w w w . r b o . o r g . b r
Original
article
What
is
the
real
angle
of
deviation
of
metacarpal
neck
fractures
on
oblique
views?
A
radiographic
study
夽
Arthur
de
Góes
Ribeiro
a,∗,
Daniel
Hidalgo
Gonc¸alez
a,
João
Manoel
Fonseca
Filho
a,
Guilherme
Marques
da
Fonseca
a,
Antonio
Carlos
Costa
a,b,
Ivan
Chakkour
aaDepartmentofOrthopedicsandTraumatology,FaculdadedeCiênciasMédicasdaSantaCasadeSãoPaulo,SãoPaulo,SP,Brazil
bDepartmentofOrthopedicsandTraumatology,FaculdadedeMedicinadoABC,SantoAndré,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received29April2015 Accepted1June2015
Availableonline27February2016
Keywords: Fractures,bone Hand
Metacarpus Radiography
a
b
s
t
r
a
c
t
Objective:Theaimofthisstudywastoestablishanindirect,easy-to-use,predictableand safemeansofobtainingthetruedegreeofdisplacementoffracturesoftheneckofthefifth metacarpalbone,throughobliqueradiographicviews.
Methods:Ananatomicalspecimenfromthefifthhumanmetacarpalwasdissectedand sub-jectedtoostectomyintheneckregion.A1-mmKirschnerwirewasfixedtothebaseofthe fifthmetacarpalbone,perpendiculartothelongitudinalaxisoftheboneandparalleltothe ground.AnothersixKirschnerwiresofthesamediameterwerebentoverandattachedto theostectomizedbonetosimulatefracturedisplacement.Axialrotationofthemetacarpus wasusedtocreateobliqueradiographicviews.Radiographicimagesweregeneratedwith differentanglesandatseveraldegreesofrotationofthebone.
Results:Wededucedamathematicalformulathatshowedthetruedisplacementoffractures oftheneckofthefifthmetacarpalbonebymeansofobliqueradiographs.
Conclusions:Obliqueradiographsat30◦ofsupinationprovidedthebestviewoftheboneand
leastvariationfromtherealvalueofthedisplacementoffracturesofthefifthmetacarpal bone.Themathematicalformuladeducedwasconcordantwiththeexperimentalmodel used.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
夽
WorkperformedintheDepartmentofOrthopedicsandTraumatology,IrmandadedaSantaCasadeMisericórdiadeSãoPaulo,São Paulo,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](A.deGóesRibeiro).
http://dx.doi.org/10.1016/j.rboe.2016.02.009
Qual
é
o
ângulo
real
do
desvio
da
fratura
do
colo
do
metacarpo
nas
incidências
oblíquas?
Estudo
radiográfico
Palavras-chave: Fraturasósseas Mão
Metacarpo Radiografia
r
e
s
u
m
o
Objetivo:Estabelecerumaformaindireta,fácil,previsíveleseguranaobtenc¸ãodovalorreal dodesviodafraturadocolodoquintometacarpoapartirderadiografiasoblíquas. Métodos: Umapec¸aanatômicadequintometacarpohumanofoidissecadaesubmetidaà ostectomianaregiãodocolo.UmfiodeKirschnerde1mmfoifixadoperpendicularaoeixo longitudinaldoossoeparaleloaosolo.OutrosseisfiosdeKirschnerdomesmodiâmetro foramdobradosepresosaoossoostectomizadoparasimularodesviodasfraturas.Rotac¸ão axialdometacarpofoiusadaparacriarasradiografiasnasincidênciasoblíquas.Imagens radiográficasforamobtidascomdiferentesânguloseemváriosgrausderotac¸ãodoosso. Resultados: Deduzimosumaequac¸ãomatemáticaquedemonstraorealdesviodafratura docolodoquintometacarpopormeioderadiografiasoblíquas.
Conclusões: Aradiografiaoblíquacom30◦desupinac¸ãoapresentamelhorvisualizac¸ãodo
ossoemenorvariac¸ãodovalorrealdodesviodafraturadocolodoquintometacarpo.A fórmulamatemáticadeduzidafoiconcordantecomomodeloexperimentalusado.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Fracturesoftheneckofthefifthmetacarpalresultfromdirect axialorobliquetraumaonthisbone.Theymaybeduetoafall ortoreceivingablow.Thesefracturesoccurfrequentlyinthe generalpopulationandaccountforaround20%ofallfractures ofthehand.1,2
Clinicalevaluationsonpatientswiththesefracturestake intoconsiderationshortening,rotationandangulardeviation duringflexion.2–4
ThereductiontechniquemostusedistheJahssmaneuver, whichimprovesthedegreeofdeviationofthedistalfragment ofthefracture.5
Thedecisiontoimplementsurgicaltreatmentdependson clinicalandradiographicparametersandalsoonthepatient’s age,profession,activitylevelandhandedness.6
It has been recommended in the recent literature that radiographicassessmentsonthesefracturesshouldbe con-ductedusinganteroposterior,lateralandobliqueradiographic views.5
Itisknownthatthebestwayofevaluatingtherealangle ofdeviationofafractureisbymeansofaradiographicview perpendicular to the fracture line.4 However, lateral radio-graphsareoftenlimitedbecauseofsuperpositionoftheother metacarpals,thetechnicalqualityoftheimage,thepresence ofplaster-cast immobilization after the reductionand the printingonphotographicpaper.7,8Tasbasetal.9studiedthe influenceoftheradiographicmethodonthemeasurements obtainedforanalyzingthesefractures.
Theobjectiveofthepresentstudywastoestablishan easy-to-use,predictableandsafeindirectmethodforascertaining therealdegreeofdeviationduringflexioninfracturesofthe neckofthefifthmetacarpal,throughapplicationin oblique-viewradiographs,whichprovideabetterviewofthebonein question.
Material
and
methods
Ananatomicalreviewofthehumanfifthmetacarpalwas con-ductedinordertounderstandthespatialpositioningofthis boneinthehand.
Afterthefifthmetacarpalofthedonorcadaverhadbeen dissectedtoremovesofttissues,itwassubjectedtowedge ostectomyintheneckregion,withavolarbasis.Thisresection wasperformedusinganoscillatingsawguidedbyatransfer systemandenabledsimulationoffractureswithdeviationsof upto90◦.
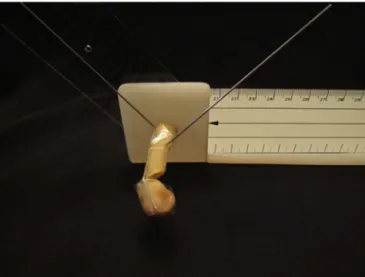
A1mmKirschner wirewasattached tothe baseofthe fifthmetacarpal,perpendiculartothelongitudinalaxisofthe bone and parallel to the ground. Another six wiresof the same diameter,withpredeterminedangularmeasurements that would reproduce the deviation ofthe fracture during flexion,werethenattachedtothedorsalcortexofthebone (Fig.1)andweremaintainedorientedorthogonallytothefirst wire.
Theanglesusedtosimulatefractures were15◦,30◦,45◦, 60◦,75◦and90◦(Fig.2).Theaxialrotationdeterminedbythe wirethatwasparalleltothegroundwasusedtocreateoblique radiographicviewsat0◦,15◦,30◦,45◦,60◦,75◦and90◦(Fig.1), whichwereestablishedwiththeaidofagoniometer.
Thebonewasfixedusinga2mmmetalscrewinaplastic supportequippedwithagoniometer(Fig.1).
Table1–Angleoffracture,measuredfromobliqueradiographicview.
Angleoffracture Rotationofmetacarpal
0(L) 15◦ 30◦ 45◦ 60◦ 75◦ 90◦(AP)
16◦ 16 15 15 12 9 5 0
29◦ 29 28 27 23 19 11 0
43.6◦ 43.6 43 40 34 25 14 0
58◦ 58 58 54 49 39 25 0
74◦ 74 73 71 64 57 38 0
89◦ 89 88 87 84 80 69 0
L,lateralview;AP,anteroposteriorview.
Fig.1–Devicesetupwithgoniometer,withthefifth metacarpalattachedtoaplasticsupport.Two1-mmK wireswerefixedtothebone:oneofthemperpendicularto thelongitudinalaxisoftheboneandtheother
perpendiculartothefirstwireinordertosimulatethe angulardeviationofthefragment.
Theanglesmeasured onthe radiographswere assessed usingtheAutoCAD®software(Fig.3).Thevaluesobtainedare presentedinTable1andFig.4.
WeaskedtheDepartmentsofEngineeringoftheMackenzie HigherEducationSchool(SãoPaulo,Brazil)andtheUniversity ofPorto(Portugal)toresearchaformulathatwouldrepresent themathematicalfunctionoftherealdeviationofthefracture, from thedeviationsfoundon oblique radiographs,without havingaccesstothepracticalresults.
Anewtableandgraphwere drawnup usingthe values foundthroughapplyingthe mathematicalformula(Table2
andFig.5).
Thetables and Figs. 4 and 5 were compared using the MicrosoftExcel®software,inordertoascertainthedegreeof similarity.Thisconfirmedthevalidityoftheformulathathad beenelaborated.
Inordertofacilitatemeasurementoftherealangleof devi-ation,wecreatedatableshowingobliqueincidencevaluesand measuredangles.Fromthis,therealvaluesforfracturescan befoundwithouttheneedtoenterthedataintheformula
(Table3).
Fig.2–One-millimeterKwiresbentat15,30,45,60,75 and90◦.
Athirdmathematicalstudywasconductedtocorrelatethe proportionsbetweentheexperimentalvaluesobtainedfrom the radiographsand the real valueof the fracture studied
(Table4).
Results
ThevaluesobtainedaredescribedinTable1andFig.4. Thetwodepartments ofengineeringproducedthesame formula:
=arctg
tgˇcos˛
Table2–Realangleoffracture,fromtheformulaappliedtotheobliqueradiographicview.
Angleoffracture Rotationofmetacarpal
0(L) 15◦ 30◦ 45◦ 60◦ 75◦ 90◦(AP)
16◦ 16 15 14 11 8 4 0
29◦ 29 28 26 21 15 8 0
43.6◦ 43.6 43 40 34 25 14 0
58◦ 58 57 54 49 39 22 0
74◦ 74 73 72 68 60 42 0
89◦ 89 89 89 89 88 86 0
L,lateralview;AP,anteroposteriorview.
Table3–Realangleoffracture,accordingtotheanglemeasuredfromtheobliqueradiographicview.
Measuredangle (indegrees)
Rotationofthehand(indegrees)
0 5 10 15 20 25 30 35 40 45 50 55 60 65 70 75 80 85 90
5 5 5 5 5 5 6 6 6 7 7 8 9 10 12 14 19 27 45 90
10 10 10 10 10 11 11 12 12 13 14 15 17 19 23 27 34 45 64 90
15 15 15 15 16 16 16 17 18 19 21 23 25 28 32 38 46 57 72 90
20 20 20 20 21 21 22 23 24 25 27 30 32 36 41 47 55 64 77 90
25 25 25 25 26 26 27 28 30 31 33 36 39 43 48 54 61 70 79 90
30 30 30 30 31 32 32 34 35 37 39 42 45 49 54 59 66 73 81 90
35 35 35 35 36 37 38 39 41 42 45 47 51 54 59 64 70 76 83 90
40 40 40 40 41 42 43 44 46 48 50 53 56 59 63 68 73 78 84 90
45 45 45 45 46 47 48 49 51 53 55 57 60 63 67 71 75 80 85 90
50 50 50 50 51 52 53 54 55 57 59 62 64 67 70 74 78 82 86 90
55 55 55 55 56 57 58 59 60 62 64 66 68 71 74 77 80 83 87 90
60 60 60 60 61 62 62 63 65 66 68 70 72 74 76 79 82 84 87 90
65 65 65 65 66 66 67 68 69 70 72 73 75 77 79 81 83 85 88 90
70 70 70 70 71 71 72 73 73 74 76 77 78 80 81 83 85 86 88 90
75 75 75 75 75 76 76 77 78 78 79 80 81 82 84 85 86 87 89 90
80 80 80 80 80 81 81 81 82 82 83 84 84 85 86 87 87 88 89 90
85 85 85 85 85 85 85 86 86 86 86 87 87 87 88 88 89 89 90 90
90 90 90 90 90 90 90 90 90 90 90 90 90 90 90 90 90 90 90 90
Table4–Percentagedifferencebetweenthemeasurementsobtainedfromtheobliqueradiographicviewandthereal anglefromthelateralviewofthedistalfragmentofthefifthmetacarpal.
Angleofdistalfragment Rotationofmetacarpal
0 15◦ 30◦ 45◦ 60◦ 75◦ 90◦(F)
16◦ 100% 94% 94% 75% 56% 31% 0%
29◦ 100% 97% 93% 79% 66% 38% 0%
43◦ 100% 98% 91% 78% 58% 32% 0%
58◦ 100% 100% 93% 84% 67% 43% 0%
74◦ 100% 99% 96% 86% 77% 51% 0%
89◦ 100% 99% 98% 94% 90% 78% 0%
Thevaluesobtainedwhenappliedtotheformula,forthe differentanglesofrotationofthemetacarpal,areshownin
Table2andFig.5.
Tofacilitatededucingtherealangleofflexion,atablewith obliqueincidencevaluesandmeasuredangleswascreated. Fromthis,the realdeviationvalueforthefracturescan be accessedwithouttheneedtousetheformula(Table3).
Toevaluatetherelationshipbetweenthevaluesobtained usingthevariousoblique viewsandthereal values(lateral view)ofthedeviationduringflexion,Table4wascreated.
Discussion
In treating fractures of the neck of the fifth metacarpal, doubtfulcasesinwhichthefracturecannotbeseenwellon radiographicimagesarefaced.Thus,itisimportanttohave options thatprovidereliable information,so thatdecisions madecanbeascorrectaspossible.
Fig.3–Radiographicimageofthedeviceused.
Angle of rotation of the metacarpal (in degrees)
0 15 100 90 80 70 60 50 40 30 20 10 0 90 75 60 45 30
16º 29º 43.6º 58º 74º 89º
(AP) (L)
Measured angle (in degrees)
Fig.4–Variationsoftheanglesmeasured,accordingtothe axialrotationofthemetacarpal.L,lateralview;AP, anteroposteriorview.
Ithasbeenrecommendedintherecentliteraturethat devia-tionoffracturesofthefifthmetacarpalshouldbemeasured bymeansofanangletracedoutbetweenthediaphysisand head,inlateralandobliqueviews.3
Some studies have presented attempts to define radiographic parameters and measurements on the fifth metacarpalthat wouldberoutinely applicable,butwithout greatsuccess.Thiswasprobablyduetothecomplexanatomy ofthisboneandtheacceptanceofanaverageofupto40◦of angulardeviation forindicating conservativetreatment for thesefractures.3,4,7,10
Angle of rotation of the metacarpal (in degrees)
Values found after application of the recently obtained formula (in degrees)
0 15 100 90 80 70 60 50 40 30 20 10 0
30 45 60 75 90
º 9 8 º 4 7 º 8 5 º 9 2 º 6 1 43.6º (AP) (L)
Fig.5–Variationsoftheanglesobtainedafterapplication oftheformulathatwascalculated.L,lateralview;AP, anteroposteriorview.
Because ofthe difficulty in evaluating preoperative and post-reductioncases,aswellasthoseforwhichconservative treatmentisused,aneedtoseekalternativesforquantifying therealangulardeviationbetweenthefracturefragmentsof thisbone,withasgreatadegreeofcertainlyaspossibledespite thelimitations,hasarisen.
However,there are noarticlesin theliteratureon stan-dardizationofangularmeasurementsonobliqueradiographs. Forthisreason,wemademeasurementsatobliqueanglesby meansofaxialrotationofthemetacarpal,instepsof15◦.
In evaluating the radiographs obtained, measurements usingAutoCAD®weremadeonthelinesprojectedfromthe Kirschnerwires.Thebonewasusedasaguideforfixationof thewiresandasameansoffamiliarizationwiththeimages ofthefracture(Fig.6).
Wefirstlynotedthatradiographswitharotationof30◦ pro-videdthebestviewofthebone,withtheleastdistortionof therealangularvalue,incomparisonwiththeotheroblique views(Fig.7).Fromanalysisonradiographswith30◦of supina-tionandpronationofthehand,weobservedthattherewas leastbonesuperpositionattheincidencewith30◦of supina-tion ofthe hand.There wasupto91%agreementbetween therealangularvalueofthefracturesandtheradiographic measurementsattheobliquepositionof30◦(Table4).
Oblique radiography isamethod thatenables measure-ment of the angular deviation that is more trustworthy. However,managementdecisionsaremadebasedonthereal angular deviation of the fracture. Through using the for-mulaproposedhere,therealdeviationofthefracturecanbe inferredfrommeasurementsontheobliqueincidence.
Theresultsfromthisstudyshowthedifferencesbetween anglemeasurementsinthelateralandobliqueviews,forthe samefracture,inthesamewayaspreviouslyreportedinthe literature3,10(Table1).
Fig.6–Anglesmeasuredonobliqueradiographsofthefifthmetacarpal,with45◦ofdeviationofthedistalfragmentduring
flexion.A,lateralview;B,15◦ofaxialrotation;C,30◦ofaxialrotation;D,45◦ofaxialrotation;E,60◦ofaxialrotation;F,75◦
ofaxialrotation.
Fig.7–Radiographsofnormalhand.A,with30◦ofsupination;B,lateralview;C,with30◦ofpronation.
conservative treatment offractures can beaccepted when oblique-viewradiographsat30◦ofsupinationshowanangular deviationvalueofupto35◦,whichrepresentsrealdeviation
of39◦(Table3).
Theeconomicimportanceofthisassessmentmethodcan alsobehighlighted,giventhattheneedforlateralradiographs fortheinitialevaluationofthefracturecanbedismissed. Fur-thermore,thepatientsarelessexposedtoradiation.
Sincethetrigonometricanalysiswasbasedonprojection ofimagesfromKirschnerwires,wecaninferthatthe applica-bilityoftheformulaextendstofracturesofotherlongbones. Weconsiderthatthelimitationsofthisstudywereitsuse ofacommercialgoniometerandthepossibleimprecisionof radiographsandinthemoldingofthemetalwires.Moreover, thisexperimentwas performedwithonlyonebone,which wasnotequivalenttothespecificspatialboneorganization ofahand.Furtherradiographicstudiesareneededinorder
toevaluatetheapplicabilityoftheformulathatwasobtained throughclinicalpractice.
WebelievethatouruseoftheAutoCAD®softwarefor mea-suring the angles increasedthe degree ofcertainty of the measurements.
Conclusion
Therewasaconstantrelationshipbetweentherealdeviation ofthefractureandtheradiographicangleinfracturesofthe metacarpals.Themathematicalformulathatwasderivedwas consistentwiththeexperimentalmodelused.
Conflicts
of
interest
Acknowledgements
ToProfessorsFabioRaiaandHelioPekelmanofthe Depart-ment of Engineering of Mackenzie University (São Paulo, Brazil), Paulo Gomes da Costa, Assistant Professor of the DepartmentofElectricalEngineeringandComputationofthe University of Porto (Porto, Portugal) and Manuel Machado, engineer graduated from the University of Porto (Porto, Portugal).
r
e
f
e
r
e
n
c
e
s
1. BraakmanM.Normalradiographicangulationinthe4thand
5thmetacarpal:areferenceguide.EurJRadiol.
1996;22(1):38–41.
2. MullerMGS,PoolmanRW,vanHoogstratenMJ,StellerEP.
Immediatemobilizationgivesgoodresultsinboxer’s
fractureswithvolarangulationupto70degrees:a
prospectiverandomizedtrialcomparingimmediate
mobilizationwithcastimmobilization.ArchOrthopTrauma
Surg.2003;123(10):534–7.
3.HofmeisterEP,KimJ,ShinAY.Comparisonof2methodsof
immobilizationoffifthmetacarpalneckfractures:a
prospectiverandomizedstudy.JHandSurgAm.
2008;33(8):1362–8.
4.LamraskiG,MonsaertA,DeMaeseneerM,HaentjensP.
Reliabilityandvalidityofplainradiographstoassess
angulationofsmallfingermetacarpalneckfractures:human
cadavericstudy.JOrthopRes.2006;24(1):37–45.
5.KlinefelterEW.Theinfluenceofpositiononthemeasurement
oftheprojectedboneangle.AmJRoentgenol.1946;55:722–5.
6.BraakmanM.ArelateralX-raysusefulinthetreatmentof
fracturesofthefourthandfifthmetacarpals?Injury.
1998;29(1):1–3.
7.OpgrandeJD,WestphalSA.Fracturesofthehand.OrthopClin
NAm.1983;14:779–92.
8.SternPJ.Fracturesofmetacarpalandphalanges.In:Grenen
DP,HotchkissRN,PedersonWC,WolfeSW,editors.Green’s
operativeandsurgery.4thed.NewYork:Churchill
Livingstone;2005.p.277–341.
9.Tas¸bas¸BA,OzakpınarHR,Delialio ˘gluMO,Da ˘glarB,Bayrakcı
K,GünelU.Realangulationdegreeinfifthmetacarpalneck
fracture.EklemHastalıkCerraahis.2011;22(2):85–8.
10.AliA,HammanJ,MassDP.Thebiomechanicaleffectsof
angulatedboxer’sfracture.JHandSurgAm.1999;24(4):