1. Rheumatology Department. Hospital Sierrallana
2. Rheumatology Department. Hospital Universitario Marqués de Valdecilla
3. Radiology Department. Hospital Universitario Marqués de Valdecilla
4. Maxillofacial Surgery Department. Hospital Universitario Marqués de Valdecilla
5. Pathology Department. Hospital Universitario Marqués de Valdecilla
6. Rheumatology Department. Hospital Universitario Marqués de Valdecilla. IDIVAL. University of Cantabria
tremely rare
2, and literature about the optimal
treat-ment is scarce. We present the first case of pediatric
GPA with limited orbital involvement successfully
treat-ed with rituximab (RTX).
CLINICAL CASE
A 15-year-old girl with unremarkable personal and
family history, presented with a one-month history of
non-tender right upper eyelid swelling. Visual acuity
and ocular movements were impaired. Her blood tests
including full blood count and complete chemistry
were normal, and acute phase reactants were between
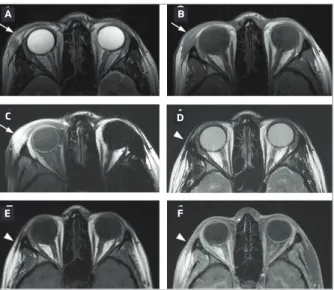
normal limits. Orbital ultrasonography and magnetic
resonance imaging (MRI) confirmed the diffuse mass
within the orbicular musculature in the outer edge of
the right orbit, slightly hyperintense with moderate
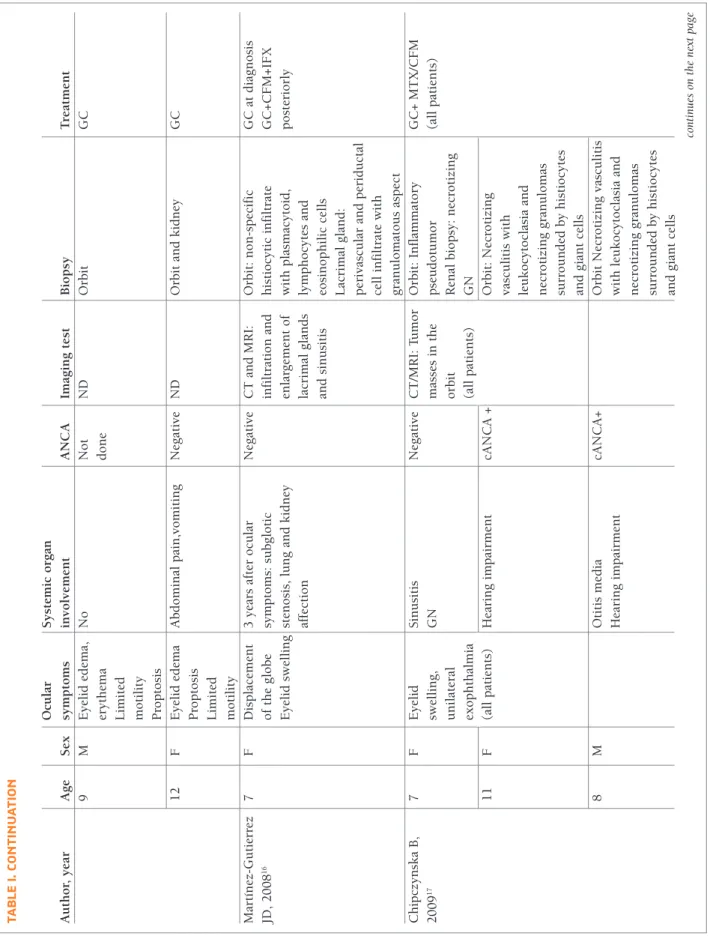
contrast enhancement (Figure 1). A biopsy of the mass
was performed showing lymphocytic infiltration
around and within the wall of medium and small
ves-sels, and necrotizing granulomas (Figure 2). A systemic
evaluation ruled out any other organ affection. ANCA
test was repeatedly negative. With the suspicion of GPA
with isolated orbital involvement, treatment with
pred-nisone (40 mg per day for 3 weeks followed by 5 mg
dose reduction every 10 days until dose of 20 mg per
day, then 2.5 mg dose reduction every week) and
methotrexate (20 mg weekly) was started. After initial
improvement, when tappering prednisone to 15 mg
per day, the upper eyelid swelling recurred. The
clini-cal worsening was confirmed with a new MRI. Then,
treatment with RTX 375 mg/m
2/week for 4 weeks was
started and followed by maintenance therapy
consist-ing of 500 mg every 6 months. The patient presented
a good clinical response, with complete resolution of
the lesion in the radiological control one year after
start-ing RTX.
ACTA REUMATOL PORT. 2019;44:258-263
Granulomatosis with polyangiitis with isolated orbital
involvement in children: a case report successfully
treated with rituximab and review of literature
Riancho-Zarrabeitia L
1, Peiró Callizo E
2, Drake-Pérez M
3, García Montesinos B
4, Terán N
5, Martínez-Taboada VM
6ABSTRACT
We report the case of a 15-year old girl who presented
with a non-tender right upper eyelid swelling.
Magnet-ic resonance confirmed the presence of an enlargement
of the orbicular muscle with moderate contrast
en-hancement. Biopsy revealed the presence of necrotizing
granulomatous vasculitis. Further studies ruled out
sys-temic involvement. Thus, she was diagnosed with
iso-lated granulomatosis with polyangiitis (GPA). Treatment
with steroids and methotrexate was started. Due to the
persistence of the lesion, rituximab (RTX) was added
with excellent clinical and radiological response. This is,
to the best of our knowledge, the first case of isolated
or-bital GPA treated with RTX in a pediatric patient.
Keywords: Pediatric; ANCA-associated vasculitis;
Or-bital inflammatory disease.
INTRODUCTION
Granulomatosis with polyangiitis (GPA) is a small and
medium-sized vessel vasculitis associated with the
pres-ence of anti-neutrophil cytoplasmic antibody (ANCA).
The incidence of GPA in European pediatric
popula-tion is less than 0.5 cases per million
1. It may affect any
organ system with potential life-threatening
morbidi-ties, thus an early diagnosis and prompt treatment are
needed. Cases with isolated organ affection are
ex-tern. However, up to 40% of cases with single organ
GPA are ANCA negative. The frequency of ocular
in-volvement, according to a recent meta-analysis, is 24%
of cases
3; nevertheless, orbital involvement is
infre-quent as initial manifestation and exceptional as a
sin-gle-organ affection
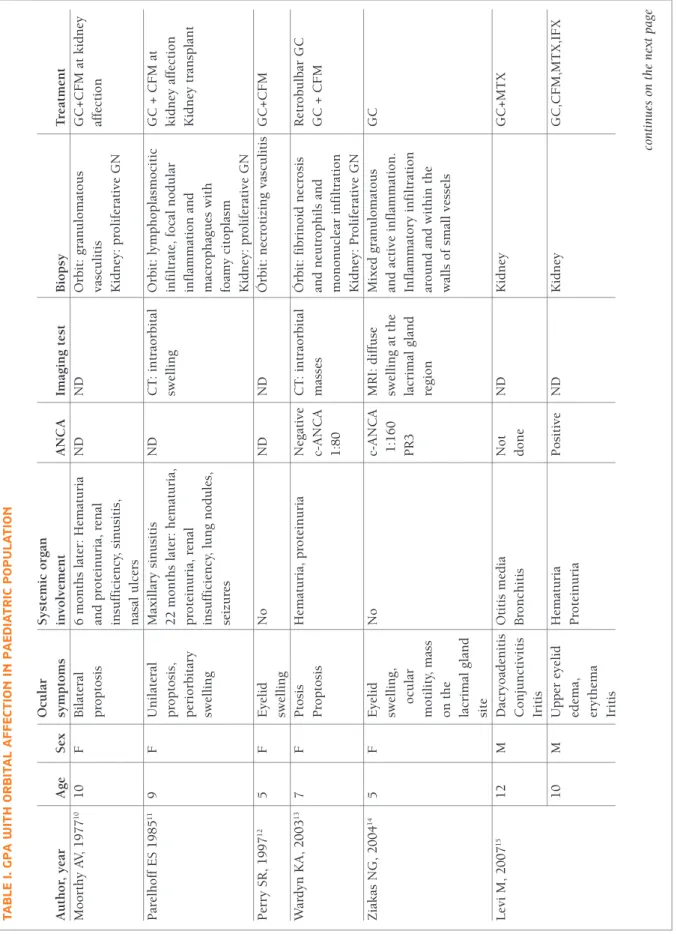
4,5. In Table I we summarize
previ-ously reported cases of paediatric GPA with orbital
affection. Due to the absence of controlled trials in
pae-diatric GPA, adult therapeutic approaches are
recom-mended. Thus, high dose steroids and preferably
cy-DISCUSSION
GPA is a very infrequent vasculitis in childhood, with
a female predominance and a mean age at diagnosis
between 11 to 14 years
2. Most commonly affected
or-gans include ear nose and throat, kidney and lungs
3,4.
Subglottic stenosis or nasal deformities such as saddle
nose deformity are more commonly observed in
chil-dren than in adults. More than 90% of patients are
pos-itive for ANCA
5, being c-ANCA the most common
pat-FIGURE 1.Diagnostic MRI with axial T2WI (A), axial T1WI (B), and axial contrast enhanced T1WI (C) shows a poorly defined mass in the external periorbital region, with heterogeneous T2 signal intensity and avid enhancement (arrows). Follow up MRI 1 year after treatment onset with axial T2WI (D), axial T1WI (E), and axial contrast enhanced T1WI (F) shows complete resolution of the mass (arrow heads).
A B
C
E
D
F
FIGURE 2.Histological examination revealed a granulomatous inflammatory process with lymphohistiocytic infiltrate, necrotizing granulomas and small and medium-sized vessels vasculitis. (A) Panoramic view of the diffuse inflammatory infiltrate with a necrotizing granuloma (between the arrows) (PAS). (B) Detail of small-sized vessels with lymphohistiocytic infiltrate and activated endothelium (PAS).
TA B LE I. G P A w IT h O R B IT A L A FF EC TI O N IN P A ED IA TR IC P O P U LA TI O N O cu la r S y st em ic o rg an A u th o r, y ea r A g e S ex sy m p to m s in v o lv em en t A N C A Im ag in g t es t B io p sy T re at m en t M o o rt h y A V, 1 9 7 7 1 0 1 0 F B il at er al 6 m o n th s la te r: H em at u ri a N D N D O rb it : g ra n u lo m at o u s G C + C F M a t k id n ey p ro p to si s an d p ro te in u ri a, r en al v as cu li ti s af fe ct io n in su ff ic ie n cy , si n u si ti s, K id n ey : p ro li fe ra ti v e G N n as al u lc er s P ar el h o ff E S 1 9 8 5 1 1 9 F U n il at er al M ax il la ry s in u si ti s N D C T : in tr ao rb it al O rb it : ly m p h o p la sm o ci ti c G C + C F M a t p ro p to si s, 2 2 m o n th s la te r: h em at u ri a, sw el li n g in fi lt ra te , fo ca l n o d u la r k id n ey a ff ec ti o n p er io rb it ar y p ro te in u ri a, r en al in fl am m at io n a n d K id n ey t ra n sp la n t sw el li n g in su ff ic ie n cy , lu n g n o d u le s, m ac ro p h ag u es w it h se iz u re s fo am y c it o p la sm K id n ey : p ro li fe ra ti v e G N P er ry S R , 1 9 9 7 1 2 5 F E y el id N o N D N D Ó rb it : n ec ro ti zi n g v as cu li ti s G C + C F M sw el li n g W ar d y n K A , 2 0 0 3 1 3 7 F P to si s H em at u ri a, p ro te in u ri a N eg at iv e C T : in tr ao rb it al Ó rb it : fi b ri n o id n ec ro si s R et ro b u lb ar G C P ro p to si s c-A N C A m as se s an d n eu tr o p h il s an d G C + C F M 1 :8 0 m o n o n u cl ea r in fi lt ra ti o n K id n ey : P ro li fe ra ti v e G N Z ia k as N G , 2 0 0 4 1 4 5 F E y el id N o c-A N C A M R I: d if fu se M ix ed g ra n u lo m at o u s G C sw el li n g , 1 :1 6 0 sw el li n g a t th e an d a ct iv e in fl am m at io n . o cu la r P R 3 la cr im al g la n d In fl am m at o ry i n fi lt ra ti o n m o ti li ty , m as s re g io n ar o u n d a n d w it h in t h e o n t h e w al ls o f sm al l v es se ls la cr im al g la n d si te L ev i M , 2 0 0 7 1 5 1 2 M D ac ry o ad en it is O ti ti s m ed ia N o t N D K id n ey G C + M T X C o n ju n ct iv it is B ro n ch it is d o n e Ir it is 1 0 M U p p er e y el id H em at u ri a P o si ti v e N D K id n ey G C ,C F M ,M T X ,I F X ed em a, P ro te in u ri a er y th em a Ir it is co n ti n u es o n t h e n ex t p a ge
TA B LE I. C O N TI N U AT IO N O cu la r S y st em ic o rg an A u th o r, y ea r A g e S ex sy m p to m s in v o lv em en t A N C A Im ag in g t es t B io p sy T re at m en t 9 M E y el id e d em a, N o N o t N D O rb it G C er y th em a d o n e L im it ed m o ti li ty P ro p to si s 1 2 F E y el id e d em a A b d o m in al p ai n ,v o m it in g N eg at iv e N D O rb it a n d k id n ey G C P ro p to si s L im it ed m o ti li ty M ar tí n ez -G u ti er re z 7 F D is p la ce m en t 3 y ea rs a ft er o cu la r N eg at iv e C T a n d M R I: O rb it : n o n -s p ec if ic G C a t d ia g n o si s JD , 2 0 0 8 1 6 o f th e g lo b e sy m p to m s: s u b g lo ti c in fi lt ra ti o n a n d h is ti o cy ti c in fi lt ra te G C + C F M + IF X E y el id s w el li n g st en o si s, l u n g a n d k id n ey en la rg em en t o f w it h p la sm ac y to id , p o st er io rl y af fe ct io n la cr im al g la n d s ly m p h o cy te s an d an d s in u si ti s eo si n o p h il ic c el ls L ac ri m al g la n d : p er iv as cu la r an d p er id u ct al ce ll i n fi lt ra te w it h g ra n u lo m at o u s as p ec t C h ip cz y n sk a B , 7 F E y el id S in u si ti s N eg at iv e C T /M R I: T u m o r O rb it : In fl am m at o ry G C + M T X /C F M 2 0 0 9 1 7 sw el li n g , G N m as se s in t h e p se u d o tu m o r (a ll p at ie n ts ) u n il at er al o rb it R en al b io p sy : n ec ro ti zi n g ex o p h th al m ia (a ll p at ie n ts ) G N 1 1 F (a ll p at ie n ts ) H ea ri n g i m p ai rm en t cA N C A + O rb it : N ec ro ti zi n g v as cu li ti s w it h le u k o cy to cl as ia a n d n ec ro ti zi n g g ra n u lo m as su rr o u n d ed b y h is ti o cy te s an d g ia n t ce ll s 8 M O ti ti s m ed ia cA N C A + O rb it N ec ro ti zi n g v as cu li ti s H ea ri n g i m p ai rm en t w it h l eu k o cy to cl as ia a n d n ec ro ti zi n g g ra n u lo m as su rr o u n d ed b y h is ti o cy te s an d g ia n t ce ll s co n ti n u es o n t h e n ex t p a ge
F : fe m al e; M : m al e; N D : n o d at a; A N C A : an ti -n eu tr o p h il c y to p la sm ic a n ti b o d y ; c-A N C A : cy to p la sm ic a n ti -n eu tr o p h il c y to p la sm ic a n ti b o d y ; p -A N C A : p er in u cl ea r an ti -n eu tr o p h il cy to p la sm ic a n ti b o d y ; P R 3 : p ro te in as e 3 ; IR : in su fi ci en ci a re n al ; G N : g lo m er u lo n ep h ri ti s; C T : co m p u te d t o m o g ra p h y ; M R I: m ag n et ic r es o n an ce i m ag in g ; G C : g lu co co rt ic o id s; M T X : m et h o tr ex at e; C F M : cy cl o p h o sp h am id e; I F X : in fl ix im ab ; R T X : ri tu x im ab TA B LE I. C O N TI N U AT IO N O cu la r S y st em ic o rg an A u th o r, y ea r A g e S ex sy m p to m s in v o lv em en t A N C A Im ag in g t es t B io p sy T re at m en t 9 F E y el id s w el li n g , F ev er s A ty p ic al C T /M R I: T u m o r O rb it : N ec ro ti zi n g G C + M T X /C F M u n il at er al R h eu m at ic p ai n s A N C A m as se s in t h e v as cu li ti s w it h ex o p h th al m ia o rb it le u k o cy to cl as ia D ey M , 2 0 1 1 1 8 9 F E y el id s w el li n g S ad d le -n o se d ef o rm it y, o ti ti s cA N C A C T : so ft t is su e Ó rb it : ch ro n ic G C 1 :2 0 sw el li n g i n in fl am m at io n w it h p A N C A la cr im al g la n d p er iv as cu la r in fi lt ra te s 1 :4 0 U re E , 2 0 1 6 1 9 9 F E y es r ed n es s, G N cA N C A M R I: b il at er al O rb it : th ic k en in g o f th e C F M , R T X ey el id s ed em a, in tr ao rb it al -v es se l w al l, m ic ro th ro m b u s T o p ic al G C p to si s an d -e x tr ac o n al s o ft an d p er iv as cu la r ex o p h ta lm u s ti ss u e le si o n s ly m p h o cy ti c in fi lt ra ti o n in t h e v es se ls l u m en a n d fi b ro si s in t h e la cr im al g la n d K id n ey : cr es ce n ti c g lo m er u lo n ep h ri ti s D ro b y sh ev a A , 1 2 M U n il at er al N o cA N C A M R I: i n fi lt ra ti v e O rb it : fi b ro v as cu la r ti ss u e G C + M T X 2 0 1 8 2 0 ey el id s w el li n g 1 :2 0 le si o n o f th e w it h d en se c o ll ag en o u s + p to si s o rb it fi b ro si s an d m ix ed in fl am m at o ry i n fi lt ra te w it h p la sm a ce ll s
clophosphamide (CYP) are used as induction therapy,
although there is an increase in the use of RTX
3-6. In
our case, due to the absence of systemic symptoms and
the potential gonadal toxicity of CYP, methotrexate and
corticosteroids were prescribed initially. RTX was then
started because of refractoriness as a second line the
-rapy. Some cases of GPA with orbital affection
success-fully treated with RTX have been published in
adult-hood
7-9, but no cases with limited orbital involvement
have been previously reported in children.
In our case, the patient presented with a limited
affection of the orbicular musculature, reasonably ru
-ling out any systemic involvement. Treatment with
steroids and methotrexate was started. RTX was
asso-ciated due to refractoriness, with excellent response
and disappearance of the lesion.
CONCLUSIONS
GPA can exceptionally present as a single-organ
dis-ease in childhood. RTX might be considered as a
po-tential treatment in cases refractory to conventional
im-munosuppressive therapy.
CORRESPONDENCE TO
Víctor Martínez Taboada Rheumatology Department
Hospital Universitario Marqués de Valdecilla Av. Valdecilla, 25
39008 Santander, Cantabria, Espanha E-mail: vmartinezt64@gmail.com
REFERENCES
1. Sacri AS, Chambaraud T, Ranchin B, Florkin B, See H, Decramer S et al. Clinical characteristics and outcomes of childhood-on-set ANCA-associated vasculitis: a French nationwide study. Nephrol Dial Transplant 2015; 30 Suppl 1:i104-i112. 2. Calatroni M, Oliva E, Gianfreda D, Gregorini G, Allinovi M,
Ramirez GA et al. ANCA-associated vasculitis in childhood: re-cent advances. Ital J Pediatr 2017; 43:46.
3. Iuidici M, Quartier P, Terrier B, Mouthon L, Guillevin L, Puechal X. Childhood-onset granulomatosis with polyangiitis and mi-croscopic polyangiitis: systematic review and meta-analysis. Or-phanet J Rare Dis 2016; 11:141.
4. Jariwala MP, Laxer RM. Primary vasculitis in childhood: GPA and MPA in childhood. Front Pediatr 2018; 16: 6:226. 5. Cabral DA, Canter DL, Muscal E, Nanda K, Wahezi DM,
Spald-ing SJ et al. ComparSpald-ing PresentSpald-ing Clinical Features in 48 Chil-dren With Microscopic Polyangiitis to 183 ChilChil-dren Who Have Granulomatosis With Polyangiitis (Wegener's): An ARChiVe Co-hort Study. Arthritis Rheumatol 2016; 68:2514-26.
6. Morishita KA, Moorthy LN, Lubieniecka JM, Twilt M, Yeung RSM, Toth MB et al. Early Outcomes in Children With An-tineutrophil Cytoplasmic Antibody-Associated Vasculitis. Arthritis Rheumatol 2017; 69:1470-9.
7. Baslund B, Wiencke AK, Rasmussen N, Faurschou M, Toft PB. Treatment of orbital inflammation with rituximab in Wegener's granulomatosis. Clin Exp Rheumatol 2012; 30(1 Suppl 70):S7--10.
8. Bitik B, Kilic L, Kucuksahin O, Sahin K, Tufan A, Karadag O et al. Retro-orbital granuloma associated with granulomatosis with polyangiitis: a series of nine cases. Rheumatol Int 2015; 35:1083-1092.
9. Joshi L, Tanna A, McAdoo SP, Medjeral-Thomas N, Taylor SR, Sandhu G et al. Long term outcomes of rituximab therapy in ocular granulomatosis with polyangiitis: impact on localized an nonlocalized disease. Ophtalmology 2015; 122:1262-1268. 10. Moorthy AV, Chesney RW, Segar WE, Groshong T. Wegener granulomatosis in childhood: prolonged survival following cy-totoxic therapy. J Pediatr 1977; 91:616-618.
11. Parelhoff ES, Chavis RM, Friendly DS. Wegener's granulo-matosis presenting as orbital pseudotumor in children. J Pe diatr Ophthalmol Strabismus 1985; 22:100-4.
12. Perry SR, Rootman J, White VA. The clinical and pathologic constellation of Wegener granulomatosis of the orbit. Ophthal-mology 1997; 104:683-94.
13. Wardyn KA, Ycinska K, matuszkiewicz-rowinska J, Chipczyn-ska M. Pseudotumour orbitae as the initial manifestation in We-gener's granulomatosis in a 7-year-old girl. Clin Rheumatol 2003; 22:472-474.
14. Ziakas NG, Boboridis K, Gratsonidis A, Hatzistilianou M, Ka-triou D, Georgiadis NS. Wegener's granulomatosis of the orbit in a 5-year-old child. Eye (Lond) 2004; 18: 658-660. 15. Levi M, Kodi SR, Rubin SE, Lyons C, Golden R, Olitsky SE et
al. Ocular involvement as the initial manifestation of Wege ner's granulomatosis in children. J AAPOS 2008; 12:94-96. 16. Martínez-Gutierrez JD, Mencia-Gutierrez E, Gutierrez-Díaz E,
Rodriguez-Peralto JL. Bilateral idiopathic orbital inflammation 3 years before systemic Wegener's granulomatosis in a 7-year-old girl. Clin Ophthalmol 2008; 2:941-944.
17. Chipczynska B, Gralek M, Hautz W, Zegadlo-Mylik M, Kocyla-Karczmarewicz B, Kanigowska K et al. Orbital tumor as an ini-tial manifestation of Wegener's granulomatosis in children: a series of four cases. Med Sci Monit 2009; 15:CS135-CS138. 18. Dey M, Lawyi L, Wilson RS. Orbital Wegener's granulomatosis
as the initial presentation in a 9-year-old child. J R Soc Med 2011; 104:332-334.
19. Ure E, Kayadibi Y, Sanli DT, Hasiloglu ZI. Orbital involvement as the initial presentation of Wegener granulomatosis in a 9-year-old girl: MRimaging findings. Diagn Interv Imaging 2016; 97: 1181-1182
20. Drobysheva A, Fuller J, Pfeifer CM, Rakheja D. Orbital granu-lomatosis with polyangiitis mimicking IgG4-related disease in a 12-year-old male. Int J Surg Pathol 2018; 26: 453-458