w w w . e l s e v i e r . p t / r p s p
Original
Article
Safety
climate
in
the
operating
room:
Translation,
validation
and
application
of
the
Safety
Attitudes
Questionnaire
João
Pedro
Alexandre
Pinheiro
a,b,∗,
António
de
Sousa
Uva
c,daDepartamentodeRadiologia,EscolaSuperiordeSaúde,UniversidadedoAlgarve,AvenidaDr.AdelinodaPalmaCarlos,8000-510Faro, Portugal
bCES–CentrodeEstudosemSaúdedaUniversidadedoAlgarve,Portugal
cEscolaNacionaldeSaúdePública,UniversidadeNovadeLisboa,AvenidaPadreCruz,1600-560Lisboa,Portugal dCISP–CentrodeInvestigac¸ãoemSaúdePública,ENSP/UNL,Lisboa,Portugal
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received19April2015 Accepted28July2015
Availableonline22November2015
Keywords: Safetyclimate Operatingroom Ergonomics Patientsafety Healthcarequality
a
b
s
t
r
a
c
t
Background:Safetyclimateassessmentisincreasinglyrecognizedasanimportantfactorin healthcarequalityimprovement,especiallyinoperatingrooms(OR).Oneofthemost com-monlyusedandrigorouslyvalidatedtoolstomeasuresafetycultureistheSafetyAttitudes Questionnaire(SAQ).ThisstudypresentsthevalidationoftheOperatingRoomVersionofthe SAQ(SAQ-OR)foruseinPortugueseHospitals.Thepsychometricpropertiesofthetranslated questionnairearealsopresented.
Methods:TheoriginalEnglishversionoftheSAQ-ORwastranslatedandadaptedtothe Portuguesesettingbyforward–backwardtranslationmethodandappliedinacentralpublic hospital.ScalepsychometricswereanalyzedusingCronbach’salphaandinter-correlations amongthescales.
Results:Theinternalconsistencytestyieldedvaluesaround0.9forall73items.TheCFAand itsgoodness-of-fitindices(SRMR0.05,RMSEA0.002,CFI0.90)showedanacceptablemodel fit.Inter-correlationsbetweenthefactorssafetyclimate,teamworkclimate,job satisfac-tion,perceptionsofmanagement,andworkingconditionsshowedmoderatecorrelation witheachother.82validquestionnaireswereanalyzedrevealingsignificantdifferencesin communicationratingsbetweendifferentjobs,mainlybetweensurgeons(4.2)andbetween nursesandsurgeons(2.9).Workingconditionsandjobsatisfactionhavethehighestscore with3.8and3.5,respectively,andperceptionsofmanagementhavethelowestscore(2.8).
Conclusion: ThePortuguesetranslationoftheSAQ-ORrevealsgoodpsychometric proper-tiesforstudyingtheorganizationalsafetyclimate,howeverlargerandfurtherstudiesare requiredtocompensatethelackofsubjectsinsomeitems.Likeotherstudies,thisscale seemstobeanacceptabletoadequatetooltoevaluatethesafetyclimate.Resultsallowed
∗ Correspondingauthor.
E-mailaddresses:jppinheiro@ualg.pt,joao.pinheiro88@gmail.com(J.P.A.Pinheiro).
http://dx.doi.org/10.1016/j.rpsp.2015.07.006
0870-9025/©2015TheAuthors.PublishedbyElsevierEspa ˜na,S.L.U.onbehalfofEscolaNacionaldeSa ´udeP ´ublica.Thisisanopenaccess articleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/4.0/).
aresatisfactory.However,thereislatitudeforimprovement,especiallyintheinvolvement ofthemanagementbodiesasthisfactorhasthelowestscoreforthemajorityofhealthcare professionals.
©2015TheAuthors.PublishedbyElsevierEspa ˜na,S.L.U.onbehalfofEscolaNacionalde Sa ´udeP ´ublica.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Clima
de
seguranc¸a
no
bloco
operatório:
traduc¸ão,
validac¸ão
e
aplicac¸ão
do
Questionário
de
Atitudes
de
Seguranc¸a
Palavras-chave: Climadeseguranc¸a Blocooperatório Ergonomia Seguranc¸adodoente Qualidadeemsaúde
r
e
s
u
m
o
Introduc¸ão: Aavaliac¸ãodoclimadeseguranc¸aécadavezmaisreconhecidacomoumfator namelhoriadaprestac¸ãodecuidadosdesaúde,especialmentenoblocooperatório(BO). Umdosinstrumentosmaiscomumente validadoseutilizadosparamedira Culturade Seguranc¸aéoSafetyAttitudesQuestionnaire(SAQ)ouQuestionáriodeAtitudedeSeguranc¸a (QAS).Esteestudoapresentaavalidac¸ãodaversãoparaBlocoOperatório(QAS-BO),para aplicac¸ãonasinstituic¸õesdesaúdeportuguesas.Ascaracterísticaspsicométricasdo ques-tionáriotraduzidosãotambémapresentadas.
Metodologia:AversãooriginaleminglêsdoQAS-BO,foitraduzidaeadaptadaparaocontexto português,atravésdoprocessodetraduc¸ão-retraduc¸ãoeaplicadonumhospitalpúblico central.AanálisepsicométricafoifeitaatravésdoalfadeCronbachedascorrelac¸õesentre escalas.
Resultados: Os testes deconsistênciainterna obtiveramvalores médiosde 0.9paraos 73itens.Aanálisefatorialeograudeajuste(SRMR0.05,RMSEA0.002,CFI0.90)obtiveram valoressatisfatórios.Asrelac¸õesentreoclimadeseguranc¸a,trabalhoemequipa,satisfac¸ão profissional,percec¸ãosobreosórgãosdegestãoecondic¸õesdetrabalhosãomoderadas. Umtotalde 82questionáriosforamanalisadoserevelaramdiferenc¸assignificativasna comunicac¸ãoentrediferentesclassesprofissionais,nomeadamenteentrecirurgiões(4.2) eentrecirurgiõeseenfermeiros(2.9).Ascondic¸õesdetrabalhoeasatisfac¸ãoprofissional obtiveramosvaloresmaiselevados,com3.8e3.5respetivamente,eapercec¸ãosobreos órgãosdegestãoovalormaisbaixo(2.8).
Conclusão: AversãoportuguesadoQAS-BO,apresentaboascaracterísticaspsicométricas paraestudaroclimadeseguranc¸adasinstituic¸õesdesaúde,nãoobstante,sãonecessários estudosmaisabrangentesdeformaacolmataroreduzidonúmerodeelementosemalguns itens.Talcomooutrosestudosrevelaram,esteinstrumentoéaceitávelparaanalisaroclima deseguranc¸a.Osresultadospermitemconcluirqueascondic¸õesdetrabalhoeasatisfac¸ão profissionalsãosatisfatórias.Noentanto,existeoportunidadedeintervenc¸ãoemelhoria, principalmentenoenvolvimentodosórgãosdegestão.
©2015OsAutores.PublicadoporElsevierEspa ˜na,S.L.U.emnomedeEscolaNacional deSa ´udeP ´ublica.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
PopulationbasedresearchsuggeststhatintheUnitedStates between 44,000 and 98,000 patients die each year from preventable errors, making medical error the eighth most commoncauseofdeath.1Operatingrooms(OR)canhavea
highprevalenceoferrors,beinganinterdisciplinary,complex activitywithastrongdependenceontechnicalskill,where ergonomicsandorganizationalfactorsplayanessentialrole. Duetothesefactorsitisimperativethatthesafety climate in the OR isanalyzed in order to improve patient safety.2
Effortsto assess and improve safety culture and to better defineitsroleinpatientsafetyarefacilitatedbyits measure-ment.By identifying attributes ofanorganization that are
both malleable and potentially related to safety,managers canintervenetoimprovethequalityofcare.Existingpatient safetyclimatemeasurementtoolsarenumerous,whereas lit-tle informationintheliteratureprovidesguidance tousers orresearchersintheselectionoftoolsforresearchorsafety improvementmeasurementinitiatives.3
Patientsafetyisfundamentaltohealthcarequality. Atten-tionhasrecentlyfocusedonthepatientsafetyclimateofan organization andits impact onpatientoutcomes.A strong safety climateappearstobeanessentialconditionforsafe patientcareinhospitals.Anumberofinstrumentsareused tomeasurethispatientsafetyclimateorculture.TheSafety Attitudes Questionnaire (SAQ) is a validated, widely used instrument toinvestigatemultiplefactorsofsafetyclimate attheclinicallevel inavarietyofinpatientandoutpatient
settings.4Variationsonthedefinitionofsafetycultureexist.5
“Safety culture” and “safety climate” are sometimes used interchangeably,butintheliterature,differentmeaningstend tobegiventotheterms.Measuringsafetycultureorsafety climate is important because the culture of an organiza-tion, team perceptions influence patient safety outcomes, and these measurescan beused to monitorchanges over time.6Thesafetycultureispartoftheoverallcultureofan
organization.7 Thisreferstohowpatientsafetyisdesigned
andimplementedwithinanorganizationandthestructures andprocessestosupportthem.8Safetyculturebecame
pop-ular after the Chernobyl nuclear disaster in 1986, when it wassuggestedthatorganizationscanreduceaccidentsand safetyincidentsthroughthedevelopmentofa“positivesafety culture”.9 Therefore, the concept of safety culture is not
unique tohealthcare,and has been widelyused inthe oil industries, gasandenergy, transport,aviation and military sectors.10The“safetyculture”isbroadlydefinedas:“aglobal
phenomenonthatspansthenorms,valuesandbasic assump-tions ofawholeorganization. Climate,on the other hand, ismorespecificandreferstoprofessionalperceptionof par-ticularaspectsoftheorganization’sculture”.11Comparedto
safetyclimate,cultureisabroadertermthatrepresentsall aspects and values of an organization as well as actions related to safety, while the climate focuses more on the perceptionthatprofessionalshaveabouthowsafetyis man-agedinorganizations.12 Safetyclimatehasbeendefinedas
“thewaywedothingsaroundhere,”orperceptionsof poli-cies,practicesand“shared”procedures.13Assuch,thesafety climate-spectrumdescribesanorganizationthatisinfluenced byhowpeoplebehave,thinkandfeelaboutsafetyissues.This isacomplexphenomenonthatisnotalwaysunderstoodby the leadersofhealthcareinstitutions, thusmaking it diffi-culttooperationalize,andessentialleadershipexperienceto achieveaclimateofsafetythroughouttheorganization.14In
thisview,thesafetycultureisabroadtermthatrepresents allaspectsand valuesofanorganizationaswellasactions relatedtosecurity,12 whilesafety climateisasubsetofthe
broadercultureandreferstoperceptionshealthprofessionals onpatientsafetywithintheorganization.15 Forthisreason,
someauthorssuggestthatitiseasiertomeasuresafety cli-mate,becausecultureismuchbroader.7Thisfocusesmore
onperceptionsofsecurityprofessionalsregardingsupportfor themanagement,supervision,risks,policiesandpracticesof security,trustandopenness.
Concerningoperatingroomsteamsarecomposedbythree differentcareers(surgery,anesthesiologyandnursing)with intermittent representations by radiology and pathology.16
Actionin OR is acomplex, interdisciplinary practice, with heavyrelianceonindividualaction(humantechnicalskills), heldwithincomplexorganizationswherehumanandteam factors(humannon-technicalskills)andorganizational fac-tors(system)playakeyroleinaconstantinteractionbetween humans,machines andequipment.2TheORinthelogicof
the open environment system receives various inputs and throughasetofactivities,transformsresources(inputs)into results(outputs)17 andissensibletoexternalinfluenceson
performanceandgroupdynamics.18Theenvironmentofthe
operatingroom,byitsverynature,isconducivetoaccidents andteamworkandcooperationiscriticaltotheefficiencyand
Table1–SAQ-ORfactorsanddefinitions.
Factors Definition
Teamworkclimate Perceivedqualityofcollaborationbetween personnel
Jobsatisfaction Positivityabouttheworkexperience Perceptionsof
management
Approvalofmanagerialaction Safetyclimate Perceptionsofastrongandproactive
organizationalcommitmenttosafety Workingconditions PerceivedqualityoftheOR’swork
environmentandlogisticalsupport (staffing,equipment,etc.)
Stressrecognition Acknowledgmentofhowperformanceis influencedbystressors
aboveallforsafetyinsurgeryanditsdeficitisresponsiblefor abouthalfoferrorsdetected.2
Methods
TheSafetyAttitudesQuestionnaire-OperatingRoom version
TheSAQwasdevelopedtomeasureattitudesregardingsafety climate.TheSAQisarefinementoftheIntensiveCareUnit ManagementAttitudes Questionnaire19andthefullversion
oftheSAQcomprises60items,whereastheORversion con-tains 59 items, with30 belongingto sixfactors:teamwork climate,jobsatisfaction,perceptionsofmanagement,safety climate,workingconditions,andstressrecognition20(Table1).
Thequestionnairetakesapproximately10–15mintocomplete andeachitemisansweredusinga5-pointLikertscale (Dis-agreeStrongly,DisagreeSlightly,Neutral,AgreeSlightly,Agree Strongly).21
TranslationoftheSafetyAttitudes Questionnaire-OperatingRoom(phase1)
ThequestionnairewastranslatedfromtheoriginalinEnglish usingtheforward–backwardtranslationmethod.TheEN-PT translationisperformedbytwoindependenttranslators(A– PortuguesepersonwithknowledgeofEnglishandB–English person with knowledge of Portuguese), in which the first performedthetranslationandthesecondcarriedoutthe veri-ficationofthattranslation.AtranslatorC(Englishpersonwith knowledgeofPortuguese)translatedthePortugueseversion ofthequestionnairebacktoEnglish.Finallywecomparedthe originalversionofthequestionnaire(writteninEnglish)with theEnglishversionofthetranslator.Theequalityor similar-itybetweenthesetwoquestionnairesindicateswhetherthe Portugueseversionofthequestionnaireissuitablefor appli-cation.
Facevalidity(phase2)
Beforeusingthe instrumentinasampleofhealthcare pro-fessionals, apre-testwas performed tovalidate,check the instrument effectiveness and make any corrections. The
facevaliditywas testedby4nursesand 4physicians, ran-domly selected from the OR team withdifferent ages and specialties. They studied the Portuguese version and were guidedtoindicateconcernsabouttheitemsandfeelfreeto proposeabetterformulation.Commentswerethendiscussed bytheresearchersandaconsensuswasreachedandafinal translatedSAQ-ORPortugueseversionwasestablished.
PsychometrictestingoftheSafetyAttitudesQuestionnaire basedonsurveydata
Across-sectionaldesignwasusedtotesttheinternal con-sistencyoftheSAQ-OR.Surgeons,Nurses,Anesthesiologists, Radiographersand Auxiliarieswithatleast1year of work-ingexperienceatacentralhospitalfromtwosurgicalwards wereaskedtofilloutthePortuguesetranslationoftheSAQ-OR. Respondentdemographiccharacteristicssuchasgender,age, professionalcategory,professionalexperience, employment statuswerealsoincluded.
Datacollectionandethicalconsiderations
ThequestionnairesweredistributedtotheSurgeons,Nurses, Anesthesiologists,RadiographersandAuxiliariesbythehead nurseandheadAnesthesiologistortheresearcherandhad tobecompleted within2months. All questionnaireswere collected in a (secured) box on the ward. Every week, a reminderwassenttowardstaff.Respondentswereinformed thatparticipationwasvoluntary.Questionnairesweretreated anonymously,and that the decisiontoreturn acompleted questionnairewasdeemedtheirinformedconsent.Thestudy wasapprovedbytheMedicalEthicsCommitteeofAlgarve’s HospitalCenter(CentroHospitalardoAlgarve–CHA).
Statisticalanalysis
Descriptivestatistics were usedto describethe population characteristicsandtheSAQ-ORitemandscale-levelresultson theunits.InternalconsistencyofthetotalSAQ-ORanditssix factors“teamworkclimate,”“safetyclimate,”“stress recogni-tion,”“workingconditions,”“jobsatisfaction”and“perception of management” was measured by calculating Cronbach’s alpha.
Thegoodness-of-fitstatisticwasusedtomeasurewhether the overall model fit was good. Three different fit indices wereused:standardizedrootmeansquareresidual(SRMR), rootmeansquareerrorofapproximation(RMSEA)and com-parative fit index (CFI). The goodness-of-fit statistics and correlationmatrixwereanalyzedwithIBMSPSSAMOS (Anal-ysisofMomentStructures)V.22.22
A good model fit between the target model and the observeddataaredistinguishedbySRMRvaluesbetween0.0 and1.0,where0.0indicatesperfectfit,andRMSEAvalues≤.05 andCFIvalues≥.95.21Confirmatoryfactoranalysis(CFA)was
used for conclusions about the conceptual and semantic equivalence ofatranslatedquestionnaire20 anddeals with
therelationshipsbetweenobservedmeasuresorindicators. Inthiscontext,CFAisusedtoverifythenumberof underly-ingfactorsoftheinstrumentandthepatternofitem–factor relationships(factorloadings).22
Normality test was performed using the Kolmogorv– Smirnovtest.Dataanalysiswasperformedbyfrequencytables anddescriptivestatistics.Inordertocomparemorethantwo groups,theKruskal–Wallistest(H)wasperformed.Finally,for areviewoftherelationshipbetweenvariables,theSpearman correlation(rs)testwasapplied.Alldatawereanalyzedusing SPSS(version20.0forWindows).
Results
Translation,validityandinternalconsistencyofSafety AttitudesQuestionnaire-OperatingRoom
TranslationoftheSafetyAttitudesQuestionnaire-Operating Room(phase1)
Nosignificantdifferencesweredetectedbetweenthe transla-tions.Ethnicgroupwaspresentinthedemographicssection oftheEnglishversionofthequestionnaire,butwasdecidedto beremovedasitwasconsideredtobeirrelevantandstill pos-sibly offensive.Somequestions wereconsidered somewhat delicate,becauseofthesensitivitiesregardingerrors,staffing, management,andworkload.
Facevalidity(phase2)
No majorremarkswere givenbythe four nurses and four physicians who evaluated the face validityofthe SAQ-OR. Minor suggestionswere giventoimprovethe clarityofthe wording,e.g.theword“medicalerror”waschangedto “clin-icalerror”(“erromédico”to“erroclínico”)astheterm“medical error”inPortugueseimpliesthattheseareerrorsperformed byphysiciansaloneandnotbyallhealthcareprofessionals. Moreoverabriefdefinitionofwhatwasconsidereda“clinical error”wasincludedonthebottomofthequestionnaire simi-lartotheoriginalEnglishversion(“Clinicalerrorisdefinedhas anymistakeinthedeliveryofcare,byanyhealthcare profes-sional,regardlessoftheoutcome”).Inaddition,onespelling mistakewasdetectedandcorrected(“fatigue”wastranslated to“fatiga”insteadof“fadiga”)(Annex1).
PsychometrictestingoftheSafetyAttitudesQuestionnaire basedonsurveydata
Thesampleconsistsof82healthcareprofessionalswhohold positionsintheoperatingroom,dividedinto5distinct pro-fessional classes. 18 surgeons (22%), 43 nurses (52%), 11 anesthesiologists(13%),6(7%)Radiographersand4auxiliaries (5%).21subjectshaveagesbetween20and29years(25.6%),26 between30and39years(31.7%),18between40and49years (22%),14between50and59years(17%)and3between60and 69years(3.7%).
We obtained a mean age of 38.7 years, a minimum of 23 yearsandamaximum of61years.Theaveragenumber ofyearsthathealthprofessionalsworkinginthatinstitution is12.6yearswith10.1yearsofprofessionalexperiencewith aminimum of1yearand amaximumof36years, respec-tively.Regardingthesexdistributionofthesample,44were female(53.7%)and38male(46.3%).Ofallsurgeons,15were males.Witha totalof43nurses,the majority(n=27) were females.
Table2–Cronbach’salphaforeachofthefactorsofthe SafetyAttitudesQuestionnaire-ORversion.
Factors Cronbach’s alpha Numberof items(n=59) Teamworkclimate 0.47 17 Safetyclimate 0.67 19 Stressrecognition 0.72 10 Jobsatisfaction 0.55 4 Workingconditions 0.50 4 Perceptionsofmanagement 0.34 5 ˛≥0.9,excellent;0.7–0.9,good;0.6–0.7,acceptable;0.5–0.6,poor; <0.5,unacceptable.
Table3–Goodness-of-fitindicesforCFAoftheSAQ-OR factors.
Samplesize 82
Standardizedrootmeansquareresidual(SRMR) 0.05 Rootmeansquareerrorofapproximation(RMSEA) 0.00 Comparativefitindex(CFI) 0.90 SRMR reference: 0.0–1.0, with 0.0indicating perfect fit.RMSEA reference: ≤0.05,good; ≥0.10, poor fit.CFI reference: 0.90–0.95, acceptable;>0.95,good.
Themajorityofrespondentsare between0and 5years workinginthe institutionwith24%,andbetween6and10 yearswith28%.Thesameappliestoyearsofexperiencewith 34.1%and31.7%respectively.Themajorityofthesampleis employedfulltime(91.5%)andonly7elementsclaimtobe hiredpart-time orcontractual. Regarding shiftsperformed, mostofthestaffsaidtheyholdvariableshifts(73.2%). Internalconsistency
Inordertostudytheinternalconsistencyoftheinstrument used,Cronbach’salphaforeachofthefactorsofthe question-nairewascalculated(Table2).TheoverallCronbach’salpha assumes avalue of0.89 for all itemsof the questionnaire whichisborderlineexcellent.
Internalconstructvalidity
Thegoodness-of-fitvaluesusedtoevaluatetheinternal con-structvalidityaredisplayedinTable3.TheSRMRvaluewas
Table5–Communicationanalysisbydifferent professions(n=82).
Communication Average Standard deviation(SD) Surgeons 3.1 0.9 Nurses 3.7 0.7 Anesthesiologists 3.3 0.9 Radiographers 3.4 0.8 Auxiliaries 3.4 0.8 Communication(overall) 3.5 0.6 1,verylow;2,low;3,adequate;4,high;5,veryhigh.
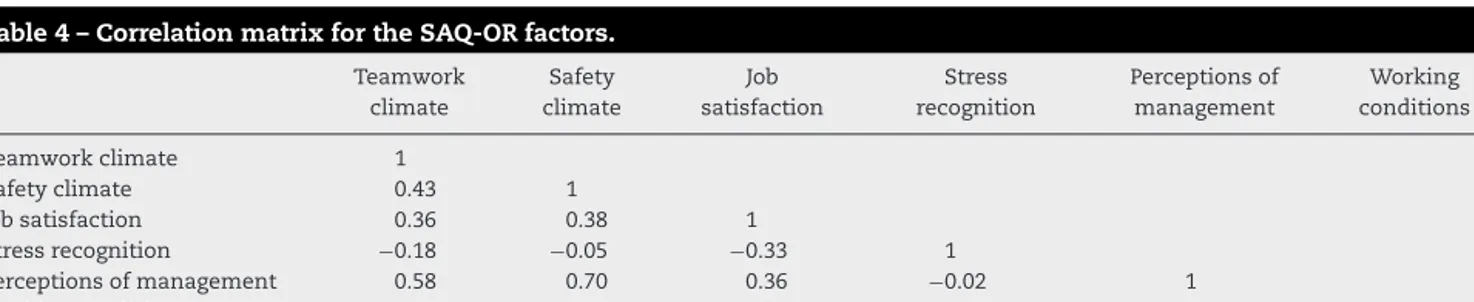
0.05,theRMSEAwas0.00,andtheCFIvaluewas0.90,which indicatesanacceptablemodelfitapproximationofthe trans-latedversionoftheSAQ-OR.Theinter-correlationsbetween the factors are presented in Table 4 and ranged from 0.2 to0.7.
Communication
Based on a Likert scale of 6 points the sample classified the qualityofcommunication. Descriptively representedin
Table 5are the averagesof theresponses forthe different professionsandinTable6aboutcommunicationbetween pro-fessionalgroups.
Inordertoascertainwhether therespondent’soccupied functionproducessomeinfluenceontheirperceptionof com-munication, thenonparametric Kruskal–Wallis (H)(Table 7) wasapplied.
SafetyAttitudesQuestionnaire-operatingroomfactors
InTable8areshownthefactorsoftheinstrumentthat com-prisesafetyclimate.Workingconditionsisthefactorthathasa higheraverage(3.8)andperceptionsofmanagementhavethe lowestaverage(2.8).Theclimateteamalsohasahighvaluein relationtootherfactors,howeverisconsiderablywithinthe average(3.4).Stillrelatedtothisfactorthesafetyclimatehas thesecondlowestratingwith3.1inaverage.
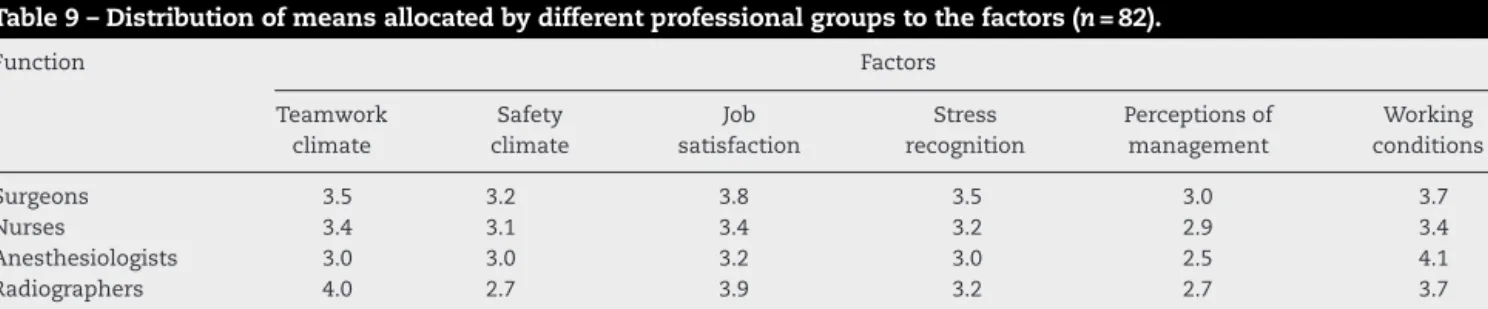
Atablewiththeirrespectiveresponseaveragesattributed bycaregiverstoeachfactorgroupswasalsomade(Table9). Thefactorswithhigherscoresaretheworkingconditionsand jobsatisfaction.
Table4–CorrelationmatrixfortheSAQ-ORfactors.
Teamwork climate Safety climate Job satisfaction Stress recognition Perceptionsof management Working conditions Teamworkclimate 1 Safetyclimate 0.43 1 Jobsatisfaction 0.36 0.38 1 Stressrecognition −0.18 −0.05 −0.33 1 Perceptionsofmanagement 0.58 0.70 0.36 −0.02 1 Workingconditions 0.45 0.24 0.23 −0.09 0.26 1
Table6–Responsedistributiononcommunicationbetweenprofessionals(n=82).
Function Communication
Surgeons Nurses Anesthesiologists Radiographers Auxiliaries
Surgeons 4.2 3.8 3.6 3.6 3.3
Nurses 2.9 3.8 3.1 3.1 3.5
Anesthesiologists 2.7 3.2 3.8 3.7 3.4
Radiographers 2.9 3.4 2.7 4.8 2.6
Auxiliaries 2.8 3.4 3.1 2.2 3.5
1,verylow;2,low;3,adequate;4,high;5,veryhigh.
Thegrayshadeshighlighttherelationbetweenthesameprofession.
Table7–Communicationinfluenceondifferentprofessions(n=82).
Function Communication
Surgeons Nurses Anesthesiologists Radiographers Auxiliaries p
Surgeons 65.6 34.4 32.5 34.0 36.2 0.00
Nurses 39.2 39.2 24.4 28.7 28.8 0.24
Anesthesiologists 38.5 28.0 44.9 19.4 27.6 0.03
Radiographers 48.5 32.2 50.0 72.9 15.6 0.00
Auxiliaries 39.7 440 43.0 24.6 43.5 0.37
Table8–Analysisofsafetyclimatefactors.
SAQfactors Average Standard deviation(SD) Teamclimate 3.4 0.4 Safetyclimate 3.1 0.4 Workingconditions 3.8 0.5 Perceptionsofmanagement 2.8 0.6 Stressrecognition 3.3 0.6 Jobsatisfaction 3.5 0.7
1,verylow;2,low;3,adequate;4,high;5,veryhigh.
Discussion
ThepurposeofthisstudywastotranslatetheSAQ-OR Ver-sionandassessthevalidityandreliabilityofthePortuguese
version.Thevaluesobtainedinthestudy ofvalidityofthe instrument bothin each factor and asa whole are of the same magnitudeofthefigures presentedbytheauthorsof thequestionnaire.19Translationsandadaptationsof“Safety
Attitudes Questionnaire” for other languages also revealed a high content validity.23,24 TheSAQ hasalso been
exten-sively usedtorelateclimatesafety withtheresultsforthe patient,24howeverthisstudydidnotaddressthisissue.The
present valueofCronbach’salphavalueiscloselylinkedto the numberofitemsevaluated. Thegreaterthe numberof items,thehigherthealphavalueobtained.25Thus,itis
pos-sible todetermine thatlowvaluesarecaused bythe small numberofitemsperfactor.26Despitetheusefulnessof
Cron-bach’salphainthestudyofreliability,itisstillanestimate, subjecttomanyinfluencestobetakenintoaccount.Thealpha valueisnotacharacteristicoftheinstrument,butratheran estimateofthereliabilityofthedataobtained,27however,the
valuesrecordedonthevalidityoftheinstrument,using Cron-bach’salpharangedbetween0.68and0.90.21,23,25Thisstudy
Table9–Distributionofmeansallocatedbydifferentprofessionalgroupstothefactors(n=82).
Function Factors Teamwork climate Safety climate Job satisfaction Stress recognition Perceptionsof management Working conditions Surgeons 3.5 3.2 3.8 3.5 3.0 3.7 Nurses 3.4 3.1 3.4 3.2 2.9 3.4 Anesthesiologists 3.0 3.0 3.2 3.0 2.5 4.1 Radiographers 4.0 2.7 3.9 3.2 2.7 3.7 Auxiliaries 4.0 DK/NA 4.3 2.7 3.5 4.1
DK/NA–don’tknow,notapplicable;CD–completelydisagree;PD–partiallydisagree;NAND–neitheragreenordisagree;PA–partiallyagree; CA–completelyagree.
wasconductedinapublichospital,morespecificallyinthe surgerydepartment.Manystudies whichusetheSAQhave sampleswithinthehundredsoreventhousandsofsubjects astheyarelarge-scalestudies.5,20,28Internalconstructvalidity
basedontheCFAandgoodness-of-fitindices(SRMR,RMSEA, andCFI)showedanacceptablemodelfit.Accordingtogood modelfitindices,thePortugueseversionoftheSAQ-ORisa validinstrument.Factorsweremoderatelycorrelatedexcept forstressrecognition,similartotheresultsofthe psychomet-rictestingofotherversionsoftheSAQ-OR.20,21
Themainelementsoftheoperatingroomteamare sur-geons,nursesandanesthesiologists.Radiographersjustadd some timely interventions, particularly in orthopedics or cardiology,16being calledbythe radiologydepartment,and
thereforenotpartofthesurgicalteamitself.Sothis profes-sionalclasshasalsobeenincludedforthesakeofconsistency as indirectly involved withpatient safety in the operating theater.Therearesignificantdifferencesrelatedto commu-nicationbetweentheoperatingroomteam.Nursesalsohave thehighestaverage(3.8)whichsuggestshigherqualityof com-municationbetweenthemandtheotherprofessionswhich agreeswith studies using the same instrument29 followed
byAuxiliaries(3.4),Radiographers(3.4)andAnesthesiologists (3.3).Surgeonshavethelowestaverage(3.1).Communication intheoperatingroomfollowscomplexpatternsandis influ-encedbyrecurrentthemescausingtension.16 Theseresults
however,shouldnotbeextrapolatedorgeneralizedbecause theyareverydependentonthenumberofindividualspresent ineachprofessionalgroup.Nevertheless,similarstudiespoint tosimilarresultsindifferentpatternsandprofessionalclasses havedifferentcommunicationstrategies.26,27,30Observational
studiesreportmoretensepatternsofcommunicationbetween surgeons and nurses.31 Communication patterns between
tensesurgeonsandanesthesiologistswerealsoobserved,but uncommon.16,27 Thiscan beexplainedbythefact thatthe
procedures for dialog are more common among surgeons and nurses. Ina study inwhich they used questionnaires anddirectobservationofsurgicalprocedures,nursesdescribe good partnership as having their opinions respected and acceptedinthe ORandthe surgeonsdescribegood collab-orationwhennursesanticipatetheirneedsandfollowtheir instructions.32 In another study conductedin anintensive
careunitwithsimilarmethodology,doctorsoftenresortedto nursestoprovideadditionalinformationandfurtherdetails onthe evaluationofthe patientduringrounds.33 However,
theydescribemanydifficultiesandlessinvolvementin deci-sionmakingprocessduringtherounds.
Thefactors“safetyclimate”and“perceptionof manage-ment”obtainedtheloweraverages(3.1and2.8respectively) andjobsatisfactionand workingconditionsthehigher(3.5 and3.8respectively).Regardingthedistributionofthe aver-ageresponseofdifferentprofessionalgroupsevidencedthat surgeonsandradiographershavethehighestjobsatisfaction
(3.8and3.9).Nursesgivegreaterscoretoteamclimate(3.4) and working conditions(3.4). Anesthesiologists give higher score tofatigueand stress than other professional groups, followedbysurgeons(3.5)andnurses(3.2).Comparedtothe studiesanalyzed,nurseshavehigherlevelsofstress,followed byanesthesiologistsandsurgeons.5,28,34Theinstrumentused
is derived from a questionnaire for aviation safety. There is overlap betweenthe twoitems ofabout 25%.Ina com-parative study,the sizeofteams betweenOR andaviation demonstrated that the pilots had less tendency to negate theeffectsoffatigueandstressonyourperformanceagainst surgeons(26%versus70%).34Beingcollaborationand
commu-nicationasimportanttothesuccessoftheprocedures,the SAQallowstomeasureteamwork,identifyproblemswithin andbetweenprofessionalgroupsandevaluateinterventions aimedatimprovingpatientsafety.16Otherauthorshave
con-cluded that, as in aviation, errors are more related with non-technicalskills suchas communication,than withthe technicalcapacityandperformance.2,18
Conclusions
The SAQ-OR demonstrates good psychometric capabilities to study safety climate,however largerstudies are needed to address the lack of data on some items. The develop-ment of a valid and reliable instrument is a longitudinal processthatrequiresnumerouspositivefindingsacross dif-ferentsettings.Theresultsindicatethatworkingconditions andjobsatisfactionareacceptable,butitiscrucialtoimprove thesafetyclimateandtheinvolvementofthemanagement bodies. Improving safety climate is crucial for increasing quality of service on surgical wards,and thus, it becomes relevantto improvethe aboveaspects. Ourresults demon-strate theperception ofprofessionalsemployed inthe OR, but the use of interviews and direct observation of surgi-calprocedures,wouldbealsointerestingforamoresuitable approach.
Conflicts
of
interest
Theauthorshavenoconflictsofinteresttodeclare.
Acknowledgments
TheauthorswouldliketothankChief-NurseMariaManuela andtheORboardoftheCentroHospitalardoAlgarve (CHA-Faro)fortheircooperation.
Annex
1.
Safety
Attitudes
Questionnaire-Operating
Room–Portuguese
Version
r
e
f
e
r
e
n
c
e
s
1. USA.InstituteofMedicine.Toerrishuman:Buildingasafer healthsystem.Washington,DC:NationalAcademyPress; 1999.
2. FragataJ.Erroseacidentesnoblocooperatório:revisãodo estadodaarte.RevPortSaúdePública.2011;Vol
Temat(10):17–26.
3. SinglaA,KitchB.Assessingpatientsafetyculture:Areview andsynthesisofthemeasurementtools[Internet].JPatient Saf.2006;2:105–16.
4. DevriendtE,HeedeK,VanDenCoussementJ,DejaegerE, SextonB,WellensNIH,etal.Contentvalidityandinternal consistencyoftheDutchtranslationoftheSafetyAttitudes Questionnaire:Anobservationalstudy.IntJNursStud. 2012;49:327–37.
5. Nordén-HäggA,SextonJB,Kälvemark-SporrongS,RingL, Kettis-LindbladA.Assessingsafetycultureinpharmacies: ThepsychometricvalidationoftheSafetyAttitudes Questionnaire(SAQ)inanationalsampleofcommunity pharmaciesinSweden[Internet].BMCClinPharmacol. 2010;10:8.
6. UK.NationalHealthcareSystem.Anintroductiontosafety climate.London:NationalHealthcareSystem;2010.
7. RossJ.Patientsafetyoutcomes:Theimportanceof
understandingtheorganizationalcultureandsafetyclimate. JPerianesthNurs.2011;26:347–8.
8. TurnbergW,DaniellW.Evaluationofahealthcaresafety climatemeasurementtool.JSafetyRes.2008;39:563–8.
9. FindleyM,SmithS,GorskiJ,O’NeilM.Safetyclimate differencesamongjobpositionsinanuclear
decommissioninganddemolitionindustry:Employees’ self-reportedsafetyattitudesandperceptions[Internet].Saf Sci.2007;45:875–89.
10.FlinR.Measuringsafetycultureinhealthcare:Acasefor accuratediagnosis[Internet].SafSci.2007;45:653–67.
11.BlegenM,PepperG,RosseJ.Safetyclimateonhospitalunits: Anewmeasure.In:HenriksenK,BattlesJB,MarksES,editors. Advancesinpatientsafety.Volume4:Programs,tools,and products.Rockville,MD:AgencyforHealthcareResearchand Quality;2012.
12.TheHealthFoundationInspiringImprovement.Evidence scan:Measuringsafetyculture[Internet].London:TheHealth Foundation;2011.Availablefrom:http://www.health.org.uk/ sites/default/files/MeasuringSafetyCulture.pdf[accessed 08.12.12].
13.UK.HealthandSafetyExecutive(HSE).OffshoreSafety Division.Safetyclimatemeasurement:Userguideandtoolkit [Internet].London:HealthandSafetyExecutive;2004. Availablefrom:http://www.lboro.ac.uk/media/
wwwlboroacuk/content/sbe/downloads/Offshore%20Safety% 20Climate%20Assessment.pdf[accessed15.01.13].
14.SammerC,LykensK,SinghKP,MainsDA,LackanNA.Whatis patientsafetyculture?:Areviewoftheliterature.JNurs Scholarsh.2010;42:156–65.
15.FlinR,BurnsC,MearnsK,YuleS,RobertsonEM.Measuring safetyclimateinhealthcare.QualSafHealthCare. 2006;15:109–15.
16.LingardL,ReznickR,EspinS.Teamcommunicationsinthe operatingroom:Talkpatterns,sitesoftension,and implicationsfornovices[Internet].AcadMed.2002;77:232–7.
17.PereiraMCA.Dinâmicasepercepc¸õessobretrabalhode equipa:umestudoemambientecirúrgico.Covilhã:Faculdade deCiênciasdaSaúde.UniversidadedaBeiraInterior;2010. MestradoIntegradoemMedicina.
18.HelmreichR,SchaeferH.Teamperformanceintheoperating room.NewJersey:Hillsdale;1994.
19.SextonJ,ThomasE.TheSafetyAttitudesQuestionnaire [Internet].Austin:UniversityofTexas;2011.Availablefrom:
http://www.hret.org/quality/projects/walkrounds-saq.shtml
[accessed25.07.13].
20.GörasC,WallentinFY,NilssonU,EhrenbergA.Swedish translationandpsychometrictestingofthesafetyattitudes questionnaire:Operatingroomversion[Internet].BMCHealth ServRes.2013;13:104.
21.SextonJ,HelmreichR,NeilandsT,RowanK,VellaK,BoydenJ, etal.TheSafetyAttitudesQuestionnaire:Psychometric properties,benchmarkingdata,andemergingresearch [Internet].BMCHealthServRes.2006;6:44.
22.BrownTA.Confirmatoryfactoranalysisforappliedresearch. NewYork,NY:TheGuilfordPress;2006(Methodologyinthe socialsciences).
23.DeilkåsET,HofossD.Psychometricpropertiesofthe NorwegianversionoftheSafetyAttitudesQuestionnaire (SAQ):genericversion:ShortForm2006[Internet].BMC HealthServRes.2008;8:191.
24.DevriendtE,VandenHeedeK,CoussementJ,DejaegerE, SurmontK,HeylenD,etal.Contentvalidityandinternal consistencyoftheDutchtranslationoftheSafetyAttitudes Questionnaire:Anobservationalstudy.IntJNursStud. 2012;49:327–37.
25.ShteynbergG,SextonBJ,ThomasEJ.JohnsHopkinsQuality andSafetyResearchGroup.Testretestreliabilityofthesafety climatescale.Austin:TheUniversityofTexasCenterof ExcellenceforPatientSafetyResearchandPractice;2005. TechnicalReport;01-05.
26.FieldA.DiscoveringstatisticsusingSPSS.3rded.LosAngeles: Sage;2009.
27.MarocoJ,MarquesG.QualafiabilidadedoalfadeCronbach? Questõesantigasesoluc¸õesmodernas?LabPsicol.
2006;4:65–90.
28.MakaryM,SextonJ,FreischlagJA,HolzmuellerCG,Millman EA,RowenL,etal.Operatingroomteamworkamong physiciansandnurses:Teamworkintheeyeofthebeholder.J AmCollSurg.2006;202:746–52.
29.WisniewskiAM,ErdleyWS,SinghR,ServossTJ,NaughtonBJ, SinghG.Assessmentofsafetyattitudesinaskillednursing facility.GeriatrNurs.2007;28:126–36.
30.HillA,HillM.Investigac¸ãoporquestionário.Lisboa:Sílabo; 2002.
31.GardeziF,LingardL,EspinS,WhyteS,OrserB,BakerGR. Silence,powerandcommunicationintheoperatingroom [Internet].JAdvNurs.2009;65:1390–9.
32.LingardL,WhyteS,EspinS.Communicationfailuresinthe operatingroom:Anobservationalclassificationofrecurrent typesandeffects.QualSafHealthCare.2004;13:24.
33.ManiasE.StreetA.Nurse–doctorinteractionsduringcritical carewardrounds.JClinNurs.2001;10:442–50.
34.SextonJ,ThomasE,HelmreichR.Error,stress,andteamwork inmedicineandaviation:Crosssectionalsurveys.BrMedJ. 2000;9:745–9.