Rev. Saúde Pública vol.41 suppl.1
Texto
Imagem
Documentos relacionados
AVR - Vascular surgeon and coordinator chief, Serviço de Cirurgia Vascular e Endovascular, Pontifícia Universidade Católica do Rio de Janeiro (PUC-Rio); Scientific director,
Ao longo dos anos, a Mega Sena fez vários premiados, mas percebe-se também (de acordo com o site da Caixa Econômica Federal) que muitos sorteios acabaram sem vencedor(es) e,
Os diretórios de empresas são bases de dados de empresas com um papel bastante importante, tanto no âmbito de prospeção de mercado como na divulgação da empresa. São
The current study set out to explore the views of ostomy patients (colorectal cancer survivors) regarding concepts and cognitions on health and illness, aiming to answer the
[r]
assessed the impact of measures such as the use of surveillance cultures for the early identiication of new cases and the implementation of contact precautions for patients
The expansion of epidemiologic surveillance activities, in addition to acute cases of Chagas disease, integrating cases of the disease in the chronic phase, has to be
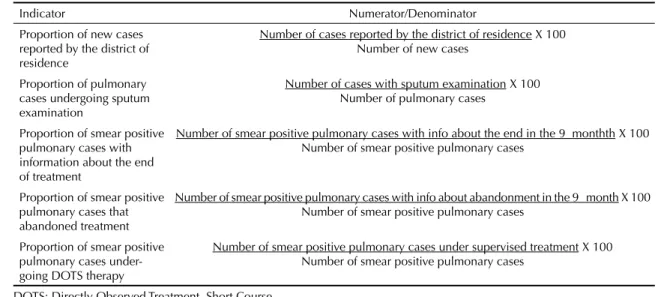
Chart 1 – Dimensions and indicators of assessment of the care produced to tuberculosis cases in Primary Health Care according to the elements of the adapted Chronic Care Model –
