SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
article
Functional
outcome
after
arthroscopic
repair
of
triple
shoulder
instability
夽
Glaydson
Gomes
Godinho
a,b,c,
Flávio
de
Oliveira
Franc¸a
a,c,∗,
José
Márcio
Alves
Freitas
a,b,c,
Lander
Braga
Calais
Correia
Pinto
a,b,c,
Carolina
Lima
Simionatto
a,b,c,
Pedro
Paulo
Gomes
Viana
Filho
a,b,caHospitalOrtopédico,BeloHorizonte,MG,Brazil bHospitalBeloHorizonte,BeloHorizonte,MG,Brazil cHospitalLifecenter,BeloHorizonte,MG,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received25April2016 Accepted30May2016 Availableonline6March2017
Keywords:
Arthroscopy/methods Shoulder
Rotatorcuff Patientsatisfaction Articularmotionrange
a
b
s
t
r
a
c
t
Objective:Toevaluatethefunctionaloutcomesofpatientssubmittedtoarthroscopicrepair oftriplelabrallesion.
Methods:Thiswasananalyticalretrospectivestudyofpatientswhounderwentarthroscopic treatmentoftriplelabrallesionfromMarch2005toDecember2014.Patientswithatleastone yearofpostoperativefollow-upwereincluded.Atotalofninepatientswereevaluated.The meanagewas32.3yearsandthedominantsidewasaffectedinfivepatients.Patientswere functionallyassessedregardingtherangeofmotion(ROM)inelevation,externalrotation withthearmclosetothebodythearminabductionof90◦,andinternalrotation,andby
theCarter–Rowescore.Thedegreeofsatisfactionwasassessedattheendofthefollow-up period.
Results:Threepatientshadlessthanfiveepisodesofinstability,fourpatientshadbetween fiveandtenepisodes,andtwopatientshadmorethantenepisodes.Sevenpatientshad pos-itiveO’BrientestforSLAPlesionsandpositiveapprehensiontestinabductionandexternal rotation,andonlyonepatienthadapprehensioninadductionandinternalrotation.Three patientspersistedwithpositiveO’Brientestandonewithapprehensioninabductionand externalrotationattheendoffollow-up.Therangeofmotionwascompleteinallcases. ThemedianCarter–Rowescoreincreasedfrom40preoperativelyto90(p=0.008).
Conclusion:Thearthroscopicrepairoftriplelabrallesionsallowsfortherestorationofthe stabilityoftheglenohumeraljoint,achievingexcellentfunctionalresults.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudyconductedatHospitalLifecenter,HospitalBeloHorizonte,andHospitalOrtopédico,BeloHorizonte,MG,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](F.O.Franc¸a).
http://dx.doi.org/10.1016/j.rboe.2017.02.004
Resultado
funcional
após
reparo
artroscópico
da
tríplice
instabilidade
do
ombro
Palavras-chave: Artroscopia/métodos Ombro
Bainharotadora Satisfac¸ãodopaciente Amplitudedomovimento articular
r
e
s
u
m
o
Objetivo: Avaliarosresultadosfuncionaisdospacientessubmetidosareparoartroscópico datríplicelesãolabraldoombro.
Métodos:Estudoanalíticoretrospectivodepacientescomtríplicelesãolabraldoombro, sub-metidosatratamentoartroscópicodemarc¸ode2005adezembrode2014.Foramincluídos pacientescompelomenosumanodeseguimentopós-operatório.Novepacientesforam avaliados.Amédiafoide32,3anoseoladodominantefoiafetadoemcincopacientes. Ospacientesforamavaliadosfuncionalmentepormeiodaamplitudedemovimentoem elevac¸ão,rotac¸ãoexternacomobrac¸ojuntoaocorpoecomobrac¸oemabduc¸ãode90◦,
rotac¸ãointernaepormeiodoescoredeCarter-Rowe.Ograudesatisfac¸ãofoiavaliadono fimdoseguimento.
Resultados: Trêspacientestiverammenosdecincoepisódiosdeinstabilidade,quatroentre cincoedezedoismaisdedez.SetepacientestiveramtestedeO’Brienpositivoparalesãodo lábiosuperiordeanteriorparaposterior(Slap,doinglêssuperiorlabrumanteriortoposterior lesion)eapreensãoemabduc¸ãoerotac¸ãoexternapositiva;apenasumapresentouapreensão emaduc¸ãoerotac¸ãointerna.TrêspacientespersistiramcomtestedeO’Brienpositivoe umcomapreensãoemabduc¸ãoerotac¸ãoexternanofimdoseguimento.Aamplitudede movimentoestevecompletaemtodososcasosnaúltimaavaliac¸ão.Amédiadoescorede Carter-Roweaumentoude40nopré-operatóriopara90(p=0,008).
Conclusão: Oreparoartroscópicodatríplicelesãolabralpermiterestauraraestabilidadeda articulac¸ãoglenoumeralealcanc¸aexcelentesresultadosfuncionais.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Thestabilityoftheglenohumeraljoint dependsona com-plexcombinationofthestaticanddynamicstabilizersofthe shoulder.1 For anterior dislocation, there isan avulsion of
theanterior-inferiorlabrumcomplexoftheperiosteumofthe glenoid,whichgeneratesanteriorinstability,especiallyinthe movementsofabductionandexternalrotation.2
Symptomsofposteriorinstabilityarevague;itmaypresent onlyaspainincertainmovements,especiallyadductionand internal rotation. It can be caused by a single trauma or byrepetitivemicrotraumas,throwingactivities,orcanresult fromconvulsionsandelectricshocks.3
Superiorlabrum anterior to posterior(SLAP) lesions are stilluncommonshoulderinjuries,withanincidenceof6%, diagnosedduringarthroscopicprocedures,accordingto Sny-deretal.4Clinicalandimagingdiagnoseshavelowsensitivity
andspecificity,5andthisconditionmaycontributetoamajor
functionaldeficitandshoulderpain.6
LoandBurkhart7definedthetriplelabrallesionasa
con-ditionthatinvolves unusuallesionsofthe glenoid labrum: superiorly, a SLAP lesion type II; anteroinferiorly, Bankart lesions; and posteroinferiorly, lesions such as the reverse Bankart(Fig.1).
Habermeyer et al.8 reported that the emergence of a
triple labral lesion is related tothe number ofrelapses in anteriordislocations,denotingthechronologicaland evolu-tionary character of these lesions. A very detailed clinical
examination should be performed, including the tests for anteriorand posteriorinstabilityandSLAP. AccordingtoLo andBurkhart,7theincidenceoftriplelabrallesionwas2.4%
inagroupof297patientswithligamentandlabrallesionsof theglenoid.
This study aimed to evaluate the functional results of patients who underwent arthroscopic correction of triple labrallesionsandtoraiseawarenessofthediagnostic diffi-cultyandunderestimationofthiscondition.
Material
and
methods
Thiswasaretrospectiveanalyticalstudyofpatients submit-tedtothearthroscopictreatmentoftriplelabrallesionsfrom March2005toDecember2014.Duringthisperiod,15patients werediagnosedandtreatedforthisconditionbytheShoulder Groupofthisinstitution.
Forthestudy,patientswhohadatriplelabrallesionanda minimumfollow-upof1yearwereselected.Exclusion crite-riawere:previousshouldersurgery,fracturesequelaeinthe region,advancedglenohumeralarthrosis,andlessthanone yearoffollow-up.Ofallpatientswhounderwentsurgery dur-ingthisperiod,11mettheinclusioncriteria.Tworefusedto participateinthestudy.Oftheninepatientsselected,seven werepersonallyassessedandtwobytelephoneduetothefact thattheylivedoutsidethecityoforiginofthestudy.
Fig.1–ArthrographyMRIimageoftherightshoulderinthecoronalandaxialT2-weightedcutsshowingtheSLAPlesion (left)andtheBankartandposteriorlabrallesions(right).
side was affected in four patients (44.4%) and left side in five(55.6%).Thedominantlimbwasaffectedinfivepatients (55.6%).
Fourpatients(44.4%)hadatraumaticlesion;four(44.4%) lesionswerecausedbyrepetitivemicrotraumasinsports prac-tice,twoofwhichwereprofessionalathletes;andonepatient (11.1%)hadhadaseizure.
TheCarter–Rowe9 score, whichtakes into consideration
thestability,rangeofmotion(ROM),andfunction,wasused forthefunctionalassessment(Table1).
ROM for anterior elevation,lateral rotation with arm in abductionandnearthebody,andmedialrotationwere com-pared. Thedegree of satisfaction of patients with surgical treatmentwasalsoassessed.Attheendoffollow-upperiod,
Table1–Carter–Rowescore.
Stability Note
Norecurrences,subluxations,or apprehension
50
Apprehensionwhenthearmwas placedincertainpositions
30
Subluxations(withnoneedfor reductions)
10
Recurrentdislocation 0
Movement
100%ofthemovement 20
75%ofnormalmovement 15
50%ofthenormalER,75%ofthe normalAEandIR
5
50%ofthenormalAE,IR,andER 0
Function
Withoutlimitationtosportor workactivities.Minimalorno discomfort
30
Smalllimitationandminimal discomfort
25
Moderatelimitationand discomfort
10
Severelimitationandpain 0
Totalpossiblepoints 100
AE,anteriorelevation;ER,externalrotation;IR,internalrotation.
patientsunderwentradiographytoassesspresenceof arthro-sis.
Atthelastpostoperativephysicalexamination,the ante-rior apprehension test in 90◦ of abduction and external
rotation,theO’Brientest,andtheposteriorapprehensiontest inadductionandinternalrotationwereassessed.
Allpatientsfilledoutaninformedconsentformfor disclo-sureofclinicaldata,andthestudywasapprovedbytheEthics CommitteeoftheOrthopedicHospital.
Surgicaltechnique
The procedure was performed with patient in contralat-erallateraldecubitus,undergeneralanesthesiaandbrachial plexusblock.Initially,thearthroscopewasinsertedthrough theposteriorportallocated2cmdistaland2cmmedialtothe posterolateralcorneroftheacromion.
Diagnosisoftriplelabrallesionwasmadebyjoint inspec-tion,inthepresenceofBankartlesion,reverseBankartlesion, andSLAPlesion(II,III,orIV).7Apeelbackmaneuverand
pal-pationofthesuperiorlabrallesionwithaprobeconfirmedthe presenceofSLAPlesion10(Figs.2and3).
Post
Ant
Slap II
Fig.3–Arthroscopicimageoftherightshoulder,
demonstratingtheanterior,posterior,andsuperiorlabral lesions.
Throughtheanterosuperior,anteroinferior,andposterior portals,threecannulaswereinserted.Theanterosuperior por-talwas usedforvisualization throughanarthroscope, and surgicalinstrumentswerepassedthroughtheanteroinferior andposteriorportals.
Thearea ofthelesions was thendebrided and opened, withdecorticationoftheedgesoftheglenoidand regulariza-tionoftheglenoidlabrum.Thefirstlesiontoberepairedwas Bankart’sreverse lesion.However,theposteriorportaldoes notprovideasuitableapproachangleforinsertingthe mini-anchorsattheposteriorborder oftheglenoid.Therefore, a needle(JelcoNo.18)wasusedtodeterminea45◦ anglewith theglenoidsurface,andmini-anchorswereinserted percuta-neously.Generally,oneortwoanchorsaresufficientforthe posteriorrepair. Thewireswere threadedandtied,andthe posteriorlesionwasfixated.
Nextstepwasthereinsertionoftheanteriorlabrum,which correctstheBankartlesion.Mini-anchors,spacedata1cm dis-tance,wereinsertedintheanteriorborderoftheglenoid,also ata45◦angleinrelationtotheglenoidsurface.Thedirection followedwasinferiortosuperior.Wireswerethenthreaded andtied.
Finally,theSLAPlesionwasrepaired,withtheintroduction ofamini-anchoronthesuperioredgeoftheglenoid;wires werepassedwithaneedleofthesurgeon’spreferenceanda mattresssuturewasmade.Thefixationandstabilityofthe glenoidlabrum wasassessedwithaprobe,inapanoramic view of the repairs (Fig. 4). The followingsteps were skin suture,dressing,andimmobilizationwithaVelpeauslingfor 21days.
Statisticalanalysis
Toassessthepre-andpost-operativerangeofmotion(ROM) and theCarter–Rowe scores, non-parametric Wilcoxontest wasused.
Data were analyzed in the statistical program Predic-tive Analytics Software (PASW 18). In all statistical tests,
Ant
Post
Slap II
Fig.4–Arthroscopicimageaftertherepairoflesionsthat comprisethetriplelabrallesion.
a5%significancelevelwasadopted.Thus,statistically signif-icant associationsare those whosep-valuewas lowerthan 0.05.
Results
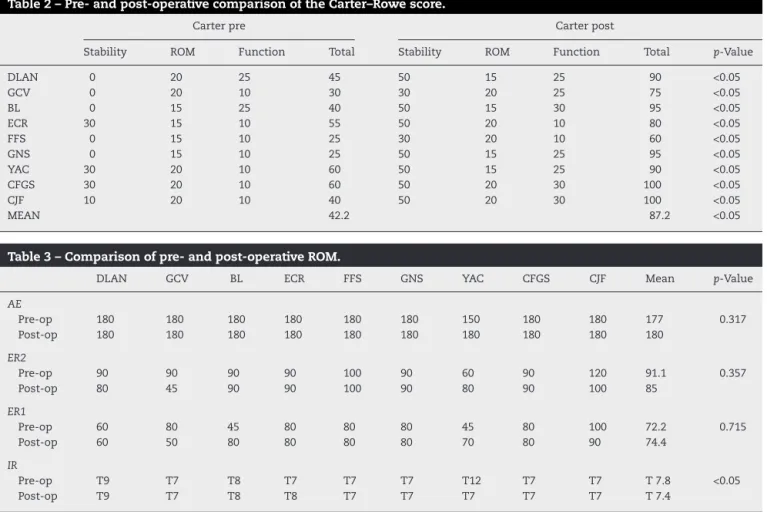
FunctionalevaluationofpatientsisshowninTable2. TheROMoftheassessedpatientsispresentedinTable3. Data on number ofepisodesofinstability are shownin
Fig.5.
Regardingphysicalevaluation,Table4presentsa compar-isonbetweenpre-andpostoperativeresultsofeachpatient intheO’Brientest,apprehensiontestinabductionand exter-nalrotation,andapprehensiontestinadductionandinternal rotation.
Ofthesevenpatientswhoagreedtoundergoradiographic evaluation at the end of the follow-up period, only one
2
3
4
< 5 episodes 5-10 episodes > episodes
Table2–Pre-andpost-operativecomparisonoftheCarter–Rowescore.
Carterpre Carterpost
Stability ROM Function Total Stability ROM Function Total p-Value
DLAN 0 20 25 45 50 15 25 90 <0.05
GCV 0 20 10 30 30 20 25 75 <0.05
BL 0 15 25 40 50 15 30 95 <0.05
ECR 30 15 10 55 50 20 10 80 <0.05
FFS 0 15 10 25 30 20 10 60 <0.05
GNS 0 15 10 25 50 15 25 95 <0.05
YAC 30 20 10 60 50 15 25 90 <0.05
CFGS 30 20 10 60 50 20 30 100 <0.05
CJF 10 20 10 40 50 20 30 100 <0.05
MEAN 42.2 87.2 <0.05
Table3–Comparisonofpre-andpost-operativeROM.
DLAN GCV BL ECR FFS GNS YAC CFGS CJF Mean p-Value
AE
Pre-op 180 180 180 180 180 180 150 180 180 177 0.317
Post-op 180 180 180 180 180 180 180 180 180 180
ER2
Pre-op 90 90 90 90 100 90 60 90 120 91.1 0.357
Post-op 80 45 90 90 100 90 80 90 100 85
ER1
Pre-op 60 80 45 80 80 80 45 80 100 72.2 0.715
Post-op 60 50 80 80 80 80 70 80 90 74.4
IR
Pre-op T9 T7 T8 T7 T7 T7 T12 T7 T7 T7.8 <0.05
Post-op T9 T7 T8 T8 T7 T7 T7 T7 T7 T7.4
AE,anteriorelevation;IR,internalrotation;ER1,externalrotation1(withthearmclosetothebody);ER2,externalrotation2(withthearmat 90◦ofabduction).
Table4–Pre-andpostoperativecomparisonoftheO’Brientest,apprehensiontestinabductionandexternalrotation, andapprehensiontestinadductionandinternalrotation.
DLAN GCV BL ECR FFS GNS YAC CFGS CJF
O’Brientest
Pre-op Neg + + + + Neg + + +
Post-op Neg + Neg + Neg Neg + Neg Neg
ApprehensioninabductionandER
Pre-op + Neg + + + Neg + + +
Post-op Neg + Neg Neg + Neg Neg Neg Neg
ApprehensioninadductionandIR
Pre-op Neg Neg Neg Neg Neg Neg Neg + Neg
Post-op Neg Neg Neg Neg Neg Neg Neg Neg Neg
ER,externalrotation;IR,internalrotation.
presentedaninitialdegenerativeconditioncompatiblewith SamilsonandPrieto11typeIarthrosis.
Regarding the degree of satisfaction, out of the nine patientsassessed,onlyonewasdissatisfied withthe treat-ment.
Discussion
Todefinethetriplelabralshoulderlesion,LoandBurkhart7
consideredasanterior,posterior,andsuperiorlabrallesions those thataffect atleast two-thirds ofthe area comprised
in the2–6 o’clock,6–10o’clock, and 2–10o’clockpositions, respectively(assumingarightshoulder).
In the present study, the criteria set forth by Lo and Burkhart7 was notused, since regardlessof the degree of
engagement in each region (anterior, posterior, and supe-rior),thepatientspresentedcharacteristicclinicalsigns,and diagnosis wasconfirmedduringarthroscopy.Therefore, the clinicalcorrelationoflesionswasweightedmoreheavilythan theisolatedanatomicalaspect.
Intheirseries,LoandBurkhart7identifiedanterior
posteriorinstabilityasthecauseinonlyonecase.Duetothe recoilmechanism,anteriorinstabilitiescouldleadtoa poste-riorlabrallesion.Thistheoryisbasedontheconceptofcyclic capsulolabraldysfunctionreportedbyWarrenetal.,12inwhich
anisolatedanteriorlabrallesion wouldnotbesufficientto causeadislocationunlesstheposteriorstabilizingstructures werealsoinjured.
Thisfact was also observedin the present study, since 55.5%ofthepatientswereinvolvedintraumaticepisodeswith anteriorinstability.Noneofthepatientshadaninitial trau-maticepisodeofposteriorinstability.
Inthisseries,aprofessionalsoccerplayer,afteranterior traumaticdislocation and sixrecurrences, presentedtriple labrallesion.Inthiscase,theorigin oftheposteriorlesion canbejustifiedbytherecoilmechanismdescribedbyLoand Burkhart7Theupperlabrallesionwouldderivefromanterior
traumaticinstabilityitself,sincetheassociationbetweenSLAP andBankartlesionswasdescribedin50%ofthecasesinthe studybyGodinhoetal.,5andreached77.8%inthestudyby
Warneretal.13
Anothermechanismthatwouldexplaintheoriginoftriple labrallesionoftheshoulderisthatobservedinthrowing ath-letes.Inthisgroupofathletes,the genesisoftheposterior labrallesion and the SLAP lesion is throughthe peelback mechanism,14associatedwithinternalimpact.15Ifthereisan
anteriordislocation,atriplelabralshoulderlesionis charac-terized,aslongastheanteriorlabrallesionispresent.
Inthiscontext,avolleyballathleteofthisseries,afteran episode of traumatic anterior dislocation due to a seizure crisis, presentedatriple labrallesion of the shoulder. The SLAPlesionmayhavebeencausedbytherecoilmechanism describedbyLoandBurkhart7orbythecombinationofactive
forcesduringtheseizure.
Thetriplelabrallesionoftheshoulderisnoteasilydetected bytheavailableimagingmethods;itcanbediagnosedinup to32.3%ofcaseswhenMRIarthrogramisusedandin8.7% whenMRIisused.16Thisfactisprobablyduetothedifficulty
indiagnosingSLAPlesions,asdemonstratedbyGodinhoetal.5
In the present study, alterations compatible with triple labrallesions wereevidenced inonlyfour patients(36.3%), which demonstrates how this diagnosis can be underesti-mated.
Treatmentofglenoidlabral lesionsinathletesmay lead tounsatisfactoryresults, especiallyregardingreturn tothe pre-injurylevel.ThesuccessrateafterisolatedrepairofSLAP lesionsisaround80%.17,18 Inturn,inanteriorlabrallesions,
the successrate rangesfrom 68% to 77%.19,20 Therefore, it
isexpectedthatinthepresenceofthetriplelabralshoulder lesionthesuccessrateisevenlower,duetotheassociationof injuries.
However,inthepresentstudy,asignificantimprovement wasobservedintheCarter–Rowe9scores.Meanscorewas42.2
pointspreoperativelyand87.2postoperatively(p<0.05).Two ofthepatients,oneofwhomwasawrestlerandtheothera volleyballplayer,arestillabletoperformprofessionalsports activities.Regarding ROM, nostatistically significant differ-enceswereobservedbetweenpre-andpostoperativeperiods. Onlyonepatientwasdissatisfiedattheendoftreatment,due tothefactthathesufferedanaccidentfollowedbya recur-renceofthelesion.Allpatientswhopracticedsports,whether
professionallyor recreationally,returned tothose activities withoutdeficit.
The literature isstill very scarceregarding this typeof lesion.Newstudieswithmoreexpressivesamplesizeshould beconductedinordertoachieveamoreaccuratestatistical assessment.
Conclusion
Arthroscopic treatment oftriple shoulderlesion leads toa significantfunctionalimprovement,withoutlossofROMand withsatisfactoryreturntothepracticeofsport.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.KimSH,HaKI,KimSH.Bankartrepairintraumaticanterior shoulderinstability:openversusarthroscopictechnique. Arthroscopy.2002;18(7):755–63.
2.BankartAS.Recurrentorhabitualdislocationofthe shoulder-joint.BrMedJ.1923;2(3285):1132–3.
3.DeLongJM,JiangK,BradleyJP.Posteriorinstabilityofthe shoulder:asystematicreviewandmeta-analysisofclinical outcomes.AmSportsMed.2015;43(7):1805–17.
4.SnyderSJ,BanasMP,KarzelRP.Ananalysisof140injuriesto thesuperiorglenoidlabrum.JShoulderElbowSurg. 1995;4(4):243–8.
5.GodinhoGG,FreitasJMA,LeiteLMB,PinaERM.LesõesSlapno ombro.RevBrasOrtop.1988;33(5):345–52.
6.NamEK,SnyderSJ.Thediagnosisandtreatmentofsuperior labrum,anteriorandposterior(Slap)lesions.AmJSports Med.2003;31(5):798–810.
7.LoIK,BurkhartSS.Triplelabrallesions:pathologyand surgicalrepairtechnique-reportofsevencases.Arthroscopy. 2005;21(2):186–93.
8.HabermeyerP,GleyzeP,RickertM.Evolutionoflesionsofthe labrum–ligamentcomplexinposttraumaticanteriorshoulder instability:aprospectivestudy.JShoulderElbowSurg. 1999;8(1):66–74.
9.RoweCR,PatelD,SouthmaydWW.TheBankartprocedure:a long-termend-resultstudy.JBoneJointSurgAm.
1978;60(1):1–16.
10.BurkhartSS,MorganCD.Thepeel-backmechanism:itsrole inproducingandextendingposteriortypeIISlaplesionsand itseffectonSlaprepairrehabilitation.Arthroscopy.
1998;14(6):637–40.
11.SamilsonRL,PrietoV.Dislocationarthropathyofthe shoulder.JBoneJointSurgAm.1983;65(4):456–60.
12.WarrenRF,KornblattIB,MarchandR.Staticfactorsaffecting shoulderstability.OrthopTrans.1984;8:89.
13.WarnerJJ,KannS,MarksP.Arthroscopicrepairofcombined Bankartandsuperiorlabraldetachmentanteriorand posteriorlesions:techniqueandpreliminaryresults. Arthroscopy.1994;10(4):383–91.
14.BurkhartSS,MorganCD,KiblerWB.Thedisabledthrowing shoulder:spectrumofpathology.PartI:pathoanatomyand biomechanics.Arthroscopy.2003;19(4):404–20.
posterosuperiorglenoidrim:anarthroscopicstudy.J ShoulderElbowSurg.1992;1(5):238–45.
16.RicchettiET,CiccottiMC,CiccottiMG,WilliamsGRJr,Lazarus MD.Sensitivityofpreoperativemagneticresonanceimaging andmagneticresonancearthrographyindetectionof panlabraltearsoftheglenohumeraljoint.Arthroscopy. 2013;29(2):274–9.
17.MorganCD,BurkhartSS,PalmeriM,GillespieM.TypeIISlap lesions:threesubtypesandtheirrelationshipstosuperior instabilityandrotatorcufftears.Arthroscopy.
1998;14(6):553–65.
18.MiyazakiAN,FregonezeM,SantosPD,SilvaLA,SellaGV, SoaresAL,etal.Avaliac¸ãodosresultadosecomplicac¸õesda suturaartroscópicadalesãoSlap.RevBrasOrtop.
2011;46(1):51–6.
19.JobeFW,GiangarraCE,KvitneRS,GlousmanRE.Anterior capsulolabralreconstructionoftheshoulderinathletesin overhandsports.AmJSportsMed.1991;19(5):428–34.