BrazJOtorhinolaryngol.2015;81(6):671---680
www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
REVIEW
ARTICLE
Functional
magnetic
resonance
and
swallowing:
critical
literature
review
夽
,
夽夽
Maíra
Santilli
de
Lima
a,
Laura
Davison
Mangilli
b,c,
Fernanda
Chiarion
Sassi
b,d,
Claudia
Regina
Furquim
de
Andrade
e,∗aSpeechTherapyinOrofacialFunctions,SpeechTherapySupportUnit,InstitutoCentraldoHospitaldeClínicas,
FaculdadedeMedicina,UniversidadedeSãoPaulo(HCFM-USP),SãoPaulo,SP,Brazil bSciences,FaculdadedeMedicina,UniversidadedeSãoPaulo(USP),SãoPaulo,SP,Brazil
cRehabilitationScienceMedicalInvestigationLaboratory,HospitaldasClínicas,FaculdadedeMedicina,
UniversidadedeSãoPaulo(HCFM-USP),SãoPaulo,SP,Brazil
dDepartmentofPhysicalTherapy,SpeechTherapyandOccupationalTherapy,FaculdadedeMedicina,
UniversidadedeSãoPaulo(FM-USP),SãoPaulo,SP,Brazil
eFaculdadedeMedicina,UniversidadedeSãoPaulo(FM-USP),SãoPaulo,SP,Brazil
Received31March2014;accepted1February2015 Availableonline7September2015
KEYWORDS
Deglutition;
Deglutitiondisorders; Magneticresonance imaging
Abstract
Introduction:Aspectsoftheneuroanatomicalrepresentationofswallowinghavebeen inves-tigatedinhumansthroughbrainmappingtechniques,suchasfunctionalmagneticresonance imaging(fMRI).
Objective: Thiscritical qualitativereviewofthe literatureanalyzed internationalscientific publicationsinthePubMeddatabasethatinvestigatedtheactivationofthecentralnervous systeminhumansduringtheactofswallowing.
Methods:Thisinvestigationwaslimitedtoarticlesthatinvestigatedadultsolderthan18years, publishedinEnglishorPortuguese,betweenJanuary2002andDecember2013.Publicationsthat didnothaveaccesstothefulltext,thatwererepeatedbyoverlappingkeywords,casestudies, literature reviews,letters tothe editor,and thosenot directlyrelated tothe topicofthe investigationwereexcluded.
Results:Atotalof649articleswereidentified,ofwhich21matchedtheinclusioncriteria.
Conclusion: The main purpose of the manuscripts that investigate the swallowing process throughfMRIwere:tocharacterizeswallowingindifferentpathologies;tocompareswallowing indifferentagegroups;todescribebrainactivationindifferentstimulationconditions.These
夽 Pleasecitethisarticleas:deLimaMS,MangilliLD,SassiFC,deAndradeCRF.Functionalmagneticresonanceandswallowing:critical
literaturereview.BrazJOtorhinolaryngol.2015;81:671---80.
夽夽Institution:FaculdadedeMedicinadaUniversidadedeSãoPaulo(USP),SãoPaulo,SP,Brazil.
∗Correspondingauthor.
E-mail:[email protected](C.R.F.deAndrade).
http://dx.doi.org/10.1016/j.bjorl.2015.08.006
672 deLimaMSetal.
studiesindicatemultiplecorticalregionsinvolvedinswallowingcontrol.Overall,thestudies indicatethatfMRIisanon-invasiveandquantitativemethodthatallowstheinvestigationof characteristicsthatarequiteoftennotclinicallyvisible.
© 2015Associac¸ãoBrasileira de Otorrinolaringologiae CirurgiaCérvico-Facial. Publishedby ElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE
Deglutic¸ão; Transtornosde deglutic¸ão; Imagempor ressonância magnética
Ressonânciamagnéticafuncionaledeglutic¸ão:revisãocríticadaliteratura
Resumo
Introduc¸ão:Aspectos darepresentac¸ãoneuroanatômicadofuncionamento corticalque con-trolaadeglutic¸ãotêmsidoinvestigadoseidentificadosemhumanos,utilizando-setécnicasde mapeamentocerebral,comoaRessonânciaMagnéticafuncional(RNMf).
Objetivo:Estarevisãocríticaqualitativadaliteraturalevantoupublicac¸õescientíficassobrea funcionalidadedosistemanervosocentraldurantetarefasdedeglutic¸ão,pormeiodabasede dadosPubMed.
Método: Olevantamentorealizadolimitou-seasereshumanos,comidadesuperiora18anos, nosidiomasinglêseportuguês,entrejaneirode2002edezembrode2013.Publicac¸õessem acessocompleto,repetidasporsobreposic¸ãodaspalavraschave,estudosdecaso,revisõesde literatura,cartasaoeditorenãorelacionadasdiretamenteaotemaforamexcluídas.
Resultado:Identificou-se 649 estudos, sendoque somente 21 se enquadraram aos critérios estabelecidos.
Conclusão:Foramencontradosartigosqueobjetivaram,pormeiodaRNMf,estudarafunc¸ão dedeglutic¸ãoempatologias;compararadeglutic¸ãoemdiferentesidades;descreveraativac¸ão cerebralemdiferentessituac¸õesdeestimulac¸ão.Estesestudosapontammúltiplasregiões corti-caisqueparticipamnocontroledadeglutic¸ão.Conclui-sequeaRNMféummétodonãoinvasivo, quantitativo,quedemonstrarespostas,muitasvezes,nãovisíveisclinicamente.
©2015Associac¸ãoBrasileira deOtorrinolaringologiaeCirurgiaCérvico-Facial.Publicadopor ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Swallowingisacomplexsensory-motorprocessthatinvolves several physiological stages.1 The hypothesis has been
proventhatmultiplebrainareasareactivatedduring swal-lowing,bothinchildrenandadults,reflectingregionsthat are responsible for different aspects of the swallowing process.2
Itisknownthatthecerebralcortexplaysanimportant functionalroleintheregulationofswallowing.3The
reflex-ive components of swallowing depend on the brainstem swallowingcenters;theonsetof swallowingisa voluntary action,whichdependsontheintegrityofthemotorareas ofthecortex.4
Some aspects of the neuroanatomical representation of cortical function that controls swallowing have been investigatedandidentifiedinhumans,usingbrainimaging techniquessuchasthefunctionalmagneticresonance imag-ing(fMRI),consideredoneofthemostrecentandadvanced methodsoffunctionalneuroimagingwithouttheuseof ion-izingradiation.5
Theadventoffunctionalmagneticresonanceimaginghas facilitatedorabetterdetectionandquantificationof orga-nizationalchangesincorticalactivation,withimproved spa-tialandtemporalresolution.5fMRIisasafeandnon-invasive
methodtoinvestigatethehumanbrain,andhasbeen indi-catedintheinvestigationofdysphagiaafterbraindamage.6
Theaimofthisstudy wastoperformacriticalanalytic summary of relevant articles on the fMRI findings during swallowingindifferentgroupsstudiedin theinternational literature.
Methods
Since this was a non-experimental study, there was no need for consent forms or institutional ethics committee approval.TheCochraneHandbook preceptswerefollowed toestablishtheresearchmethod.7
Functionalmagneticresonanceandswallowing 673
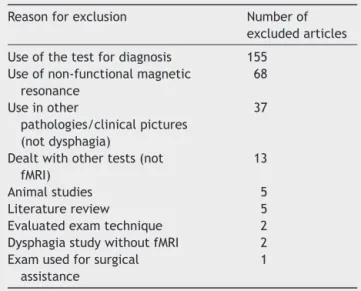
Table1 Reasonsforarticleexclusion.
Reasonforexclusion Numberof excludedarticles
Useofthetestfordiagnosis 155 Useofnon-functionalmagnetic
resonance
68
Useinother
pathologies/clinicalpictures (notdysphagia)
37
Dealtwithothertests(not fMRI)
13
Animalstudies 5
Literaturereview 5 Evaluatedexamtechnique 2 DysphagiastudywithoutfMRI 2 Examusedforsurgical
assistance
1
fMRI,functionalmagneticresonanceimaging.
excluded,aswellaspublicationsthatdidnotallowaccess tothe full text (obtainedfrom the CAPES JournalPortal) and those repeated due to overlapping keywords. Of the full texts obtained, those related to case studies, litera-turereviews,studieswithanimals,letterstotheeditor,and thosethatwerenotdirectlyrelatedtothetopicof inves-tigationwereexcluded.Textsthatwereeffectivelyrelated totheresearchtopicwereanalyzed.Allstagesofthestudy wereindependentlyconductedbytheresearchers.Incase ofdisagreementamongtheresearchers,onlytexts witha consensualfinal opinionwere included.Duetoitsnature, thiswasnotasingle-blindstudy.
After crossing ‘‘deglutition×magnetic resonance’’,
‘‘deglutition×magnetic resonance spectroscopy’’,
‘‘deglutition disorders×magnetic resonance’’, and
‘‘deglutition disorders×magnetic resonance
spec-troscopy’’,atotalof649articleswerefound,ofwhich151 hadunavailablesummaries.Oftheremaining498,189were repeated.Thus,309articleswereevaluatedandofthese, only21wereincludedinthisstudy.
Thereasonfortheexclusionof288articlesfromthestudy isshowninTable1.The21selectedarticleswerecritically evaluatedregardingthefollowing:objectives;numberand gender of participants;age range;criteriaand evaluation methods;results;andconclusions.
Results
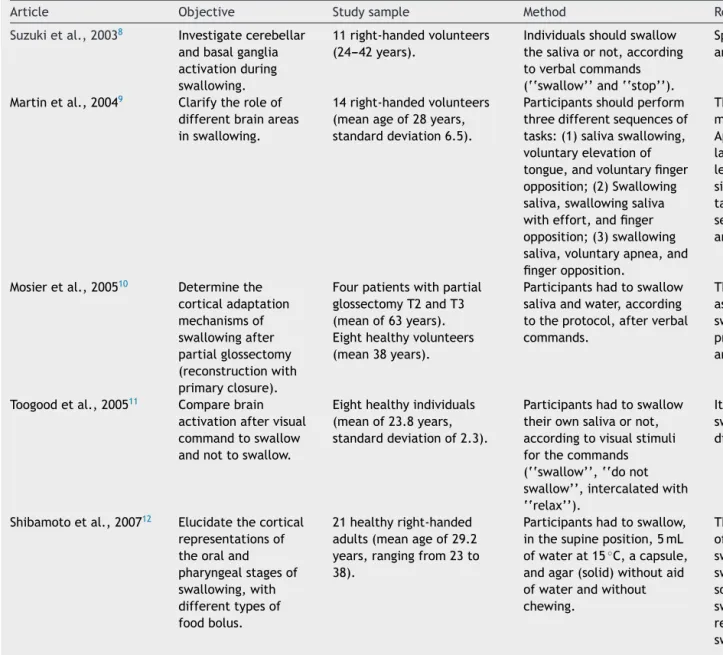
ThestudyresultsarebrieflydescribedinTable2.
Discussion
Thirteendifferentgroupsofauthorswereidentified.There was no prevalence or differentiation of results between genders.Allitemshadquantitativeanalysis,supportedby statistical results. Of the 21 selected articles,only one23
included the participationof raters,to givereliability to thevideofluoroscopicevaluation.
Of the assessed articles, nine2,10,15,17---24 used control
groupstomakecomparisons.In20articles,2,8---27 thestudy
design was cross-sectional, with evaluation/performance of a single examination, and in only one21 the design
waslongitudinal, includingthe evaluation/performanceof examinationattwodifferentmoments,i.e.,pre-and post-operatively.Accordingtothemethodologicaldesignofthis study,allarticlesusedthefMRIexam,butotherexamswere alsoused in association, such aselectromyography(EMG) andvideofluoroscopicswallowingstudy(VFSS).
TheparametersconsideredforevaluationduringthefMRI examination werenot consistent. Some studies evaluated the role of swallowing saliva, water, and barium15,16,23,24;
others,the swallowingof saliva and/or water2,9,10,13,17---21;
whereasanotherassessedtheswallowingofsolids,liquids, and semisolids to differentiate consistencies.12 Regarding
the instructions to perform the tasks, verbal commands wereused,suchas‘‘swallow’’and‘‘donot swallow’’,8,11
as well as the visual and/or auditory and/or gustatory stimulation.14,22,25---27
Ingeneral,toanalyzetheresultsofthefMRIexamination, thebloodoxygenation leveldependent (BOLD),regionsof interest(ROI), corticallateralization,anddiffusion tensor imaging(DTI)criteriawereused,aswellastimelatency.
Afteracriticalreviewofthearticles,itwasobservedthat studiesthatpresentedthefindingsoffMRIduringswallowing taskscan bedivided intothreegroups: studies describing brain activation in healthy individuals in different con-ditions and with different stimuli8,11---14,16,19,22,26,27; studies
of patients with diseases/comorbidities, who were com-paredtohealthyindividuals,10,17,18,21,23---25withthefollowing
comorbidities: Alzheimer’s disease (AD),23,24 obesity,25
tonguecancer,10,21amyotrophiclateralsclerosis(ALS),17and
ischemiccerebrovascularaccident(CVA)18;andstudies
com-paringbrainactivationatdifferentages.2,15,20,24
Forbetterpresentationanddiscussionofthestudy find-ings,thematicagglutinationwasperformedaccordingtothe abovementionedgroups.IncasesofAD,inbrief,significantly lowerresponse(BOLD)wasobservedinseveralcorticalareas thataretraditionallyinvolvedinnormalswallowing.Oneof the studies23 concluded that, while the swallowing
disor-derisgenerallyobservedinthefinalstagesofAD,changes incorticalcontrolofswallowingcanstart longbeforethe dysphagiabecomesapparent.
Studies of patients with tongue cancer10,21 sought to
determine the adaptation mechanisms of the nervous system,aftertheglossectomy.ThefMRIfindingsof glossec-tomizedpatientsshowedgreateractivationintheparietal cortexand adaptiveresponses (in cortexareasassociated withtonguemovement planningduringswallowing)ofthe CNSafterglossectomy.
The study that explored the structural and functional changesinpatientswithamyotrophiclateralsclerosis,with orwithout dysphagia17 foundthat, duringvoluntarysaliva
swallowing, all individuals had the same activated corti-calarea,butthedysphagicpatientsshowedadecreasein activation.Itwasalsodemonstratedthat,evenincasesin whichthediseasecannotbedetectedbyconventionalMRI, fMRImay disclose thealterations in brain functionduring swallowing,showingpossibleswallowingdisordersthatmay developinthefuture.
Thefindingsofarticles8,9,11---14,16,19,22,26,27 thatonly
674
de
Lima
MS
et
al.
Table2 Summaryofthearticlesusedinthisreview.
Article Objective Studysample Method ResultsandConclusions
Suzukietal.,20038 Investigatecerebellar
andbasalganglia activationduring swallowing.
11right-handedvolunteers (24---42years).
Individualsshouldswallow thesalivaornot,according toverbalcommands (‘‘swallow’’and‘‘stop’’).
Spontaneousswallowinginvolvedthebasalganglia andcerebellumaswellascorticalstructures.
Martinetal.,20049 Clarifytheroleof
differentbrainareas inswallowing.
14right-handedvolunteers (meanageof28years, standarddeviation6.5).
Participantsshouldperform threedifferentsequencesof tasks:(1)salivaswallowing, voluntaryelevationof tongue,andvoluntaryfinger opposition;(2)Swallowing saliva,swallowingsaliva witheffort,andfinger opposition;(3)swallowing saliva,voluntaryapnea,and fingeropposition.
Thisfindingsuggeststhattheseareasofthebrain maymediatespecificprocessesforswallowing. Approximately60%ofsubjectshadstrongfunctional lateralizationofthepostcentralgyrustowardthe lefthemispheretoswallow,while40%showeda similaractivationtrendforthetongueelevation task.Thisfindingsupportstheviewthattheoral sensorimotorcortexintheleftandrighthemispheres arenotfunctionallyequivalent.
Mosieretal.,200510 Determinethe
corticaladaptation mechanismsof swallowingafter partialglossectomy (reconstructionwith primaryclosure).
Fourpatientswithpartial glossectomyT2andT3 (meanof63years). Eighthealthyvolunteers (mean38years).
Participantshadtoswallow salivaandwater,according totheprotocol,afterverbal commands.
Theadaptiveresponsesinvolvecortexareas associatedwithtonguemovementplanningduring swallowing.Thisreflectsadaptivebiomechanical processesoftonguemovementduringswallowing andtonguesensitivityalterationswerenotverified.
Toogoodetal.,200511 Comparebrain
activationaftervisual commandtoswallow andnottoswallow.
Eighthealthyindividuals (meanof23.8years, standarddeviationof2.3).
Participantshadtoswallow theirownsalivaornot, accordingtovisualstimuli forthecommands (‘‘swallow’’,‘‘donot swallow’’,intercalatedwith ‘‘relax’’).
Itwasconcludedthatthe‘‘swallow’’ב‘donot
swallow’’paradigmisaneffectivemethodto differentiatecorticalareasofswallowingprocessing.
Shibamotoetal.,200712 Elucidatethecortical
representationsof theoraland pharyngealstagesof swallowing,with differenttypesof foodbolus.
21healthyright-handed adults(meanageof29.2 years,rangingfrom23to 38).
Participantshadtoswallow, inthesupineposition,5mL ofwaterat15◦C,acapsule,
andagar(solid)withoutaid ofwaterandwithout chewing.
Functional
magnetic
resonance
and
swallowing
675
Martinetal.,200713 Assesstheneural
representationsof voluntaryswallowing inhealthyelderly.
Ninehealthyelderlywomen (mean74.2years,standard deviation8.1)
Participantshadtoswallow thesalivaaccumulatedinthe mouthor3mLofwater injectedintotheoralcavity, inaccordancewiththevisual command.
Therewasafour-foldincreaseinthevolumeof cerebralactivationwhenswallowingwatercompared tosalivaswallowing,particularlytherightpremotor cortexandtheprefrontalcortex.Thisspecific activationpatternmayrepresentacompensatory responsetothedemandsofswallowingwater consideringtheage-relateddecreaseinoral sensorimotorfunction.
Lowelletal.,200814 Differentiatethe
motor,sensory planning,and componentsofmotor performanceofthe cerebralcontrolof swallowing.
14healthyindividuals,only oneleft-handed(meanage of36years,standard deviationof10.4,ranging from21to52years).
Fourconditionswere employedduringfMRI:oral sensorystimulation(air pulse),directswallowing, indirectswallowing,and apnea.Duringthe
examination,theindividuals wereaskedtoperformtasks afterreceivingavisual stimulus---symbol:(1)atube forairflow---oral-sensory stimulation,(2)alamp---for indirectswallowing,(3)a glass--- fordirectswallowing and(4)lungswithanX-ray ---forapnea.
Sensoryoralstimulationandindirectswallowing showedactivationinneuralareasrelatedtoareas activatedduringspontaneousswallowing. Itissuggestedthatoralsensorystimulationand indirectswallowinghaveimportantimplicationsfor interventioninswallowingdisordersassociatedwith neurologicaldiseases.
Humbertetal.,200915 Toassessthe
functionalalterations inswallowing accordingtoage.
11elderlyindividuals(mean ageof72.3years,standard deviationof7.5,ranging from64to83years). 12youngindividuals(mean ageof27.9years,standard deviation4,rangingfrom23 to37years).
Participantshadtoswallow saliva,water,andbarium, alternatingwithpausesin swallowing,accordingtothe commands.
Thefindingssuggestthattheelderlyindividuals showedahighercorticalinvolvementtocomplete thesameswallowingtaskswhencomparedtothe youngerones.Theelderlyshowedahigherlatencyto theonsetofpharyngealswallowingandincreased residueoftheingestedmaterialinthepharynx. Thesefindingssuggestthattheelderlyhadahigher corticalinvolvementtocompletethesame swallowingtasksthanyoungerindividuals. Kawayetal.,200916 Toinvestigatebrain
activationafter simultaneousdisplay ofstimuliassociated withswallowing movements.
12healthyandright-handed adults,withvisionand hearingwithinthenormal range(20---28years).
Auditoryandvisualstimuliof theactofswallowingand neckanatomywere presentedinassociation duringswallowing.The corticalareasactivatedwith differenttypesofstimuli wereanalyzed.
Accordingtothisstudy,theaudiovisualstimuli associatedwiththeswallowingmovementcanbe appliedinthetreatmentofpatientswithdysphagia. Theactivationofareasassociatedwiththe
676
de
Lima
MS
et
al.
Table2 (Continued)
Article Objective Studysample Method ResultsandConclusions
Lietal.,200917 Toexplorethe
structuraland functionalchangesin patientswith amyotrophiclateral sclerosis(ALS),with orwithoutdysphagia, comparedtohealthy adults.
ALSpatients,fivewith dysphagiaandfivewithout dysphagia(32---58years).
Participantsshouldswallow theirownsalivaorstopthe action,accordingtovisual commands.
Duringvoluntaryswallowingofsaliva,the preeminentfocalactivationcorrespondedtothe samecorticalareainbothgroups;however,a decreaseinactivationwasobservedinALSpatients withdysphagia
Tenindividualsmatchedfor genderandagetothestudy group.
Combined,non-invasiveneuroimagingtechniques maybeusefultoolsforassessingrehabilitation, prognosis,andstudystrategiesfordysphagicpatients withALS,particularlyforpatientsthathave
‘negative’MRIbyconventionalmethods. Lietal.,200918 Toinvestigate
neurorehabilitation mechanismsafter dysphagiainpatients withunilateral stroke,when comparedtohealthy adults.
Tenpatientsafterischemic strokewithsevere
dysphagiaforatleastthree days(meanageof70.9 years,standarddeviationof 3.4,rangingfrom62to78 years).
Tenhealthyelderly individuals(meanage70.3 years,standarddeviation 4.2,rangingfrom65to75 years).
Participantshadtoswallow theirownsalivaorstopthe action,accordingtovisual commands.
Theresultsindicatethataunilateralstrokeofeither cerebralhemispheremaycausedysphagiaand recoveryofthissymptommaybeassociatedwiththe factthatotherunaffectedareasstartbeing
activatedduringswallowing.
Malandrakietal.,200919 Toidentifyneural
activationsof differentcerebral componentsof swallowinginhealthy youngadults.
Tenhealthyyoung individuals(mean21.7 years,standarddeviationof 2).
Waterwasinjectedintothe oralcavityofthe
participants,whoshould followrandomvisual commands(‘‘swallow’’, ‘‘getreadytoswallow’’, ‘‘touchyourtongue’’, ‘‘clearyourthroat’’).
Areasactivatedduringeachofthetaskcomponents showedpartialdifferentiationofneurallocationfor theseveralcomponentsofswallowing.Thestudywas abletoidentifythebrainareasinvolvedinthe swallowingtask,inagreementwithpreviousfindings.
Malandrakietal.,201020 Toassessage
differencesin patternsofneural lateralizationduring swallowing.
Tenyoungright-handed individuals(meanageof 21.7years,standard deviationof2.1).
Nineadults(meanage70.2 years,standarddeviation 3.9)
Waterwasinjectedintothe oralcavityofthe
participants,whoshould followthecommandsthat appearedonatelevisionat random(‘‘swallow’’,‘‘get readytoswallow’’,‘‘touch yourtongue’’,‘‘clearyour throat’’).
Withincreasingage,thehemisphericcorticalcontrol ofswallowingseemstobecomemore
Functional
magnetic
resonance
and
swallowing
677
Haupageetal.,201021 TocorrelateCNS
adaptation mechanismswith changesinlanguage function.
Sixindividualsdiagnosedwith tonguecancer(meanageof50.8 years---21---66).
Ninehealthyindividuals(meanage 35.6;30---48).
Theparticipantswere evaluatedpriortosurgeryand aftersixmonthsthroughfMRI, withthreetasks:‘‘tongue touch’’,dryswallowingand waterswallowingafter auditorycommand,comparing theinter-individualactivation areas(preandpostoperative), preoperativepatientwith control,andpostoperative withcontrol.
Patientswhorecoveredtonguefunctionafter partialglossectomyshowadaptiveresponsesin theCNS.Theincreasedcorticalactivationareas aftersurgeryareinvolvedwiththeplanning,the movementandsensationofthetongueduring swallowing.Postoperativeactivationpatterns wereclosertocontrollevelsthantothe preoperativeexams.
Babaeietal.,201022 Totestwhether
activityofthe corticalswallowing networkcanbe increasedbysensory stimulirelatedto food.
14healthyandright-handed individuals(meanageof28years, standarddeviationof10).
Thesubjectsreceiveddifferent visualandolfactorycommands toperformsalivaorfood swallowing(water,lemonade, milkchocolate,and
popcorn-flavoredsolution)at sametemperature.
Signalintensityalongallsub-corticalregionsof theswallowingnetworksignificantlyincreased withstimulationwithflavor,whencomparedwith swallowingofsalivaandwater.Thesimultaneous olfactory,gustatory,andvisualstimulationof ingestedsubstancesincreasestheactivityofthe swallowingcerebralcorticalnetwork.This increaseinactivitymayhaveimplicationsinthe managementofdysphagia.
Humbertetal.,201023 Tocomparethe
neuralactivationand thephysiologyof swallowingin patientswithnewly diagnosed
Alzheimer’sdisease (AD)andhealthy individualsmatched forage.
13Alzheimerpatients(mean74.3 years,standarddeviation8.6, rangingfrom58to88).
11healthyindividuals(meanage 72.3years,standarddeviation7.5, rangingfrom64to83).
Bariumandwaterwere injectedintotheoralcavityof thepatientsandsubjects shouldswallowwhentheyfeel theentirecontentintheir mouth;aswellassalivawhen theysawthevisualcommand.
ThegroupwithADhadsignificantlylower responseinmanycorticalareasthatare
traditionallyinvolvedinnormalswallowing.They didnotrecruitnewregions,orcompensatein regionsthatarenormallyactivatedduring swallowing.Althoughswallowingdisordersare usuallyobservedinthefinalstagesofAD,changes inthecorticalcontrolofswallowingcanstartlong beforedysphagiabecomeapparent.
Humbertetal.,201124 Toassessbrain
responsesin swallowingtasks, comparingindividuals byageandthe presenceof Alzheimer’sdisease (AD),throughfMRI.
13elderlyindividualswith Alzheimer’s(meanof74.3years, standarddeviation8.6years ---range:58---88years).
12healthyyoungindividuals(mean age27.9years,standarddeviation 4.0years---range:23---37years) 11healthyelderlyindividuals(mean 72.3years,SD7.5,range:58---88 years).
Swallowingofsaliva,water, andbarium,intercalatedwith momentsofpauseinthe swallowingtaskafter predeterminedcommands.
678
de
Lima
MS
et
al.
Table2 (Continued)
Article Objective Studysample Method ResultsandConclusions
Sticeetal.,201125 Comparebrainactivation
duringfoodreceivingtasks andreceivingmonetary rewardinyoungindividuals withhighandlowriskfor obesity.
60youngindividualsof normalweight,withhigh andlowriskforobesity accordingtotheirfamily members(meanof15 years,standard
deviation2.9).Ofthese, 35hadhighriskfor obesity.
Theyoungindividualswere giventwostimuliduringthe examination:(1)stimuluswith foodreward:afterthe representationofimages---a milkshakeorwater---received therespectivefood.This stimulusoccurredaftera periodoffastingtoinduce hunger;(2)stimuluswith monetaryreward:duringa game,theparticipantreceived ‘‘money’’asareward
(figuratively).
Individualswithhighriskforobesityshow highercorticalactivationwhenreceivingthe milkshake,comparedtolow-riskones.These youngindividualsshowhighresponsivenessto circuitsconnectedtoreward,ingeneral,with highresponsivenessinthesomatosensory regionconnectedtofood,whichcanleadto overeatingthatresultin‘‘blunting’’of dopaminesignalingandhighresponsivenessto foodstimuli.
Malandrakietal.,20112 Todeterminewhether
swallowingeventsrecruit differentareasof activation,withdifferent amplitudes,comparing youngandelderly individuals.
Nineright-handed elderlyindividuals(mean 70.2years,standard deviation3.9). Tenhealthyyoung individuals(mean21.7 years,standard deviation2.1).
Waterwasinjectedintothe oralcavityoftheparticipants, whichshouldfollowthe commandsthatappearedona televisionatrandom
(‘‘swallow’’,‘‘getreadyto swallow’’,‘‘touchwithyour tongue’’,‘‘clearyour throat’’).
Therewasdecreasedactivationintheelderly comparedtoyoungindividualsduring swallowingandtheanalyzedtasks.These reductionsweresignificantinseveralprimary somatosensoryareas,indicatingadeclinein neuralprocessingofsensorysignalsto coordinatetheswallowingresponse.
Babaeietal.,201226 Toinvestigatethe
reproducibilityofpositive andnegativecortical activity(BOLD)relatedto swallowingindifferent sessionsoffMRIinregions ofinterestpreviously demonstratedinother studies.
16right-handed asymptomaticadult individualsaged20---34 years,ofwhomnine werewomen.
Aprojectionscreenwasplaced infrontofthescannerto displayvisualcues(verbal command)toswallowand/or theimageofacrossforocular fixationbetweenswallows(3s). Twoseparatesessionswere carriedout.
Functionalmagneticresonanceandswallowing 679 Babaei et al., 2013 27 To determine the functional connectivity (FC) between brain regions involved in swallowing and characterize the differences in FC between these regions when involved in different tasks (rest or control task). 16 right-handed, adult, asymptomatic individuals aged 20---34 years, of which nine were women. First the individuals had swallowing analyzed according to a protocol and then, with the aid of a screen for visual projection of commands, three different conditions were assessed: (1) swallowing task after 21 random commands to swallow; (2) ocular fixation on the image of a cross with 21 commands to relax substituting the ocular fixation mark; (3) wakefulness with eyes closed at rest. Functional connectivity of the swallowing network regions is robust and reproducible across different experimental conditions and is significantly higher during swallowing task when compared to the control of visual task or rest. SD, standard deviation; fMRI, functional magnetic resonance imaging; AD, Alzheimer ’s disease; CNS, central nervous system; TV , television; pre-op, preoperative period; post-op, postoperative period; ALS, amyotrophic lateral sclerosis; CV A, cerebrovascular accident.
toperformthetaskofswallowing,differentages,and dif-ferentcentralnervoussystemfoci---showedthefollowing: (1)higher brainactivation: during liquid swallowing com-paredtosolids;duringwaterswallowingcomparedtosaliva swallowing;whenthefoodofferedhadflavor,comparedto salivaandwater;whentherewasaverbalcommandto per-formswallowing;whenusingolfactory,gustatory,andvisual stimuliassociatedwithswallowing;andwhenusingsensory stimulationwithairinjectionintheoral cavityduringthe swallowing(comparedtothetimesin whichtherewasno injectionofair);(2)increasedactivationinareasofinterest (programmingandperformance) whenvisual andauditory stimuliassociatedwithswallowingwere usedin combina-tiontocarryoutthefunction;(3)thattheoralsensorimotor cortexintheleftandrighthemispheresarenotfunctionally equivalent;and (4) that spontaneous swallowing involves theactivationofthecerebellumandbasalganglia,aswell ascorticalstructures.
By analyzing the normal standards for brain activation duringswallowingtasks,itwasobservedthatalthoughthe contrastanalysis failed to identifythe specific activation foci for swallowing, overlapping activation maps suggest thatthemostlateralextentoftheprecentralandanterior parietalcortex,rostralanteriorcingulatecortex,precuneus and left parietal operculum are preferentially activated inswallowing.9Suzuki etal.(2003),8 however,found that
regionsactivated duringswallowing wereobserved in the sensorimotorcortex, insula, cerebellum,putamen, globus pallidus,thalamus,anteriorcingulategyrus,supplementary motorarea,superiortemporalgyrus,andinthesubstantia nigra;thecerebellumwasbilaterallyactivated,especially ontheleftside;activationoftheglobuspallidusand puta-menwasbilateral.
Inthepastfewyears,agrowingnumberof neuroimag-ingstudiesinhealthysubjectshaveshownmultiplecortical regions involved in the control of swallowing. Functional brain imaging may help to elucidate the relevant neural mechanisms, identifying the neural patterns that control thiscomplex sensory-motor action, providing evidence of functionalchangesinthecerebralcortexaftera comorbid-ity,suchasthosecitedinthisreview,helpingtoidentifyand thecorrectrehabilitationofdysphagia.
This critical review showed that the examination is of greatimportanceintheearlyidentificationofbrain alter-ations, facilitating the choice of a better rehabilitation approachfor dysphagic patients,or thoseat risk for dys-phagia,allowingimprovementoftheclinicalpictureorrisk prevention.
Conclusion
This study demonstrated that the fMRI is a non-invasive, quantitativemethodthatprovidesspecificanswers,which aresometimesnotclinicallyidentified.
680 deLimaMSetal.
inthe assessedarticles,both in caseselection and inthe studymaterialsandmethods.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Corbin-LewisK,LissJM,SciortinoKL.Controledadeglutic¸ão normal.In:Corbin-LewisK,LissJM,SciortinoKL,editors. Anato-miaclínicaefisiologiadomecanismodedeglutic¸ão.SãoPaulo: CengageLearning;2009.p.95---109.
2.MalandrakiGA,PerlmanAL,KarampinosDC,SuttonBP.Reduced somatosensoryactivationsinswallowingwithage.HumBrain Mapp.2011;32:730---43.
3.MartinRE,SessleBJ.Theroleofthecerebralcortexin swal-lowing.Dysphagia.1993;8:195---202.
4.HamdyS,RothwellJC,AzizQ,ThompsonDG.Organizationand reorganizationofhumanswallowingmotorcortex:implications forrecoveryafterstroke.ClinSci.2000;99:151---7.
5.Mosier K, Patel R, Liu WC,Kalnin A, MaldjianJ, Baredes S. Corticalrepresentationofswallowingnormaladults:functional implications.Laryngoscope.1999;109:1417---23.
6.ErtekinC,AydogduI.Neurophysiologyofswallowing.Clin Neu-rophysiol.2003;114:2226---44.
7.TheCochraneCollaborationCochranehandbookforsystematic reviewsofintervention;2011.
8.SuzukiM,AsadaY,Ito J,HayashiK,InoueH, KitanoH. Acti-vationofcerebellumandbasalgangliaonvolitionalswallowing detectedbyfunctionalmagneticresonanceimaging.Dysphagia. 2003;18:71---7.
9.MartinRE,MacIntoshBJ,SmithRC,BarrAM,StevensTK,Gati JS, et al. Cerebral areas processing swallowing and tongue movementareoverlappingbutdistinct:afunctionalmagnetic resonanceimagingstudy.JNeurophysiol.2004;92:2428---93.
10.MosierK,LiuWC,BehinB,LeeC,BaredesS.Corticaladaptation followingpartialglossectomywithprimaryclosure:implications forreconstructionoftheoraltongue.AnnOtolRhinolLaryngol. 2005;114:681---7.
11.ToogoodJA,Barr AM,StevensTK,GatiJS,Menon RS,Martin RE.Discretefunctionalcontributionsofcerebralcorticalfociin voluntaryswallowing:afunctionalmagneticresonanceimaging (fMRI)go,no-gostudy.ExpBrainRes.2005;161:81---90.
12.ShibamotoI,TanakaT,FujishimaI,KatagiriN,UematsuH. Cor-ticalactivationduringsolidbolusswallowing.JMedDentSci. 2007;54:25---30.
13.MartinR,BarrA,MacIntoshB,SmithR,StevensT,TavesD,etal. Cerebralcorticalprocessingofswallowinginolderadults.Exp BrainRes.2007;176:12---22.
14.LowellSY,PolettoCJ,Knorrr-ChungBR,ReynoldsRC,Simonyan K, Ludlow CL. Sensory stimulation activates both motor andsensorycomponentstheswallowingsystem.Neuroimage. 2008;42:285---95.
15.HumbertIA,FitzgeraldME,McLarenDG,JohnsonS,PorcaroE, KosmatkaK,etal. Neurophysiologyofswallowing:effectsof ageandbolustype.Neuroimage.2009;44:982---91.
16.Kawai T, Watanabe Y, Tonogi M, Yamane G, Abe S, Yamada Y, et al. Visual and auditory stimuli associated with swal-lowing: an fMRI study. Bull Tokyo Dent Coll. 2009;50: 169---81.
17.LiS,ChenQ,YuB,XueK,LuoC,XuY,etal.Structuraland functionalchangesmappedinthebrainsofamyotrophic lat-eralsclerosispatientswith/withoutdysphagia: apilotstudy. AmyotrophLateralScler.2009;10:280---7.
18.LiS,LuoC,YuB,YanB,GongQ,HeC,etal.Functional mag-netic resonance imagingstudy on dysphagiaafter unilateral hemisphericstroke: a preliminary study.J Neurol Neurosurg Psychiatry.2009;80:1320---9.
19.MalandrakiGA,SuttonBP,PerlmanAL,KarampinosDC,Conway C.Neuralactivationofswallowingandswallowing-relatedtasks inhealthyyoungadults:anattempttoseparatethecomponents ofdeglutition.HumBrainMapp.2009;30:3029---226.
20.MalandrakiGA,SuttonBP, PerlmanAL, Karampinos DC. Age-related differences in laterality of cortical activations in swallowing.Dysphagia.2010;25:238---49.
21.HaupageS,PeckKK,BranskiRC, HsuM,HolodnyA,KrausD. FunctionalMRIoftonguemotortasksinpatientswithtongue cancer:observationsbeforeandafterpartialglossectomy. Neu-roradiology.2010;52:1185---91.
22.BabaeiA,KernM,AntonikS,MepaniR,WardBD,LiSJ,etal. Enhancingeffectsofflavorednutritivestimulioncortical swal-lowingnetworkactivity.AmJPhysiolGastrointestLiverPhysiol. 2010;299:G422---9.
23.Humbert IA, McLaren DG, Kosmatka K, Fitzgerald M, John-son S, Porcaro E, et al. Early deficits in cortical control of swallowing inAlzheimer’s disease. JAlzheimersDis. 2010;9: 1185---97.
24.HumbertIA,McLaren DG,MalandrakiG, JohnsonSC,Robbins J. Swallowing intentional off-state in aging and Alzheimer’s disease: preliminary study. J Alzheimers Dis. 2011;26: 347---54.
25.SticeE,YokumS,BurgerKS,EpsteinLH,SmallDM.Youthatrisk forobesityshowgreateractivationofstriataland somatosen-soryregionstofood.JNeurosci.2011;23:4360---6.
26.BabaeiA,WardBD,AhmadS,PatelA,NenckaA,LiSJ,etal. Reproducibilityofswallow-inducedcorticalBOLDpositiveand negativefMRIactivity.AmJPhysiolGastrointestLiverPhysiol. 2012;303:600---9.