theimportance ofpreoperative
radiographicstudiesforchoosingthecorrectsizeofthe
pros-thesiscomponents,andalsoemphasizedtheimportanceof
restoringtheoffset.Thelatterisdirectlyrelatedtothestability
ofthearthroplasty.1,3–6
Dysmetriaisafrequentcomplicationoftotalhip
arthro-plasty.Itcauseslumbalgia,gait disordersand sciaticnerve
injuries.7–11
In this study, using conventional radiographs, we
present a preoperative planning method for primary
total hip arthroplasty based on measuring the
compo-nents through overlaying transparencies of the prosthesis
on the preoperative radiograph. The study had the
fol-lowing objectives: to assess the accuracy of predicting
the sizes of the acetabular and femoral components; to
analyze the restoration of the offset; and to correct the
dysmetria.
Material
and
methods
TheprojectforthisstudywasapprovedbytheEthics
Commit-teeoftheABCMedicalSchool,underthenumberCEP258/2007.
Between March2005and July2009,56primarytotal hip
arthroplastyproceduresperformedon56patientsatHospital
EstadualMárioCovaswereanalyzed.
Themeanagewas65years.Inall,37patients(66.1%)were
femaleand19(33.9%)weremale.Allthepatientshada
diag-nosisofarthrosis.
The inclusion criterion was the presence of unilateral
hiparthrosis.Theexclusioncriteriawerebilateralarthrosis;
moderate or severe acetabularprotrusion according to the
Sotelo-GarzaandCharnleyclassification;12acetabular
dyspla-siagreater than CrowetypeI;13 femoralneckfracture;and
alterationsinotherjointsthatcauseddysmetria.
Allthearthroplastyproceduresweretotalandcemented,
andwereperformedusingaposteriorapproach.
Pelvicradiographswereperformedinanteroposterior(AP)
view,centeredonthepubicsymphysis,withthelowerlimbs
rotatedinternallyby15◦ andadistanceof1mbetweenthe
bulboftheapparatusandthefilm;andinlateralviewcovering
theproximalone-thirdofthefemur.
Theacetabularcomponentwasmeasuredbyoverlayingthe
acetabulartransparencyontheAPradiographofthenormal
hip,inordertochoosethenumberthatfittedtheoutlineofthe
acetabulumbest.Theparametersusedweretheupperlateral
borderoftheacetabulum,theteardropandKöhler’siliosciatic
Fig.1–(A)Overlayingthetransparencyoftheacetabular componentonthenormalside.Thewhitearrowontheleft sideindicatestheupperlateralborderoftheacetabulum. Thewhitearrowontherightsideindicatestheteardrop. Thecenterofrotation(CR)ofthehipismarkedonthe transparencyandisindicatedbytheblackarrow.(B) Köhler’siliosciaticline.ThewhitearrowindicatesKöhler’s iliosciaticline.Thesizeoftheacetabularcomponent shouldnotgobeyondtheiliosciaticline.Theblackarrow indicatesthecenterofrotation.
determinedsuchthatitwouldnotgobeyondtheiliosciatic
line(Fig.1B).
Afterthecenterofrotation(CR)ofthenormalhiphadbeen
markedontheradiograph(Fig.1AandB),itwastransferred
tothesidetobeoperated.Totransferit,threereferencelines
wereusedasparameters:
LineH:goingalongthelowerlimitoftheteardrops(Fig.2A)
LineV1:goingalongthelateralborderoftheteardroponthe
normalsideandperpendicularlytotheintersectionwithline
H(Fig.2A)
LineV2:goingalongthelateralborderoftheteardroponthe
sidetobeoperatedandperpendicularlytotheintersection
withlineH(Fig.2A)
Fromthereferencelines,theCRwastransferredfromthe
normaltotheaffectedside.Wethendefinedfourdistances
measuredinmillimeters:
Fig.2–(A)ReferencelinesH,V1andV2.Thecenterof rotationismarkedonthenormalside,indicatedbyan arrow.Referencelines:thefirstgoesalongtheloweredge oftheteardrops(lineH);thesecondisperpendiculartoline Handgoesalongthelateraledgeoftheteardroponthe normalside(lineV1);thethirdisalsoperpendiculartoline Handgoesalongthelateraledgeoftheteardroponthe sidetobeoperated(lineV2).(B)TransferoftheCRfromthe rightside(normal)totheleftside.Distanceashouldbe equaltoa′anddistancebshouldbeequaltob′.
Distancea:fromtheCRofthenormalsidetolineV1(Fig.2B);
Distanceb:fromtheCRofthenormalsidetolineH(Fig.2B);
Distancea′: samelengthasdistancea,startingatlineV2
(Fig.2B);
Distance b′: same lengthas distanceb, startingatline H
(Fig.2B).
Theintersectionpointbetweenthedistancesa′andb′was
theCRofthesidetobeoperated.
Thefemoraloffsetwasthedistancealongalinegoing
per-pendicularlyfromthecenterofrotationofthefemoralhead
totheintersectionwithalinegoingthroughthemiddleofthe
longaxisofthefemur.14
The offset of the prosthesis was the distance from a
Fig.3–Offsetoftheprosthesis.
prosthesisheadtotheintersectionwithalinegoingthrough
themiddleofthemajorlongitudinalaxisofthefemoralnail
(Fig.3).
Tochoosethesizeofthe femoralcomponent,its
trans-parencywasoverlaidontheAPradiographonthesidetobe
operated(Fig.4).Thefemoralcomponentchosenwas
deter-minedtobetheonewithanoffsetclosesttothatofthenormal
side.
Thedysmetriacouldbeoneofthreetypes:atthecostofthe
femur,atthecostoftheacetabulumoratthecostofboththe
femurandtheacetabulum(mixedorcombined).15Toidentify
Fig.4–Measurementusingthetransparency.
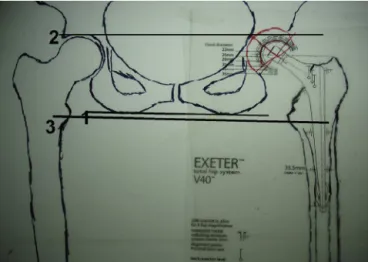
Fig.5–Normalhips.Line1goesalongthelowerlimitof thesciatictuberosities.Line2goesalongtheupperlateral edgeoftheacetabula.Line3goesthroughthemidpointof thelessertrochanters.Thethreelinesareparallel.
dysmetria, theparametersusedwerethreelinesontheAP
radiographofthepelvis,centeredonthepubicsymphysis:15
Line1:determinedbytracingoutastraightlinethroughthe
mostdistalpointsofthesciatictuberosities;
Line2:determinedbytracingoutastraightlinealongthe
upperlateraledgeoftheacetabula;
Line3:determinedbytracingoutastraightlinethroughthe
midpointsofthelessertrochanters.
Innormalhips,thethreelinesareparallel(Fig.5).
Tomeasurethedysmetria,theparametersusedwereline
H,going along the lower limitofthe teardrops, and line3
(Fig.6).
Thepelviswiththeacetabularcomponentchosen,the
cal-culatedCRandthefemurtobeoperatedweredrawnusing
Dysmetria = a–b
Fig.7–Thewhitearrowindicatesthedrawingofthepelvis withtheacetabularcomponent.Theblackarrowindicates thedrawingofthefemur.
tracingpaperoverlainontheAPradiograph(Fig.7).The
draw-ingofthepelviswasthenoverlainonthedrawingofthefemur,
and bothof thesewere placedon the transparency ofthe
femoralcomponent(Fig.8).
Theleveloftheosteotomyofthefemoralneckfor
equaliz-ingthelimbswasdefinedbyslidingthedrawingsacrossthe
femoraltransparency.Forthis,lines1,2and3hadtobekept
parallel(Fig.8).
Thechi-squaretestwasappliedtoascertaintheaccuracy
ofthepredictionsfortheacetabularandfemoralcomponents.
TheMann–Whitneytestwasappliedtocomparetheplanned
offsetmeasurementswiththoseobtainedonthe
postopera-tiveradiograph.
Dysmetriawasanalyzedaftertheoperation.
Weused the Statistical Package for the Social Sciences
(SPSS),version17.0,toobtainresultsofastatisticalnature.
Results
Accuracy of 78.6% (p<0.001) in predicting the size of the
acetabularcomponent was observed (Table 1). Accuracyof
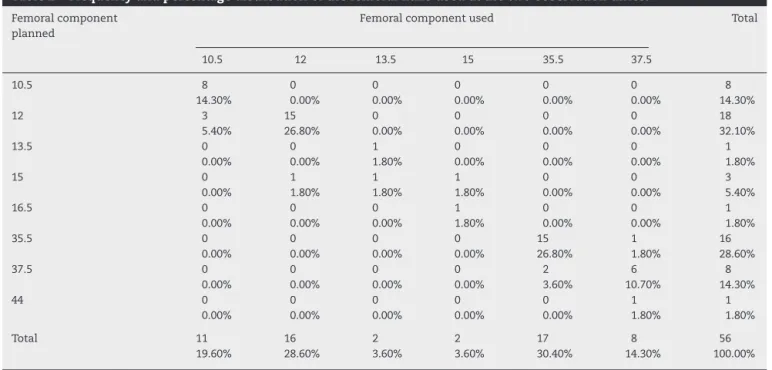
82.2% (p<0.001) in predicting the femoral nail was found
(Table2).
Fig.8–Preoperativeplanning.Lines1,2and3areparallel.
Theoffsetsmeasuredinthepreoperativeplanning were
statisticallysimilartotheoffsetsmeasuredonpostoperative
radiographs,withp=0.630(Table3).
ThemeandisplacementoftheCRwas4mminthe
hori-zontalaxisand6mmintheverticalaxis.
Themeanpreoperativedysmetriawas1.6cm,witharange
from0.0to3.9cm(Table4).Aftertheoperation,weobserved
that the limbs had been equalized in 27 patients (48.3%),
stretchedin18(32.1%)andshortenedin11(19.6%).Themean
postoperativedysmetriawas0.4cm,witharangefrom0.0to
2.1cm(Table5).Weobservedthatthepostoperativedysmetria
waslessthanorequalto1.0cmin87.5%ofthepatientsand
lessthanorequalto0.5cmin69.6%.
Withregardtothefemoralnail,itwasobservedtobe
pos-itioned neutrallyin43 hips(76.7%),withvalgusrotationin
three(5.4%)andwithvarusrotationin10(17.9%).
Theanalysisofthemeaninclinationoftheacetabular
com-ponentinthefrontalplaneshowedthatthiswas42◦,witha
rangefrom30◦to58◦.
Thevariationsintheoffsetonpostoperativeradiographs
in relation to what was planned were statistically similar
(p=0.123),withregardtoneutral,varusandvalguspositions
ofthefemoralnail.
The correlation betweenvariations inthe postoperative
offsetvaluesrelativetowhatwasplannedandtheinclination
oftheacetabularcomponentwasnotstatisticallysignificant
(p=0.657).
Discussion
During the 1970s, only limited numbers of implants were
placed.2,16 Today, there are several different designsand a
large number of sizes available,17 which makes planning
essential.2,16 However,fewstudieshaveevaluatedthe
accu-racyofcomponentsizepredictions.2,6,16,18,19
Webeganthisinvestigationwiththeaimofevaluatingthe
methodusedinourinstitution.
Today,planningmethodsusingdigitalradiographsexist.
These enable high precision,6,20 as demonstrated by Eggli
etal.,6whoobservedaccuracyofaround90%incomponent
predictions.
InBrazil,digitalradiographsarestillnotusedroutinely.The
methoddescribedinourstudy waslessprecise,butcanbe
appliedtoconventionalradiographswithoutadditionalcost
fortheprocedure.
Inoursample,weobservedthattheaccuracywas78.6%for
theacetabularcomponentsand82.2%forthefemoral
com-ponents. These values were similar to those presentedby
Paniegoetal.,2whofoundaccuraciesof83%forthe
acetab-ularcomponentsand76%forthefemoralcomponents;andto
thosereportedbyGonzálezDellaValleetal.,16whoobserved
accuraciesof83%and78%,respectively,fortheacetabularand
femoralcomponents.Bothoftheauthorgroupsusedplanning
methodswithconventionalradiographs.
Itisdifficulttopredicttheexactmagnificationin
conven-tionalradiographs.Forthisreason,inordertominimizethe
possibledeviations,westandardizedproductionofthe
Table1–Frequencyandpercentagedistributionoftheacetabularcomponentsusedatthetwoobservationtimes.
Acetabularcomponent planned
Acetabularcomponentused Total
44 48 50 52
44 18 0 0 0 18
32.10% 0.00% 0.00% 0.00% 32.10%
48 0 20 0 0 20
0.00% 35.70% 0.00% 0.00% 35.70%
50 0 1 3 0 4
0.00% 1.80% 5.40% 0.00% 7.10%
52 0 5 1 3 9
0.00% 8.90% 1.80% 5.40% 16.10%
54 0 0 0 3 3
0.00% 0.00% 0.00% 5.40% 5.40%
56 0 0 1 1 2
0.00% 0.00% 1.80% 1.80% 3.60%
Total 18 26 5 7 56
32.10% 46.40% 8.90% 12.50% 100.00%
Source:HospitalEstadualMárioCovas.
Table2–Frequencyandpercentagedistributionofthefemoralnailsusedatthetwoobservationtimes.
Femoralcomponent planned
Femoralcomponentused Total
10.5 12 13.5 15 35.5 37.5
10.5 8 0 0 0 0 0 8
14.30% 0.00% 0.00% 0.00% 0.00% 0.00% 14.30%
12 3 15 0 0 0 0 18
5.40% 26.80% 0.00% 0.00% 0.00% 0.00% 32.10%
13.5 0 0 1 0 0 0 1
0.00% 0.00% 1.80% 0.00% 0.00% 0.00% 1.80%
15 0 1 1 1 0 0 3
0.00% 1.80% 1.80% 1.80% 0.00% 0.00% 5.40%
16.5 0 0 0 1 0 0 1
0.00% 0.00% 0.00% 1.80% 0.00% 0.00% 1.80%
35.5 0 0 0 0 15 1 16
0.00% 0.00% 0.00% 0.00% 26.80% 1.80% 28.60%
37.5 0 0 0 0 2 6 8
0.00% 0.00% 0.00% 0.00% 3.60% 10.70% 14.30%
44 0 0 0 0 0 1 1
0.00% 0.00% 0.00% 0.00% 0.00% 1.80% 1.80%
Total 11 16 2 2 17 8 56
19.60% 28.60% 3.60% 3.60% 30.40% 14.30% 100.00%
Source:HospitalEstadualMárioCovas.
Arthroplasty procedures aim to restore the hip biome-chanicstonormalconditions,throughchoosingappropriate prosthesissizes, so as toavoid intraoperativeand postop-erativecomplicationsandconsequentlyincreaseprosthesis longevity.
Theimportanceoftheoffsetisrelatedtothefunctioningof theabductormusculature:1,4,5,21throughplanning,itis
possi-bletorestoreit.1,3–6,21,22Itsrestorationisrelatedtothestability
ofthearthroplasty.1,3,6,21Theoffsetsmeasuredinthe
preop-erative planningin oursamplewere statisticallysimilarto
Table3–Descriptionofandcomparisonbetweentheoffsetsplannedandused.
Pairofvariables n Mean Standard deviation
Minimum Maximum 25th
percentile
Median 75th
percentile
Significance (p)
Offsetplanned(mm) 56 39.7 5.4 30.0 55.0 35.0 38.5 42.0 0.630
Offsetused(mm) 56 40.3 6.4 30.0 57.0 35.0 39.0 45.0
Table4–Descriptionoftheaffectedlowerlimbbeforetheoperation.
Lengthofaffectedlower limbbeforethe operation(cm)
n Mean Standard
deviation
Minimum Maximum 25th
percentile
Median 75th
percentile
Shortened 53 1.7 0.9 0.4 3.9 1.0 1.5 2.3
Equalized 3 0.0 0.0 0.0 0.0 0.0 0.0 0.0
Total 56 1.6 0.9 0.0 3.9 0.9 1.5 2.2
Source:HospitalEstadualMárioCovas.
Table5–Descriptionoftheaffectedlowerlimbaftertheoperation.
Lengthofaffectedlower limbbeforethe operation(cm)
n Mean Standard
deviation
Minimum Maximum 25th
percentile
Median 75th
percentile
Shortened 11 0.9 0.7 0.3 2.1 0.4 0.8 1.7
Stretched 18 0.7 0.3 0.4 1.5 0.5 0.6 1.0
Equalized 27 0.0 0.0 0.0 0.0 0.0 0.0 0.0
Total 56 0.4 0.5 0.0 2.1 0.0 0.3 0.6
Source:HospitalEstadualMárioCovas.
thosemeasuredonpostoperativeradiographs.Thisisrelated totheaccuracyof82.2%inpredictingthesizeofthefemoral nails,whichhadfixedoffsetvalues.Therefore,ifthesizeof thefemoralcomponentiscorrect,thereisagreaterlikelihood ofachievingtheplannedoffset.
In1988,Yoderetal.23observedgreaterratesofloosening
ofthefemoralcomponentwhentheacetabularcomponent
wasplacedaboveandlaterallytothecenterofrotation.In
1996,Pagnanoetal.24observedgreaterratesoflooseningof
theacetabularandfemoralcomponentswhenthe
acetabu-larcomponentwasplacedabovethecenterofrotation,even
withoutlateraldisplacement.Inoursample,meanvariations
fromtheplannedcenterofrotationwere4mminthe
hori-zontalaxisand6mmintheverticalaxis.Thesewerecloseto
whatwaspresentedbyPaniegoetal.,2whoobservedthat96%
ofthecentersofrotationwereplacedwithdisplacementof
lessthan4mmfromtheplannedcenterofrotation.Itseems
tousthat thechangesinpositionofthe centerofrotation
aredifficulttomeasure,sincetheycanvarygreatlywiththe
magnificationofconventionalradiographs,giventhatthese
changesaremeasuredinmillimeters.Yoderetal.23observed
that measurements of4–5mmare very imprecise on
con-ventionalradiographs,whichexplainsthegreateraccuracyof
planningwhendigitalradiographsareused.
Insituationsinwhichtheacetabulumpresentslossofbone
stockordysplasia,placementoftheacetabularcomponentat
thecenter ofidealrotationismoredifficult,sinceinthese
casesadditionalcoveragewithgraftsfromthefemoralhead
maybeneeded.Thesecaseswereexcludedfromourstudy,
sincetheycouldhaveledtobiasintheanalysison
displace-mentofthecenterofrotation.
Dysmetria is a common complication following hip
arthroplasty.7–9 Itscorrectioncanbeenvisagedthrough
pre-operativeplanning1,3,6,21andalsoduringtheoperation.8The
operatedside oftenbecomes stretched.7 Dysmetria greater
than1cmhasbeencorrelated withlumbalgia.9 Ourresults
wereinferiortothosepresentedbyEgglietal.,6whoobserved
dysmetriaoflessthan5mmin94%ofthecases.Inour
sam-ple,weobservedabsoluteequalizationin48.2%ofthecases.
In87.5%,thedysmetriawaslessthanorequalto10mmand
in69.6%itwaslessthanorequalto5mm.However,itneeds
tobetakenintoconsiderationthatthestudybyEgglietal.6
wasconductedusingdigitalradiographs.
Dolhain etal.5 reportedthatvarus orvalguspositioning
of the femoraland acetabular components influenced the
offset of the arthroplasty. In our sample, the relationship
betweenthevaluesofincreased,decreasedandequalized
off-setachievedaftertheoperationthroughputtingthefemoral
component into a varus, valgus or neutral position was
analyzed.Itwasobservedthattherewerenostatistically
sig-nificantdifferencesbetweenthecategoriesofthevariableof
femoralnailposition(p=0.123).Thefemoralnailwasplacedin
aneutralpositionin76.7%ofthecases,invarusin17.9%and
invalgusin5.4%.However,inthecasesinwhichweobserved
valgusorvaruspositioning,thesewereslighterrorsthatdid
notgiverisetoanysignificantvariationsinoffset.
Going againstwhat wasobservedbyDolhainet al.,5 we
foundfromoursamplethatthevariationsinoffsetwerenot
relatedtothevariationsininclinationoftheacetabular
com-ponent.
Dobzyniacetal.25determinedthattheidealforthefemoral
componentwastopositionthenailinneutralinthefrontal
plane,with20◦to30◦ofanteversionandneutralposition.For
theacetabularcomponent,itshouldbe45◦ofabductionand
20◦to30◦ofanteversion.Lewinnecketal.11definedasafety
zonefortheacetabularcomponentcomprisinganinclination
of30◦to50◦,inthefrontalplane,andanteversionof5◦to25◦.
Inoursample,theacetabularcomponentwaspositionedwith
ameaninclinationinthefrontalplaneof42◦,witharange
from30◦to58◦.
Toobtaingreaterprecisioninpositioningprosthesis
com-ponents,computer-aidednavigationsystemsweredeveloped,
thus enabling lower variationinpositioning theacetabular
costisstillhighinBrazil.Inourstudy,themeaninclinationof
theacetabularcomponentinthefrontalplanewas42◦,witha
rangefrom32◦to58◦.Thisvariationwasgreaterthanwhathas
beenpresentedusingcomputer-aidednavigationsystems.
The preoperative planning enabled greater precision in
choosingthesizesoftheacetabularandfemoralcomponents
andfacilitatedcorrectionofthedysmetria.Itmadeit
possi-bletopredictintraoperativedifficultiessuchastheneedfor
femoralheadbonegraftingforadditionalgraft coverage in
casesofacetabulardysplasia,theneedforinsituosteotomy
ofthefemoralneckincasesofsevereacetabularprotrusion
andtheneedforsmallcomponentsinshortpatients.Itmade
itpossibletochooseafemoralcomponentforrestoringthe
offset,andtodeterminetheidealcenterofrotationonthe
affectedside.
Conclusions
a) Weobservedaccuracyof78.5%and82.2%,respectively,for
theacetabularandfemoralcomponents;
b) The offsets measured during the preoperative planning
werestatisticallysimilartothosemeasuredonthe
post-operativeradiographs;
c) Therewasabsoluteequalizationin48.2%ofthecases.In
87.5%,thedysmetriawaslessthanorequalto1cmandin
69.6%itwaslessthanorequalto0.5cm.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
Weare gratefulforcollaborationfrom ProfessorsGiancarlo
Polesello, Sérgio Mainine, Alberto Miyazaki and Joel
Mura-chovski,whoseopinionswerefundamentalindrawingupthis
study.
r
e
f
e
r
e
n
c
e
s
1. CharnleyJ.Lowfrictionarthroplastyofthehip.NewYork: Springer-Verlag;1979.
2. PaniegoG,ButtaroM,GonzálezDellaValleA,PiccalugaF. Utilidadepredictibilidaddeummétododeplaneamiento preoperatorioparalaartroplastiatotaldecadera.RevAsoc ArgentOrtopTraumatol.2004;69(1):6–12.
3. BonoJV.Digitaltemplatingintotalhiparthroplasty.JBone JointSurgAm.2004;86Suppl.2:118–22.
4. CharlesMN,BourneRB,DaveyJR,GreenwaldAS,MorreyBF, RorabeckCH.Soft-tissuebalancingofthehip:theroleof femoraloffsetrestoration.InstrCourseLect.2005;54:131–41.
5. DolhainP,TsigarasH,BourneRB,RorabeckCH,MacDonaldS, McCaldenR.Theeffectivenessofdualoffsetstemsin restoringoffsetduringtotalhipreplacement.ActaOrthop Belg.2002;68(5):490–9.
6. EggliS,PisanM,MüllerME.Thevalueofpreoperative planningfortotalhiparthroplasty.JBoneJointSurgBr. 1998;80(3):382–90.
7.KonyvesA,BannisterGC.Theimportanceofleglength discrepancyaftertotalhiparthroplasty.JBoneJointSurgBr. 2005;87(2):155–7.
8.McGeeHM,ScottJH.Asimplemethodofobtainingequalleg lengthintotalhiparthroplasty.ClinOrthopRelatRes. 1985;(194):269–70.
9.JastyM,WebsterW,HarrisW.Managementoflimblength inequalityduringtotalhipreplacement.ClinOrthopRelat Res.1996;(333):165–71.
10.TurulaKB,FribergO,LindholmTS,TallrothK,VankkaE.Leg lengthinequalityaftertotalhiparthroplasty.ClinOrthop RelatRes.1986;(202):163–8.
11.LewinnekGE,LewisJL,TarrR,CompereCL,ZimmermanJR. Dislocationsaftertotalhip-replacementarthroplasties.J BoneJointSurgAm.1978;60(2):217–20.
12.Sotelo-GarzaA,CharnleyJ.TheresultsofCharnley
arthroplastyofthehipperformedforprotrusioacetabuli.Clin OrthopRelatRes.1978;(132):12–8.
13.CroweJF,ManiVJ,RanawatCS.Totalhipreplacementin congenitaldislocationanddysplasiaofthehip.JBoneJoint SurgAm.1979;61(1):15–23.
14.LecerfG,FessyMH,PhilippotR,MassinP,GiraudF,FlecherX, etal.Femoraloffset:anatomicalconcept,definition, assessment,implicationsforpreoperativetemplatingand hiparthroplasty.RevChirOrthopTraumatol.2009;95(3): 210–9.
15.CabralFP,RondinelliPC,CôrtesS.Artroplastiatotaldo quadril:planejamentopré-operatório.In:RondinelliPC, editor.Oquadrildoadulto.SãoPaulo:Medsi;2001.p.1089–91 [ClínicaOrtopédica,v2,n.◦.4].
16.GonzálezDellaValleA,SlullitelG,PiccalugaF,SalvatiEA.The precisionandusefulnessofpreoperativeplanningfor cementedandhybridprimarytotalhiparthroplasty.J Arthroplasty.2005;20(1):51–8.
17.MassinP,GeaisL,AstoinE,SimondiM,LavasteF.The anatomicbasisfortheconceptoflateralizedfemoralstems:a frontalplaneradiographicstudyoftheproximalfemur.J Arthroplasty.2000;15(1):93–101.
18.CarterLW,StovallDO,YoungTR.Determinationofaccuracy ofpreoperativetemplatingofnoncementedfemoral prostheses.JArthroplasty.1995;10(4):507–13.
19.KnightJL,AtwaterRD.Preoperativeplanningfortotalhip arthroplasty.Quantitatingitsutilityandprecision.J Arthroplasty.1992;7Suppl.:403–9.
20.OddyMJ,JonesMJ,PendegrassCJ,PillingJR,WimhurstJA. Assessmentofreproducibilityandaccuracyintemplating hybridtotalhiparthroplastyusingdigitalradiographs.JBone JointSurgBr.2006;88(5):581–5.
21.LinclauL,DokterG,PeeneP.Radiologicalaspectsin preoperativeplanningandpostoperativeassessmentof cementlesstotalhiparthroplasty.ActaOrthopBelg. 1993;59(2):163–7.
22.RittmeisterM,CallitsisC.Factorsinfluencingcuporientation in500consecutivetotalhipreplacements.ClinOrthopRelat Res.2006;(445):192–6.
23.YoderSA,BrandRA,PedersenDR,O’GormanTW.Totalhip acetabularcomponentpositionaffectscomponentloosening rates.ClinOrthopRelatRes.1988;(228):79–87.
24.PagnanoW,HanssenAD,LewallenDG,ShaughnessyWJ.The effectofsuperiorplacementoftheacetabularcomponenton therateoflooseningaftertotalhiparthroplasty.JBoneJoint SurgAm.1996;78(7):1004–14.
25.DobzyniakM,FehringTK,OdumS.Earlyfailureintotalhip arthroplasty.ClinOrthopRelatRes.2006;(447):76–8.
27.SchleicherI,NoglerM,DonnellyW,SledgeJ. Acetabularplacementusinganimagelessnavigation system,acadavertrial.JBoneJointSurgBr.2004;86Suppl. 3:474.
28.DorrLD,MalikA,WanZ,LongWT,HarrisM.Precisionand biasofimagelesscomputernavigationandsurgeonestimates
foracetabularcomponentposition.ClinOrthopRelatRes. 2007;(465):92–9.