SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
article
Anatomical
and
radiological
characteristics
in
adolescent
idiopathic
scoliosis
with
surgical
indication
夽
Mauro
Costa
Morais
Tavares
Junior
a,∗,
Felipe
Ribeiro
Ledur
a,
Olavo
Biraghi
Letaif
a,
Raphael
Martus
Marcon
b,
Alexandre
Fogac¸a
Cristante
b,
Tarcisio
Eloy
Pessoa
de
Barros
Filho
baUniversidadedeSãoPaulo,FaculdadedeMedicina,HospitaldasClínicas,InstitutodeOrtopediaeTraumatologia,SãoPaulo,SP,Brazil
bUniversidadedeSãoPaulo,FaculdadedeMedicina,DepartamentodeOrtopediaeTraumatologia,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received15July2016 Accepted18July2016 Availableonline28April2017
Keywords:
Scoliosis/anatomy&histology Scoliosis/radiography Adolescent
Treatmentoutcome
a
b
s
t
r
a
c
t
Objective:Thisstudyaimstoanalyzetheanatomicalandradiologicalcharacteristicsof ado-lescentidiopathicscoliosispatientswithsurgicalindication.
Methods:Retrospective, descriptive study of 100medical recordspertaining to patients includedinthegroupofscoliosiswithsurgicalindicationfromtheyears2008to2015. Descriptivestatisticswereusedforstatisticalanalysis.
Results:28patientsmettheinclusionandexclusioncriteria,andwereselectedforthestudy. Theaverageagewas15.4(SD±1.2years);intheselectedsample,thefemale/maleratio was6:1;thekyphosismeasuredindegreesbyCobbanglebetweenT5–T12hadanaverage 32.10(SD±13.37);accordingtotheLenkeclassification,themostprevalenttypewastype2, representing28.6%ofcases.
Conclusion:Themeanpatientageinthepresentstudywas15.4(SD±1.2years);themost prevalenttypewastype2intheLenkeclassification.Thereisaneedfornewanatomicaland radiologicalstudiestoelucidatethemorphologicalcharacteristicscommoninadolescent idiopathicscoliosispatients.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudyconductedatInstitutodeOrtopediaeTraumatologia,HospitaldasClínicas,FaculdadedeMedicina,UniversidadedeSãoPaulo, SãoPaulo,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](M.C.TavaresJunior). http://dx.doi.org/10.1016/j.rboe.2017.04.002
Características
anatomorradiológicas
na
escoliose
idiopática
do
adolescente
com
indicac¸ão
cirúrgica
Palavras-chave:
Escoliose/anatomia&histologia Escoliose/radiografia
Adolescente
Resultadodotratamento
r
e
s
u
m
o
Objetivo: Avaliar as características anatomorradiológicas em pacientes com escoliose idiopáticadoadolescentecomindicac¸ãocirúrgica.
Métodos: Estudodescritivoretrospectivode100prontuáriosdepacientesdogrupode esco-liosecomindicac¸ãocirúrgicade2008a2015.Aanáliseusadafoiaestatísticadescritiva.
Resultados: Preencheramoscritériosdeinclusãoeexclusão28pacienteseforam seleciona-dosparaoestudo.Amédiafoide15,4±1,2anosDP;naamostraselecionada,aproporc¸ão menina:meninofoide6:1;acifosefoimedidaemgrauspeloângulodeCobbentreT5-T12e tevecomomédia32,10◦±13,37◦DP;segundoaclassificac¸ãodeLenke,omaisprevalentefoi otipo2,observadoem28,6%doscasos.
Conclusão: Aidademédiadospacientesnopresenteestudofoide15,4anos;omais preva-lente foi otipo2da classificac¸ãode Lenke.Novos trabalhosanatomorradiológicos são necessáriosparaelucidarcaracterísticasmorfológicascomunsnospacientescomescoliose idiopáticadoadolescente.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Scoliosisisathree-dimensionaldeformityofthespinal col-umn. The main diagnostic criterion is a spinal curvature exceeding10degreesonaanteroposteriorviewradiographof thespine.1–4Adolescentidiopathicscoliosis(AIS)isacommon
conditionthataffects0.5–5% ofchildren.5 Thefemale:male
ratioranges from1.5:1to3:1, substantiallyincreasingwith age.5Theco-occurrencebetweenmonozygotictwinsishigher
than70%.1
Thediagnosis ofAIS ismade byexclusion,when other causesofscoliosis,suchasvertebralmalformationsor neu-romusculardisorders,areexcluded.1,2TheetiologyofAISis
unknown and multifactorial.1,5–7 It isvery difficult to
ade-quatelycharacterizethemorphologyofthemostimportant spinalcurvaturesinpatientswithAIS,asthereisagreat vari-abilityamongindividuals.
Someprognosticfactorsfortheprogressionofthespinal deformityare:thoraciccurveormultiplecurves,Cobbangle greater than 25 degrees atdiagnosis, and delayed skeletal maturation.8TheLenkeclassificationisoftenusedtodefine
treatment in AIS. However, even within the six standard definedcurves,therearestructuralvariationswithinthesame kindofcurve,9whatmayinterferewiththesurgicaltreatment.
Newstudiesareimportanttoelucidatetheprevalent clin-icalfeatures in patients withAIS in order toassist in the correctanatomicalandradiologicalunderstandingofthe dis-ease.Therefore,thisstudyaimedtoassesstheanatomicaland radiologicalcharacteristicsofpatientswithAISwithsurgical indication.
Material
and
methods
This was a retrospective descriptive study of 100 medical chartsofpatientsfromtheIOTHC-FM-USPscoliosisgroup,
assessed from 2008 to 2015. The inclusion criteria were: patients withAIS withsurgical indicationand presenceof apanoramicradiographofthespineinanteroposteriorand lateralview.Theexclusioncriteriawere:patientswith incom-plete registers regarding demographic data, non-walking patients,andthosewithdefinedcausesforthescoliosis.
TheclassificationsusedwereCobb angleandthe Lenke classification.Descriptivestatisticswereusedforanalysis.
Thepresent study wasapprovedbytheResearch Ethics Committeeoftheinstitution.
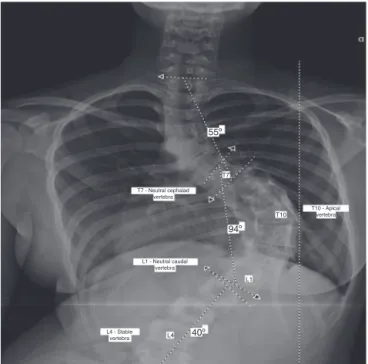
Thefollowingparameterswereassessed:patientage(in years);Cobbangle(measuredindegrees),andthefirst(most cephalad)andthelastvertebra(mostcaudal)oftheCobbangle ofthemaincurveofeachpatient;Lenkeclassificationofeach patient’scurve;neutralcephalad,neutralcaudal,andneutral apicalvertebraeofthemaincurve;andstablevertebra.The resultsareshownincharts,tables,sheets,orfigures.
Results
After 100 medical registers from scoliosis group patients treatedfrom2008to2015wereretrospectivelyanalyzed,28 mettheestablishedinclusioncriteriaandwereselected.The meanageofpatientswas15.4±1.2years(Fig.1).
Ofthe28patientsanalyzed,24weregirlsandfourwere boys,aratioof6:1.Overall,themostprevalentapicalvertebra wastheT8,in35.7%ofthecases,followedbyT9,in25%of cases.In turn,themostprevalent stablevertebraewere L4 andL3,representing25%and21.4%ofthecases,respectively (Tables1and2).Themostprevalentneutralcephaladvertebra wasT5,in32.1%ofthecases,followedbyT6,in25%.Themost prevalentneutralcaudalvertebraewereL1andL2,in35.7% and21.4%ofthecases,respectively(Tables3and4).
12
10
Frequency
Age
8
6
4
2
0
12.0 13.0 14.0 15.0 16.0 17.0
Fig.1–Patientsage.
Table1–Apicalvertebra.
Frequency Percentage Valid percentage
Accumulated percentage(%)
L3 1 3.6 3.6 3.6
T10 4 14.3 14.3 17.9
T11 2 7.1 7.1 25.0
T12 1 3.6 3.6 28.6
T6 2 7.1 7.1 35,7
T7 1 3.6 3.6 39.3
T8 10 35.7 35.7 75.0
T9 7 25.0 25.0 100.0
Total 28 100.0 100.0
Table2–Stablevertebra.
Frequency Percentage Valid percentage
Accumulated percentage(%)
L1 2 7.1 7.1 7.1
L2 2 7.1 7.1 14.3
L3 6 21.4 21.4 35.7
L4 7 25.0 25.0 60.7
L5 4 14.3 14.3 75.0
T11 4 14.3 14.3 89.3
T12 3 10.7 10.7 100.0
Total 28 100.0 100.0
Table3–Neutralcephaladvertebra.
Frequency Percentage Valid percentage
Accumulated percentage(%)
T10 1 3.6 3.6 3.6
T11 1 3.6 3.6 7.1
T3 1 3.6 3.6 10.7
T4 3 10.7 10.7 21.4
T5 9 32.1 32.1 53.6
T6 7 25.0 25.0 78.6
T7 5 17.9 17.9 96.4
T9 1 3.6 3.6 100.0
Total 28 100.0 100.0
Table4–Neutralcaudalvertebra.
Frequency Percentage Valid percentage
Accumulated percentage(%)
L1 10 35.7 35.7 35.7
L2 6 21.4 21.4 57.1
L4 1 3.6 3.6 60.7
L5 1 3.6 3.6 64.3
T11 5 17.9 17.9 82.1
T12 5 17.9 17.9 100.0
Total 28 100.0 100.0
12
10
Frequency
T5-T12 Kyphosis
8
6
4
2
0 10
5 15 20 25 30 35 40 45 50 55 60 65 70 75
Fig.2–T5–T12kyphosis.
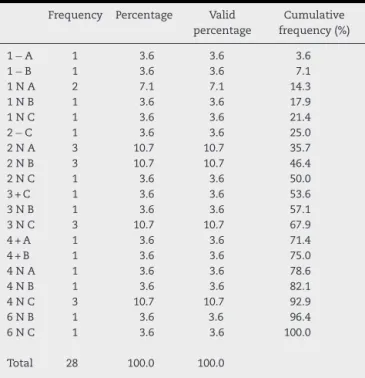
AccordingtotheLenkeclassification,themostprevalent typeofAISinthisstudywastype2,observedin28.6%ofthe cases,followedbytype4,in25.1%.Fig.3showsanexample ofthemeasurementsusedinthestudyofapatientwithAIS.
Table5–Lenkeclassification.
Frequency Percentage Valid percentage
Cumulative frequency(%)
1−A 1 3.6 3.6 3.6
1−B 1 3.6 3.6 7.1
1NA 2 7.1 7.1 14.3
1NB 1 3.6 3.6 17.9
1NC 1 3.6 3.6 21.4
2−C 1 3.6 3.6 25.0
2NA 3 10.7 10.7 35.7
2NB 3 10.7 10.7 46.4
2NC 1 3.6 3.6 50.0
3+C 1 3.6 3.6 53.6
3NB 1 3.6 3.6 57.1
3NC 3 10.7 10.7 67.9
4+A 1 3.6 3.6 71.4
4+B 1 3.6 3.6 75.0
4NA 1 3.6 3.6 78.6
4NB 1 3.6 3.6 82.1
4NC 3 10.7 10.7 92.9
6NB 1 3.6 3.6 96.4
6NC 1 3.6 3.6 100.0
Total 28 100.0 100.0
Nopatientswereclassifiedastype5inthesampleselected (Table5).
Discussion
Thepresentstudyaimedtoevaluatetheradiographic param-etersofthecurvesandepidemiologicaldataofpatientswith scoliosisinthesurgicalwaitinglistofthisinstitution.Inthe presentstudy,onlytheradiographicmethodforevaluationof theimages,whichremainsthegoldstandardforthediagnosis ofscoliosis,wasused.Regardingtheresults,previous stud-iesindicatedthattheprevalenceandseverityofthisdisease arehigheringirls,andthatthisrelationshipincreaseswith age.10Inthepresentseries,ahigherprevalenceofthedisease
ingirlswasobserved,ataratioof6girls:1boy,inagreement withtheliterature.
Amongthe numerousclassificationsystemsforAIS,the KingandLenkeclassificationsarenoteworthy.In1983,Howard Kingpresentedhisclassificationsystem,inwhichfivetypes ofcurveweredescribed.Hisworkdefinedforthefirsttime someconceptsthatarewidelyusednowadays,suchasstable vertebraandstructuralorcompensatorycurves.11 However,
alow inter- and intraobserver agreementwas reported for thatclassification.12,13In2001Lenkeetal.14publishedanew
classificationsystemforAISdefiningsixtypesofcurve;for thefirsttime,thesagittalplanedeformityofthespinal col-umnwastakenintoaccountforAISclassification.Ahigher inter-andintraobserveragreementwasobservedforthisnew classificationwhencomparedwithKing’s.14
In the present study, only the Lenke classification was used,due toits higher interobserveragreement, aiming to minimize biasfrom errors inthe classification oftypes of curvesofpatients. Inthe present sample,Lenke classifica-tion type2 curves were the most prevalent; however, the literaturefeaturestype1asthemostcommonpattern.15
ThemaintreatmentchoicesforAISaretheuseoforthoses and surgery.Themostcommonorthosesusedinthe treat-ment ofAISwithdemonstrated efficacyare theMilwaukee vestandthoraco-lumbo-sacralorthosis.16,17Themainsurgical
indicationinAISisathoraciccurveof50◦ormore,measured bytheCobbangleduringskeletalmaturation.18Therefore,the
correctclassificationandmeasurementofthedegreeof scoli-osisisparamountindeterminingthecorrecttreatmentofthe condition.
Therearenorecentstudiesintheliteraturethatindicate the distribution ofanatomical or morphological character-istics in patients with AIS. Thus, the present study has contributed toelucidatetheprevalenceofthesefindingsin the casesofAISinourinstitution, inorder tomoreclearly identifywhattypeofpatientisbeingtreated;withthecorrect diagnosis,abettertreatmentcanbeproposed.
Recentstudieshaveshownthatpelvicincidencemaybe relevantasacompensatoryorcausalfactorinthe develop-mentofscoliosis.19 Theseparameterswerenotanalyzedin
thisstudy,andmayproveimportantinfutureresearch. Fur-thermore,duetotheretrospectivecharacteristicofthestudy, alackofdataor recordingissues wereobservedinvarious charts.Ofthe100recordsanalyzed,only28mettheinclusion andexclusioncriteria,afactthathasundoubtedlyaffectedthe findingsofthestudy.Thisstudyshouldnotbegeneralizedto otherpopulations,astheselectedsamplecomprisedpatients fromanoutpatientclinicwhoalreadyhadhadsurgical indi-cation,afactthat,byitself,greatlyimpactsthefindings.
Conclusion
Inthepresentstudy,themeanageofpatientswas15.4±1.2 years.Aratioof6girls:1boywasobserved.Themeankyphosis, measuredindegreesbytheCobbanglebetweenT5andT12, was32.10◦±13.37.AccordingtotheLenkeclassification,the mostprevalenttypeofAISinthisstudywastype2,observed in28.6%ofthecases,followedbytype4,in25.1%.Nopatients wereclassifiedastype5inthesampleselected(Table5).
Newanatomoradiologicalstudiesareneededtoelucidate thecommonmorphologicfeaturesinpatientswithAIS.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.TrobischP,SuessO,SchwabF.Idiopathicscoliosis.Dtsch ArzteblInt.2010;107(49):875–83.
2.WestrickER,WardWT.Adolescentidiopathicscoliosis:5-year to20-yearevidence-basedsurgicalresults.JPediatrOrthop. 2011;311Suppl.:S61–8.
3.PanchmatiaJR,IsaacA,MuthukumarT,GibsonAJ,LehovskyJ. The10keystepsforradiographicanalysisofadolescent idiopathicscoliosis.ClinRadiol.2015;70(3):235–42. 4.AdoborRD,JorangerP,SteenH,NavrudS,BroxJI.Ahealth
5. KoniecznyMR,SenyurtH,KrauspeR.Epidemiologyof adolescentidiopathicscoliosis.JChildOrthop.2013;7(1):3–9. 6. GoodbodyCM,SankarWN,FlynnJM.Presentationof
adolescentidiopathicscoliosis:thebiggerthekid,thebigger thecurve.JPediatrOrthop.2017;37(1):41–6.
7. YamanO,DalbayrakS.Idiopathicscoliosis.TurkNeurosurg. 2014;24(5):646–57.
8. WajchenbergM,MartinsDE,LazarM.Whatisthebestwayto determinethecauseofadolescentidiopathicscoliosis?Ann TranslMed.2015;3(4):48.
9. AtmacaH,InanmazME,BalE,CaliskanI,KoseKC.Axialplane analysisofLenke1Aadolescentidiopathicscoliosisasanaid toidentifycurvecharacteristics.SpineJ.2014;14(10):2425–33. 10.SchlösserTP,vanderHeijdenGJ,VersteegAL,CasteleinRM.
Howidiopathicisadolescentidiopathicscoliosis?A systematicreviewonassociatedabnormalities.PLoSOne. 2014;9(5):e97461.
11.KingHA,MoeJH,BradfordDS,WinterRB.Theselectionof fusionlevelsinthoracicidiopathicscoliosis.JBoneJointSurg Am.1983;65(9):1302–13.
12.CummingsRJ,LovelessEA,CampbellJ,SamelsonS,MazurJM. Interobserverreliabilityandintraobserverreproducibilityof thesystemofKingetal.fortheclassificationofadolescent idiopathicscoliosis.JBoneJointSurgAm.1998;80(8):1107–11. 13.BehenskyH,GiesingerK,OgonM,KrismerM,HannesB,
KarlmeinradG,etal.Multisurgeonassessmentofcoronal
patternclassificationsystemsforadolescentidiopathic scoliosis:reliabilityanderroranalysis.Spine(PhilaPa1976). 2002;27(7):762–7.
14.LenkeLG,BetzRR,HaherTR,LappMA,MerolaAA,HarmsJ, etal.Multisurgeonassessmentofsurgicaldecision-makingin adolescentidiopathicscoliosis:curveclassification,operative approach,andfusionlevels.Spine(PhilaPa1976).
2001;26(21):2347–53.
15.LenkeLG,BetzRR,ClementsD,MerolaA,HaherT,LoweT, etal.Curveprevalenceofanewclassificationofoperative adolescentidiopathicscoliosis:doesclassificationcorrelate withtreatment?Spine(PhilaPa1976).2002;27(6):604–11. 16.BlountWP,SchmidtAC,KeeverED,LeonardET.The
Milwaukeebraceintheoperativetreatmentofscoliosis.J BoneJointSurgAm.1958;40(3):511–25.
17.WattsHG,HallJE,StanishW.TheBostonbracesystemforthe treatmentoflowthoracicandlumbarscoliosisbytheuseofa girdlewithoutsuperstructure.ClinOrthopRelatRes. 1977;(126):87–92.
18.WeinsteinSL,ZavalaDC,PonsetiIV.Idiopathicscoliosis: long-termfollow-upandprognosisinuntreatedpatients.J BoneJointSurgAm.1981;63(5):702–12.