Rev. Soc. Bras. Med. Trop. vol.43 número3
Texto
Imagem
Documentos relacionados
This was the first demon- reinforce the routine delivery of measles stration of the feasibility of interrupting vaccine in all health facilities and to con-
of measles vaccine storage montly, temperature.. Leia-se: of measles vaccine storage,
In conclusion, prompt recognition of the maculopapular rash and Koplik’s spots can help in the early diagnosis of measles, which in turn can aid in limi ting the transmission
Serological evidence of hantavirus infection in an urban area in Mato Grosso State, Brazil. Rev Soc Bras
While PAHO’s recommended vaccination strategy for measles eradication primarily targets infants and children, a small percentage of adolescents and young adults may have escaped
Following the successful initiative to eradicate poliomyelitis from the Americas, the activities carried out to eliminate measles from the Western Hemisphere by the
The Executive Committee observed that progress has already been made towards the elimination goal but stressed that much still remains to be done if the goal is to
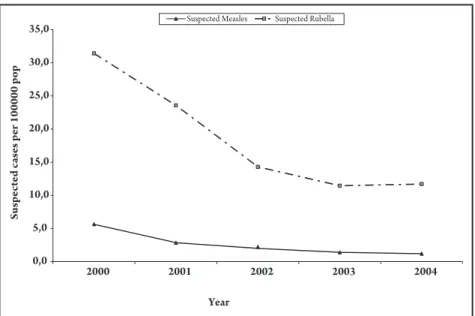
This impressive and rapid reduc ti on in disease burden, resultin g from in cre a sed coverage wi th th e measles vaccine an d its app li ca ti on in mass campai g ns, paved the way
