r e v b r a s o r t o p . 2016;51(4):482–485
SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Case
Report
Pelvic
migration
of
the
helical
blade
after
treatment
of
transtrochanteric
fracture
using
a
proximal
femoral
nail
夽
Pedro
Luciano
Teixeira
Gomes
∗,
Luís
Sá
Castelo,
António
Lemos
Lopes,
Marta
Maio,
Adélia
Miranda,
António
Marques
Dias
CentroHospitalardeTrás-os-MonteseAlto-Douro,DepartamentodeOrtopediaeTraumatologia,VilaReal,Portugal
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received1July2015
Accepted25July2015
Availableonline4July2016
Keywords:
Femoralfractures
Prosthesesandimplants
Orthopedicpins
Elderly
a
b
s
t
r
a
c
t
Proximalfemoralnailswithahelicalbladeareanewgenerationofimplantsusedfor
treat-ingtranstrochantericfractures.Thebladedesignprovidesrotationalandangularstability
forthefracture.Despitegreaterbiomechanicalresistance,theysometimespresent
com-plications.Intheliterature,therearesomereportsofcasesofperforationofthefemoral
headcausedbyhelicalblades.Here,aclinicalcaseofmedialmigrationofthehelicalblade
throughthefemoralheadandacetabulumintothepelviccavityispresented.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora
Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http://
creativecommons.org/licenses/by-nc-nd/4.0/).
Migrac¸ão
pélvica
de
lâmina
helicoidal
após
tratamento
de
fratura
transtrocantérica
com
cavilha
proximal
do
fêmur
Palavras-chave:
Fraturasdofêmur
Próteseseimplantes
Pinosortopédicos
Idoso
r
e
s
u
m
o
Ascavilhasproximaisdofêmurcomlâminahelicoidalrepresentamumanovagerac¸ão
deimplantesusadosnotratamentodefraturastranstrocantéricas.Odesenhodalâmina
forneceestabilidaderotacionaleangularàfratura.Apesardamaiorresistênciabiomecânica,
porvezesapresentamcomplicac¸ões.Naliteraturaencontram-sedescritosalgunscasosde
perfurac¸ãodacabec¸afemoralporlâminashelicoidais.Apresenta-seumcasoclíniconoqual
ocorreumigrac¸ãomedialdalâminahelicoidalatravésdacabec¸afemoraledoacetábulopara
acavidadepélvica.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevierEditora
Ltda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http://
creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudyconductedattheCentroHospitalardeTrás-os-MonteseAlto-Douro,DepartamentodeOrtopediaeTraumatologia,VilaReal,
Portugal.
∗ Correspondingauthor.
E-mail:[email protected](P.L.Gomes).
http://dx.doi.org/10.1016/j.rboe.2015.07.013
2255-4971/©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditoraLtda.Thisisanopenaccessarticle
rev bras ortop.2 0 1 6;51(4):482–485
483
Introduction
Transtrochantericfracturesare aprevalent conditioninthe
elderly. The incidence of this disease has increased
con-siderablyin recent years,as a resultof populationaging.1
Improving the treatment ofthesefractures is essential for
patientquality oflife, reducing the lengthofhospitalstay
andpromotingaquickrecoverytopre-fracturefunctional
sta-tus.Therearemanyimplantsavailableforthetreatmentof
suchfractures.InstableAO31-A1transtrochantericfractures,
extramedullary devices(plates) can beapplied, with
favor-able results.2 However, in unstable AO 31-A2/A3 fractures,
intramedullaryimplantshaveabiomechanicaladvantage,2,3
withbettertransmissionoftheaxialload.Morerecently,anew
generationofproximalfemoralnailswithhelicalbladeshas
beendeveloped,featuringalargercontactareaand
compres-sionbetweenthebladeandthecancellousbone,promoting
betterstabilityagainstvaruscollapse,especiallyinpatients
with osteoporoticbones.4,5 Nonetheless, complications are
sometimesobserved,especiallythose relatedtofixation.6–8
Thisstudypresentsacaseofperforationofthefemoralhead
andthebottomoftheacetabulumwithpelvicmigrationofthe
helicalblade.
Case
report
An88-year-old female, with ahistory ofhypertension and
heart failure,had a fallfrom herown heightin2014 with
traumaintheleft hip.Aradiographic studyrevealed aleft
AO 31-A1 trochanteric fracture (Fig. 1). She was urgently
treatedwith proximal femoralnail (10mm×170mm, 130◦)
and antirotation blade (100mm). Surgical procedure was
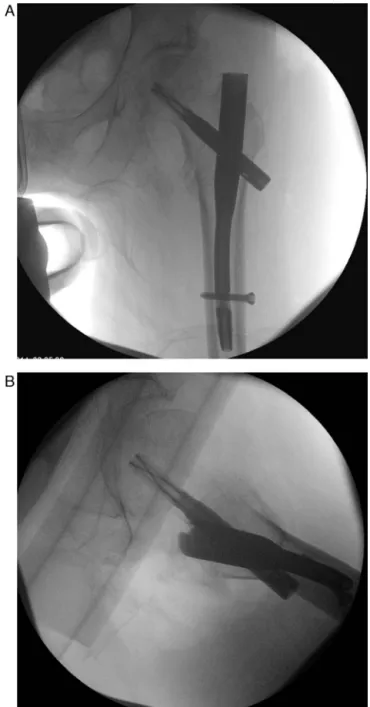
uneventful.Ahelicalbladewasplacedinthecenter-bottom
position in the anteroposterior incidence (Fig. 2A) with a
Parker’sratio (anteroposterior)9 of38 and slightlyposterior
in the lateral incidence (Fig. 2B) with a Parker’s ratio
(lat-eral)of36.Thecalculated“tip-apex”distance10was24mm,
andthecervicodiaphysealanglewas136◦.Postoperatively,the
fracture wassignificantly reduced (Fig. 3).The patientwas
dischargedtoarehabilitationinstitution,withtheindication
Fig.1–TransthrocanthericAO31-A1fractureontheleft.
ofambulation withawalker andpartialload. Shewas
re-evaluedatanoutpatientconsultationonthesecondmonth
postoperative,complainingofpaininthelefthipanddifficulty
inmobilization;thepatientdeniednewtraumaticepisodes.
Radiographically,aperforationofthefemoralheadand the
bottomoftheacetabulumbythehelicalbladewasobserved,
withintrapelvicmigrationFigs. 4and5).Thematerialwas
extractedusingthepreviousapproach,uneventfully.The
frac-tureevolvedtovarusmalunionandallowedambulationofthe
patient.
Discussion
The problem of rotational instability, followed by the
varus collapse of the femoral head and by the cephalic
484
rev bras ortop.2 0 1 6;51(4):482–485Fig.3–Hipradiographyintheimmediatepostoperative period.
perforationof the nail tothe hip joint,isa well-described
phenomenon,4 known as cut-out, and occurs with some
platesandcephalomedullarynailsusedinthetreatmentof
transtrochantericfractures.Proximalfemoralnailswith
heli-calbladesweredevelopedtoaddressthisproblem.Thespiral
bladeisinsertedbyimpactionandpromotesthecompression
ofthecancellous bonearoundthe implant.Several
biome-chanicalstudieshavedemonstratedtheadvantagesofspiral
bladeswhencomparedwithconventionalscrews.4,5The
sta-bilityobtainedafterfracturefixationisinfluencedbyseveral
factors,suchasthereductionachievedandthepositioningof
thenailinthefemoralhead.Thisinsertionshouldbemade
Fig.4–Pelvicmigrationofthehelicalbladeonthesecond monthpostoperatively.
Fig.5–Amplifiedimages(anteroposteriorandprofile) showingtheperforationofthebottomoftheacetabulumby thehelicalblade.
thecenter-bottompositionintheanteroposteriorandcentral
focus on lateral incidence,thus placingthe implant inthe
areawithhighertrabeculardensity.Baumgaertner10defined
the variabletip-apexdistanceand concludedthat implants
placedatadistanceofmorethan25mmwereathigherrisk
ofcut-out.However,thecomplicationpresentedinthisreport
isnotaconventionalcaseofcut-out,butanewphenomenon
ofimplantfailuredescribedascut-throughbyFreietal.6and
previously reported by Simmermacher et al.7 and Brunner
etal.8aperforationofthefemoralheadbythebladeinsertion
axis,withoutsignificantlossofreduction.Thecasedescribed,
rev bras ortop.2 0 1 6;51(4):482–485
485
have presented more serious complications with vascular
injuryand a different outcome.Recently,Nikoloski et al.11
conductedastudytoadapttheconceptoftip-apexdistance
toPFNAimplants;the previous variableshowed abimodal
distributioninthecasesofcut-out,whichwasnotobserved
inprevious implants.This suggests thatthe helical blades
shouldnotbeplacedtooclosetothesubchondralbone.Zhou
andChang12definedatip-apexdistancebetween20mmand
25mmforplacementofthehelicalblade.
Osteoporosisinfluencesthecut-outevent.Bonnaireetal.13
haveshownthatbonemineraldensityoflessthan0.6g/cm3
increasestheriskofimplantfailure.Mostauthors6–8suggest
thatthemaincauseofcentralperforationofthefemoralhead
areduetoafailureofthehelicalbladetoslidesidewaysas
the fracture collapses. This failure toslide may occur due
todefectsoftheblade/nailinterfaceortoimpactionofthe
baseofthebladeagainstthelateral cortex.Furthermore,it
hasbeensuggestedthepresenceoftheZ-effect,which,over
severalloadcyclesduringambulation,wouldpromotemedial
migrationofthehelicalblade.14Theoccurrenceofanew
trau-maticepisodecanalsobethesourceoftheproblem.Regarding
thetreatmentofthesecomplications,whichusuallyoccurin
thefirst twomonthsaftersurgery,Brunneret al.,8 intheir
series ofthree cases, reviewed the fixation with a shorter
helicalblade,maintaining the samenail intwo cases,and
throughcementlesstotalhiparthroplastyinanothercase.In
thepresentcase,theentirematerialwasextracted,sincethe
88-year-oldpatientdidnotpresentanestheticconditionsfor
totalarthroplastyandbecausetheuseofthesameimplant
inanewfixationattemptcouldresultinmigration,requiring
reintervention.Inordertoreducetheincidenceofthis
com-plication,thefractureshouldbeadequatelyreducedandthe
bladeshouldbecorrectlypositionedinthefemoralhead.Prior
drillingoftheentirebladepathisunnecessaryandshould
beavoided,especiallyinthepresenceofosteoporoticbone.6,8
Recently,thepossibilitytoimprovefixationbycementingthe
femoralheadusingaperforatedspiralbladewasdeveloped.
Thecentral perforation ofthe femoralhead bythe helical
bladeisauniquecomplicationinherenttothistypeofimplant.
Morebiomechanicalresearchisneededtoclarifythe
perfora-tionmechanism.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.HungriaNetoJS,DiasCR,AlmeidaJB.Características epidemiológicasecausasdafraturadoterc¸oproximaldo fêmuremidosos.RevBrasOrtop.2011;46(6):660–7.
2.KumarR,SinghRN,SinghBN.Comparativeprospectivestudy ofproximalfemoralnailanddynamichipscrewinthe treatmentofintertrochantericfracturefemur.JClinOrthop Trauma.2012;3(1):28–36.
3.CurtisMJ,JinnahRH,WilsonV,CunninghamBW.Proximal femoralfractures:abiomechanicalstudytocompare intramedullaryandextramedullaryfixation.Injury. 1994;25(2):99–104.
4.SommersMB,RothC,HallH,KamBC,EhmkeLW,KriegJC, etal.Alaboratorymodeltoevaluatecutoutresistanceof implantsforpertrochantericfracturefixation.JOrthop Trauma.2004;18(6):361–8.
5.StraussE,FrankJ,LeeJ,KummerFJ,TejwaniN.Helicalblade versusslidinghipscrewfortreatmentofunstable
intertrochanterichipfractures:abiomechanicalevaluation. Injury.2006;37(10):984–9.
6.FreiHC,HotzT,CadoschD,RudinM,KächK.Centralhead perforation,orcutthrough,causedbythehelicalbladeofthe proximalfemoralnailantirotation.JOrthopTrauma. 2012;26(8):e102–7.
7.SimmermacherRK,LjungqvistJ,BailH,HockertzT,Vochteloo AJ,OchsU,etal.Thenewproximalfemoralnailantirotation (PFNA)indailypractice:resultsofamulticentreclinicalstudy. Injury.2008;39(8):932–9.
8.BrunnerA,JöckelJA,BabstR.ThePFNAproximalfemurnail intreatmentofunstableproximalfemurfractures–3casesof postoperativeperforationofthehelicalbladeintothehip joint.JOrthopTrauma.2008;22(10):731–6.
9.ParmarV,KumarS,AsterA,HarperWH.Reviewofmethods toquantifylagscrewplacementinhipfracturefixation.Acta OrthopBelg.2005;71(3):260–3.
10.BaumgaertnerMR,SolbergBD.Awarenessoftip-apex distancereducesfailureoffixationoftrochantericfractures ofthehip.JBoneJointSurgBr.1997;79(6):969–71.
11.NikoloskiAN,OsbroughAL,YatesPJ.Shouldthetip-apex distance(TAD)rulebemodifiedfortheproximalfemoralnail antirotation(PFNA)?Aretrospectivestudy.JOrthopSurgRes. 2013;8:35.
12.ZhouJQ,ChangSM.FailureofPFNA:helicalbladeperforation andtip-apexdistance.Injury.2012;43(7):1227–8.
13.BonnaireF,WeberA,BöslO,EckhardtC,SchwiegerK,LinkeB. Cuttingoutinpertrochantericfractures–problemof osteoporosis?Unfallchirurg.2007;110(5):425–32.