SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Case
Report
Reconstruction
with
iliac
pedestal
cup
and
proximal
femur
tumor
prosthesis
after
wide
resection
of
chondrosarcoma
–
10-year
follow-up
results
夽
Diogo
Lino
Moura
∗,
Rúben
Fonseca,
João
Freitas,
António
Figueiredo,
José
Casanova
CentroHospitalareUniversitáriodeCoimbra,DepartamentodeOrtopedia,Coimbra,Portugal
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received23September2016
Accepted21November2016
Availableonline30December2016
Keywords:
Boneneoplasms
Chondrosarcoma Pelvis
Reconstruction
a
b
s
t
r
a
c
t
Chondrosarcomaisamalignantcartilage-formingneoplasm.Itisdifficulttotreatbecause
ofresistancetobothchemotherapyandradiation,makingwidelocalexcisiontheonly
treat-ment.Thisreportpresentsanactive,43year-oldmanwhowasdiagnosedwithrecurrent
clearcellchondrosarcomaoftheproximalleftfemur,previouslyreconstructedwithatotal
hipprosthesis,extendingtotheweight-bearingdomeoftheacetabulum.Cancerstaging
studyrevealednosignsoftumordisseminationatdistance.Giventheexcellentfunctional
statusofthepatient,theauthorsperformedaEnneking–Dunhamtypeperiacetabularpelvic
resectionandresectedenbloc,withthetotalhipprosthesisincluding22cmofthefemur
andaportionofthehipabductorapparatus.Acetabularreconstructionwasperformedwith
anon-cementedpedestalcupprosthesisfixedattheiliac,andin-femurreconstruction
uti-lizedacementedsilver-coatedproximalfemurmodularprosthesis.Today,aftera10-year
follow-up,thepatientiswalkingwithoutcrutches,hepracticesrecreationalcyclingwithout
assistance,andheisasymptomaticandfreeoftumoraldisease.Atpresent,nosignsof
rel-evantloosening,instability,infection,heterotopicossification,oranyothercomplications
havebeenobserved.Pelvicreconstructionsarechallengingandriskysurgeries;however,the
appearanceofmorefunctionalimplants,likethepedestalcupprosthesis,anditscorrect
applicationandindication,mayallowpromisingclinicalandfunctionalresultswithlow
complicationsrate.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora
Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http://
creativecommons.org/licenses/by-nc-nd/4.0/).
夽
WorkperformedattheCoimbraHospitalandUniversityCenter,OrthopedicsDepartment,Coimbra,Portugal.
∗ Correspondingauthor.
E-mails:dflmoura@gmail.com,dflm12345@gmail.com(D.L.Moura).
http://dx.doi.org/10.1016/j.rboe.2016.11.007
2255-4971/©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditoraLtda.Thisisanopenaccessarticle
doaparelhoabdutordoquadril.Areconstruc¸ãoacetabularfoirealizadacomumaprótese
depedestalnãocimentadafixadanoilíacoeareconstruc¸ãonofêmurutilizouumaprótese
modularcimentadaparaofêmurproximalcomrevestimento emprata.Hoje,apósum
seguimentodedezanos,opacienteandasemmuletas,praticaciclismorecreativosem
assistênciaeestáassintomáticoelivrededoenc¸atumoral.Nãoforamobservadossinais
deafrouxamentorelevante,instabilidade,infecc¸ão,ossificac¸ãoheterotópicaouquaisquer
outrascomplicac¸ões.Asreconstruc¸õespélvicassãocirurgiasdifíceisearriscadas;
entre-tanto,osurgimentodeimplantesmaisfuncionais,comoaprótesedepedestal,esuacorreta
aplicac¸ãoeindicac¸ãopodempermitirresultadosclínicosefuncionaispromissores,com
baixataxadecomplicac¸ões.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier
EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http://
creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Chondrosarcomaisacartilageformingmalignneoplasm.It
is the second most common primary malignancy of bone
and is more frequent in males above 40 years old.It can
beprimaryorsecondary,frequentlyoriginatingfrombenign
tumors’malignization.Mostfrequentlocationsincludepelvis,
proximal femur and scapula. Chondrosarcoma is difficult
to treat because it is resistant to both chemotherapy and
radiation, making wide local excision the only effective
treatment.1,2Theextentoftheresectionmarginsdependson
thetumorgradeandlocation.3,4Localrecurrenceisfrequently
seenafterintralesionalexcision,thuswidelocalexcisionis
sometimesemployeddespitesignificant morbidity, evenin
low-gradelesions.Thesurgeonmustweigh theriskof
sig-nificantmorbidity withthe abilitytominimize the chance
oflocalrecurrenceandmaximizethelikelihoodoflong-term
survival.2Themostimportantpredictorsofpoorprognostic
forpatientswithchondrosarcomaareahighhistologicalgrade
andageover50yearsold.5,6
Chondrosarcoma,Ewing sarcoma and osteosarcoma are
the most frequentprimitive malignant bone tumor
affect-ing the iliac bone.7 As opposed to iliac and obturator ring
resections,iliacwingandacetabularresectionsrequire
recon-struction. This is due to the pelvic ring disruption that
affects weight bearing, demanding reconstruction to allow
ambulationandanacceptablefunctionalresult.7
Reconstruc-tion of periacetabular defects after pelvic tumorresection
ranks amongthe most challengingprocedures in
orthope-dicsurgery.7,8Currentsolutionsincludetotalhipreplacement
and reconstructionwithsaddle ormodulartumor
prosthe-sis,pedestalcupprosthesis,massiveallograftwithorwithout
prosthesisandfemoro-ilacarthrodesis.7,9Thechoiceismade
balancing the following items: remaining acetabular bone
stockqualityforprosthesisfixation;generalhealthstatusand
functionallevelofthepatient.9
Case
description
We present the caseofa 43 year-oldactive manthat was
diagnosedwitharecurrentclearcellchondrosarcomaofthe
proximalleft femur,extendingtothe weight-bearingdome
oftheacetabulum.Cancerstagingstudyrevealednosignsof
tumordisseminationtodistance.Thepatientwaspreviously
submitted in other healthcareinstitution to two curettage
resections ofbenignlocal chondrogenictumors(17 and 16
yearsagorespectively)andoneproximalfemurresection
fol-lowed by reconstruction witha modular revision total hip
arthroplastyS-ROM®(12years ago).Thelattersurgerywas
performed already with the diagnosis of chondrosarcoma
(Fig.1).
Giventhe excellentfunctional status ofthe patient and
the localizedtumordisease,wedecided toperform awide
resection and reconstruction.Using ilioinguinal and lateral
Fig.1–Proximalleftfemurresectionfollowedby reconstructionwithamodularrevisiontotalhip arthroplastyS-ROM®.
resection Enneking–Dunham type II (Fig. 3).10 In order to
achieveclearmarginsthe tumorwasresectedinbloc with
thetotalhipprosthesis,22cmoffemurandaportionofthe
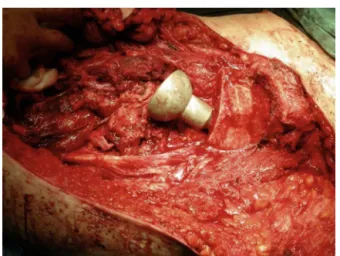
abductorhipapparatus.Thetumorwassurroundingthehip
prosthesisand its macroscopic appearanceis presentedin
Fig. 4. Acetabularreconstruction was performedwith
non-cementedpedestalcupprosthesisfixedattheiliac(Pedestal
Cup Zimmer®) (Fig. 5). In femur reconstruction we used a
cementedsilver coatedfemurproximalmodularMUTARS®
prosthesis(Fig.6).Afterpolyethyleneinsertapplication,
pros-thesisreductionandstabilitytests,atreviratubewasapplied
toensurereconstructionofsofttissueandmuscular
reinser-tions(Fig.7).Inordertoachieveadequateacetabularpedestal
Fig.2–Macroscopicaspectoftherecurrentclearcell chondrosarcomaoftheproximalleftfemur–ilioinguinal andalateralthighapproaches.
Fig.3–PeriacetabularpelvicresectionEnneking–Dunham typeII.
fixationandstability,surgeryresultedina2cmshorteningof
theinferiorlimb,correctedwithacompensatoryshoe.
Results
Postoperative periodwasunremarkable (Fig. 8). Progressive
weightbearingwasstartedaccordingtopaintolerance.The
patient was walking without crutches at3 months
follow-up. After10 years thepatient iswalking withoutcrutches,
only withaslight Trendelenburg sign.He isa recreational
cyclistandheisasymptomaticandtumoraldiseasefree.Until
Fig.5–Acetabularreconstructionwithanon-cemented pedestalcupprosthesisfixedattheiliac(PedestalCup Zimmer®).
Fig.6–Femurreconstructionwithacementedsilvercoated femurproximalmodularMUTARS®prosthesisand
acetabularandfemurreconstructionfinalaspect.
Fig.7–Treviratubeapplicationtoassurereconstructionof softtissueandmuscularreinsertions.
peakincidenceduringthethirdandfourthdecadesoflife.
Clearcellchondrosarcomaisanepiphysealtumorthatcanbe
confoundedwithlowgradechondrosarcoma.Howeverithasa
relativelyindolentmalignancy:itcanbelocallyaggressiveand
roughly25%ofpatientsexperiencelocalrecurrencesoftheir
tumorsordevelopmetastasis.Howevertumor-relateddeathis
uncommon,particularlywhenthelesionhasbeencompletely
resected“enbloc”.11
In the present case, either due to recurrence or tumor
cells persistence afterprevious resections, the patient was
diagnosedwithasizable chondrosarcoma(8cm lengthand
5cmthickness)ofarareandaggressivetype,inafemurthat
hadaprevioustotalhipprosthesis.Treatmentoptionhadto
bewidetumorresectionwithclearmargins,involvingboth
acetabulumandfemurresectionsduetothetumorextension.
Giventheexcellentgeneralcondition,absenceofsignsof
dis-seminateddiseaseandthehighfunctionallevel(inayoung
patient),acetabularefemurreconstructionwerenecessary.
Periacetabular reconstruction remains a high
techni-cal demanding challenge. Reconstructive techniques are
generallyassociatedwithunsatisfactorymechanicaland
non-mechanical complication rates.8 Enneking–Dunham type II
pelvicresectionsareassociatedwithmoremechanical
com-plications than isolated type I and typeIII resections.12–14
There are two main options for periacetabular
recons-tructions that require some remaining iliac bone stock:
saddle prosthesis, with aproximal saddle component that
articulates with the remaining iliac bone; ball-socket type
prosthesiswithapedestalorstem componentfixedatthe
remainingiliac.9Saddleprosthesiswerepreviouslythe
gold-standard forperiacetabular reconstructions, howeversome
studiesfoundtheywereassociatedwithhighratesofmajor
complications, such as infection, prosthesismigration and
dislocation.9,13,15–17Instead,despiteofpedestalcupprosthesis
arerecentimplants,theirmoreadvantageousbiomechanicsin
termsofaxialstressdistributionacrossbone–implant
inter-face, allowsthemtobeachieving goodoutcome reportsin
literature.Thisreconstructionisalsocurrentlyconsideredan
easiersurgicaltechnique,takinglesssurgicaltimeand
hav-inglowercomplicationsrateatshorttermcomparingtoother
pelvicreconstructions.8,18
Ourcentercurrentchoiceinperiacetabularreconstructions
isthepedestalcupprosthesisfixedattheiliacanda
modu-larsilvercoatedprosthesisfortheproximalfemur.Silveris
knowntohaveantimicrobialactivityandsilver-coatedtumor
Fig.8–Postoperativepelvicandfemurradiographs.
lowerrateofearlyperiprostheticinfection.19–21
Acknowledg-ingthehighriskofinfectionofpatientssubmittedtomajor
invasiveresectionsofbonetumorsand reconstructed with
bigdimensiontumorprosthesis,wecurrentlychoosesilver
coatedprosthesisforthistypeofsurgery.
Asthemajorityofpatientsinwhichthesereconstructions
areperformed haveshortlifeexpectancy,current scientific
evidenceaboutsurvivaloftheseimplantsatmediumandlong
termisabsent.Wepresenttherarecaseofapatientsubmitted
to acetabular and proximal femoral arthroplastic
recon-struction and the functional,mechanical and radiographic
resultsat10yearfollow-upperiod.Patientisasymptomatic,
independently ambulating and even practicescycling. Our
team does not recommend sports practice (mainly those
associated with impact activities or an important risk of
falls) following pelvicand femur reconstructions. However
thepatientassumedtotalresponsibilityforhisdecisionand
continues sports activity without any adverse event until
today.Theonlylimitationreferredbythepatientisaslight
Trendelenburgclaudication,probablyduetopartialresection
oftheabductorhipapparatus. Theexcellentresultsofthis
patientmaybeexplainedbythewideandclearmarginsof
tumorresection,therespectforanatomicalstructuresandits
Fig.9–Full-limbradiographat10yearsfollow-up.
proximal femur prosthesis that had excellent clinical and
functionaloutcomesat10yearsfollow-up,withoutany
com-plicationuntilnow.Pelvicreconstructionsarechallengingand
riskysurgeries.Thedevelopmentofmorefunctionalimplants,
suchasthe pedestalcup prosthesis,its correctapplication
andindications,mayallowpromisingclinicalandfunctional
results,withalowrateofcomplications.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.GuderWK,HardesJ,GoshegerG,NottrottM,StreitbürgerA. Osteosarcomaandchondrosarcomaofthepelvisandlower extremities.Chirurg.2015;86(10):993–1003.
2.LeddyLR,HolmesRE.Chondrosarcomaofbone.CancerTreat Res.2014;162:117–30.
3.EnnekingWF.Asystemofstagingmusculoskeletal neoplasms.InstrCourseLect.1988;37:3–10.
4.AthanasouN,BielackS,DeAlavaE,DeiTosAP,FerrariS, GelderblomH,etal.Bonesarcomas:ESMOclinicalpractice guidelinesfordiagnosis,treatmentandfollow-up.AnnOncol. 2010;21Suppl.5:204–13.
5.SöderströmM,EkforsTO,BöhlingTO,TeppoLH,VuorioEI, AroHT.Noimprovementintheoverallsurvivalof194 patientswithchondrosarcomainFinlandin1971–1990.Acta OrthopScand.2003;74(3):344–50.
6.EvansHL,AyalaAG,RomsdahlMM.Prognosticfactorsin chondrosarcomaofbone:aclinicopathologicanalysiswith emphasisonhistologicgrading.Cancer.1977;40(2):818–31.
7.AnractP,BiauD,BabinetA,TomenoB.Pelvicreconstructions afterbonetumorresection.BullCancer.2014;101(2):184–94.
8.BusMP,SzafranskiA,SellevoldS,GorynT,JuttePC,BramerJA, etal.LUMiC(®)endoprostheticreconstructionafter
periacetabulartumorresection:short-termresults.Clin OrthopRelatRes.2016Mar28[Epubaheadofprint]PubMed PMID:27020434.
9.IssackPS,KotwalSY,LaneJM.Managementofmetastatic bonediseaseoftheacetabulum.JAmAcadOrthopSurg. 2013;21(11):685–95.
10.EnnekingWF,DunhamWK.Resectionandreconstructionfor primaryneoplasmsinvolvingtheinnominatebone.JBone JointSurgAm.1978;60(6):731–46.
12.AllanDG,BellRS,DavisA,LangerF.Complexacetabular reconstructionformetastatictumor.JArthroplasty. 1995;10(3):301–6.
13.MenendezLR,AhlmannER,FalkinsteinY,AllisonDC. Periacetabularreconstructionwithnewendoprosthesis.Clin OrthopRelatRes.2009;467(11):2831–7.
14.CampanacciM,CapannaR.Pelvicresections:theRizzoli Instituteexperience.OrthopClinNorthAm.1991;22(1):65–86.
15.KitagawaY,EkET,ChoongPF.Pelvicreconstructionusing saddleprosthesisfollowinglimbsalvageoperationfor periacetabulartumour.JOrthopSurg(HongKong). 2006;14(2):155–62.
16.JansenJA,vandeSandeMA,DijkstraPD.Poorlong-term clinicalresultsofsaddleprosthesisafterresectionof periacetabulartumors.ClinOrthopRelatRes. 2013;471(1):324–31.
17.DonatiD,D’ApoteG,BoschiM,CevolaniL,BenedettiMG. Clinicalandfunctionaloutcomesofthesaddleprosthesis.J OrthopTraumatol.2012;13(2):79–88.
18.DePaolisM,BiazzoA,RomagnoliC,AlìN,GianniniS,Donati
DM.Theuseofiliacstemprosthesisforacetabulardefects
followingresectionsforperiacetabulartumors.Scientific
WorldJ.2013;2013:717031,
http://dx.doi.org/10.1155/2013/717031,eCollection2013.
19.PiccioliA,DonatiF,GiacomoGD,ZiranuA,CareriS,Spinelli
MS,etal.Infectivecomplicationsintumourendoprostheses
implantedafterpathologicalfractureofthelimbs.Injury.
2016,http://dx.doi.org/10.1016/j.injury.2016.07.054.
S0020-1383(16)30362-X.
20.WafaH,GrimerRJ,ReddyK,JeysL,AbuduA,CarterSR,etal. Retrospectiveevaluationoftheincidenceofearly
periprostheticinfectionwithsilver-treatedendoprosthesesin high-riskpatients:case–controlstudy.BoneJointJ.
2015;97-B(2):252–7.