w w w . r b o . o r g . b r
Original
article
Evaluation
of
postoperative
results
from
videoarthroscopic
treatment
for
recurrent
shoulder
dislocation
using
metal
anchors
夽
Éder
Menegassi
Martel
∗,
Airton
Rodrigues,
Francisco
José
dos
Santos
Neto,
Cleiton
Dahmer,
Abel
Ranzzi,
Rafaella
Scuzziato
Dubiela
HospitalOrtopédicodePassoFundo,PassoFundo,RS,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received23February2015 Accepted31March2015 Availableonline13January2016
Keywords:
Sutureanchors Shoulderdislocation Recurrence
Osteoarthritis
a
b
s
t
r
a
c
t
Objective:To clinically and radiologically evaluate the results from videoarthroscopic treatmentusingmetalanchorsinpatientswithrecurrentshoulderdislocationandits com-plications.
Methods:This wasa retrospectivestudy on47 patients (47 shoulders)operatedby the shouldergroupoftheorthopedichospitalbetweenFebruary2010andFebruary2012.A questionnaire,interviewandphysicalandradiographicexaminationswereused,withthe classificationofSamilsonandPietro.Themeanpostoperativefollow-upwas33months (range12–47months).ThestatisticalanalysisconsistedofusingFisher’sexacttestthrough theIBMSPSS22statisticalsoftware.Thesignificancelevelusedwas5%.
Results:Recurrencewasobservedinninecases.Thepatientswere,onaverage,26.5yearsold atthefirstepisode,and19.1%wereaged20yearsorunder.Amongthese,55.6%presented recurrence.Inrelationtoageatthetimeofthesurgicalprocedure,theaverageagewas 27years,and12.8%wereaged20yearsorunder.Nineteenpatientspresentedprominent anchorsand,ofthese,21%manifestedarthrosis.
Conclusion: Therewasastatisticallyidentifiedcorrelationbetweentherecurrencerateand agelessthanorequalto20yearsatthetimesoffirstdislocationandthesurgicalprocedure. Furtherstudiesshouldbeconductedinordertocomparetheuseofabsorbableanchors, whichdespitehighercost,mayprovidelowerriskofdevelopingglenohumeralarthrosisin somecases.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
夽
WorkperformedintheShoulderandElbowGroup,HospitalOrtopédicodePassoFundo,PassoFundo,RS,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](É.M.Martel).
http://dx.doi.org/10.1016/j.rboe.2015.03.015
Avaliac¸ão
de
resultados
pós-operatórios
do
tratamento
videoartroscópico
para
luxac¸ão
recidivante
de
ombro
com
o
uso
de
âncoras
metálicas
Palavras-chave:
Âncorasdesutura Luxac¸ãodoombro Recidiva
Osteoartrite
r
e
s
u
m
o
Objetivos: Avaliarclinicaeradiologicamenteosresultadosdotratamentovideoartroscópico comusodeâncorasmetálicasem pacientescomluxac¸ãorecidivante deombroesuas complicac¸ões.
Métodos: Estudoretrospectivode47pacientes(47ombros)operadosdefevereirode2010 afevereirode2012pelogrupodoombrodohospitalortopédico,pormeiodequestionário, entrevista,examefísicoeradiográfico,comousodaclassificac¸ãodeSamilsonePietro.O seguimentomédionopós-operatóriofoide33meses(variac¸ãode12-47).Aanáliseestatística consistiunousodotesteexatodeFisherpormeiodopacoteestatísticoIBMSPSS22,como usodeumníveldesignificânciade5%.
Resultados: Recidivafoiobservadaemnovecasos.Ospacientestinham,emmédia,26,5 anosnoprimeiroepisódio,dosquais19,1%apresentavamidademenorouiguala20anos. Dentreestes,55,6%apresentaramrecidiva.Emrelac¸ãoàidadenoprocedimentocirúrgico, foiencontradaumamédiade27anos;12,8%apresentavamidademenordoqueouiguala 20anos;19pacientesapresentaramâncorassalientesedesses21%manifestavamartrose.
Conclusão:Houvecorrelac¸ãoestatisticamenteidentificadaentreoíndicederecidivaeaidade menorouiguala20anosnomomentodaprimo-luxac¸ãoedoprocedimentocirúrgico.Mais estudosdevemserfeitosparacompararusodeâncorasabsorvíveis,que,apesardeterum customaiselevado,podemterumriscomenordedesenvolvimentodeartroseglenoumeral emalgunscasos.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Primaryanteriorshoulderdislocationusuallyoccursamong young adultsduring contactsports or among elderly indi-vidualsduetolow-energyfalls.Anteriordislocationamong elderly people has peculiarcomplications, while recurrent instabilityisaparticularproblemofyoungadults.1
Instability symptomsdevelopduring the first twoyears aftertheprimarydislocation,andthisisconsideredtobethe mainprognosticfactor indeterminingtheriskofrecurrent instability.Theexactrecurrencerateremainsuncertain,but itrangesfrom3.9%to3.0%intheliterature.2–8
Overthelastthreedecades,therehavebeengreatadvances in the development of videoarthroscopy techniques. The improvementsinthequalityofthesurgicalimplantsandthe increasinglevelofexperienceofsurgeonshavecontributed toward obtaining results from treating shoulder instability thataremoresatisfactory.1
Theadventofmetalanchorshasmadeitpossibletoreplace the transosseoussuturingtechnique,especially incasesof glenohumeralinstabilityandrotatorcuffinjuries.9,10However,
thismaterialdosnotinherentlyleadtocomplicationssuchas loosening,breakage,migrationand,especiallyincorrect posi-tioninginsidethejoint,whichgivesrisetofrictionagainstthe humeralheadorglenoidcavityandcausesvaryingdegreesof chondrallesionandearlyglenohumeralarthrosis.11,12
Thepresent study compriseda retrospective evaluation offactors that might influencethe surgical results among patientsundergoingvideoarthroscopictreatmentofrecurrent shoulderdislocationwithuseofmetalanchors.Thefindings
andclinicalrepercussionsreportedintheliteraturewere dis-cussed.
Methods
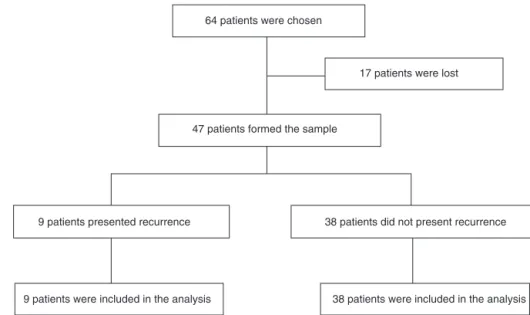
Inthisretrospectivestudy,47patients(47shoulders)outof the60operatedbytheshoulderandelbowgroupofan ortho-pedichospitalwereevaluated.Theother17patientswerelost duringthefollow-up(Fig.1).Themedicalfilesofpatientswho underwentvideoarthroscopictreatmentusingmetalanchors betweenFebruary2010andFebruary2012werereviewed.
Patients with recurrentshoulder instabilityand a mini-mum postoperativefollow-up of12 months were included inthe study,without regardforsex. Patientswho received absorbable anchors, cases ofosteoarthrosis seen on radio-graphs before the operation and cases presenting other pathological conditionsoftherotator cuff,neckorbrachial plexuswereexcluded.
64 patients were chosen
17 patients were lost
47 patients formed the sample
9 patients presented recurrence 38 patients did not present recurrence
9 patients were included in the analysis 38 patients were included in the analysis
Fig.1–Characteristicsofthestudy.
Duringtheevaluation,aquestionnairewasappliedtothe patients to characterize the sample. Theissues addressed included personal data, age, occupation, sports practice, dominance,numberofanchors,traumaticornon-traumatic preoperativeepisodesofdislocationandavisualpainscale. Thephysicalexaminationconsistedofbilateralevaluationof therangeofmotion,apprehensiontest,relocationtest, sul-custest,anteriorandposteriordrawertest,hyperlaxity(lateral rotation>85◦)andhyperabductiontest.Thepatientswerealso
evaluated radiographicallyregarding the positioning ofthe anchors,existenceofbonealterationsintheglenohumeral cavityandsigns ofarthrosis asdescribedbySamilson and Prietro15(Table1).
All the participants signed a free ad informed con-sent statementbefore any evaluationrelating tothe study was performed. Theproject was properly approved bythe ResearchEthicsCommitteeoftheUniversityofPassoFundo, through the Brazil Platform, on January 8, 2014 (CAAE: 19258813.1.0000.5342).
Surgicaltechnique
Thesurgicalprocedurewasperformedwiththepatientunder generalanesthesia andbrachialplexusblock, positionedin lateraldecubitusonthesideoppositetotheaffected shoul-der.Onthe surgicaltable,verticalandlongitudinaltraction
Table1–RadiologicalclassificationofSamilsonand
Pietro.
TypeI Mildarthrosis:inferiorhumeralexostosisand/or glenoidexostosismeasuring<3mminheight. TypeII Moderatearthrosis:inferiorhumeralexostosis
and/orglenoidexostosismeasuring3mmto7mm withslightglenohumeralirregularity.
TypeIII Severearthrosis:inferiorhumeralexostosisand/or glenoidexostosismeasuring>7mmwithjoint narrowingandglenohumeralsclerosis.
wereappliedandthelimbwaskeptpositionedinabduction ofapproximately30◦andflexionof15◦.
Aposteriorportalwasusedforvideoarthroscopy,located 2cmdistallyand2cmmediallytotheposterolateralangleof theacromion.Intheanteriorregionoftheshoulder,another twoportalswere openedinorder toplace cannulae.These werealwayskeptlaterallytothecoracoidprocessinorderto minimizepossiblevesselandnervelesions.Beforethe can-nulaewereemplaced,thejointwasinvestigated,takingthe referencepointofthelongtendonofthebicepsandits supe-riorlabralinsertion.Theanterior,inferiorandposteriorlabra, joint surfaces,ligaments,capsule,recessesand rotatorcuff werethenevaluated.
Followingthis,theopticaldevicewastakentothe antero-superiorportalandtheirrigationwasmovedtotheposterior portal, forawider viewofthe anteriorlabrum,which was highlightedandthenopenedupusingashaverbladeinorder toobtainabedsuitableforhealingofthereinserted capsu-lolabralcomplex.Thesameprocedurewasperformedonthe surfaceoftheglenoidborder,fromwherethelabrumhad orig-inallybeendeinserted.Inthis,inadditiontodebridementof theremainingsifttissues,wealsousedanabrasionbladeto scarifythesubchondralbone.
Afterthedebridementthatwasnecessaryhadbeen per-formed,thelabrumwasreinsertedintoitsorigin,bymeans ofasuturingtechniqueusinganchors.Wepreferentiallyused threemetalanchorsofdimensions2.7mm×5.0mmloaded withFiberWire®no.2.Plicationofthecapsulewasdonein conjunctionwiththelabralsuturingtechniqueinthecases that presentedwith threeor moreepisodes ofdislocation. SlidingGiantknotswereusedforfixation.16
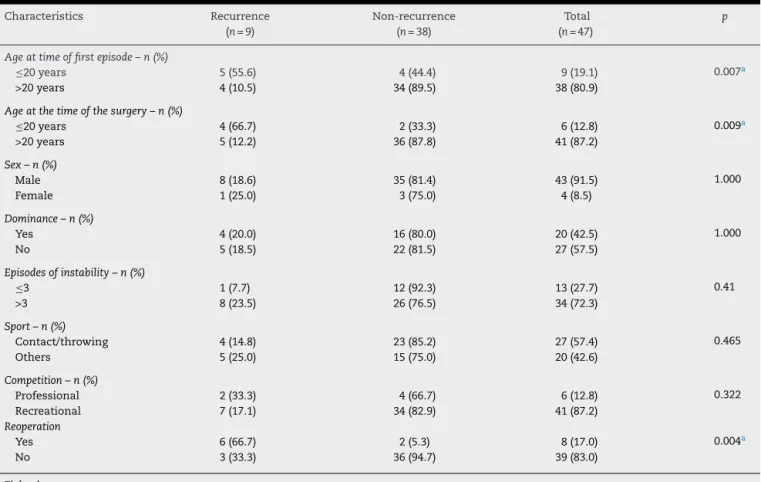
Table2–Patients’characteristics.
Characteristics Recurrence Non-recurrence Total p
(n=9) (n=38) (n=47)
Ageattimeoffirstepisode–n(%)
≤20years 5(55.6) 4(44.4) 9(19.1) 0.007a
>20years 4(10.5) 34(89.5) 38(80.9)
Ageatthetimeofthesurgery–n(%)
≤20years 4(66.7) 2(33.3) 6(12.8) 0.009a
>20years 5(12.2) 36(87.8) 41(87.2)
Sex–n(%)
Male 8(18.6) 35(81.4) 43(91.5) 1.000
Female 1(25.0) 3(75.0) 4(8.5)
Dominance–n(%)
Yes 4(20.0) 16(80.0) 20(42.5) 1.000
No 5(18.5) 22(81.5) 27(57.5)
Episodesofinstability–n(%)
≤3 1(7.7) 12(92.3) 13(27.7) 0.41
>3 8(23.5) 26(76.5) 34(72.3)
Sport–n(%)
Contact/throwing 4(14.8) 23(85.2) 27(57.4) 0.465
Others 5(25.0) 15(75.0) 20(42.6)
Competition–n(%)
Professional 2(33.3) 4(66.7) 6(12.8) 0.322
Recreational 7(17.1) 34(82.9) 41(87.2)
Reoperation
Yes 6(66.7) 2(5.3) 8(17.0) 0.004a
No 3(33.3) 36(94.7) 39(83.0)
Fisher’sexacttest.
a Significantvalue,forp≤0.05.
Methodologyofthestatisticalanalysis
Thedata analysiswas done bymeans ofthe IBMSPSS 22 statisticpackage.Fisher’sexacttestwasusedtoanalyze asso-ciationsbetweenthevariables.Thesignificancelevelusedwas
p≤0.05.
Results
Duringthestudyperiod,47patientswereanalyzed.Among these,nine(19.1%)presentedrecurrence.Thepatients’mean ageatthetimeofthefirstepisodewas26.5years,and19.1% ofthemwereofageslessthanorequalto20years.Among thesepatientswhoseageswerelessthanorequalto20years atthe time ofthe first dislocation, 55.6% presented recur-rence.Thiswas statisticallysignificant:p=0.007; RR=5.278; 95%CI=[1.764;15.789](Table2).
Thepatients’meanageatthetimeofthesurgical proce-durewas27 years,withaminimumageof17 yearsand a maximumof52years;12.8%presentedageslessthanorequal to20years.Thesepatientsrepresented66.7%ofthegroupthat presentedrecurrence,andthisproportionwasstatistically sig-nificant,withachanceofrecurrencethatwasapproximately 5.5timesgreater:p=0.009;RR=5.467;95%CI=[2.016;14.821]. In this sample, four women and 43 men underwent operations,and this didnotshown any statistically signif-icant difference through Fisher’s exact test. Eight cases of
recurrence(n=9)wereamongmen;81.4%ofthemenand75% ofthewomendidnotpresentrecurrence.Thedominantside wasinvolvedin20patients(42.5%).Therewasnoassociation, from a statistical point of view, between recurrence and dominance(p=1.000).
Regardingthenumberofepisodesofinstability,34patients presentedmorethanthreeepisodesand,ofthese,23.5% pre-sentedrecurrence.However,92.3%ofthepatientswiththree or fewerepisodesdidnotpresentrecurrence.Nostatistical differencewasfound.
Inanalyzingtherelationshipbetweenthepresenceofbone lesionsintheglenoidandrecurrences,90.5%ofthepatients whopresentedlesionswereamongthosewhodidnotpresent. There was no statisticallysignificant correlation(p=0.519). Equally, therewasno statisticalsignificancewithregardto shouldersthatpresentedHill-Sachslesion.Only12%werein thegroupthatpresentedrecurrence(p=0.216)(Table3).One patientpresentedadiagnosisofassociatedSLAPlesion,which wasrepairedatthetimeofthesurgeryandpresentedgood evolution.
Therewerereportsofpainin31.9%ofthecases.Themean numberofanchorswas3.1(rangefrom2to5).Inthegroup withrecurrences,thenumberofanchorsrangedfromtwoto three(meanof2.9).Fiveofthenewrecurrenceswere associ-atedwithtrauma.
Table3–Complications/radiographicfindings.
Complications/radiographicfindings Recurrence Non-recurrence Total p
(n=3) (n=38) (n=41)
Salientanchor–n(%)
Yes 1(5.3) 18(94.7) 19(46.3) 0.556
No 2(9.1) 20(90.9) 22(53.7)
Arthrosis/SamilsonI–n(%)
Yes 0(0.0) 4(100.0) 4(9.8) 0.729
No 3(8.1) 34(91.9) 37(90.2)
Glenoidlesions
Yes 2(9.5) 19(90.5) 21(51.2) 0.519
No 1(5.0) 19(95.0) 20(48.8)
Hill-Sachs
Yes 3(12.0) 22(88.0) 25(61.0) 0.216
No 0(0.0) 16(100.0) 16(39.0)
Fisher’sexacttest.
Significantvalue,forp≤0.05.
Table4–Arthrosisinshoulderswithsalientanchors.
Characteristic Arthrosis/SamilsonI–n(%) Total p
Yes No
Salientanchor–n(%)
Yes 4(21.1) 15(78.9) 19(46.3) 0.038a
No 0(0.0) 22(100.0) 22(53.7)
Fisher’sexacttest.
a Significantvalue,forp≤0.05.
analyzed.Wealsofoundonepatientwithabrokenanchor, whopresentedgoodevolution.
Furthermore, in relation to the presence of prominent intra-articularanchors(Fig.2),theresultsdidnotshow statis-ticallysignificantvaluesamongthevariablestested.Itshould benotedthatonlyonecaseofprominenceofananchorwas
Fig.2–Viewofintra-articularsalientanchors.
foundinthegroupofrecurrences,andtherewere19casesin total.Amongthe19patientswhopresentedsalientanchors, 21.1%(four)presentedarthrosis(Fig.3),whichwasstatistically significant,withp=0.038(RR=0.789;95% CI=[0.626;0.996]). Thus,presenceofasalientanchorrepresentedariskfactor fordevelopmentofarthrosisaftertheoperation.
Discussion
Videoarthroscopictreatmentforanteriorshoulderdislocation isamatterofcontroversy.Thus,anyprocedurethathasthe aimofstabilizingtheglenohumeraljointshoulddosowitha minimumoflossofmovement.14
Inthepresentstudy,ninepatients(19.1%)presented recur-rence.Three ofthemhave sofar chosennotto undergo a newsurgicalinterventionandsixhaveundergoneopenrepair usingabonegraft.Inasampleof106patientstreatedusing thestapling techniquein1982,Johnson17 (who wasoneof
thepioneersofvideoarthroscopicrepairfortraumaticanterior instability)showedarecurrencerateof21%.Kossetal.6
stud-ied27patientswhounderwentarthroscopicrepairofBankart lesionsandreportedthattherecurrenceratewas30%. Follow-ingthesametrend,Sadovsketal.7reviewed77patientswho
had been treated videoarthroscopically and found a recur-rencerateof3.9%.Tanet al.8foundthatvideoarthroscopic
anteriorstabilizationoftheshoulderseemedtobeeffective, withafailure rateof9%;85% oftheir patientsreturned to theirsportsactivities.Theyobservedthatabsorbableand non-absorbableanchorsseemedtobeequallyeffective,without anysignificantdifferences.
We found that failure of postoperative stabilization occurredin19.1%.Thispercentagewasinlinewiththe lit-eraturewithregardtorepairsusinganchors,giventhatthe rates presented have ranged from 3.9% to 30%.6–8 Among
thepatientswhopresentedrecurrenceandunderwentopen repair,theLatarjettechniquewasappliedinfivecasesandthe Bristowtechniqueinonecase,sofarwithoutanyrecurrences. However,Griesseretal.18conductedasystematicreviewon
theoriginalormodifiedprocedures ofBristowandLatarjet, whichare currentlyconsideredto bethegoldstandard for repairingbonelesions,andfoundthattherewasa substan-tialriskofcomplications(30%),includingrecurrentdislocation (2.9%)andreoperation(6.9%).
Ina randomizedprospectiveseriesof40 patients, Mag-nusson et al.19 compared two different videoarthroscopic
techniquesfortreatingBankartlesionsusingbioabsorbable and non-absorbable implants, in relation to function and arthropathy.Thepatientswereevaluatedsixand24months aftertheoperation,andrecurrenceofdislocationwasfound in5%.Arthropathywasreportedin30%(fivemildcasesand onemoderatecase)inthenon-absorbablegroupandin33% intheabsorbablegroup(sixmildcases).
In a systematic review with meta-analysis on 62 stud-ies with 3044 videoarthroscopy procedures, Hobby et al.20
concludedthatthemosteffectivetechniquesfor videoarthro-scopicstabilizationhadfailureratessimilartothatofopen stabilization,aftertwoyearsoffollow-up.
Inaretrospectivereviewarticleon570patients,Buscayret etal.21reportedthattheincidenceofglenohumeralarthrosis
was19.7%afterameanfollow-upof6.5years,subsequentto anoperationtoobtainanteriorshoulderstabilizationusinga varietyofmetalanchors.Kaaretal.11described eightcases
ofcomplicationsfrom useofmetalanchors:threeofthese evolvedwithchondral lesionsofthe humeralhead,among whichtwowereduetomechanicalfrictionfromtheanchors andonewasduetoassociatedinfection.
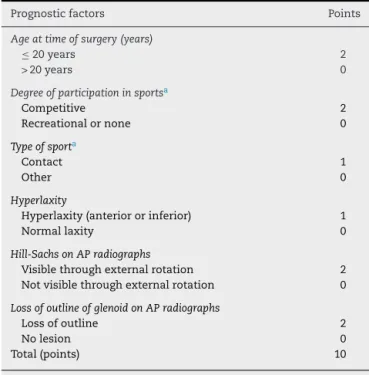
Table5–InstabilitySeverityIndexScore(ISIS),from
preoperativeevaluation.
Prognosticfactors Points
Ageattimeofsurgery(years)
≤20years 2
>20years 0
Degreeofparticipationinsportsa
Competitive 2
Recreationalornone 0
Typeofsporta
Contact 1
Other 0
Hyperlaxity
Hyperlaxity(anteriororinferior) 1
Normallaxity 0
Hill-SachsonAPradiographs
Visiblethroughexternalrotation 2 Notvisiblethroughexternalrotation 0
LossofoutlineofglenoidonAPradiographs
Lossofoutline 2
Nolesion 0
Total(points) 10
AP,anteroposterior.
a Degreeofparticipationinsportsandtypeofsportwereevaluated
beforetheoperation.
Inaretrospectivestudyoneightpatients,Ejnismanetal.22
concludedthatimproperinsertionofmetalanchorsin gleno-humeralsurgicalproceduresforfixationoflabrallesionscould leadtoextensivearthropathyoftheshoulderjoint.Thus,with delays inreachingthe correctdiagnosis, thiscould leadto earlyglenohumeralarthrosis.
Inourstudy,wefoundfourpatients(21.1%)witharthrosis. WeonlyfoundtypeIarthrosis,probablybecauseoftheshort postoperativeperiodofupto47months.Twopatientsevolved witharthrosis,evenafterrepositioningoftheanchors.The intervalbetweenthefirstandsecondsurgicalprocedureswas sixtoeightmonths.Furthermore,presenceofsalientanchors wasshownonradiographsinthecasesof19patients(46.3%). However,onlyfourpatients(21.1%)developedarthrosis.This suggeststhatsalientanchorsseenonradiographsarenota goodpredictorforevolutionofglenohumeralarthrosis.Thus, videoarthroscopywouldbethepreferredmethodfor diagnos-ingpoorlyplacedanchors,sincethisprovidesdirectviewing oftheglenohumeraljoint.
BurkhartandDeBeer23analyzed194casesof
videoarthro-scopicrepairsofBankartlesionsandconcludedthatpatients whowerecandidatesforvideoarthroscopicsurgeryneededto befreefrom significantbonefailures(Hill-SachsorBankart lesions in whichthe glenoid has the shape ofaninverted pear),andthatcontactathleteswithoutbonelesionscouldbe treatedusingthismethod.Theyalsoconcludedthatthe Latar-jetprocedureshouldbereservedforpatientswithsignificant bonelossfromtheglenoid.
Balg et al.24 conductedaprospective case-control study
of14.5%.They identified six riskfactors that predicted an increasedrecurrence rateandcreated theInstability Sever-ity Index Score (ISIS), which ranged from 0 to 10 points (Table5).Theyconcludedthatscoresgreaterthansixpoints representedarecurrenceriskof70%aftervideoarthroscopic repair.
Inarecentreviewoftenarticlesthatcomparedabsorbable andnon-absorbableanchors,Papaliaetal.25concludedthatit
wasnotpossibletosuggestwhichmethodwouldbetheone recommendedforroutineuse.Thus,thecost–benefit relation-shipwouldneedtobetakenintoconsideration.
Longoetal.26 conductedasystematicreviewon46
arti-clesthatdealtwithdifferenttechniquesforrecurrentshoulder dislocation.TheyconcludedthattheBristowandLatarjet pro-cedurescontinuedtobeagoodsurgicaloption fortreating post-traumaticanteriorshoulderinstability.TheBristowand Latarjetvideoarthroscopicproceduresseemedtohavebetter resultsinrelationtopreventionofrecurrenceand rehabilita-tion,butrandomizedstudieswouldbenecessaryinorderto reachdefinitiveconclusions.
Thepresentstudyhassomelimitations,suchastheshort durationofthefollow-up(rangingfrom12to47months)and thelossof17patientsfromthefollow-up.Wedidnotevaluate theUCLAscaleortheCarter-Rowescore.
Conclusion
Useofmetalanchorsisnolongerthebestmethodtochoose, giventhepotentialriskofrecurrenceandarthrosis,and there-foreother techniques needto betaken into consideration. Furtherstudiesare neededonordertocomparetheuse of absorbableanchors,which despitehavinghigher cost,may giverisetolowerriskofdevelopmentofglenohumeral arthro-sisinsomecases.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. GodinhoGG,Franc¸aFO,FreitasJMA,MenezesCM,FreireSG, WanderleyAL,etal.Tratamentoartroscópicodainstabilidade anteriortraumáticadoombro:resultadosalongoprazoe fatoresderisco.RevBrasOrtop.2008;43(5):157–65.
2. ChecchiaSL,SantosPD,MiyazakiAN,SilvaLA,FregoneziM. Afecc¸õesdoombroecotovelo.In:CamargoOPA,SantinRAL, OnoNK,KojimaKE,editors.Ortopediaetraumatologia: conceitosbásicos,diagnósticoetratamento.SãoPaulo:Roca; 2004.p.126–47.
3. RobinsonCM,DobsonRJ.Anteriorinstabilityoftheshoulder aftertrauma.JBoneJointSurgBr.2004;86(4):469–79.
4. PötzlW,WittKA,HackenbergL,MarquardtB,SteinbeckJ. Resultsofsutureanchorrepairofanteroinferiorshoulder instability:aprospectiveclinicalstudyof85shoulders.J ShoulderElbowSurg.2003;12(4):322–6.
5. ItoiE,HatakeyamaY,SatoT,KidoT,MinagawaH,
WakabayashiI,etal.Immobilizationinexternalrotationafter shoulderdislocation:aninterimreportofanongoingtrial
[abstract].In:9thinternationalcongressonsurgeryofthe shoulder.2004.
6.KossS,RichmondJC,WoodwardJSJr.Two-tofive-year follow-upofarthroscopicBankartreconstructionusinga sutureanchortechnique.AmJSportsMed.1997;25(6): 809–12.
7.SadovskÃP,MusilD,StehlÃkJ.Arthroscopicstabilizationof theshoulder.ActaChirOrthopTraumatolCech.
2006;73(1):23–7.
8.TanCK,GuisasolaI,MachaniB,KempG,SinopidisC, BrownsonP,etal.Arthroscopicstabilizationoftheshoulder:a prospectiverandomizedstudyofabsorbableversus
nonabsorbablesutureanchors.Arthroscopy. 2006;22(7):716–20.
9.BarberFA,HerbertMA,RichardsDP.Suturesandsuture anchors:update2003.Arthroscopy.2003;19(9):985–90.
10.BacillaP,FieldLD,SavoieFH3rd.ArthroscopicBankartrepair inahighdemandpatientpopulation.Arthroscopy.
1997;13(1):51–60.
11.KaarTK,SchenckRCJr,RockwoodCAJr.Complicationsof metallicsutureanchorsinshouldersurgery:areportof8 cases.Arthroscopy.2001;17(1):31–7.
12.SilverMD,DaigneaultJP.Symptomaticinterarticular migrationofglenoidsutureanchors.Arthroscopy. 2000;16(1):102–5.
13.SnyderSJ,StraffordBB.Arthroscopicmanagementof instabilityoftheshoulder.Orthopedics.1993;16(9):993–1002.
14.AlmeidaFilhoIA,VeadoMAC,FimM,CorreaLVS,Carvalho JuniorERA.Avaliac¸ãofuncionaldoreparoartroscópicoda instabilidadeanteriorrecidivantedoombro.RevBrasOrtop. 2012;47(2):214–21.
15.SamilsonRL,PrietoV.Dislocationarthropathyofthe shoulder.JBoneJointSurgAm.1983;65(4):456–60.
16.FleegaBA.TheGiantKnot:anewone-wayself-locking securedarthroscopicslipknot.Arthroscopy.1999;15(4): 451–2.
17.JohnsonLL.Arthroscopyoftheshoulder.OrthopClinNorth Am.1980;11(2):197–204.
18.GriesserMJ,HarrisJD,McCoyBW,HussainWM,JonesMH, BishopJY,etal.Complicationsandre-operationsafter Bristow–Latarjetshoulderstabilization:asystematicreview.J ShoulderElbowSurg.2013;22:286–92.
19.MagnussonL,EjerhedL,Rostgård-ChristensenL,SernertN, ErikssonR,KarlssonJ,etal.Aprospective,randomized, clinicalandradiographicstudyafterarthroscopicBankart reconstructionusing2differenttypesofabsorbabletacks. Arthroscopy.2006;22(2):143–51.
20.HobbyJ,GriffinD,DunbarM,BoileauP.Isarthroscopic surgeryforstabilizationofchronicshoulderinstabilityas effectiveasopensurgery?Asystematicreviewand meta-analysisof62studiesincluding3044arthroscopic operations.JBoneJointSurg.2007;89-B:1188–96.
21.BuscayretF,EdwardsTB,SzaboI,AdeleineP,CoudaneH, WalchG.Glenohumeralarthrosisinanteriorinstabilitybefore andaftersurgicaltreatment:incidenceandcontributing factors.AmJSportsMed.2004;32(5):1165–72.
22.EjnismanB,AndreoliCV,PochiniAC,MonteiroGC,FaloppaF, CohenM.Artropatiaglenoumeralpós-tratamentodelesões labiaiscomimplantesmetálicos.RevBrasOrtop.
2006;41(5):167–72.
23.BurkhartSS,DeBeerJF.Traumaticglenohumeralbonedefects andtheirrelationshiptofailureofarthroscopicBankart repairs:significanceoftheinverted-pearglenoidandthe humeralengagingHill-Sachslesion.Arthroscopy. 2000;16(7):677–94.
25.PapaliaR,FranceschiF,BalzaniLD,D’AdamioS,DenaroV, MaffulliN.Thearthroscopictreatmentofshoulderinstability: bioabsorbableandstandardmetallicanchorsproduce equivalentclinicalresults.Arthroscopy.2014;30(9): 1173–83.