w w w . r b o . o r g . b r
Original
Article
Evaluation
of
spinopelvic
balance
among
patients
undergoing
surgical
treatment
for
lumbar
disk
hernia
夽
Rafael
de
Paiva
Oliveira
a,
Vinícius
Gonc¸alves
Coimbra
a,
Yuri
Lubiana
Chisté
b,
José
Lucas
Batista
Junior
c,
Charbel
Jacob
Junior
c,
Igor
Machado
Cardoso
c,
Rodrigo
Rezende
c,∗aHigherSchoolofHealthSciences,SantaCasadeMisericórdiadeVitória,Vitória,ES,Brazil bUniversidadeFederaldoEspíritoSanto,Vitória,ES,Brazil
cHospitalSantaCasadeMisericórdiadeVitória,Vitória,ES,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received22April2013 Accepted19June2013 Availableonline13April2014
Keywords:
Intervertebraldiskdisplacement Spine
Intervertebraldisk
a
b
s
t
r
a
c
t
Objective:toevaluatespinopelvicbalanceusingthepelvicincidence,sacralslopeandpelvic tiltamongpatientswithlumbardiskherniaswhounderwentsurgicaltreatment.
Methods:thirtypatientsatthespinalservicesofHospitalSantaCasadeMisericórdiade VitóriaandHospitalVilaVelhawereevaluatedbymeasuringtheirspinopelvicbalancefrom theanglesofpelvictilt,sacralslopeandpelvicincidence,withtheirrespectivemeans,on simplelateral-viewlumbopelvicradiographsthatneededtoencompassthelumbarspine, sacrumandproximalthirdofthefemur.
Results:thespinopelvicbalancemeasurementsobtainedfromthemeananglesofthe pop-ulationstudied,forpelvicincidence,sacralslopeandpelvictilt,were45◦,36.9◦and8.1◦, respectively.Theconfidenceintervalforthemeanpelvicincidencewasfrom41.9to48.1 (95%CI),thusincludingareferencevaluethatcharacterizeditaslow,foranasymptomatic population,thusconfirmingthatthesamplewasextractedfromapopulationwiththis characteristic.
Conclusion: amongthesepatientswithlumbardiskherniaswhounderwentsurgical treat-ment,theaveragespinopelvicbalancewasfoundtohavepelvicincidencelowerthanwhat hasbeenreportedintheliteratureforanasymptomaticpopulation.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
夽Pleasecitethisarticleas:OliveiraRdP,Gonc¸alvesCoimbraV,LubianaChistéY,LucasBatistaJuniorJ,JacobJuniorC,MachadoCardoso
I,etal.Avaliac¸ãodoequilíbrioespinopélvicoempacientessubmetidosatratamentocirúrgicodehérniadediscolombar.RevBrasOrtop. 2014;49:189–193.
夽夽
WorkperformedattheVertebralColumnService,HospitalSantaCasadeMisericórdiadeVitória,Vitória,ES,Brazil. ∗ Correspondingauthor.
E-mail:[email protected](R.Rezende).
Avaliac¸ão
do
equilíbrio
espinopélvico
em
pacientes
submetidos
a
tratamento
cirúrgico
de
hérnia
de
disco
lombar
Palavras-chave:
Deslocamentododisco intervertebral
Colunavertebral Discointervertebral
r
e
s
u
m
o
Objetivo:avaliaroequilíbrioespinopélvico,pormeiodaincidênciapélvica,dodeclivesacral edaversãopélvica,empacientesportadoresdehérniasdiscaislombaressubmetidosa tratamentocirúrgico.
Métodos: foramavaliados30pacientesdoServic¸odeColunaVertebraldoHospitalSanta CasadeMisericórdiadeVitóriaedoVilaVelhaHospital,pormeiodaaferic¸ãodoequilíbrio espinopélvico,obtidopelamensurac¸ãodosângulosdaversãopélvica,dodeclivesacraleda incidênciapélvica,comsuasrespectivasmédias,nasradiografiassimpleslombopélvicas, tipoperfil,queenglobaram,obrigatoriamente,colunalombar,sacroeterc¸oproximaldo fêmur.
Resultados: a medida do equilíbrio espinopélvico, obtida pela média dos ângulos na populac¸ãoestudadadaincidênciapélvica,dodeclivesacraledaversãopélvica,foide45◦, 36,9◦e8,1◦,respectivamente.Ointervalodeconfianc¸adamédiadaincidênciapélvicaentre 41,9-48,1(95%IC)contémovalordereferênciaqueacaracterizacomobaixa,parauma populac¸ãoassintomática,oqueconfirmaqueaamostrafoiextraídadeumapopulac¸ãocom essacaracterística.
Conclusão:nospacientesportadoresdehérniadiscallombarsubmetidosatratamento cirúr-gicofoiencontrado,emmédia,umequilíbrioespinopélvicocomincidênciapélvicaabaixo doencontradonaliteraturaparaumapopulac¸ãoassintomática.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Disk hernias are defined as a continuous process of disk degenerationthatcausesmigrationofthenucleuspulposus beyond the physiological limits of the fibrous ring.1 Lum-bar hernias occur most frequently and mainly affect men inthe age groupfrom 30 to50 years,in thesegments L4-L5andL5-S1.Becauseoftheepidemiologicalimportanceof thisdisease,itisconsideredtobeaworldwidehealth prob-lem,giventhephysicalandfunctionalincapacitythatitmay cause.1–4
Theetiologyofdiskherniasismultifactorial,through asso-ciationsofdegenerativediskalterationsthatcausedecreases inproteoglycancontentinthenucleuspulposus,insituations inwhichthereisanincreaseindiskpressure,especiallydue torotationandflexionofthespine.Despitethisknowledge ofthemultifactorialnatureofdiskhernias,betterdefinition oftheiretiologicaloriginhasbeensoughtbecause,through this,measurescanbetaken withtheaimofpreventingor diminishing the consequent disorders that this condition creates.1,2
Over recent years, the spinopelvic balance between osteoarticularandneuromyofascialelementsofthestructure ofthespine,pelvisandlowerlimbshasgainedprominence withregardtothegenesisofvariouspathologicalconditions ofthe spine.An associationbetween diskhernias and the spinopelvicsystemhasbeenobserved.5–18
Throughthisgreaterknowledgeofthespinopelvicbalance, wehaveattemptedtoevaluateandusethepelvicincidence, sacralslopeandpelvictiltandtheircorrelationwithpatients presentinglumbardiskherniasinordertoidentifypatients withatendencytodevelopthiscondition.Inthismanner,we
aimedtorefinestrategiesforpreventionandadequate prog-nosisforthispopulation.
Materials
and
methods
This was a retrospective study that was approved by the Research Ethics Committee under the number 04993212.3. 0000.5065. Inthis study,30patients attended atthe Spinal ServiceofHospitalSantaCasadeMisericórdiadeVitóriaand VilaVelhaHospitalwereevaluated(21men;agerange:18–62 years).
The inclusion criteria were that the patients needed to presentalumbardiskherniawithanindicationforsurgery, andneededtohaveundergoneaminimumof20 physiother-apysessions withoutimprovement,but withoutpresenting anycriteriaofinstabilityondynamicradiographs.
Patients were excluded from the study if they did not present an indication for surgical treatment using the microdiscectomy technique, and also if they achieved improvementthroughphysiotherapyorwerefoundtopresent criteriaofinstabilityonpreoperativeradiographsofthe lum-barspine.
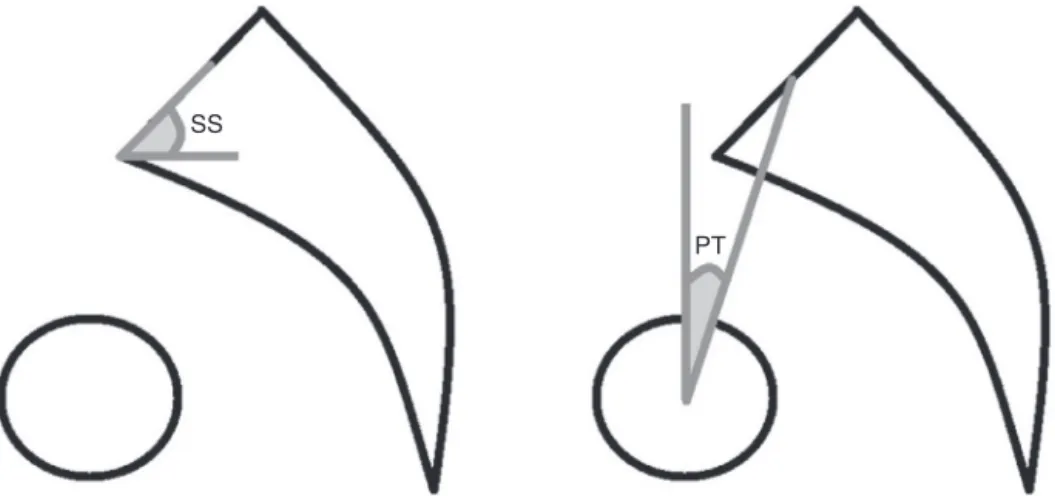
Thespinopelvicbalancewasmeasured usingtheangles of pelvic incidence, sacral slope and pelvic tilt on simple lumbopelvic radiographs inlateralview.These radiographs neededtoencompassthelumbarspine,sacrumandproximal thirdofthefemur.
PI
Fig.1–Illustrationofpelvicincidence(PI).
thetwocentersofthefemoralheads,whichisknownasthe bicoxofemoralaxis(Fig.1).
Thesacralslopeconsistsoftheintersectionbetweena hor-izontallinethatfollowsthegroundandalinethatfollowsthe sacralplateau.Thepelvictiltconsistsoftheintersectionof averticalline,perpendiculartotheground,withaline join-ingthebicoxofemoralaxistothecenterofthesacralplateau (Fig.2).Itisknownthatthesumoftheanglesofthepelvictilt andsacralslopeequalsthevalueofthepelvicincidence.
Thefrequencieswereanalyzedwith95%confidence inter-vals (95% CI; Taylor series). The results were represented numericallybymeansofabsolutevalues,andsomedatawere alsoexpressedaspercentages.TheKolmogorov–Smirnovtest was appliedinorder to ascertainwhether the distribution ofprobabilitiesofthedatawasnormal:thishypothesiswas accepted.Student’sttestwasappliedtomakecomparisons betweenthe meansofthe variables.Thedataanalysiswas doneusingtheMicrosoftOffice/Excel2007software.
Results
Thirtypatientswere evaluated.Therewere 21menofages ranging from 18 to 58 years (mean of 40 years) and nine
women of ages ranging from 18 to 62 years (mean of 33 years).
The spinopelvic balance was measured from the pelvic incidence,sacralslopeandpelvictilt,andthemeanvalues foundwere45◦,36.9◦ and8.1◦,respectively.Thedistribution
oftheparametersobservedcanbeseeninFig.3.
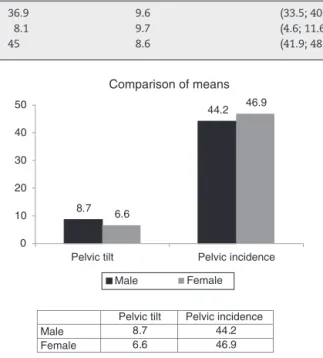
FromStudent’sttest,therewasnosignificantdifferencein themeansfortheparametersstudiedbetweenindividualsof differentsexes,asshowninFig.4.Thedescriptivelevelswere
p=0.206,p=0.622andp=0.411fortheparametersofthesacral slope,pelvictiltandpelvicincidence.
Fromspecificanalysisonthepelvicincidence,weobserved thatitsmeanvalueinourstudywas45◦anditpresenteda
confidenceintervalfrom41.9◦ to48.1◦(minimumand
maxi-mumvalues,respectively).Themeanvaluesforslopeandtilt were36.9◦and8.1◦,withaconfidenceintervalasdescribedin
Table1.5,7,8,10,12,13,17
Discussion
Several studies onspinopelvic balance and diseases ofthe spine have been developed with the aim of better under-standing whatits relationshipwiththe humanbody is.Its importanceissuchthatRoussoulyetal.,9in2003,classified lumbarlordosisintofourmorphologicalpatterns,takingthe angleofthesacralslopeasthereference.6,9,11–13,15
Themainradiologicalparametersusedforevaluatingthe spinopelvic balance are the pelvic incidence, sacral slope, pelvictiltandlumbarlordosis.Thefirstoftheseisan individ-ualanatomicalconstantandtheothersarevariable,according tothepostureadopted.Thepelvicincidence,whichwas stud-iedbyLegayeetal.7in1998,wastheresultfromsummingthe anglesofsacralslopeandpelvictilt.Thepelvicincidencewas afundamentalangleforcomprehendingthisbalance.6–15
Inourstudy,wesoughttoidentifywhatthe pelvic inci-dence,sacralslopeandpelvictiltvalueswere,inpatientswith lumbardiskherniaswhounderwentsimplemicrodiscectomy. Wetooktheviewthatbetterunderstandingofthespinopelvic balanceinthesepatientsmightinfluencethetypeofsurgery andpreventiveactionsrelatingtodiskhernias.
The mean pelvicincidence in the asymptomatic popu-lation ranges from 52◦ to 55◦, according to the references
SS
PT
Table1–Statisticsontheparametersobserved.
Minimum Maximum Mean Standarddeviation 95.0%CI
Sacralslope 16 55 36.9 9.6 (33.5;40.3)
Pelvictilt −9 30 8.1 9.7 (4.6;11.6)
Pelvicincidence 29 71 45 8.6 (41.9;48.1)
Sex Sacral slope Pelvic tilt Pelvic incidence
Male 35 21 56
Male 36 13 49
Male 44 5 49
Male 45 −3 42
Male 16 20 36
Male 20 23 43
Male 29 13 42
Male 44 3 47
Male 49 −1 48
Male 25 19 44
Male 33 3 36
Male 41 7 48
Male 37 7 44
Male 50 4 54
Male 41 0 41
−20 −10 0 10 20 30 40 50 60 70 80 29 27 25 23 21 19 17 15 13 11 9 7 5 3 1
Sacral slope Pelvic tilt Pelvic incidence
Male 19 10 29
Male 37 −3 34
Male 30 8 38
Male 31 4 35
Male 42 0 42
Male 41 30 71
Female 41 16 57
Female 35 7 42
Female 33 3 36
Female 23 29 52
Female 55 −9 46
Female 44 −1 43
Female 46 13 59
Female 44 0 44
Female 42 1 43
Fig.3–Distributionoftheparametersobserved.
that we analyzed. In ourstudy, the mean valuefor pelvic incidenceamongourpatientswas45◦.Inanalyzingthe
con-fidenceinterval,weobservedthat therewas avariationof ±3.1◦ (95%CI:41.9–48.1),whichsuggests thatpatientswith
lumbardiskhernias who donotpresentany improvement throughphysiotherapyand needsurgicaltreatmenthave a
Pelvic tilt
Pelvic incidence
Male 8.7
44.2
Female 6.6
46.9
8.7 44.2 6.6 46.9 0 10 20 30 40 50
Pelvic tilt Pelvic incidence
Comparison of means
Male
Female
Fig.4–Comparisonofthemeansfortheparameters betweenthesexes.
pelvic incidence lower than what is found in the asymp-tomaticpopulation.5,7,8,10,12,13,17
Thepelvicincidenceisaconstantanglethatis geomet-ricallyequivalent tothe sumoftheangularmeasurements ofthepelvictiltandsacralslope,whichcanvaryaccording tothepatient’spositioning.Inanalyzingthemeanvaluesfor theslopeandtiltfrom ourstudyinrelationtothoseinthe literature, weobservedthat there were largediscrepancies inthemeasurements, whichwerenotuniformbetweenall thestudiesanalyzed.Thiscanpossiblybeexplainedbythe methodologyusedineachstudyforpositioningthepatientat thetimeoftheradiologicalexamination.5,7,10,12
Conclusion
Patientswithlumbardiskherniaspresentspinopelvic equi-librium with low pelvic incidence, compared with the asymptomatic population. These patientsseem tohavean additionalriskfactorthatinfluencestheetiologyoflumbar diskhernias,becauseofgreaterpressureoccurringatthelevel oftheintervertebraldisk,especiallyinthesegmentsL4-L5and L5-S1.
We consider that further studies on the correlation betweenspinopelvicbalanceandlumbardiskherniasare nec-essary.Webelievethatthisparametershouldbefullyanalyzed beforepatientswithdiskherniasaretreated.
Conflicts
of
interest
r
e
f
e
r
e
n
c
e
s
1. VialleLR,VialleEM,HenaoJE,GiraldoG.Hérniadiscallombar. RevBrasOrtop.2010;45(1):17–22.
2. BarrosFilhoTE,BasileJúniorR,CristanteAF,AraújoMP. Colunatoracolombar:síndromesdolorosas.In:HebertS, BarrosFilhoTE,XavierR,PardiniJúniorAG,editors.Ortopedia etraumatologia:princípioseprática.4thed.PortoAlegre: Artmed;2009.p.122–35.
3. DeyoRA,LoeserJD,BigosSJ.Herniatedlumbarintervertebral disk.AnnInternMed.1990;112(8):598–603.
4. StienenMN,CadoschD,HildebrandtG,GautschiOP.The lumbardischerniation–management,clinicalaspects,and currentrecommendations.Praxis(Bern1994).
2011;100(24):1475–85.
5. BarreyC,RoussoulyP,PerrinG,LeHuecJC.Sagittalbalance disordersinseveredegenerativespine.Canweidentifythe compensatorymechanisms?EurSpineJ.2011;20Suppl. 5:626–33.
6. LeHuecJC,RoussoulyP.Sagittalspino-pelvicbalanceisa crucialanalysisfornormalanddegenerativespine.EurSpine J.2011;20Suppl.5:556–7.
7. LegayeJ,Duval-BeaupèreG,HecquetJ,MartyC.Pelvic incidence:afundamentalpelvicparameterfor
three-dimensionalregulationofspinalsagittalcurves.Eur SpineJ.1998;7(2):99–103.
8. GuiguiP,LevassorN,RillardonL,WodeckiP,CardinneL. Physiologicalvalueofpelvicandspinalparametersofsagittal balance:analysisof250healthyvolunteers.RevChirOrthop ReparatriceApparMot.2003;89(6):496–506.
9. RoussoulyP,Pinheiro-FrancoJL.Biomechanicalanalysisof thespino-pelvicorganizationandadaptationinpathology. EurSpineJ.2011;20Suppl.5:609–18.
10.LegayeJ,HecquetJ,MartyC,Duval-BeaupèreG.Equilibre sagittaldurachis:relationsentrebassinetcourbures rachidiennessagittalesenpositiondebout.Rachis. 1993;5(5):215–26.
11.LabelleH,RoussoulyP,BerthonnaudE,DimnetJ,O’BrienM. Theimportanceofspino-pelvicbalanceinL5-s1
developmentalspondylolisthesis:areviewofpertinent radiologicmeasurements.Spine(Philadelphia,PA,1976). 2005;30Suppl.6:S27–34.
12.LeeCS,ChungSS,ChungKH,KimSR.Significanceofpelvic incidenceinthedevelopmentofabnormalsagittalalignment. JKoreanOrthopAssoc.2006;41(2):274–80.
13.RajnicsP,TemplierA,SkalliW,LavasteF,IllesT.The importanceofspinopelvicparametersinpatientswith lumbardisclesions.IntOrthop.2002;26(2):104–8.
14.MangioneP,SénégasJ.Sagittalbalanceofthespine.RevChir OrthopReparatriceApparMot.1997;83(1):22–32.
15.RoussoulyP,BerthonnaudE,DimnetJ.Geometricaland mechanicalanalysisoflumbarlordosisinanasymptomatic population:proposedclassification.RevChirOrthop ReparatriceApparMot.2003;89(7):632–9.
16.PelletN,AunobleS,MeyratR,RigalJ,LeHuecJC.Sagittal balanceparametersinfluenceindicationsforlumbardisc arthroplastyorALIF.EurSpineJ.2011;20Suppl.5: 647–62.
17.BarreyC,JundJ,NosedaO,RoussoulyP.Sagittalbalanceofthe pelvis–spinecomplexandlumbardegenerativediseases.A comparativestudyabout85cases.EurSpineJ.
2007;16(9):1459–67.