SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
Article
Surgical
treatment
of
intraarticular
fractures
of
the
calcaneus:
comparison
between
flat
plate
and
calcaneal
plate
夽
Luiz
Carlos
Almeida
da
Silva
∗,
João
Mendonc¸a
de
Lima
Heck,
Marcelo
Teodoro
Ezequiel
Guerra
UniversidadeLuteranadoBrasil(Ulbra),HospitalUniversitário,Canoas,RS,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received16February2016
Accepted2May2016
Availableonline29December2016
Keywords:
Calcaneus/injuries Calcaneus/surgery
Fractures,bone/surgery
Fracturefixation,internal
a
b
s
t
r
a
c
t
Objective:Toevaluatetheclinicalresultsofsurgicaltreatmentofintraarticularfracturesof
thecalcaneus,comparingtheuseofcalcanealplateandflatplate.
Methods:Thiswasaretrospectivestudyassessingthepostoperativeresultsof25patients
between2013and2015.Patientsundergoingsurgicaltreatmentofintraarticularfractures
ofthecalcaneuswithoutconcomitantsurgicallesionswereincluded.Patientswhodidnot
completeappropriatefollow-upaftersurgerywereexcludedfromthestudy.
Results:Theunavailabilityofcalcanealplatesatresource-limitedsettings,associatedwith
theavailabilityandlowercostofflatplates,mayhavebeenaconfoundingfactorinthe
presentstudy.However,therewasnostatisticaldifferencebetweentheoutcomesof
frac-turestreatedwithcalcanealplatesorflatplates.
Conclusion: Statisticalinferenceshowsthat,whencalcanealplatesarenotavailable,itis
possibletouseflatplateswithsimilarclinicaloutcomes.
©2016PublishedbyElsevierEditoraLtda.onbehalfofSociedadeBrasileiradeOrtopedia
eTraumatologia.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http://
creativecommons.org/licenses/by-nc-nd/4.0/).
Tratamento
cirúrgico
das
fraturas
intra-articulares
do
calcâneo:
comparac¸ão
dos
resultados
entre
placa
reta
e
placa
própria
para
calcâneo
Palavras-chave:
Calcâneo/lesões Calcâneo/cirurgia
Fraturasósseas/cirurgia
Fixac¸ãointernadefraturas
r
e
s
u
m
o
Objetivo:Avaliarosresultadosclínicosdotratamentocirúrgicodasfraturasintra-articulares
docalcâneo(TCFIAC)ecompararousodeplacaprópriaparacalcâneo(PPC)eplacareta(PR).
Métodos:Estudoretrospectivoqueavaliouoresultadopós-operatóriode25pacientesentre
2013e2015.Foramincluídos pacientessubmetidosaoTCFIACequenãoapresentavam
lesõescirúrgicasconcomitantes.Pacientesquenãoforamdevidamenteacompanhadosno
pós-operatórioforamexcluídosdaanálise.
夽
StudyconductedattheUniversidadeLuteranadoBrasil(Ulbra),HospitalUniversitário,DepartamentodeOrtopediaeTraumatologia,
Canoas,RS,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](L.C.Silva).
http://dx.doi.org/10.1016/j.rboe.2016.05.007
2255-4971/©2016PublishedbyElsevierEditoraLtda.onbehalfofSociedadeBrasileiradeOrtopediaeTraumatologia.Thisisanopen
Resultados: AindisponibilidadedaPPCemservic¸oscomrecursoslimitados,associadaà
disponibilidadeeaomenorcustodaPR,podetersidofatordeconfusãonopresenteestudo.
Contudo,nãohouvediferenc¸aestatísticaentreosresultadosdasfraturastratadascomPPC
ouPR.
Conclusão:Ainferênciaestatísticapermiteconcluirque,naausênciadaPPC,épossívelusar
aPRcomdesfechosclínicossemelhantes.
©2016PublicadoporElsevierEditoraLtda.emnomedeSociedadeBrasileirade
OrtopediaeTraumatologia.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND
(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Calcanealfracturescorrespondto2%ofskeletalfracturesand
about60%offracturesofthetarsalbones.1,2Despitethegreat
developmentoforthopedictraumatologyinthelastcentury,
treatmentofthesefracturesisstillcontroversialandresults
areoftenunsatisfactory,duetothecomplexanatomicalshape
ofthecalcaneus,itscancellousstructure,andthefactthatitis
subjectedtoconstantweightload.3–6Thus,thisinjurycauses
majorsocioeconomicandfunctionalimpairmenttopatients,
andrepresentsaburdentopublicandprivatecompensation
policies.1
Inrecentdecades,withtheimprovementofimaging
stud-ies,a better understanding of the mechanisms oftrauma,
andobservanceoftheprinciplesofanatomicalreductionand
absolute stability for joint fractures, it is now possible to
improve clinical outcome forthis typeoffracture. For this
purpose,severaltypesofimplantsareavailable,including
cal-canealplates(CP)andflatplates(FP).7
Therefore,this study aimedtoevaluatethe clinical
out-comesofsurgicaltreatmentofintra-articularfracturesofthe
calcaneus(STIAFC)andcomparetheuseofCPandFP.
Material
and
methods
Thiswasaretrospectivecohortstudy,whichevaluatedlate
postoperative resultsof 25 patients operatedbetween
Jan-uary 2013 and January 2015. This study was approved by
theResearchEthicsCommitteeunderNo.117817/2014/CAAE
40266114.9.0000.5328.
Inclusioncriteriacomprisedpatientswhounderwent
sur-gicaltreatmentbyopenreductionandinternalfixation(ORIF)
ofaunilateralcalcanealintra-articularclosedfracturewithout
otherassociatedfractures,whohadpreoperativecomputed
tomographyandradiographsofthefoot,ankle,andcalcaneus,
andwhohadsignedaninformedconsentform.
Exclusioncriteriawerepatientswhowereoperatedusing
theEssex-Loprestitechniqueorthoseinwhomaminimally
invasive surgery was performed; fractures treated
conser-vatively due to patient’s own reasons or lack of surgical
indication;associatedfractures;lackofadequate skin
con-dition,edema,andblistersinthelateral aspectofthefoot,
not resolved by the date of the surgery; absence of
clini-cal conditions due to vascular disorders, heart disease,or
decompensateddiabetes;severetraumaticbraininjury;
psy-chosocialproblem;heavysmoking;refusaltoundergosurgical
treatment;bilateralfractures;andrefusaltosigntheinform
consentform.
Duringthisperiod,64feetof52patientswereoperatedby
thesamesurgeon.Allpatientswerecalledforreevaluation;
25patientsundergoingSTIAFCmettheinclusioncriteriaand
wereincludedinthestudy.
Allpatientswereevaluatedbythesamesurgeonwho
per-formedallsurgeries.Thefollowingassessmentscales were
used:AmericanOrthopaedicFootandAnkleSociety(AOFAS),
theGlobalSocialFunctioningScale(GSFS),visualanalog(VAS),
andtheMedicalOutcomesStudy36(SF-36).8
Clinically, the followingaspectswere analyzed: subtalar
joint in the standing and supinepositions; varus and
val-gusdeviationofthehindfoot;abduction;adduction;pronation
andsupinationoftheforefoot;rangeofmotionforankle
flex-ionandextension;appearanceofsurgicalscars;andneedfor
crutches.Fortheclassificationoffractures,theSanders9and
Essex-Lopresti10classificationswereused.
Similarly,allpatientsunderwentlatepostoperative
anal-ysis with radiographic study in Bröden’s view; calcaneus
radiographsinprofileand axial;bilateral radiographic
eval-uation of the feet with monopodal support; radiographic
evaluationoftheankleinprofile,anteroposterior,andin15◦of
internalrotation;andbilateralcomputedtomographywith
5-mmthickaxial,coronal,andsagittalcuts.
Thesamplewasdividedintotwogroupsaccordingtothe
typeofORIFmade.GroupIconsistedofpatientstreatedwith
3.5-mmone-thirdtubularFP.GroupIIincludedpatients
under-goingtreatmentwithCP.
Thecriterionforthechoiceofmaterialwasrandomand
based onthepossibilityofusingCP,whichwasnotalways
available.Asfixationcriteria,isolatedFPortwocombinedFP
wereusedwhenCPwasnotavailable.CPwasusedwhenever
available.
AllpatientswereoperatedwiththeclassicL-shaped
lat-eralaccessroute,starting3cmfromtheposteriorregionof
thelateralmalleolus,passing3cmbelowthat,extendingto
thecalcaneocuboidjoint.Duetothehighriskofskin
necro-sis,dissectionwasmadeatthesubperiosteallevel.Theflap
wasfoldeddownandmaintainedcraniallywiththree2.0mm
Kirschnerwiresattachedtothetalus,withvisualizationofthe
sheathoftheperoneusmuscles, whichwaspreferably
pre-served.Underdirectvisualizationofthefracture,reduction
wascarriedout,withtemporaryfixationusingKirschnerwires
performedafterintraoperativeradiographicconfirmationof
thereduction.DefinitefixationwasmadewitheitherCPor
FP.Afterclosurebyplanes,anelasticcompressionbandage
Table1–Demographicandclinicalcharacteristicsofthesample.
Typeofplate pa
CP(n=14) FP(n=11)
Age 47.7 10.4 45.5 11.29 0.617a
Sex 0.230
Female 3 21.4% 0 0.0%
Male 11 78.6% 11 100.0%
Traumamechanism 1.000
Bicycle×motorcyclecollision 1 7.1% 0 0.0%
Fallfromheight 13 92.9% 11 100.0%
Operatedside 0.414
Right 7 50% 8 72.7%
Left 7 50% 3 27.3%
Rearfootpositioninorthostasis 0.695
Neutral 8 57.1% 5 45.5%
Valgus 6 42.9% 6 54.5%
Subtalararthrosis 1.000
No 5 35.7% 3 27.3%
Yes 9 64.3% 8 72.7%
CP,calcanealplates;FP,flatplates.
a p-valueforFisher’sexacttest.
weeks.Partialloadwasauthorizedatthesixthpostoperative
week.Autograftstofillthespacecreatedinsidethecalcaneus
werenotused.
Quantitative variables were described as mean and
standard deviation; categoricalvariables were described as
simple(n)andrelative(%)frequency.Toassessthemean
dif-ferencebetweentypesofmaterial,thet-testforindependent
samplestestwas used.To verify theexistenceofan
asso-ciationbetweentypesofmaterialandcategoricalvariables,
Fisher’sexact testwasused. Thesignificancelevel wasset
at5%.StatisticalanalyseswereperformedwithSPSSversion
18.0.
Results
Regardinggender,amongpatientsundergoingtreatmentwith
CP,11(78.6%)weremenandthree(21.4%)werewomen.Among
patientswhoweretreatedwithRP,11(100%)weremen.
Regardingtypeoftrauma,ofthepatientsundergoing
treat-mentwithCP,one(7.1%)hadsufferedtraumaduetoabicycle
collisionwithamotorcycleand13,fallfromheight;inturn,
all11(100%)patientstreatedwithFPhadsufferedafallfrom
height(Table1).
TheoperatedsideofpatientstreatedwithCPwastheright
sideinsevenpatients(50%)andleftinseven(50%).Among
patientsundergoingtreatmentwithFP,eight(72.7%)hadthe
rightsideoperatedandthree(27.3%),left.
Regardingthepostoperativepositionofthehindfootwhile
standing,amongpatientswhounderwenttreatmentwithCP,
eight(57.1%)presentedthehindfootinaneutralposition,and
six(42.9%),hindfootinvalgus.Inturn,amongpatientswho
underwenttreatmentwithFP,five(45.5%)presentedthe
hind-footinaneutralpositionandsix(54.5%)invalgus.
Regardingsubtalararthrosis,amongpatientswho
under-wenttreatmentwithCP,five(35.7%)evolvedwithoutsubtalar
arthrosisandnine(64.3%)presentedit.Amongpatientswho
underwenttreatmentwithRP,three(27.3%)evolvedwithout
subtalararthrosis,whileeight(72.7%)developedthecondition
(Table1).
Regardingtheclassificationoffractures,19patients(76%)
hadjointdepressionfractureandsix(24%),tongue-type
frac-ture.AsfortheSandersclassification,eight(32%)patientshad
type2Afracture;two(8%),type2B;six(24%),type3AB;three
(12%), type3AC;two(8%), type3BC;andfour (16%),type4
(Table2).
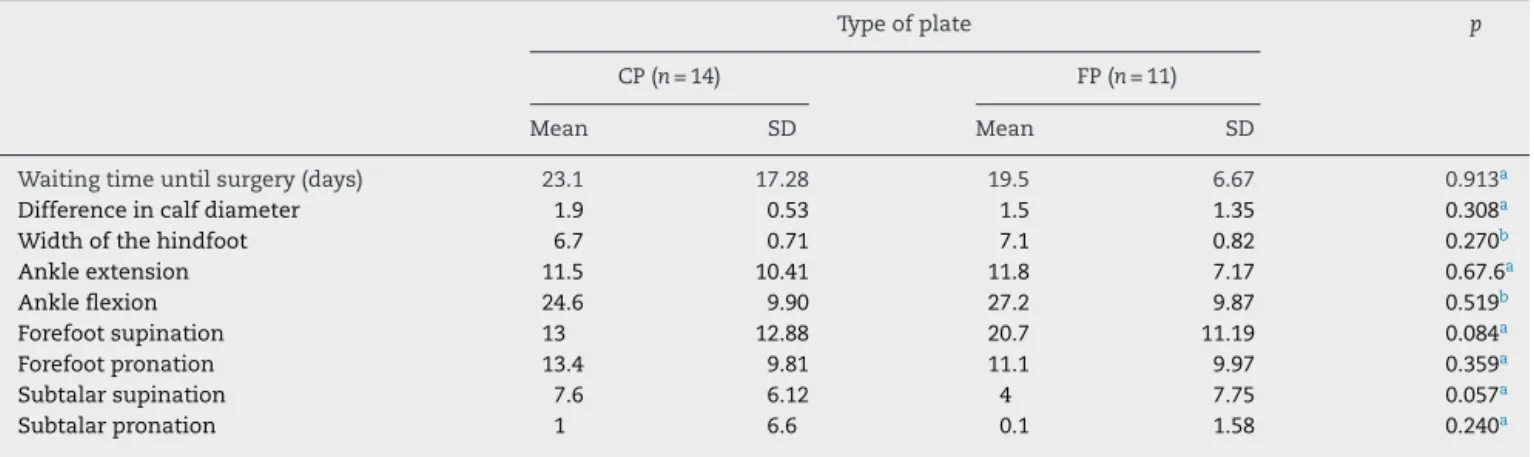
The results of both groups regarding waiting time for
surgery and physical examination are shown in Table 3.
Regarding clinical assessmentscales, Tables 4and 5 show
resultswithoutstatisticaldifferencebetweenthetwotypesof
plates.Therefore,therewasnodifferenceinclinicaloutcomes
betweenORIFinthecomparisonofCPandFP.
Table2–Classificationoffractures.
Typeofplate pa
CP(n=14) FP(n=11)
Essex-Lopresticlassification 0.350 Jointdepression 12 85.7% 7 63.6%
Tongue 2 14.3% 4 36.4%
Sandersclassification 0.655
2A 5 35.7% 3 27.3%
2B 1 7.1% 1 9.1%
3AB 2 14.3% 4 36.4%
3AC 3 21.4% 0 0%
3BC 1 7.1% 1 9.1%
4 2 14.3% 2 18.2%
CP,calcanealplates;FP,flatplates.
Table3–Resultsofthegroupsinrelationtothewaitingtimeforsurgeryandmeasurementsofthephysicalexamination.
Typeofplate p
CP(n=14) FP(n=11)
Mean SD Mean SD
Waitingtimeuntilsurgery(days) 23.1 17.28 19.5 6.67 0.913a
Differenceincalfdiameter 1.9 0.53 1.5 1.35 0.308a
Widthofthehindfoot 6.7 0.71 7.1 0.82 0.270b
Ankleextension 11.5 10.41 11.8 7.17 0.67.6a
Ankleflexion 24.6 9.90 27.2 9.87 0.519b
Forefootsupination 13 12.88 20.7 11.19 0.084a
Forefootpronation 13.4 9.81 11.1 9.97 0.359a
Subtalarsupination 7.6 6.12 4 7.75 0.057a
Subtalarpronation 1 6.6 0.1 1.58 0.240a
Datapresentedasmeanandstandarddeviation(SD).CP,calcanealplates;FP,flatplates.
a p-valueforMann–Whitneytest. b p-valueforindependentsamplet-test.
Table4–Resultsassessedbytheclinicalassessmentscales.
Typeofplate p
CP(n=14) FP(n=11)
Mean SD Mean SD
PF-SF36ScaleScores 52.9 36.15 52.3 28.84 0.912a
RP-SF36ScaleScores 25.0 39.22 25.0 35.36 0.804a
BP-SF36ScaleScores 47.0 34.90 54.3 27.67 0.578b
GH-SF36ScaleScores 74.6 27.77 74.7 25.41 0.889a
VT-SF36ScaleScores 65.7 20.27 71.8 24.52 0.502b
SF-SF36ScaleScores 63.4 36.51 63.9 36.43 0.846a
RE-SF36ScaleScores 38.1 43.8 36.4 43.35 0.907a
MH-SF36ScaleScores 69.1 20.12 68.7 25.85 0.964b
PF-SF36Norm-basedScaleScores 37.4 15.15 37.1 12.10 0.967b
RP-SF36Norm-basedScaleScores 35.1 11.7 35.0 9.98 0.804a
BP-SF36Norm-basedScaleScores 40.0 14.94 43.2 11.85 0.575b
GH-SF36Norm-basedScaleScores 52.1 13.1 52.2 11.89 0.889a
VT-SF36Norm-basedScaleScores 54.1 9.61 57.0 11.62 0.502b
SF-SF36Norm-basedScaleScores 41.2 15.85 41.3 15.80 0.868a
RE-SF36Norm-basedScaleScores 35.8 13.61 35.2 13.70 0.907a
MH-SF36Norm-basedScaleScores 46.6 11.43 46.3 14.70 0.962b
PCS-SF36 38.1 13.37 39.2 9.47 0.817b
MCS-SF36 47.3 10.9 47.4 13.92 0.975b
Datawerepresentedasmeansandstandarddeviations(SD).CP,calcanealplates;FP,flatplates.
a p-valueforMann–Whitneytest. b p-valueforindependentsamplet-test.
Table5–Resultsaccordingtotheassessmentscales.
Typeofplate pa
CP(n=14) FP(n=11)
Mean SD Mean SD
VAS 4.6 2.73 3.6 2.38 0.344
AOFAS 66.1 26.37 52 20.64 0.160
Radiologicalwidthofthehindfoot 4.7 0.38 4.4 0.60 0.217
Pitchangleofthecalcaneus 21 5.88 16.6 5.66 0.74
Talusdeclinationangle 18 4.79 18.9 2.95 0.587
Datapresentedasmeanandstandarddeviation(SD).CP,calcanealplates;FP,flatplates.
Discussion
Calcanealjointfractures aresevereinjuriesand maycause
permanentanddisablingsequelae.Theyusuallyaffectyoung
andeconomicallyactivemen,andthusthesefracturescan
haveanimportantsocioeconomicimpact.
Inthissample,wefoundthat88%ofpatientsweremale
andhad amean age of47.6 years.Accordingtothe
litera-ture,themostcommoncauseofintra-articularfracturesofthe
calcaneusisafallfromheight,1whichwasconfirmedinthe
presentstudy,asthiscauseaccountedfor96%ofthefractures.
TheEssex-Lopresti10 radiological classificationisa
clas-sical tool that determines the line of fracture and allows
treatment planning. Tomographic classifications help to
assesstheseverityandprognosisoftheinjury;theSanders
classificationisthemostcommonlyused.9 However,
tomo-graphicclassificationsarenotuniformandeachgroupaims
tocreate its own classification,which makesit difficult to
compareresultsaswellastoidentifythetypeofinjurythey
describe.Tomographyisconsideredtobeanexcellenttestto
identifydetails ofthe fragmentsandthe jointimpairment;
however,itisnotavailableinallservices.Thislimitation
jus-tifiestheuseofaradiologicalclassification.
According to the Essex-Lopresti classification,
intra-articular fractures can be tongue-type or joint depression
type.In mostseries, joint depressionis the mostfrequent
type offracture, accounting for 43%–61% ofintra-articular
fractures.11,12Inthepresentstudy,76%offractureswerejoint
depression-typeand24%,tongue-type.
For open surgery,there isa consensustowait between
sevenand 14 daysbetween traumaand operation, sothat
theedemareducesandblisterformationisprevented,except
inopen fractures,whichshouldreceive immediatesurgical
treatment,orwhenpercutaneousfixationisindicated.7,13In
thepresentstudy,themeantimebetweentraumaand
oper-ationofthe25fractureswas23.1days(SD17.28)forCPand
19.5daysforFP(SD6.67).
Thelateral L-shapedaccessroute hasbeenwidelyused
because it allowsbetter visibility ofthe fracture, fragment
reduction,andinternalfixation.7,13Inthisstudy,theextended
lateralL-shapedaccesswasefficient;itwasusedasastandard
techniqueforallcases.
Woundnecrosisisusuallytheresultofimproperincision
and exposureor long surgery.14 Necrosis isobserved more
frequentlyin theend ofthe lateral L-shapedincision.15 In
thepresentstudy,apatienttreatedwithCPneededsurgical
debridementduetoskinnecrosis,whichsolvedtheproblem
withouttheneedofaskingraft.
Symptomsassociatedwithimplantsproblems,whichare
rarelyreportedintheliterature,includeprominentimplant,
skinirritation,andheelpain.Problemsusuallyarisebecause
plate and screws cause irritation to the skin, tendons, or
nerves,orbecauseascrewpenetratesthefacetjoint.16,17
Ten-doninvolvementduetoimplantscanresultintendinitisor
rupture,andleadtotendinitisandsecondarypain.18Inthe
presentstudy,theCPhadtoberemovedinonepatientdueto
skinirritationandpain.Furthermore,inthreepatientswho
weretreatedwithFP,thesynthesismaterialhadtoberemoved
duetoFPandscrewprominence.
Theuseofbonegraftiscontroversial;someauthors
con-siderittobeosteoinductiveandosteoconductive,whileothers
consider itunnecessary.7,19 Itisnoteworthythattheuseof
bonegraft increasestheincidenceofmorbidity,asanother
incision ismade forgraft harvesting.In thepresent study,
bonegraftsfromtheiliacbonewerenotused.Instead,agraft
takenfromthelateralwallofthecalcaneuswasusedtofill
theremainingbonelossafterfracturereduction.
Assessing the resultsusing the AOFAS scale,the
litera-turepresentsratesofexcellentresults,rangingfrom42.22%
to62%.20–22 Inthisstudy,47.6%oftheresultswere
consid-eredgoodorexcellent.Itisnotpossibletostatewithcertainty
thatthetypeoffracturemayhaveinfluencedthescore,asin
thepresentsample,thenumberoftongue-typefractureswas
smallwhencomparedwithjointdepression.
Post-traumaticarthrosisusuallyoccursinthesubtalarand
calcaneocuboidjoints.23 Theliteraturereportsanincidence
rate of1.2%instudies withlong term follow-up.6,16 When
intractablepaincannotbecontrolledbyanalgesics,subtalar
arthrodesismaybethebestoption.16Inthepresentstudy,one
patienttreatedwithFP,withafractureclassifiedasSanders4,
presentedintractablepainandunderwentsubtalar
arthrode-sis,whichimprovedthesymptoms.
Therearemanycontroversiesregardingthetypeofimplant
anditsselectioncriteria.ForORIF,moststudiesappliedaplate
tothelateralwallofthecalcaneus.24Regardingstabilization
screwsforthesustentaculumtali,therearealsocontroversies
regardingwhethertheyshouldbefixatedthroughtheplate.
PlatesinseveralshapescanbeusedforORIFofcalcaneal
frac-tures,anddifferenttypesofsyntheticmaterialsareadvocated
bydifferentauthors.24–30
Modernplateshavealowerprofile,whichhassolved
prob-lems related to excessive skin tension, prominence of the
implantundertheskin,andsubsequentdehiscenceofthe
sur-gicalwound.24Thechoiceforalateralplatedependsonthe
severityofthecalcanealfractureand onbonequality.
Sim-plefracturesingoodqualityboneappeartobeadequatefor
FPfixation,whilecomplexfractureswithcomminutionmay
requireCPorevenlockingplates.24
FPhasbeenusedformanyyears.Intheearly1990s,due
topost-operativecomplicationsatthetime,ORIFtechniques
usingtwoFPsforfixationweredeveloped.Then,the
develop-mentofsingle,H-andY-shapedplatesstarted.30
The literaturefeatures numerousarticles on the use of
lockedplatewithminimallyinvasivetechnique.Fewstudies,
however,addresstheuseofFPforthetreatmentofcalcaneal
fractures,which,fortheBraziliansurgeon,isstillareality,due
tothecountry’shealthcaresystem.
Althoughthiswasaretrospectivestudy,ithelpedtoassess
theoutcomeofpatients.Itcanbeconcludedthattheresults
were very similar to those reported in the literature. The
present studyalsoindicatesthe needtodeveloptreatment
protocolsthatallowprospectivestudies,whichcouldprovide
morereliableinformationonfractures,bothpre-operatively
andduringtheirevolution.
AnotherimportantfactoristhatCPisnotalwaysavailable,
especiallyinpublicservicesthatfacefinancialdifficulties.In
turn,FPismorereadilyavailableandinexpensive.These
fac-tors impact surgicaltreatment. The unavailabilityofCP in
ofFP,mayhavebeenconfoundingfactorinthepresentstudy.
However,thisstudydemonstratedthatthereappearstobeno
significantimpairmentinthetreatmentofcalcanealfractures
whenCPisnotavailable.
Conclusion
Statistical inference allowsfor the conclusion that, in the
absenceofCP,FPcanbeusedwithsimilarclinicaloutcomes.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. MitchellMJ,McKinleyJC,RobinsonCM.Theepidemiologyof
calcanealfractures.Foot(Edinb).2009;19(4):197–200.
2. GriffinD,ParsonsN,ShawE,KulikovY,HutchinsonC,
ThorogoodM,etal.Operativeversusnon-operativetreatment
forclosed,displaced,intra-articularfracturesofthe
calcaneus:randomisedcontrolledtrial.BMJ.2014;349:g4483.
3. ZhangT,SuY,ChenW,ZhangQ,WuZ,ZhangY.Displaced
intra-articularcalcanealfracturestreatedinaminimally
invasivefashion:longitudinalapproachversussinustarsi
approach.JBoneJointSurgAm.2014;96(4):302–9.
4. LimEV,LeungJP.Complicationsofintraarticularcalcaneal
fractures.ClinOrthopRelatRes.2001;391:7–16.
5. WileyWB,NorbergJD,KlonkCJ,AlexanderIJ.Smileincision:
anapproachforopenreductionandinternalfixationof
calcanealfractures.FootAnkleInt.2005;26(8):590–2.
6. YuX,PangQJ,ChenL,YangCC,ChenXJ.Postoperative
complicationsafterclosedcalcaneusfracturetreatedbyopen
reductionandinternalfixation:areview.JIntMedRes.
2014;42(1):17–25.
7. SandersR.Currentconseptsreview–displacedintra-articular
fracturesofthecalcaneus.JBoneJointSurgAm.
2000;82(2):225–50.
8. SooHooNF,VyasR,SamimiD.Responsivenessofthefoot
functionindex,AOFASclinicalratingsystems,andSF-36after
footandanklesurgery.FootAnkleInt.2006;27(11):930–4.
9. SandersR.RadiologicalevaluationandCTclassificationof
calcanealfractures.In:JahssM,editor.Disordersofthefoot
andankle.3rded.Philadelphia:WBSaunders;1990.p.
2326–54.
10.Essex-LoprestiP.Themechanism,reductiontechnique,and
resultsinfracturesoftheoscalcis.BrJSurg.
1952;39(157):395–419.
11.ChhabraN,ShermanSC,SzatkowskiJP.Tongue-type
calcaneusfractures:athreattoskin.AmJEmergMed.
2013;31(7):1151.e3–4.
12.deVroomeSW,vanderLindenFM.Cohortstudyonthe
percutaneoustreatmentofdisplacedintra-articularfractures
ofthecalcaneus.FootAnkleInt.2014;35(2):156–62.
13.WuK,WangC,WangQ,LiH.Regressionanalysisof
controllablefactorsofsurgicalincisioncomplicationsin
closedcalcanealfractures.JResMedSci.2014;19(6):495–501.
14.MelcherG,DegondaF,LeuteneggerA,RuediT.Ten-year
follow-upafteroperativetreatmentforintra-articular
fracturesofthecalcaneus.JTrauma.1995;38(5):713–6.
15.ZwippH,RammeltS,BarthelS.Calcanealfractures–open
reductionandinternalfixation(ORIF).Injury.2004;35Suppl.
2:SB46–54.
16.HuangPJ,HuangHT,ChenTB,ChenJC,LinYK,ChengYM,
etal.Openreductionandinternalfixationofdisplaced
intra-articularfracturesofthecalcaneus.JTrauma.
2002;52(5):946–50.
17.BuckleyR,ToughS,McCormackR,PateG,LeightonR,Petrie
D,etal.Operativecomparedwithnonoperativetreatmentof
displacedintra-articularcalcanealfractures:aprospective,
randomized,controlledmulticentertrial.JBoneJointSurg
Am.2002;84(10):1733–44.
18.WaldeTA,SauerB,DegreifJ,WaldeHJ.Closedreductionand
percutaneousKirschnerwirefixationforthetreatmentof
dislocatedcalcanealfractures:surgicaltechnique,
complications,clinicalandradiologicalresultsafter2–10
years.ArchOrthopTraumaSurg.2008;128(6):585–91.
19.SinghAK,VinayK.Surgicaltreatmentofdisplaced
intra-articularcalcanealfractures:isbonegraftingnecessary?
JOrthopTraumatol.2013;14(4):299–305.
20.GwakHC,KimJG,KimJH,RohSM.Intraoperative
three-dimensionalimagingincalcanealfracturetreatment.
ClinOrthopSurg.2015;7(4):483–9.
21.SchepersT,BackesM,SchepNW,CarelGoslingsJ,LuitseJS.
Functionaloutcomefollowingalockedfracture-dislocationof
thecalcaneus.IntOrthop.2013;37(9):1833–8.
22.RammeltS,ZwippH,SchneidersW,DurrC.Severityofinjury
predictssubsequentfunctioninsurgicallytreateddisplaced
intraarticularcalcanealfractures.ClinOrthopRelatRes.
2013;471(9):2885–98.
23.GallinoRM,GrayAC,BuckleyRE.Theoutcomeofdisplaced
intra-articularcalcanealfracturesthatinvolvethe
calcaneocuboidjoint.Injury.2009;40(2):146–9.
24.DhillonMS,BaliK,PrabhakarS.Controversiesincalcaneus
fracturemanagement:asystematicreviewoftheliterature.
MusculoskeletSurg.2011;95(3):171–81.
25.BenirschkeSK,SangeorzanBJ.Extensiveintraarticular
fracturesofthefoot.Surgicalmanagementofcalcaneal
fractures.ClinOrthopRelatRes.1993;292:128–34.
26.IllertT,RammeltS,DrewesT,GrassR,ZwippH.Stabilityof
lockingandnon-lockingplatesinanosteoporoticcalcaneal
fracturemodel.FootAnkleInt.2011;32(3):307–13.
27.RakV,IraD,MasekM.Operativetreatmentofintra-articular
calcanealfractureswithcalcanealplatesandits
complications.IndianJOrthop.2009;43(3):271–80.
28.GeelCW,FlemisterASJ.Standardizedtreatmentof
intraarticularcalcanealfracturesusinganobliquelateral
incisionandnobonegraft.JTrauma.2001;50:1083–9.
29.RammeltS,BarthelS,BiewenerA,GavlikJM,ZwippH.
Calcaneusfractures.Openreductionandinternalfixation.
ZentralblChir.2003;128(6):517–28.
30.DhillonMS.Fracturesofthecalcaneus.London:Jaypee